Critically appraised topic: Effect of noninvasive ventilation delivered by helmet vs. face mask on the rate of endotracheal intubation in patients with acute respiratory distress syndrome
Free accessResearch articleFirst published online November, 2017
Critically appraised topic: Effect of noninvasive ventilation delivered by helmet vs. face mask on the rate of endotracheal intubation in patients with acute respiratory distress syndrome
In patients with Acute Respiratory Distress Syndrome (ARDS) requiring non-invasive ventilation (NIV) for more than 8 h, the use of the helmet interface, when compared with a face mask, was associated with a significantly lower endotracheal intubation rate (NNT = 2) and a reduction in length of Intensive Care Unit (ICU) stay, hospital mortality (NNT = 5) and 90-day mortality (NNT = 4). Level of evidence: 2B (RCT with wide confidence intervals)
Appraised by: Christopher WM Horner
Citation: Patel BK, Wolfe KS, Pohlman AS et al. Effect of Noninvasive Ventilation Delivered by Helmet vs Face Mask on the Rate of Endotracheal Intubation in Patients with Acute Respiratory Distress Syndrome. JAMA 2016;315:2435-2441.
Patients: Adult patients admitted to a medical ICU requiring NIV for more than 8 h for ARDS as defined by the Berlin Criteria.1
Intervention: After 8 h of NIV via a facemask, patients were randomised by computer to either continue with the facemask interface (control group) or switch to the helmet interface (intervention group).
Outcomes: Primary outcome was the proportion of patients who required endotracheal intubation. Secondary outcomes were 28-day invasive ventilator free days; ICU and hospital length of stay; and hospital and 90-day mortality.
Study design:
Single-centre, unblinded randomised control trial with intention-to-treat analysis
Study patients:
Inclusion criteria: Patients 18 years or older who required more than 8 h of NIV via a facemask for ARDS as defined by the Berlin criteria1 from September 2012 to September 2015.
Exclusion criteria: Impending cardiopulmonary arrest, Glasgow Coma Score (GCS) less than 8, absence of airway protective gag reflex, raised intracranial pressure (ICP), tracheostomy, upper airway obstruction, pregnancy or patient not for endotracheal intubation.
A total of 4226 patients were admitted to the medical ICU during this period and so underwent screening. Among them, 740 met the inclusion criteria, 657 were excluded and 83 underwent randomisation.
Study groups: Thirty-nine patients were assigned to continue on NIV via facemask and Philips Respironics V60 non-invasive ventilator. Forty-four patients were randomly assigned to receive NIV via the helmet interface and Engström Carestation, GE Healthcare ICU ventilator as the helmet interface was not compatible with the Philips Respironics V60. NIV was titrated according to a standard protocol in both groups and the decision to intubate was made by the primary care team, based on predetermined criteria, without involvement of the researchers.
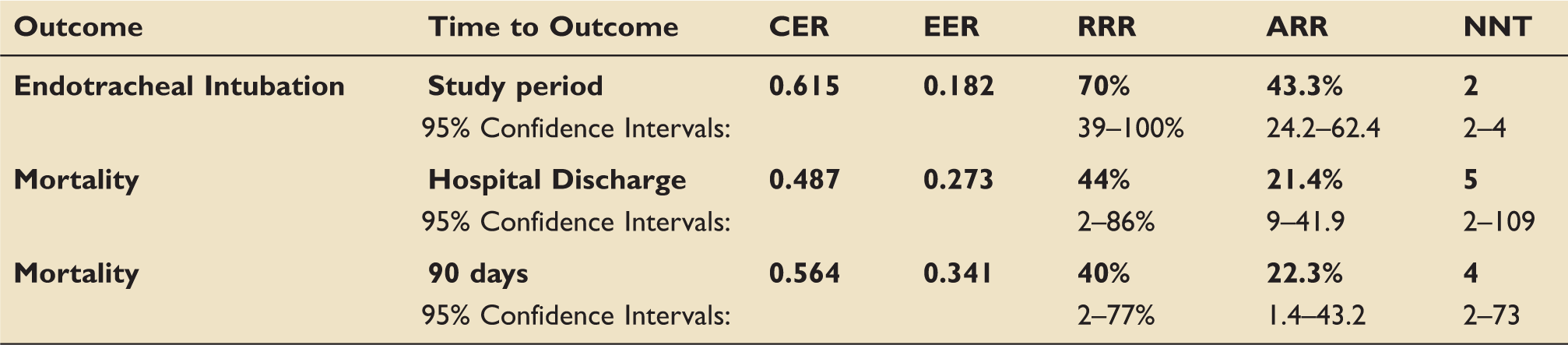
The results: (see Table 1). The two groups had very similar demographics and starting APACHE II scores. The study was stopped early by an independent data and safety monitoring board for both efficacy and safety. There was a significantly lower intubation rate in the helmet group vs. the facemask group (primary outcome, 18.2% vs. 61.5%, p < 0.001). Exploratory secondary analyses revealed that the intervention group had statistically: more ventilator-free days (28 vs. 12.5, p < 0.001); shorter ICU length of stay (4.7 days vs. 7.8 days, p = 0.04); lower hospital mortality (27.3% vs. 48.7%, p = 0.04) and lower 90-day mortality (34.1% vs. 56.4%, p = 0.02).
