
Abstract

We read with interest the findings of the survey by Silversides et al. 1 and wish to raise consideration for an interdisciplinary approach to deresuscitation. The authors highlight several notable findings in their survey, including large variability in deresuscitation practice, with 14% of providers opting for fluid administration for diuretic un-responsiveness during fluid overload. Further, regarding diuretic selection for fluid removal, approaches also varied from 7.9% utilizing intermittent bolus diuretics and up to 53.7% utilizing continuous infusion diuresis with albumin concomitantly. 1
Approach to diuretic dosing and monitoring.
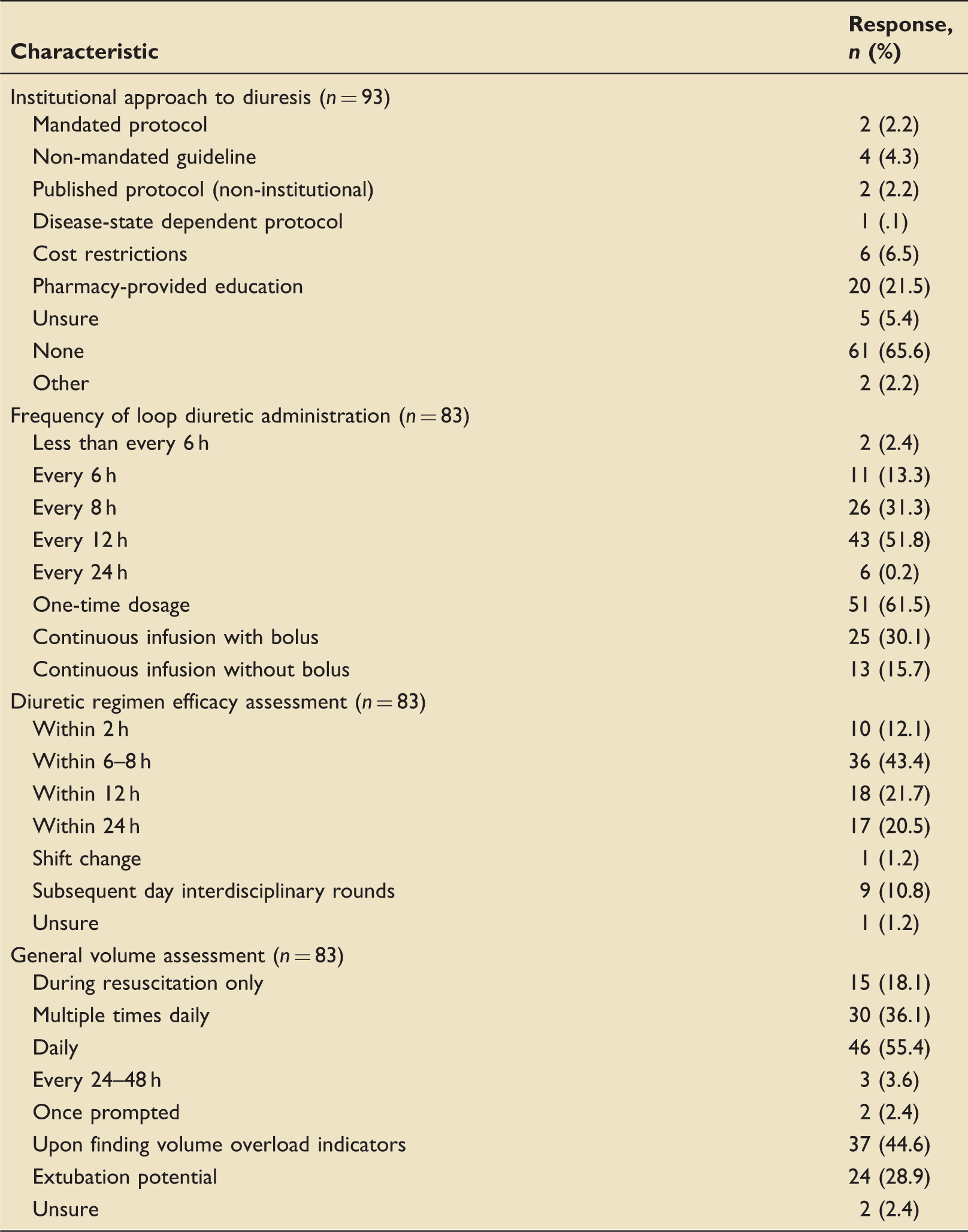
Adjunctive agents utilized and indication (n = 83).
