
Abstract

1R Out-of-hospital cardiac arrest and PCI – A single-site study from the South West of England
N Williams and R Appelboam
2R Abstract not available
3R Oesophageal sealing and aspiration via a novel nasogastric tube to prevent gastro oesophageal reflux in critically ill patients: Results from a feasibility study
B Lane, MT Gwinnutt, BD Murray and N Scawn
4R Prokinetic agents in intensive care – Where are we now?
BA Summers, BA McGrath and M Dean
5R The DAISY project: Identifying dysphagia in acute cervical spinal cord injury
J McRae
6R Using serum hepcidin to identify iron deficiency in previously critically ill patients at time of hospital discharge
A Shah, K Wray, S McKechnie, S Stanworth, R Kirkbride, D Griffith, T Walsh, H Drakesmith and N Roy
7R Abstract not available
8R Necrotising soft tissue infection: A retrospective case study
SH Chia and G Dempsey
9R Endotracheal tube colonisation and ventilator-associated pneumonia in cardiac surgery patients
E Senanayake, R Giri, S Gopal, A Nevill and H Luckraz
10R Cytochrome c oxidase: Evaluating the metabolic impact of impaired cerebral autoregulation
D Highton, C Elwell and M Smit
11R The moon, the madness, the myth? Lunar cycle and the incidence of delirium on the intensive care unit
S Berhane, C Arrowsmith, C Peters and SC Robert
12R Clinical sedation monitoring using a novel technology (Responsiveness Index): Clinical experience of patients enrolled in the DESIST clinical trial
EC Phillips, J Antonelli, K Kydonaki, T Quasim, J Ruddy, A Davidson, J Rutherford, P Peltola, MOK Särkelä, K Uutela, TS Walshand for the Development and Evaluation of Strategies to Improve Sedation practice in inTensive care (DESIST) study investigators
13R User experience of three interventions developed to improve sedation management in intensive care units: Concurrent qualitative study within the DESIST study
K Kydonaki, J Hanley, J Antonelli, TS Walshand for the Development and Evaluation of Strategies to Improve Sedation practice in inTensive care (DESIST) study investigators
14R SoundEar devices passively reduce ambient sound in critical care
NR Plummer, J Baldwin and S Laha
15R Noises in the intensive care unit
Julie L Darbyshire, Emma Jeffs, Sarah Vollam, Lisa Hinton and J Duncan Young
16R An improved classifier for mortality prediction in adult critical care admissions
A Shenfield, M Rodrigues, D Valentine, D Liu and J Moreno-Cuesta
17R A study of the impact of alcohol on admissions to a large Welsh intensive care unit
Ceri Battle, Morgan Pengelly, Karen James, Abigail Clayton and Craig Jerwood
18R Visiting in intensive care: A survey of UK units
KS Deacon, JL Mitchell and LG Mould
19R Team perceptions of risk and safety: A qualitative study of ICU staffing
D D’Lima, E Murray and S Brett
20R Abstract not available
21R A case note analysis of the reasons for early unplanned acute hospital re-admissions among adult ICU survivors
D Nassif, N Jones, E Donaghy, L Salisbury, P Ramsay, N Lone and T Walsh
22R Abstract not available
23R Direct monitoring of physical activity in critical care: Feasibility, tolerability and validity of the ActivPAL accelerometer
G Atkins, D McWilliams and C Snelson
24R Mapping physical activity in critically ill patients in a UK intensive care unit: A prospective observational service study
J Mortimore, J Rose, N Hart, S Berney and B Connolly
25R Can verbal encouragement and self-reported patient motivation predict active participation in physiotherapy on critical care?
