
Abstract

Background
Post-pyloric feeding tube (PPFT) insertion in critically ill patients may lower the rate of pneumonia by 30% and increase the amount of nutrition delivery. 1 However, PPFT placement is challenging, either requiring sophisticated radiological or endoscopic assistance. 1 Non-endoscopic methods that have been described for PPFT are cumbersome and/or require special feeding tubes.2–5 The Corpak 10-10-10 rule is a novel way of bedside insertion of a PPFT.6,7 This pilot study describes a further simplification of that method in critically ill patients with gastric ileus.
Methods
This was an observational study performed in a convenience sample of adult critically ill patients admitted under the care of the author between October 2017 and November 2018. All patients had undergone a bedside non-endoscopic insertion of a PPFT. The de-identified details of all included patients were prospectively collected in a spreadsheet. Institutional ethics committee approval was obtained to analyse this data.
The main inclusion criterion was the failure to absorb enteral feeding by the gastric route, defined as fourth-hourly gastric residual volume ≥400 mL for ≥48 h. The only exclusion criterion prior to insertion of the PPFT was mechanical bowel obstruction.
The non-endoscopic bedside insertion technique of the PPFT was as follows:
A standard fine-bore feeding tube (Corflo 8F tube) with a stylet in situ was used in all patients. The insertion of the tube did not warrant any changes to the patient’s position in the bed. After lubricating the tip of the tube with a water-based lubricant gel, the tube was inserted either nasally or orally into the stomach to a depth of ∼30–40 cm. The stylet was not removed. After confirming appropriate gastric position on a chest X-ray, the bedside nurse was instructed to manually advance the tube by ∼10 cm every hour till a depth of ∼70–80 cm. The final position of the tip of the tube was confirmed using a combined lower chest-upper abdominal X-ray.
Results
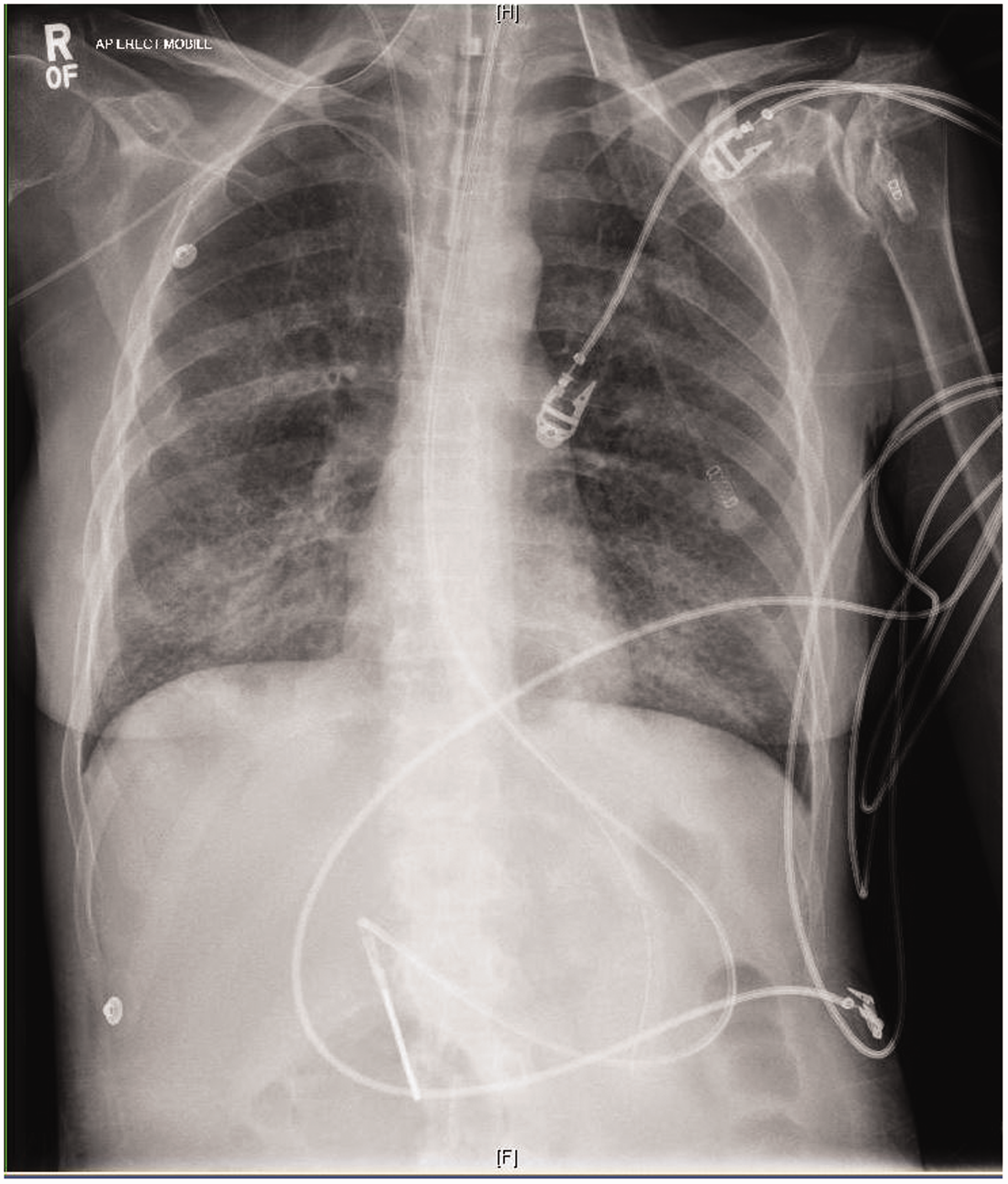
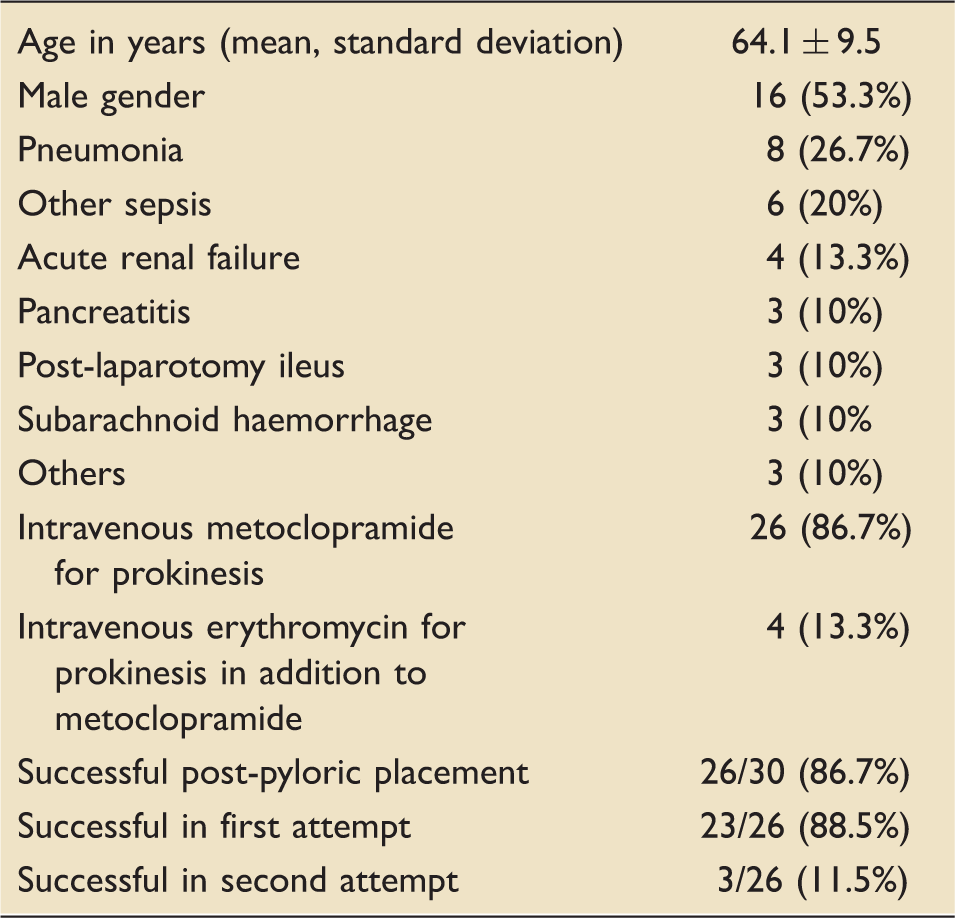
Table 1 lists the details of the patients. Post-pyloric placement was successful in 26 of the 30 patients (86.7%) (Figures 1 and 2). The nasal route was used in 26 patients (86.7%) and the oral route was used in 4 patients (13.3%). The final position of the tip of the tube was in the jejunum in 17 patients (65.4%) and in the third or fourth part of the duodenum in 9 patients (34.6%). Of note, the insertion was successful in all three patients with post-laparotomy ileus and all three patients with pancreatitis. In every patient, enteral nutrition was well absorbed through the PPFT with the target nutritional rate achieved within 24 h. In the unsuccessful patients, the tube was found curled in the mouth in two patients and coiled in the stomach in two patients. There were no procedural complications.