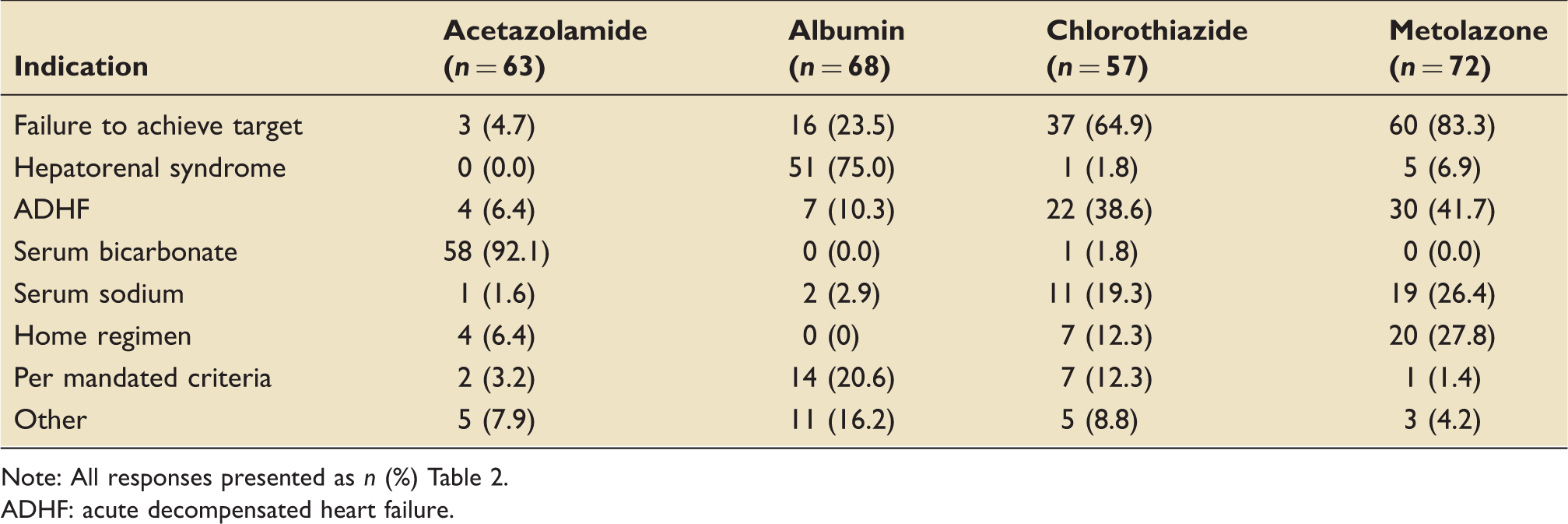
Note: All responses presented as n (%) Table 2.
ADHF: acute decompensated heart failure.
Notable within our survey, limited pharmacist involvement was observed overall (Figure 1). Pharmacist-assisted or pharmacist-driven protocols have shown increased rates of target attainment, improved monitoring, and higher appropriateness of drug therapy.2,3 The defined fundamental and desirable roles of a critical care pharmacist include interdisciplinary education, assistance with pharmacotherapy selection and monitoring, participation in clinical research, and development and implementation of protocols.
4
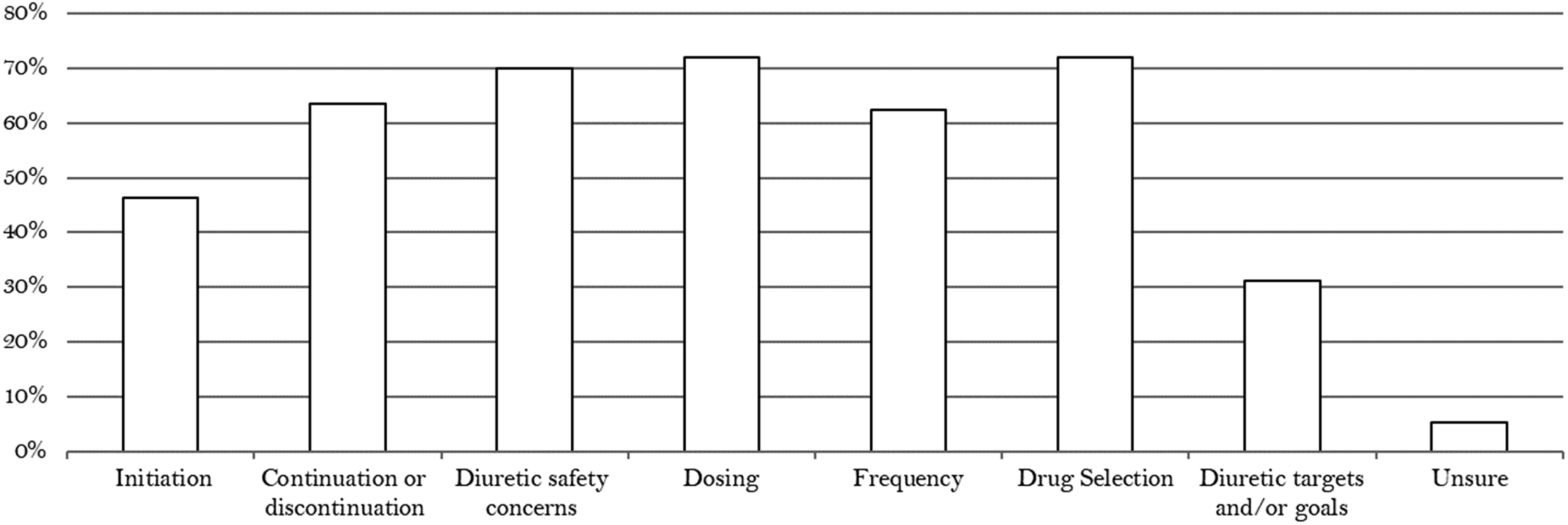
Correspondingly, pharmacist assistance in our cohort, when performed, encompassed many activities (Figure 2).