CA Lawrence, F Lorencatto and JJ Francis
26R Abstract not available
27R Abstract not available
28R The effect of bed percussion vibration therapy on airflow in mechanically ventilated patients with severe respiratory failure
K Morris, L Osman, A Wilson and E Main
29R Mortality in critically ill non-surgical patients with pre-existing pulmonary hypertension
KB Bauchmuller, Y Arunan, R Condliffe, C Billings and GH Mills
30R Computational modelling of oxygen delivery in acute respiratory distress syndrome: Optimising positive end-expiratory pressure
M Chikhani, A Das, M Haque, W Wang, O Cole, DG Bates and JG Hardman
1R Out-of-hospital cardiac arrest and PCI – A single-site study from the South West of England
N Williams and R Appelboam
Royal Devon and Exeter NHS Trust, Exeter, UK
There is a substantial body of evidence which supports the use of immediate percutaneous coronary intervention (PCI) for patients presenting with out-of-hospital cardiac arrest (OOHCA) with return of spontaneous circulation without obvious extra cardiac cause.1–3 The evidence also demonstrates neurological status on presentation should not be used for prognostication and thus refusal of PCI on those grounds.4 Despite this, we know there is significant variation in practice with few centres mandating PCI for all comers, with lack of ST elevation on the electrocardiogram (ECG) or low Glasgow Coma Scale (GCS) commonly cited reasons for not taking patients immediately for PCI. This study looks at practice at a large district general hospital in the South West of England.
Between January 2010 and December 2014, 159 patients were referred to the intensive care unit having suffered an OOHCA and resuscitated to achieve return of spontaneous circulation. Of these patients, 17 had a clear non-cardiac cause for their arrest, and they were excluded from the remainder of the analysis. Of the remaining group, 76 (48%) had PCI on the day of presentation, with a further 22 (14%) having PCI on a subsequent day. For patients having PCI on presentation, 48% had ST elevation and 52% without. Of all patients having PCI, 47 (29%) had ‘successful’ PCI with resolution of flow past an occlusive lesion.
The in-hospital survival rate was 46% overall, with 80% of survivors discharged from hospital with a Cerebral Performance Score of 1 or 2 (capable of independent living). For patients having PCI on presentation, 55% survived, as compared with 25% who did not have PCI.
The data from our centre demonstrate a low overall rate of PCI for patients presenting with OOHCA and would seem to suggest a survival benefit for PCI on the day of presentation. We plan to use these data as a basis for further engagement of cardiology colleagues to consider PCI for all comers where there is no clear extra cardiac cause for OOHCA, irrespective of GCS or ECG on presentation.
References
2R Abstract not available
3R Oesophageal sealing and aspiration via a novel nasogastric tube to prevent gastro oesophageal reflux in critically ill patients: Results from a feasibility study
B Lane, MT Gwinnutt, BD Murray and N Scawn
Liverpool Heart and Chest Hospital, Liverpool, UK
Ventilator-associated pneumonia (VAP) is one of the most common nosocomial infections in intensive care affecting up to 28% of patients.1 Gastro oesophageal reflux plays a major role in its pathogenesis as supine positioning, nasogastric feeding and the presence of tracheal pepsin have all been demonstrated to be independent risk factors for VAP.2,3
We present the first use of a commercially available, novel nasogastric aspiration tube (Nutriseal, Israel) which aims to reduce the risk of gastro oesophageal reflux. The tube incorporates six small channels arranged in its outer wall which exit in the distal and mid oesophagus. Low-pressure suction is applied to these channels, drawing the oesophagus against the tube to create a sealing effect. In addition, any accumulated reflux contents in the oesophagus are actively aspirated from the suction ports.
Local ethics board approval was obtained. Informed consent was gained from patients, prior to cardiac and thoracic aortic surgery. The device was inserted post-operatively in 16 adult patients when nasogastric tube insertion was indicated on clinical grounds. Correct positioning of the tube was confirmed radiographically using integrated radiopaque markers. Oropharyngeal samples were obtained for pepsin assay, as a marker for reflux,3,4 prior to tube insertion and at 12 hourly intervals for the next 60 h. The Mann–Whitney U test was used to compare pepsin levels during tube use with baseline samples. Clinician and nurse questionnaires were administered to assess ease of use.
