
Abstract
Introduction
Elevated sound levels in critical care are associated with sleep deprivation and an increased incidence of delirium. We aimed to determine whether a sound-activated visual noise display meter could cause a sustained reduction in sound levels overnight in an adult critical care unit.
Method
Sound levels were recorded overnight for eight days before and after the introduction of a visual noise display meter, with a further eight days recorded four months later after continued use of the visual noise display meter.
Results
Median ambient sound levels were significantly reduced from 57.4 dB by 3.9 dB, with a sustained reduction of 3.6 dB from baseline after four months of the device operating. Peak ambient sound levels had a small but significant reduction from 66.0 dB by 0.7 dB, with a sustained reduction of 0.8 dB after four months.
Discussion
Sound-activated visual noise display meters can be effective in providing a sustained reduction in ambient sound overnight in adult critical care units, which would appear to be driven by behavioural change.
Introduction
Critical care units are noisy and busy environments, with patients being subjected to disturbances throughout the day and night.1,2 Elevated ambient sound levels are associated with adverse physiological and psychological effects on hospitalised patients, including annoyance, sleep disturbance and interference with rest and recovery.3–5 Furthermore, the physiological and psychological effects of poor sleep, including its association with delirium, is becoming increasingly recognised.3–7 Delirium in critical care is independently associated with a longer inpatient length of stay, prolonged recovery and a higher patient mortality and morbidity.7,8
Polysomnography, a multi-parametric sleep study tool used to investigate and diagnose sleep disorders, has demonstrated poor sleep-wake cycles in mechanically ventilated critical ill patients. 9 It is also evident that critical care patients’ exhibit severely altered sleep architecture, with patients frequently experiencing broken sleep cycles, large variations in total sleep time, and loss of the normal circadian rhythm with a higher frequency of daytime sleeping compared to night-time sleeping. One of the key contributors to this is postulated to be noise.10,11
The World Health Organisation (WHO) recommendations for noise levels suggest that hospitalised patients in observation or treatment areas should not be exposed to ambient sound levels of greater than 35 dB, with a night-time peak noise level of 40 dB. 12 Lack of compliance with these recommendations in the critical care setting has been demonstrated by multiple studies, with elevated sound levels being attributed to both equipment and human activity.1,2,6,13,14 It is thought that hospitals are becoming increasingly louder, and some studies suggest that maintaining levels of ambient sound below the WHO recommendations is not achievable without a specific noise reduction management programme.15–17
In a previous study, our critical care unit trialled a bundle of measures to reduce night-time environmental noise and light, with the aim of limiting iatrogenic sleep disturbance. 18 The measures taken to reduce sound included: limiting staff conversation around patient bed-spaces, reducing alarm levels on equipment, reducing sound levels on phones and pagers, and offering patients earplugs overnight. The measures taken to reduce environmental light and promote normal circadian sleep patterns included: offering patients eye masks; switching off overhead lights from 23:00 h until 07:00 h; and grouping together patient care activities and interventions to allow a minimum of 2 h of undisturbed sleep. Within the controlled conditions of the trial, the bundle was shown to improve sleep, half the incidence of delirium, and reduced mean ambient sound overnight by 6.9 dB within two weeks of implementation However, outside of research conditions the adoption of these measures has not been sustained, as it is felt that the measures are not ingrained in routine staff practice.
SoundEar is a noise monitoring and visual warning device, which can constantly measure, document and display ambient sound levels to provide a visual representation of noise levels in a given environment. 19 It can be used to visually alert staff when noise levels are approaching or breach a pre-set threshold. The use of SoundEar devices in neonatal critical care units and operating theatres in this manner has demonstrated a reduction in sound levels that patients are exposed to.20,21
This study aimed to evaluate whether the use of the SoundEar device can reduce night-time noise levels in the adult critical care environment, and whether continued use of its warning system could lead to a sustained reduction in night-time noise levels.
Methods
Study design
The study took place in a 24-bedded, mixed medical, surgical, and neurosciences adult critical care unit in Preston, Lancashire, UK. A SoundEar 3 device (SoundEar A/S, Birkerød, Denmark), a noise meter with visual feedback capabilities, was deployed over the nurses’ station in the centre of seven-bedded closed bay within the critical care unit, containing five beds within the bay and two side rooms. The microphone was positioned over the centre of the nurses’ station, as this was found to be the loudest point in the area during our pilot study, and calibrated prior to the start of the study. The display on the device was visible from all bed spaces.
Baseline data collection was undertaken over a period of eight consecutive nights. Following this the SoundEar 3 device’s visual warning system was introduced and a further eight consecutive nights data collection was taken. Follow up data was collected after four months of continued use of the device. No investigators were present in the clinical environment during data collection periods. Neither the staff in the unit nor the patients were made aware that this study was being conducted or that noise levels were being recorded. No other interventions targeting the night-time environment were implemented at this time.
The study was registered with the Research and Innovation Department at Lancashire Teaching Hospitals, and ethical approval waived.