Outcomes.
Outcome
Time to Outcome
CER
EER
RRR
ARR
NNT
Endotracheal Intubation
Study period
0.615
0.182
70%
43.3%
2
95% Confidence Intervals:
39–100%
24.2–62.4
2–4
Mortality
Hospital Discharge
0.487
0.273
44%
21.4%
5
95% Confidence Intervals:
2–86%
9–41.9
2–109
Mortality
90 days
0.564
0.341
40%
22.3%
4
95% Confidence Intervals:
2–77%
1.4–43.2
2–73
Key: CER: control event rate (mask ventilation); EER: experimental event rate (hood ventilation); RRR: relative risk reduction; ARR: relative risk reduction; NNT: number needed to treat. Bold text and numbers relate to main data to be conveyed, normal text is data relating to statistical parameters.
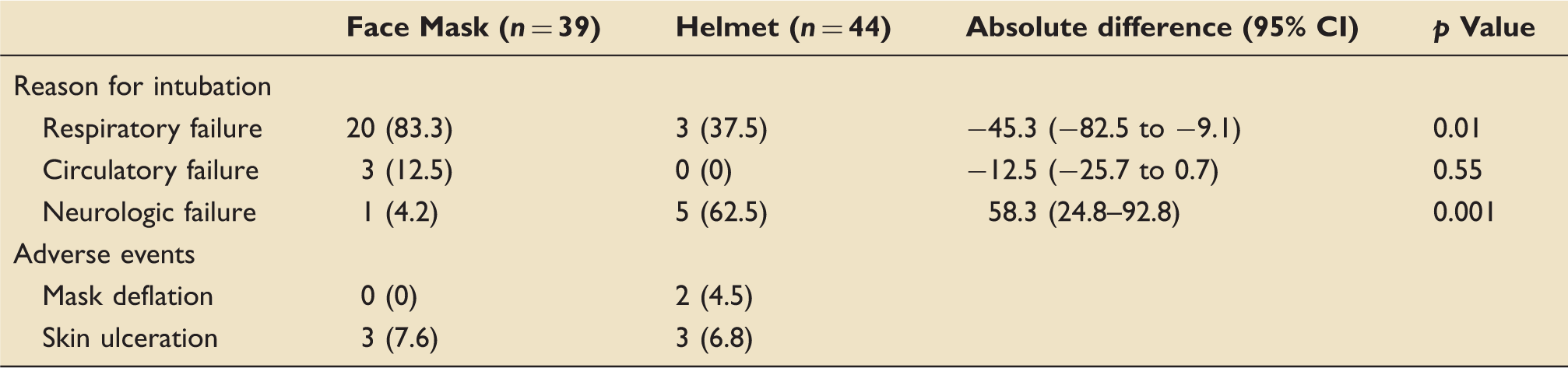
The reason for intubation differed between the two groups with neurologic failure being more common in the hood group and respiratory failure more so in the mask group (Table 2). Adverse event rates were similar.
Reasons for intubation and adverse events.