Nutriseal nasogastric aspiration tubes were inserted in 16 patients. The median length of time patients had a trial tube in situ was 5.5 days [IQR 2.7–9.4]. Sixty-five oropharyngeal aspirates were sent for assay. Insertion of the nasogastric aspiration tube resulted in a statistically significant reduction in pharyngeal pepsin levels from baseline with median values of 14 6 ng/ml [IQR 28–214] vs. 27.5 ng/ml [IQR 0–74] (p = 0.036) (Figure 1). Nursing staff and clinicians found the tubes easy to use. There were no unexpected adverse incidents attributed to use of the device.
Box plot showing median oropharyngeal pepsin levels at baseline and at 12 hourly intervals from nasogastric tube insertion. Baseline in red. Post-nasogastric tube insertion in blue boxes. Circles represent outliers.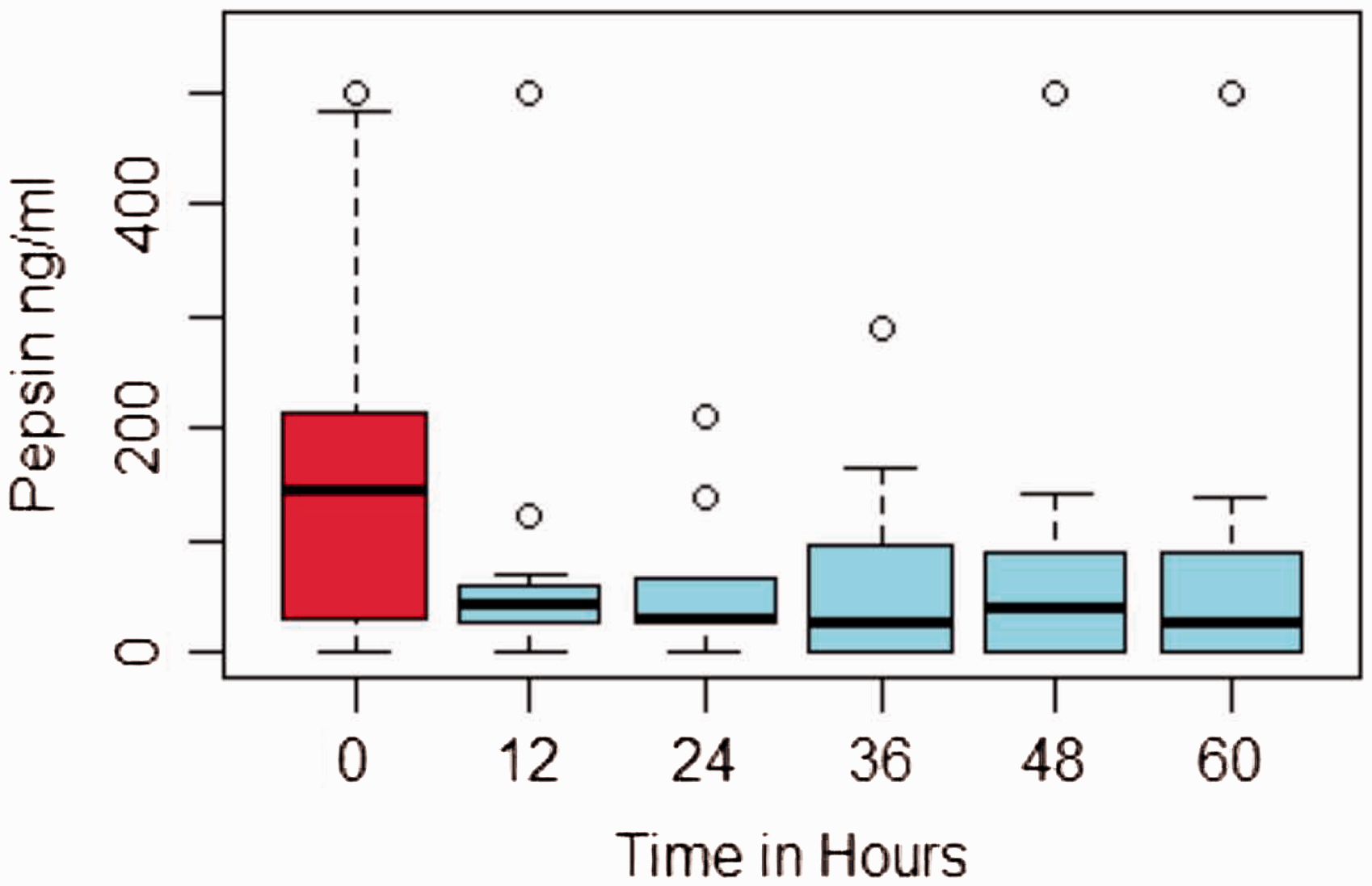
This proof of concept study shows the device is safe and easy to use in a cardiac intensive care setting. The tube significantly reduced gastro oesophageal reflux which may decrease the risk of ventilator associated pneumonia as well as offsetting the risk of enteral feeding in mechanically ventilated patients.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding and support to carry out this study was provided by Swing Medical, Tel Aviv, Israel.
References
4R Prokinetic agents in intensive care – Where are we now?
BA Summers, BA McGrath and M Dean
University of Salford, Salford, UK
Intolerance to enteral feeding in intensive care is common and can contribute to direct or indirect morbidity and mortality. The use of prokinetic agents may improve the success and tolerance of enteral feeding but practice varies widely regarding the choice of agent, route of administration and optimum co-delivery of enteral nutrition. We therefore performed a systematic review examining available evidence regarding the use of prokinetic agents to promote enteral feeding in the intensive care unit.
