
Abstract

There is no doubt that as doctors we are committed to the implementation of safe practice and developing a high degree of technical competence. However, studies have shown that it is often not technical skills which are lacking, when things go wrong. Factors such as human fallibility, miscommunication, poor coordination of team activity, human–technology interaction and suboptimal management of the environment are all contributory to making errors. The aim of the National Safety Standards for Invasive Procedures (NatSSIPs) guideline is to address these areas by building on the existing World Health Organization (WHO) checklist structure and formalising the organisational, educational and governance structures that currently exist in our organisations. It is only by building a patient safety focused mentality within the National Health Services (NHS) that these guidelines will bring about change and the subsequent improvements we strive for.
Background
Improving patient safety has been one of the main focuses of the NHS over recent years. This is illustrated by the numerous campaigns initiated since the launch of the first high-profile project, the Never Events Framework in 2009, 1 the goal of which was to increase patient safety by encouraging greater transparency and accountability following serious patient safety incidents. Within the theatre environment, WHO checklists were similarly introduced in 2009, 2 focusing on the theatre environment in an effort to improve surgical safety and consequentially reduce morbidity and mortality.
Interestingly, despite the WHO checklist being rolled out across the country, surgical never events have remained the most commonly occurring never event within the English NHS, with 329 events in 2012–2013 alone. This led to NHS England commissioning the Surgical Never Events Taskforce to examine and clarify the reasons why these patient safety incidents continued to occur. In 2014, the taskforce published a document called ‘Standardise, Educate and Harmonise’ which recognised that checklists alone were not sufficient to improve safety and a more integrated approach was required, such as those used in other high-risk industries, e.g. aviation. 3
The NatSSIPs document 4 addresses the three themes from the ‘Standardise, Educate and Harmonise’ paper, providing high-level national standards for all invasive procedures during which a surgical never event might take place. Each individual institution will be expected to produce localised standards that satisfy the new national guidance, the aim of which is to change global attitudes to patient safety and ensure there is a culture shift in normal staff behaviour within our hospitals, the ultimate aim of which is to place patient safety firmly at the heart of our future NHS.
Previously, the use of the WHO checklist was confined to the operating theatre; however, NatSSIPs extends the remit of standardised procedural standards to all invasive procedures, moving this culture beyond the walls of the operating department and into the wider hospital setting. This is of particular interest to the intensive care community. With the management of intensive care patients frequently involving multiple ‘invasive procedures’, there is an opportunity for the integration of Local Safety Standards for Invasive Procedures (LocSSIPs) into our daily practice, leading to enhanced working practices in the intensive care unit. Previously, individual units have developed and used procedure-specific checklists, e.g. percutaneous tracheostomy and intubation; however, the creation and adoption of a culture focusing on improving patient safety have not been uniform across the board. It is this precise issue that NatSSIPs aim to address.
To that end, the guideline is also explicit in its requirement to focus on education as a component of each local guideline, specifically necessitating the need for uniformity in how staff are trained and educated to perform different procedures. The persons capable of performing the procedure on each unit should be identified and assessment of their capacity to perform the procedure should be regularly checked and documented, e.g. via appraisal or during an induction to a new unit.
Lastly, the document addresses how robust governance structures will be required to support the implementation of each LocSSIPs. Organisations will need to ensure there is consistency in reporting and publication of serious incidents, with regular audit to confirm each procedure is being performed according to the documented standards. The introduction of an Action Log to record the complications and problems encountered during each procedure has been suggested as a means to achieve this. Whatever the strategy employed to identify problems, it will be an essential to embed a culture of disseminating any learning points back to those responsible for performing the procedure. This will also allow for regular review of each individual LocSSIPs to ensure it remains fit for purpose and address any recurring safety issues.
