
Abstract

It is now expected that trainees in intensive care medicine will be accredited in focused intensive care echocardiography (FICE) before completing their training. At the Royal Berkshire Hospital, Reading, we have conducted three FICE courses since the introduction of FICE. We have trainees attending from around the country. Our subjective feeling was that whilst there is considerable interest in echocardiography in critical care and an initial enthusiasm, this does not always translate into full accreditation. We surveyed all attendees of our first two courses from 2013 to 2014 to assess how many had gained full accreditation and for those who had not, what (if any) had the barriers been in achieving this. Survey available to view at: www.ficesurvey.co.uk.
Our response rate to the survey was 50%. One had achieved full accreditation in the year subsequent to their course. The majority of individuals 9/15 (60%) had not progressed beyond the initial 10 supervised scans. As demonstrated in the chart below, the main barriers to progression seemed to be other time commitments of both the trainees and the trainers.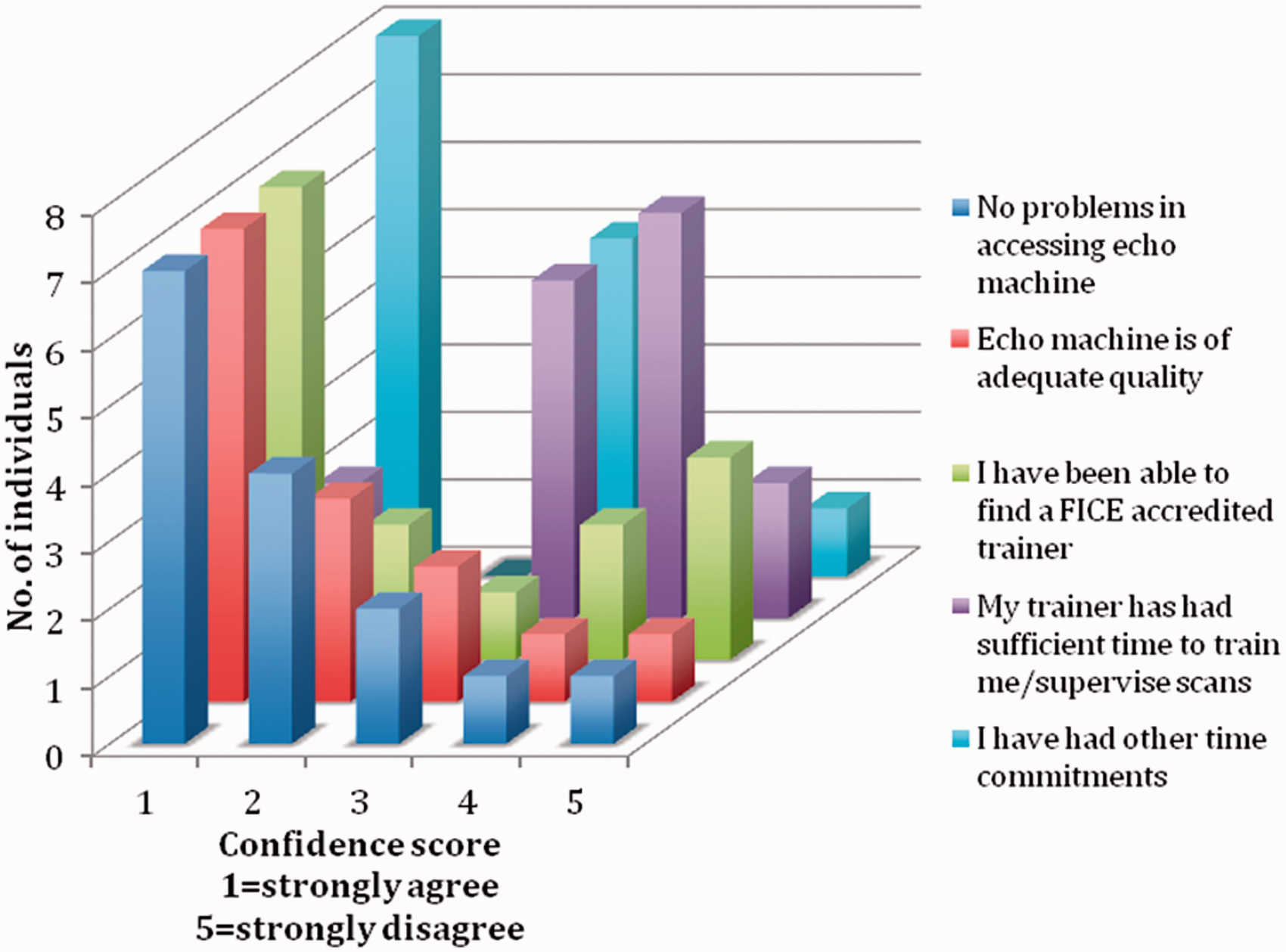
The majority of those surveyed, 71%, felt an extension in the period required to achieve the 50 scans would be desirable; 7/15 (47%) stated that despite not achieving accreditation they were using echocardiography to inform their clinical decisions of which only 4 had completed their first 10 supervised scans.
Echocardiography and ultrasound will form an integral part of the assessment of all critical care patients in the years to come. We believe that it would be beneficial to extend this survey to all FICE-registered individuals and ascertain whether our results are reflective nationally. If this is the case, then there needs to be consideration of how to modify the training programme to improve accreditation rates.
At present we think there are two problems with FICE training. Firstly, many trainees registering for FICE are not in specialist intensive care medicine training and therefore whilst they may spend a short period of time in intensive care as part of anaesthetics, medical or emergency medicine training, this is not sufficient to attain the required number of scans or supervision. At present there is lack of approved training courses in emergency echocardiography outside of intensive care medicine.
Secondly, the time period required for trainees to achieve their 50 scans could be extended. This may result in more individuals achieving accreditation allowing robust quality assurance. To prevent attrition in the rates of scans being achieved, it could be required that a certain number of scans are reached within a given time period, i.e. if accreditation could be over 24 months then it could be required that half the scans are performed by the end of the first year.
As demonstrated in our survey, once individuals can perform the investigation, some will use it to make clinical decisions, despite not having being adequately supervised and accredited which represents a significant potential risk for harm to patients. The implementation of FICE training was essential to ensure proper assessment of critically ill patients; however, maybe the time has to come to revisit the structure of the programme.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.