A search of Medline (1946–2013), Embase (1980–2013), The Cochrane Library (1898–2013) and Google Scholar was performed. Key search terms included ‘intensive care’, ‘critical care’, ‘Erythromycin’, ‘metoclopramide’, ‘prokinetic’, ‘enteral nutrition’, ‘gastrointestinal motility’ and ‘gastric emptying’. Abstracts from all clinical trials, review articles and case reports examining the effects of prokinetics on enteral feeding were reviewed. The following exclusion criteria were applied: age <16, trials using currently unavailable prokinetic agents and trials exclusively examining the placement of feeding tubes, Twenty-three remaining clinical trials were individually critically analysed in detail against an a priori checklist of defined criteria concerning study design, power and reliability of results.
Metoclopramide and erythromycin are the main agents being compared in the 13 trials prior to 2007 which concentrate on single-agent therapy. Overall, these trials conclude that prokinetics could be beneficial in patients with intolerance to enteral feeding, increasing gastric motility as shown by increased levels of paracetamol absorption or reduced gastric residual volumes.
Since 2007, four trials have examined combination therapy as well as single-agent therapy. As a single agent, erythromycin was significantly more efficacious showing reduction in gastric residual volumes whereas the greatest overall benefit was seen using combination.–4 The issue of tachyphylaxis is evident with significant reduction in benefit after approximately 48 h of therapy. However, overall evidence is limited; studies with the strongest design lack power, and, conversely, well-powered studies lack reliability in their design such as lack of blinding. Due to the heterogeneity of the methods and outcomes, meta-analysis is not feasible. The lack of clinical outcomes such as mortality or length of stay is another limitation when interpreting the benefit of prokinetics in intensive care.
Despite limitations, available evidence suggests intravenous metoclopramide and erythromycin both individually increase tolerance to enteral feed. The greatest effect is seen when these agents are used synergistically for up to 48 h, after which tachyphylaxis reduces their efficacy. Further studies into clinically relevant outcomes such as mortality and length of stay are required before stronger recommendations can be made.