Jejunal placement. Duodenal placement. Patient characteristics and results.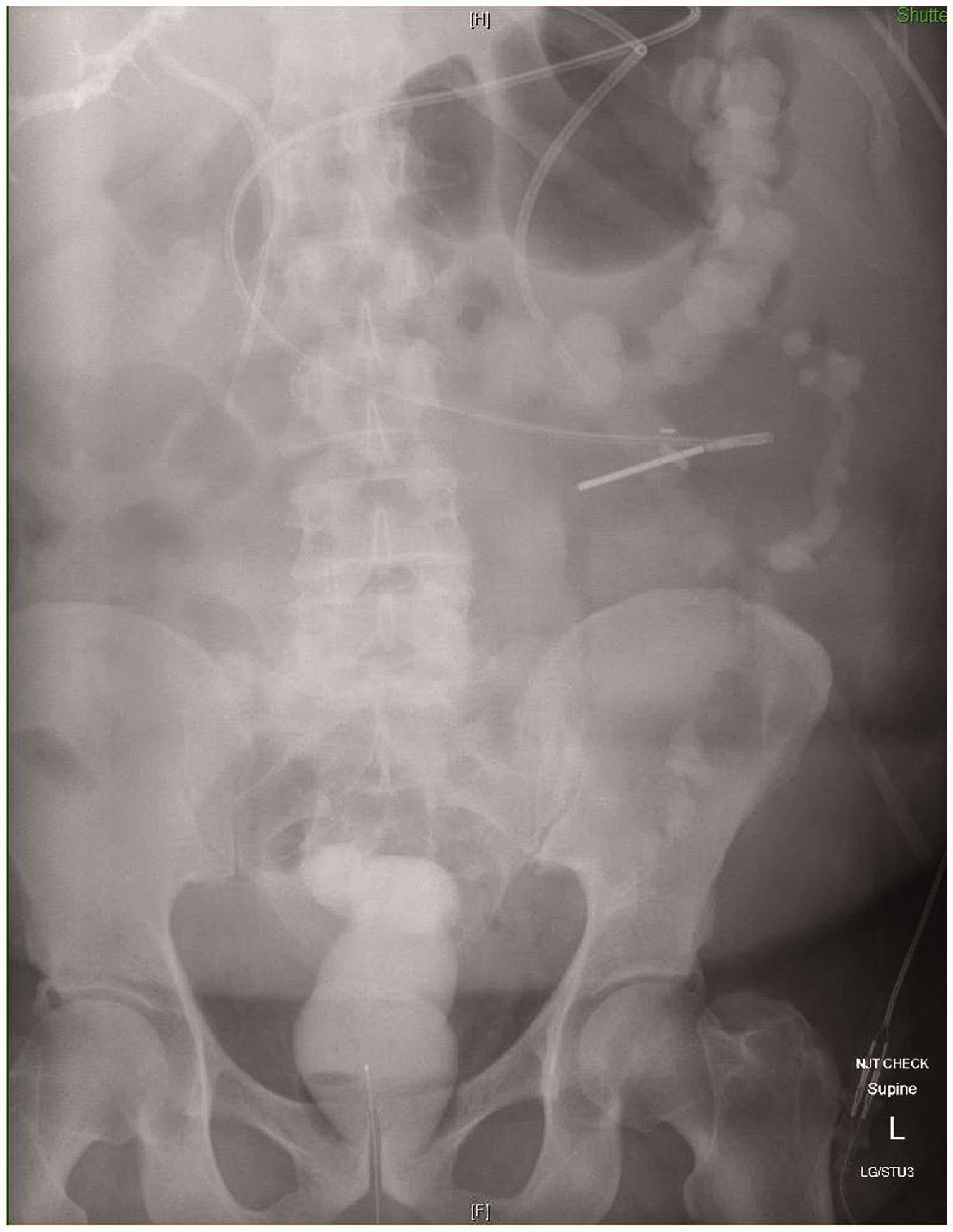
Discussion and conclusion
This study describes a simple non-endoscopic technique to insert a PPFT. It has the advantage of being implemented by the bedside nurse using simple manoeuvres, inexpensive equipment and no special investigations, with a high success rate even in patients with surgical abdominal pathology. However, it is at best a ‘proof of concept’ pilot study due to its inherent limitations of being done in convenience sample in a single centre without randomisation or masking. Even so, a simple procedure like this with few or no complications may be a reasonable option for intensivists to consider in patients who do not absorb gastric tube feeding despite pharmacological measures.
Footnotes
Acknowledgements
The author is responsible for the following roles: conceptualisation, data curation, formal analysis, methodology and writing the manuscript. This work is approved by the NBMLHD Ethics Committee (Approval Number – Project No: 18/56 (A)).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.