Face Mask (n = 39)
Helmet (n = 44)
Absolute difference (95% CI)
p Value
Reason for intubation
Respiratory failure
20 (83.3)
3 (37.5)
−45.3 (−82.5 to −9.1)
0.01
Circulatory failure
3 (12.5)
0 (0)
−12.5 (−25.7 to 0.7)
0.55
Neurologic failure
1 (4.2)
5 (62.5)
58.3 (24.8–92.8)
0.001
Adverse events
Mask deflation
0 (0)
2 (4.5)
Skin ulceration
3 (7.6)
3 (6.8)
EBM questions:
Do the methods allow accurate testing of the hypothesis?Yes. Although a single-centre study, all eligible patients were approached and computer randomisation used. Knowing that blinding to treatment was not possible, treatment decisions were left to the primary care team guided by predetermined protocols for titrating NIV and indications for intubation without input from the researchers.
Do the statistical tests correctly test the results to allow differentiation of statistically significant results?Yes. Appropriate statistical tests were used to compare categorical and continuous results. Aiming to detect an absolute risk reduction of 20% and assuming a baseline intubation rate of 50% resulted in 206 patients being calculated as required to power the study at 80%. A predetermined significance of p < 0.001 was set as the criteria for early study cessation for efficacy. Despite only having relatively small groups, this significance was met at first interim analysis.
Are the conclusions valid in light of the results?Yes. There was a very significant difference in intubation rate (primary outcome) between the two groups which remained when adjusted for APACHE II score. However, as discussed by the authors, the absolute difference may have been less had the trial continued to full recruitment. The control group had an intubation rate similar to that reported by Antonelli et al.,2 although higher than that reported more recently.3
Did any results get omitted and why?No. All patients who were recruited and randomised were included in the analysis with no data lost to follow-up.
Did the authors suggest areas for further research?Yes. The authors acknowledge the need for multicentre studies to determine external validation of their findings.
Did the authors make any recommendations based on the results and were they appropriate?No. Although there was a very significant reduction in intubation rate and 90-day mortality through the use of the helmet interface, the authors concluded that multicentre trials would be needed before strong recommendations could be made.
Is this study relevant to my clinical practice?Yes. ARDS is a condition associated with high intubation rates.2,3 Intubation in this patient group is associated with infectious, neurologic, respiratory and musculoskeletal complications. As a result, any intervention that can reduce the need for intubation in this patient group should be carefully considered.
What level of evidence does this study represent?2B. A randomised control trial with large confidence intervals. Also, no attempt was made at blinding, and although not possible to blind patients or primary care team, the data analysis could have been done with blinding to which group was control or intervention.
What grade of recommendation can I make based on this result alone?C. As only a single-centre study, the recommendation to use the helmet interface vs. the facemask in patients requiring longer treatment with NIV would have to be extrapolated to assume its relevance to other centres.
What grade of recommendation can I make when this study is considered alongside other available evidence?C. Further studies involving multiple centres and ideally blinding during data analysis would be needed to strengthen the recommendation. However, with high flow nasal oxygen systems showing their role in this patient group,3 it could be argued that facemask NIV should not be the control arm in any future study.
Should I change my practice based upon these results?Possibly. The very significant difference found by this study was hypothesised to be due to patients tolerating higher peak end expiratory pressures (PEEP) when using the helmet interface. Rather than converting to only using the helmet interface perhaps at this stage, it should just be added to the armoury of techniques for consideration in the management of patients admitted to the ICU with ARDS.
Should I audit my own practice based upon these results?No. Other than establishing local intubation rates for patients admitted to the ICU requiring NIV for ARDS, no clear audit standard was suggested by this study.
Footnotes
Appraised by:
Christopher WM Horner, Speciality Trainee 3, Department of Anaesthetics and Intensive Care, University Hospitals Birmingham NHS Foundation Trust, UK christopher.horner@uhb.nhs.uk
References
1.
RanieriVMRubenfeldGDThompsonBTet al.ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin Definition. JAMA2012; 307: 2526–2533.
2.
AntonelliMContiGMoroMLet al.Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: a multi-center study. Intensive Care Med2001; 27: 1718–1728.
3.
FratJPThilleAWMercatAet al.FLORALI Study Group; REVA Network. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med2015; 372: 2185–2196.