References
5R The DAISY project: Identifying dysphagia in acute cervical spinal cord injury
J McRae
London and London Spinal Cord Injury Centre, University College, Stanmore, UK
Acute cervical spinal cord injury patients (CSCI) are primarily admitted to major trauma centres (MTC) whilst awaiting transfer to specialist spinal injury units (SIU). Delays identified by the Spinal Injuries Association1 are due to limited respiratory beds, leaving admitting intensive care units (ICU) to commence ventilatory support and plan cervical spine surgery, known to cause laryngeal impairment. Dysphagia incidence is around 40%2 with silent aspiration impacting on respiratory function and associated with increased mortality and morbidity.3 Allied Heath Professionals (AHP) are often involved to manage ventilator weaning, feeding and resolve swallowing problems.
The aim of this study is to investigate the clinical decisions made by team members in different ICU settings that admit CSCI patients.
An online survey comprising of 35 multiple-choice questions covering five topics: tracheostomy and ventilator weaning, nutrition, swallowing, mouthcare and communication was distributed through critical care networks and professional bodies to doctors, nurses, dietitians, physiotherapist and speech and language therapists (SLT). Biographical information was collected on profession, type and size of hospital ICU.
Responses were received from 219 professionals from 87 UK hospitals. Nearly a third were doctors, another third were nurses with AHP responses from physiotherapists (16.3%), SLTs (13.9%) and dietitians (4.8%).
Respondents were based in MTC (32.9%), District General Hospitals (DGH) (26.9%), Teaching Hospitals (14.2%) and 7.8% worked in a MTC with a SIU on-site. The majority (69.4%) worked in large hospitals with over 500 beds and 60.6% in ICU’s with over 10 beds. 85.4% reported that their unit admitted SCI patients.
National ventilator weaning protocols were developed4 to ensure a safe and effective weaning transition for those with CSCI; however, 42.1% reported using a locally agreed protocol. Measures of vital capacity were used more by SIU staff (90.5%) than MTC staff (49.3%) and SIU routinely capped off the tracheostomy (76.2%) compared to MTC (16.4%) and DGH (21.9%).
With regard to tracheostomy care, 57.7% of respondents considered a cuff prevented aspiration of secretions and 12.1% thought that this allowed safe oral intake. Eating with the cuff up happened ‘sometimes’ by 52.9% of staff at MTC, compared to 40% SIU and 60% DGH.
Enteral feeding commenced only after failure to take adequate oral intake (82.6%) or prolonged intubation (50.7%). Gastrostomy tube was considered after ongoing swallowing problems (75%) or recommendation by SLT (63.2%). SLT (86.8%) and nurses (54.2%) most commonly screened for swallowing problems and 41.5% of staff used a blue dye test.
Coughing (95.1%) was almost universally accepted as a sign of dysphagia, followed by food from tracheostomy (91.5%) and aspiration pneumonia (89.4%). With 90.4% using bedside swallow assessment and only 37.8% using flexible nasendoscopy, this may explain why silent aspiration is missed.
In summary, a wide range of clinical decisions are made by staff in the respiratory and feeding management of CSCI patients. This affects length of stay resulting in complications. A structured protocol is proposed, ensuring consistent screening and interventions, with education and support from Spinal Outreach Teams.
