
Abstract
To the Editor,
Vitamin D [25OH)D] has been hypothesized to promote innate and acquired immunity. The enzyme 1α-hydroxylase exists within macrophages and dendritic cells and is thought to convert vitamin D into its active form. 1 Since 2009, many studies have associated critical illness with vitamin D deficiency. 2 While mortality benefit of vitamin D supplementation on general hospital admission has been demonstrated, to our knowledge, its effect on septic critical care admission has not been evaluated. 3
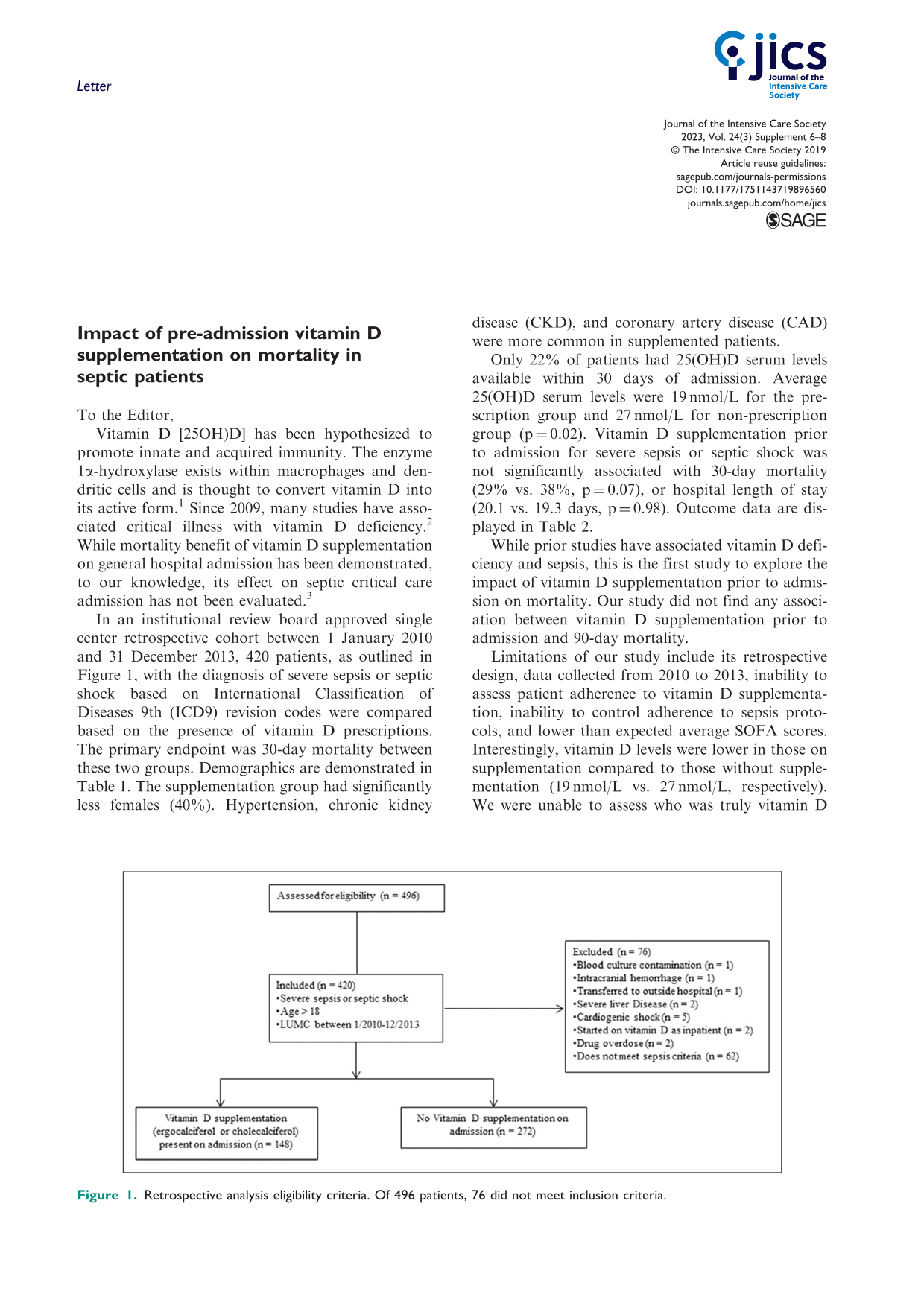
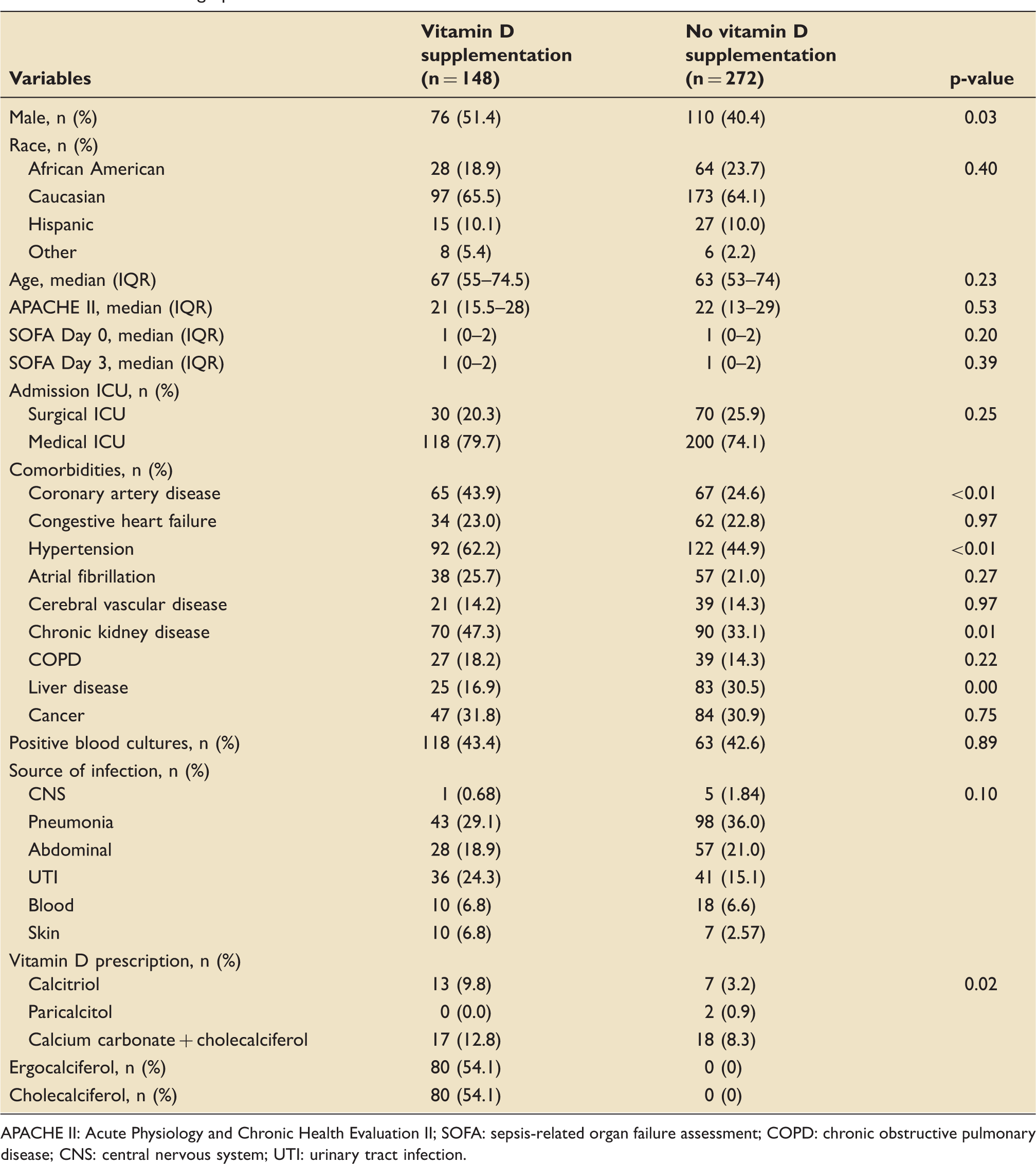
In an institutional review board approved single center retrospective cohort between 1 January 2010 and 31 December 2013, 420 patients, as outlined in Figure 1, with the diagnosis of severe sepsis or septic shock based on International Classification of Diseases 9th (ICD9) revision codes were compared based on the presence of vitamin D prescriptions. The primary endpoint was 30-day mortality between these two groups. Demographics are demonstrated in Table 1. The supplementation group had significantly less females (40%). Hypertension, chronic kidney disease (CKD), and coronary artery disease (CAD) were more common in supplemented patients.
Retrospective analysis eligibility criteria. Of 496 patients, 76 did not meet inclusion criteria. Baseline demographics. APACHE II: Acute Physiology and Chronic Health Evaluation II; SOFA: sepsis-related organ failure assessment; COPD: chronic obstructive pulmonary disease; CNS: central nervous system; UTI: urinary tract infection.
Clinical outcomes.

IQR: interquartile range.
While prior studies have associated vitamin D deficiency and sepsis, this is the first study to explore the impact of vitamin D supplementation prior to admission on mortality. Our study did not find any association between vitamin D supplementation prior to admission and 90-day mortality.
Limitations of our study include its retrospective design, data collected from 2010 to 2013, inability to assess patient adherence to vitamin D supplementation, inability to control adherence to sepsis protocols, and lower than expected average SOFA scores. Interestingly, vitamin D levels were lower in those on supplementation compared to those without supplementation (19 nmol/L vs. 27 nmol/L, respectively). We were unable to assess who was truly vitamin D deficient between the groups nor the number of patients that were taking their prescription.
Our results are consistent with limited subgroups in studies that have looked at supplementation after critical care admissions that encompass other forms of shock.4,5 Further exploration into this subject deserves evaluation through a prospective study design that ensures compliance with supplementation and includes monitoring of vitamin D serum concentration goals.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.