Frequency of pharmacist involvement in deresuscitation. Pharmacist recommendations regarding deresuscitation.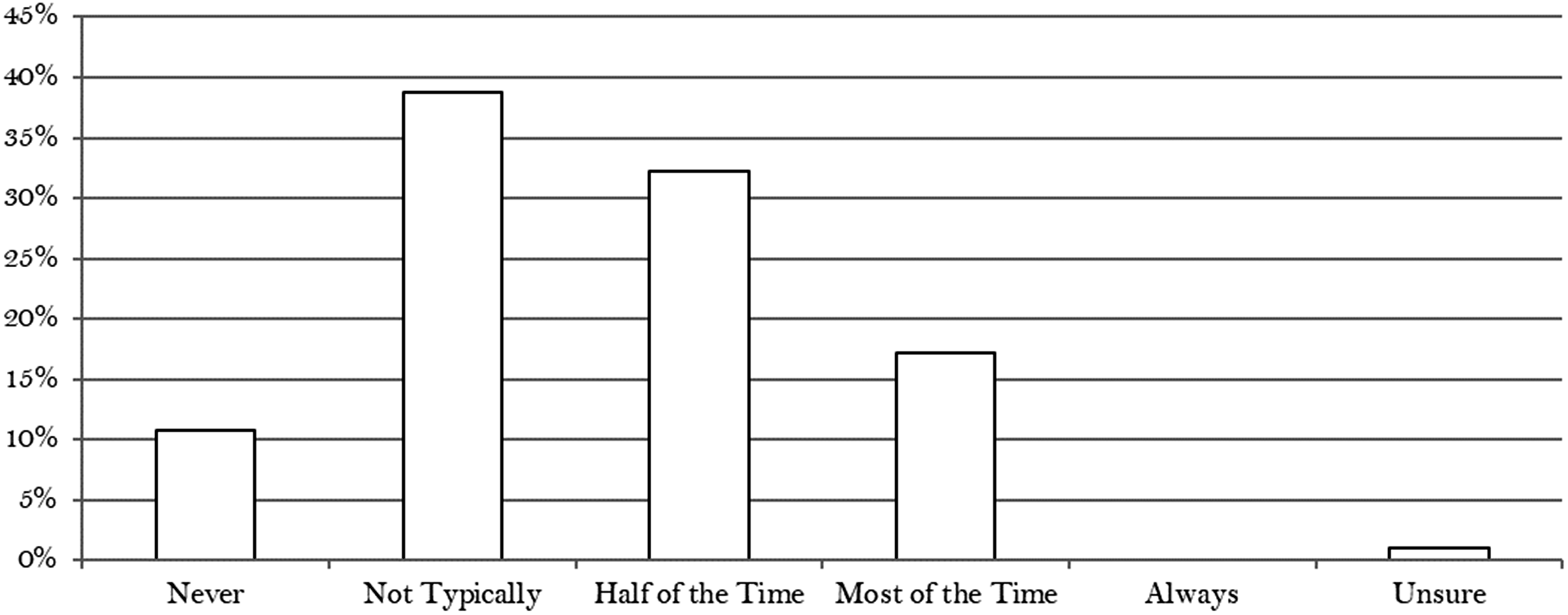
Our survey supports the finding by Silversides et al. regarding a wide variability in current approaches to deresuscitation while suggesting limited pharmacist involvement overall. We believe the lack of standardized deresuscitation measures as seen in both cohorts represents an opportunity for interdisciplinary collaboration and concur that development of standardized approaches and randomized controlled trials of deresuscitation are needed. Given the lack of surrounding diuretic pharmacokinetic and pharmacodynamics in this population, pharmacists are in a unique position to assist with development of such protocols. 5 We propose the inclusion of clinical pharmacists in project and/or protocol development in alignment with standard pharmacy roles to assist in the overall improvement of clinical outcomes in the critically ill population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.