References
6R Using serum hepcidin to identify iron deficiency in previously critically ill patients at time of hospital discharge
A Shah1, K Wray2, S McKechnie1, S Stanworth3, R Kirkbride4, D Griffith5,6, T Walsh5,6, H Drakesmith2 and N Roy2
1Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, Oxford, UK
2Weatherall Institute of Molecular Medicine, John Radcliffe Hospital, Oxford, UK
3NHS Blood & Transplant, Oxford, UK
4Royal Infirmary of Edinburgh, NHS Lothian, Edinburgh, UK
5Centre for Inflammation Research, University of Edinburgh, Edinburgh, UK
6Department of Anaesthesia, Critical Care and Pain Medicine, University of Edinburgh, Edinburgh, UK
Anaemia during critical illness is multifactorial and well studied. There is less data on anaemia during the recovery phase of critical illness and its relation to long-term outcomes.1 Iron deficiency is the largest and treatable cause of anaemia worldwide, but in intensive care (ICU), diagnosis of iron depletion is complicated by concomitant inflammation, which raises serum ferritin, the commonest estimate for iron status. Hepcidin has emerged as a key regulator of iron metabolism. Its expression is increased in states of inflammation and iron overload and repressed in iron deficiency, hypoxia and erythroid expansion.2,3
Our aims were:
To identify the proportion of patients discharged from ICU who remain anaemic at, or close to, hospital discharge; To identify the proportion of anaemic patients with iron deficiency anaemia (IDA), anaemia of inflammation (AID) and combined anaemia of inflammation and iron deficiency (IDI); and To investigate if serum hepcidin values are significantly lower in the IDI group compared to the AID group.
Anaemia was defined according to World Health Organization guidelines: males <130 g·L−1 and females <120 g·L−1. In the presence of inflammation (C-reactive protein (CRP) >8 mg·L−1), a ferritin cut-off of 150 µg·L−1 was used to differentiate between IDI (<150) and AID (>150).3 Serum samples collected as part of RECOVER, a multicenter randomised controlled trial assessing the effects of a complex rehabilitation intervention after ICU discharge on patient outcomes, were analysed.4 We assayed serum hepcidin, soluble transferrin receptor, CRP, ferritin and other markers of iron status. Statistical significance was defined as p < 0.05.