Experience of a local centre – The Walton Centre
In January 2016, Dr. Sandeep Lakhani, clinical director of Anaesthesia and Neuro-critical care at The Walton Centre convened a group to establish safety checklists for invasive procedures performed within the intensive care department. This group contained the majority of stakeholders within the unit and included:
Two consultant Anaesthetists A consultant Neurosurgeon Lead Intensive Care nurse Nursing staff from critical care outreach Senior Operating Department Practitioner Clinical fellow Operational services manager
The critical care LocSSIPs group worked in parallel with three other LocSSIPs groups within the hospital covering other clinical areas: theatres, radiology and wards/outpatients.
During initial meetings, a draft terms of reference was created to outline the group’s authority, role, membership and review details. It was also agreed that the group would be responsible for producing checklists for the following procedures:
Tracheostomy insertion Emergency intubation in Critical Care Bronchoscopy Chest drain insertion Central venous access Naso-gastric tube insertion
Arterial line insertion was a well-discussed area as it is, in some opinions, more ‘invasive’ than simple cannulation; however, due to the frequency that arterial line insertion is performed within the department and the fact is sits across the boundary of opinions with regard to the definition of ‘invasive procedure’, it was not included. Obviously, there is the potential for a retained guidewire never event and so the group agreed to keep this under review.
Several other procedures specific to Neuro-critical Care were also considered; however, it was felt that further discussion with the Trust’s other LocSSIPs groups would be required before their implementation, e.g. Lumbar drain insertion, intracranial pressure bolt insertion, intrathecal injections and the tapping of V-P shunts.
The starting point for the design of the WHO style checklists was the two checklists already in use by the department for tracheostomy insertion and central line insertion. The broad concept and contents of these checklists were kept; however, modifications to the structure to correlate with the five steps to safe surgery were adopted and a pre, during and post procedure time out were incorporated.
After the design and content of the checklists had been decided, the group determined how the new checklists would be rolled out for use within the Trust. At the time of writing this article, this process is ongoing; however, the order of events will follow the following timeline:
The development of a standard operating procedure for the checklists Small scale roll out of the checklists within individual department to pick up any operational problems Re-evaluation of the LocSSIPs based on operator experiences and feedback Full roll out of the checklists to all areas within the hospital where the procedure is performed
In this full roll out, a series of rolling workshops will be held for all permanent staff members to identify reasoning, roles and responsibilities for all involved. For the rotating Anaesthetic trainees passing through the department, this workshop could be held during their induction. During the initial three months, feedback forms will be circulated and collected to ascertain areas of improvement for the checklists which can be enacted by the LocSSIPs group in due course. This will be in addition to the regular review of each LocSSIPs.
The Intensive Care Society/Faculty of Intensive Care Medicine example checklists
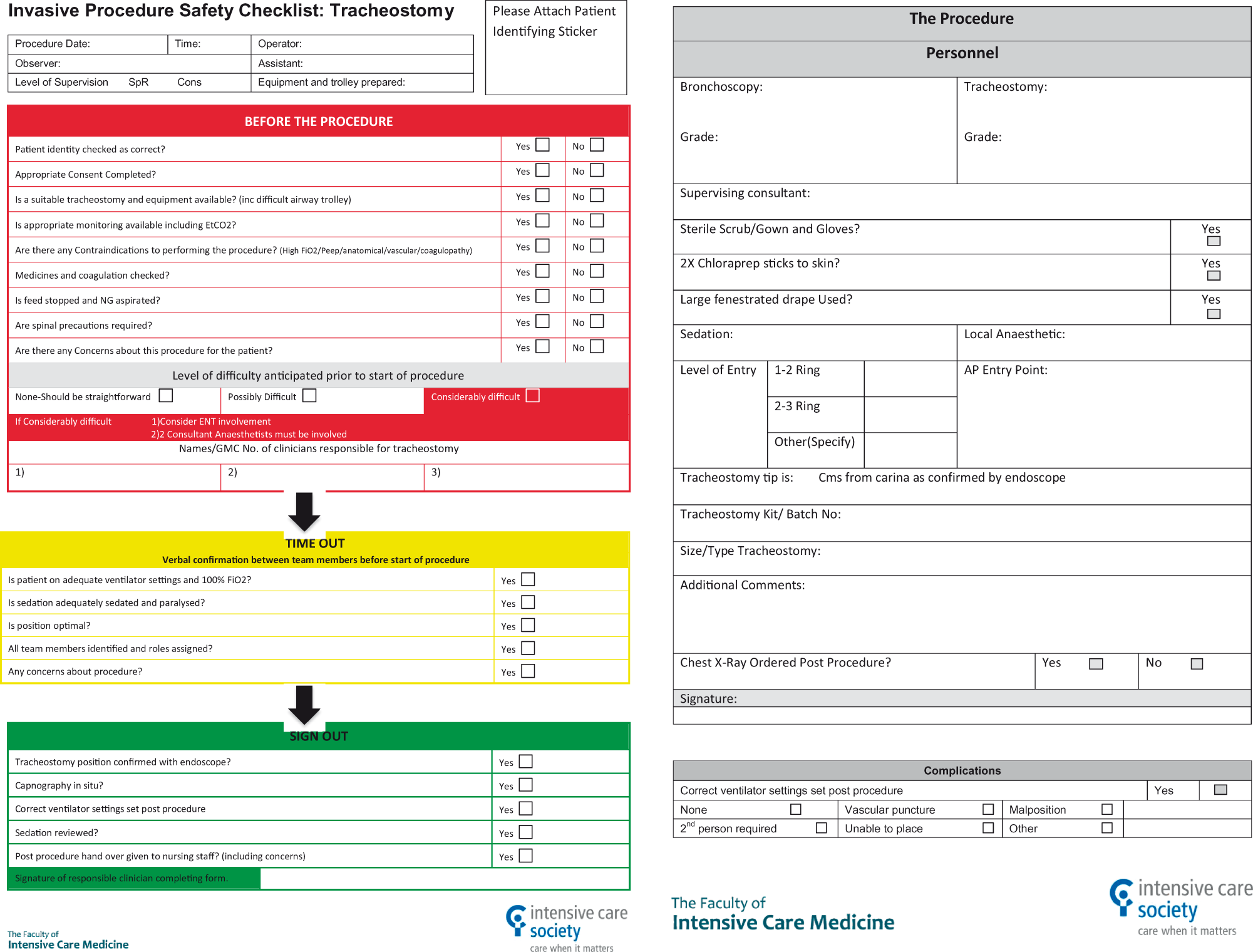
After the publication of the NatSSIPs document, the Intensive Care Society (ICS) and Faculty of Intensive Care Medicine (FICM) Joint Standards Committee discussed the introduction of these guidelines and have in conjunction with The Walton Centre in Liverpool produced generic checklists for the six procedures described above.
Percutaneous tracheostomy Intubation Bronchoscopy Central venous catheter line insertion Chest drain insertion Naso-gastric tube insertion
The aim of these documents is to provide a starting point for hospitals that have yet to formally adopt LocSSIPs which adhere to the new national guidance. There is certainly some urgency with regard to their development as following the publication of NatSSIPs, institutions were required to initiate a review of local policies and begin the development of localised safety standards by September 2016. In light of this, the ICS/FICM have produced WHO style pre, intra and post procedure checklists (that will be available from the ICS website at the end of January), which should accompany the performance of each invasive procedure. The checklists are not designed to stand alone with each individual institution being responsible for the education, training and clinical governance required for each procedure. Like we have seen before, an institutional change does not come from the mere introduction of a checklist, but it comes from a cultural change and the adoption of safety conscious behaviour amongst its staff.
Footnotes
Acknowledgements
The authors thank Dr Sandeep Lakhani (The Walton Centre) and Dr Gary Masterson, Dr Stephen Webb, and the Joint Standards Committee of the Intensive Care Society/Faculty of Intensive Care Medicine for their help with this work. The Walton Centre was also the institute where work for the project was performed. Edited 4th June 2017 by Peter Bamford.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.