Data collection
Ambient (LAS, or A-weighted) and peak (LCpeak, or C-weighted) sound levels 22 were recorded overnight, defined as 23:00 h to 07:00 h. Recordings were made by the SoundEar for eight days with the visual warnings on the device not activated.
Following this the visual warnings on the device were activated. They were set to display green if ambient sound was less than 60 dB, orange if ambient sound was between 60 dB and 70 dB, and red if ambient sound was above 70 dB. Warnings remained off during the day-time (07:00 to 23:00 h). Data on ambient and peak overnight sounds levels was then recorded for a subsequent eight days.
After initial data collection, the devices were left in clinical practice with warning devices activated overnight. Four months after the initial data collection, the same recordings on ambient and peak overnight sounds levels were collected for a further eight days.
Data analysis
Data were exported from the noise meters as comma-separated values (CSV) files. LAS readings were made every second, LCpeak up to 10 times a second. Data were analysed in R 3.2.3 (R Core Team, Vienna, Austria) 23 using the ggplot2 package. Sound levels for each day were summarised as a time series to check for anomalous values.
As sound levels were non-normally distributed, ambient and peak sound levels between intervention phases are presented as median [interquartile range]. Non-normality of data also prohibits the use of t tests and ANOVA, whilst the non-symmetry of the distributions prohibits the use of Wilcoxon signed rank test. We therefore opted to test that there was a difference in time under a given threshold using the Kolmogorov-Smirnov test. However, since this does not indicate the reason for the difference (median, variance, outliers, etc.), we explicitly tested for a reduction in median sound level using Mood's median test. 24
Results
Change in total peak and ambient sound levels at different intervention stages.

Significantly different (p < 0.0001) by Mood's median test.
Median peak sound levels had a small but significant reduction of 0.7 dB from 66.0 dB [64.4–67.9] to 65.3 dB [64.4–66.5] after intervention with the SoundEar 3 device (p < 0.0001). This effect also persisted at four months with peak sound levels remaining at 65.2 dB [63.6–67.2] (p < 0.0001).
The effect of the SoundEar device on sound levels through time during the night can be visualised using threshold plots showing the proportion of total time spent below a specified sound level threshold (Figure 1). These demonstrate that both ambient and peak sound levels spent a greater proportion of time at a lower level both after intervention (green) and at four months follow-up (blue) when compared to the pre-intervention baseline (red).
Proportion of time per intervention phase that (a) ambient and (b) peak sound levels remained below a given threshold. Red: baseline; green: after introduction of visual noise warning devices; blue: at four month follow up.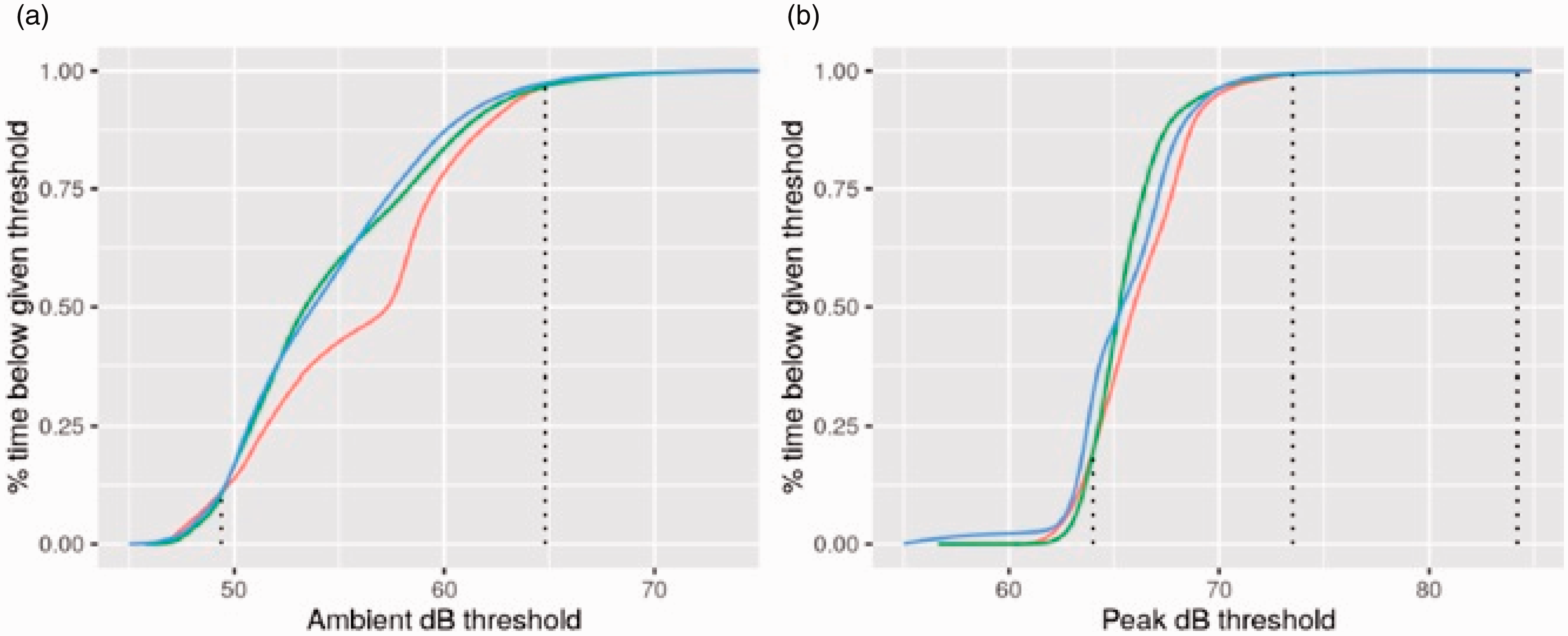
Ambient sound levels spent more time below a threshold of 49.4 to 64.8 dB (shown with dotted lines) after intervention and at follow up when compared to the pre-intervention baseline. Peak sound levels spent more time below a threshold of 64.0 to 73.5 dB after intervention, with peak levels remaining below the baseline up to 84.2 dB at four months follow-up. Two-sample Kolmogorov-Smirnov testing demonstrated a significant difference comparing baseline and post-intervention and comparing baseline with four months (p < 0.0001 in both cases).