In sum, 117 patient samples were analysed. Proportions of different types of anaemia are shown in Figure 1. Mean (SD) sample collection day was 4.6 (6.08) days prior to hospital discharge and 18.5 (18.5) days post-ICU discharge; 110/117 (94%) patients were anaemic prior to hospital discharge. Overall, 89/117 (76%) had an AID and 11/117 (9%) had IDI based on our pre-defined criteria. Geometric mean (95% CI) hepcidin levels were significantly lower in the IDI group compared to the AID group: 9.13 (3.57–23.3) ng mL−1 vs. 28.6 (24.8–33.1) ng mL−1 (p < 0.05). Using area under the curve for receiver operator characteristic (AUCROC) curves for our diagnosis of IDI, hepcidin <8 ng mL−1 had a sensitivity of 36.3% and a specificity of 95.8%, while hepcidin of <19 ng mL−1 had a sensitivity of 72.7% and a specificity of 71.7% with an AUCROC of 0.722.
Flow of classification of different types of anaemia classified by haemoglobin, CRP and ferritin cut-offs.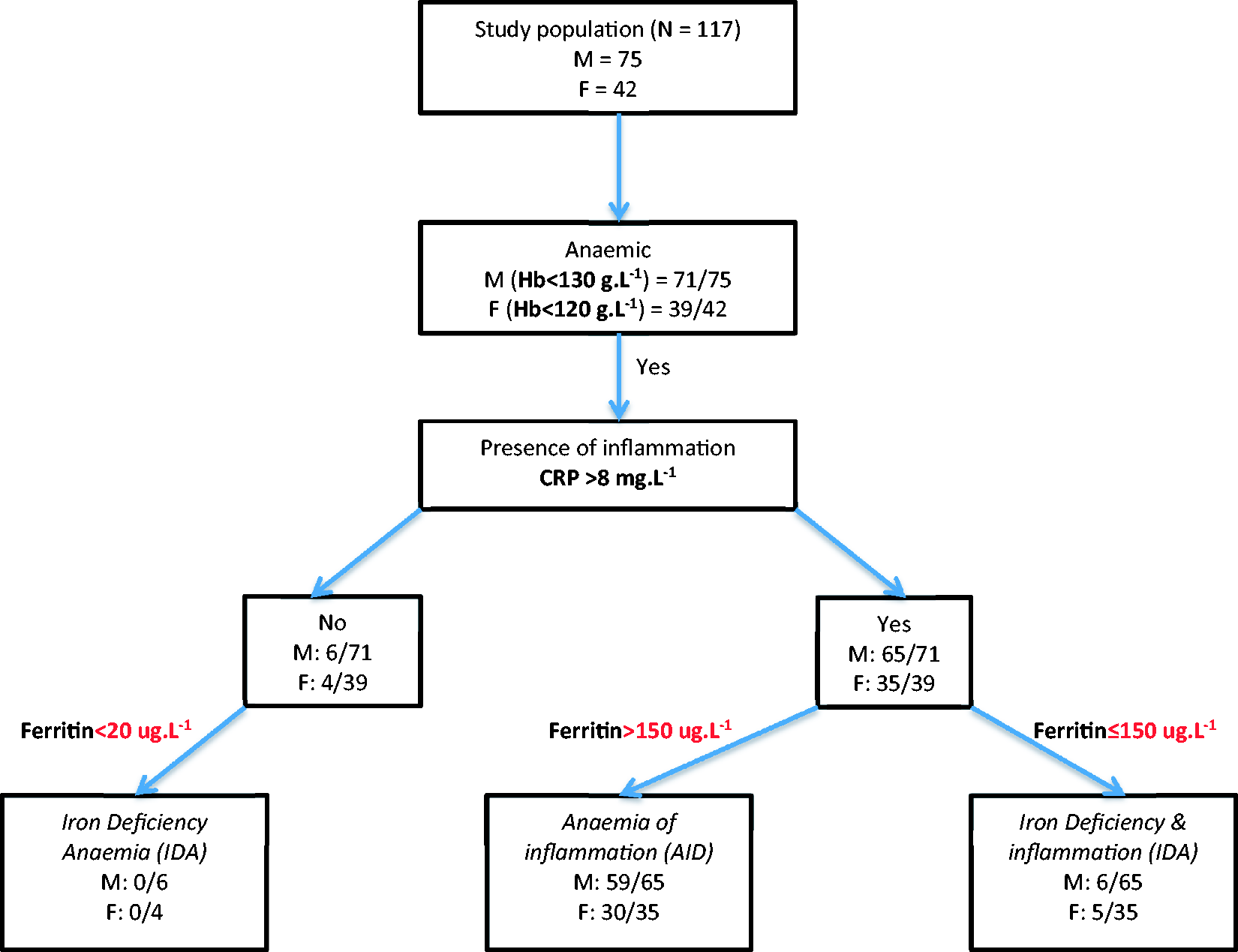
The majority of patients discharged from ICU, and subsequently hospital, have an AID and a small proportion develop IDI based on current available tests. We have shown that serum hepcidin is a promising diagnostic test of iron deficiency in the context of inflammation. However, the hepcidin levels are elevated to a point where, based on previous studies, patients would not be expected to respond to oral iron.2,5 Prospective studies are therefore needed to further understand hepcidin regulation during the acute and recovery phases of critical illness, to assess if intravenous iron may be beneficial in treating anaemic patients recovering from critical illness, and determine if serum hepcidin levels could identify those most likely to respond to this therapy.
Author Note
H Drakesmith and N Roy contributed equally to this work.
References
7R Abstract not available
8R Necrotising soft tissue infection: A retrospective case study
SH Chia and G Dempsey
Intensive Care Unit, Aintree University Hospital, Liverpool, UK
Patient characteristics: Survivors to hospital discharge versus non-survivors.