During the study period the bed occupancy remained at > 95%, which is the norm for this critical care unit. Whilst no unusual clinical patterns of patient-related or staffing-related activity were identified, this was not specifically measured for the purposes of this study, thus the results are not adjusted for activity levels or acuity of patients.
Discussion
This study demonstrated that introduction of a SoundEar 3 visual noise warning device during night-time hours within an adult critical care unit can offer a sustained and significant reduction in both ambient and peak sound levels. The device acted as an isolated intervention to significantly reduce night-time ambient and peak sound levels, a change that was sustained after a four-month period.
Greater reductions in ambient rather than peak sound levels were produced using the SoundEar 3 visual warning system. It is plausible that the greater reduction in ambient sound levels was due to direct visual feedback regarding noise levels passively affecting modifiable human behaviours, such as volume and quantity of speech. The lesser reduction observed in peak sound levels may be explained by the SoundEar3 having a reduced influence on less-modifiable or non-modifiable noises, such as medical devices, monitoring alarms, and unintentional peak noises from doors, bins and moving equipment.
Staff members were intentionally not made aware that the device was being introduced, nor that sound levels were being recorded in addition to the visual demonstration of noise levels being displayed. This was therefore an isolated intervention, rather than being part of a concomitant programme of noise reduction or environmental modification, yet demonstrated a sustained reduction in sound levels just by the device being present, without any form of education being required. Although feedback from clinical staff to demonstrate the extent to which they modified their behaviour in accordance with the SoundEar 3 visual noise display was not formally gathered as part of this study, staff commented to the investigators in routine clinical practice that the SoundEar3 reminded them overnight to reduce their volume of speech. Feedback also suggested that the system reminded staff to promote sleep via other measures, such as grouping interventions to minimise disruptions to sleep.
Based on these results, we suggest that sound-activated visual noise warning devices should be considered in adult critical care units as part of an effort to promote healthy sleeping patterns in critically ill patients. The benefits of the SoundEar 3 system include a system that is easy to introduce and maintain, and which can record and produce visual feedback to noise levels that are not dependent on staff monitoring.
The limitations of the study included recording noise in a central area, within a seven-bedded closed bay in the critical care unit, as opposed to taking measurements at individual bed-spaces or at the patients’ ear level. Any variation in sound levels in the immediate environment around individual bed-spaces, including clinical and non-clinical equipment, was not measured in this study. It can be postulated that patients in the same clinical area could have been exposed to differing sound levels during the course of the study. We also note that despite the positive results of this intervention and the significant impact that this intervention had on noise levels, patients continued to be exposed to noise levels above the WHO recommendations for hospitalised patients. 12
Furthermore, whilst it is clear that noise reduction can be achieved with the use of the SoundEar 3 device, the question of its link to the incidence of delirium was not investigated in this study. Further research is now underway to ascertain whether the SoundEar devices can act synergistically with an environmental night-time modification programme, to improve sleep quality and reduce the incidence of delirium, and hence have potential to reduce the overall cost of treating critical illness.
A priority is now to assess whether the introduction of a bundle of sleep promoting measures as used in our previous study 18 alongside the SoundEar device can act synergistically to reduce both ambient sound and delirium rates. Nevertheless, we feel that the SoundEar3 is a valuable addition to the technological landscape that can offer a moderate and sustained reduction in night-time noise levels.
Footnotes
Acknowledgement
SoundEar 3 devices were provided free of charge by SoundEar A/S (BirkerÃd, Denmark), with explicit agreement to publish results regardless of positive or negative findings.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.