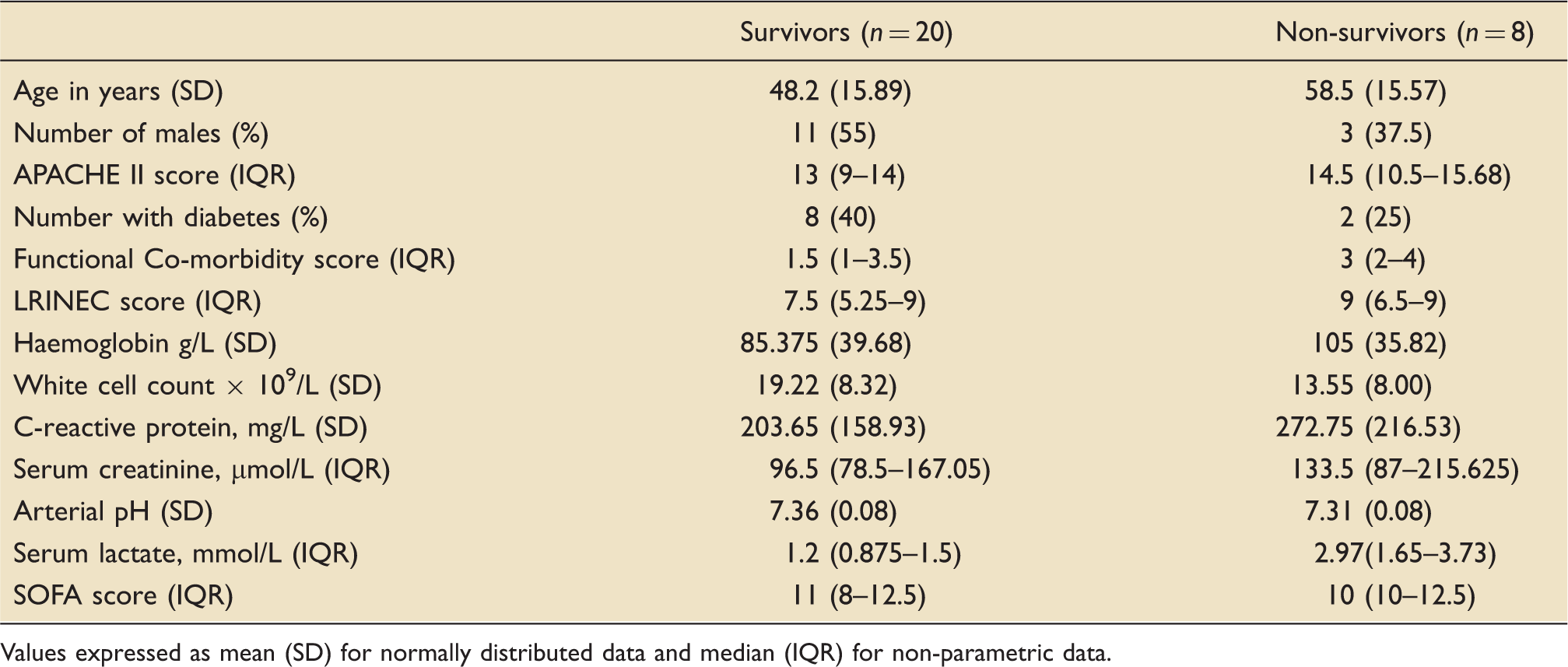
Values expressed as mean (SD) for normally distributed data and median (IQR) for non-parametric data.
In this cohort, the serum lactate in non survivors was higher and found to be statistically significant at 2.97 (p = 0.048, Mann–Whitney U test).
References
9R Endotracheal tube colonisation and ventilator-associated pneumonia in cardiac surgery patients
E Senanayake1, R Giri2, S Gopal3, A Nevill4 and H Luckraz1
1Cardiothoracic Surgery, Heart & Lung Centre, Wolverhampton, UK
2Cardiothoracic Anaesthesiology, Heart & Lung Centre, Wolverhampton, UK
3Intensive Care, Heart & Lung Centre, Wolverhampton, UK
4University of Wolverhampton, UK
Mean (95%CI) bacterial colony forming units (CFU) cultured from distal inner lumen of endotracheal tubes.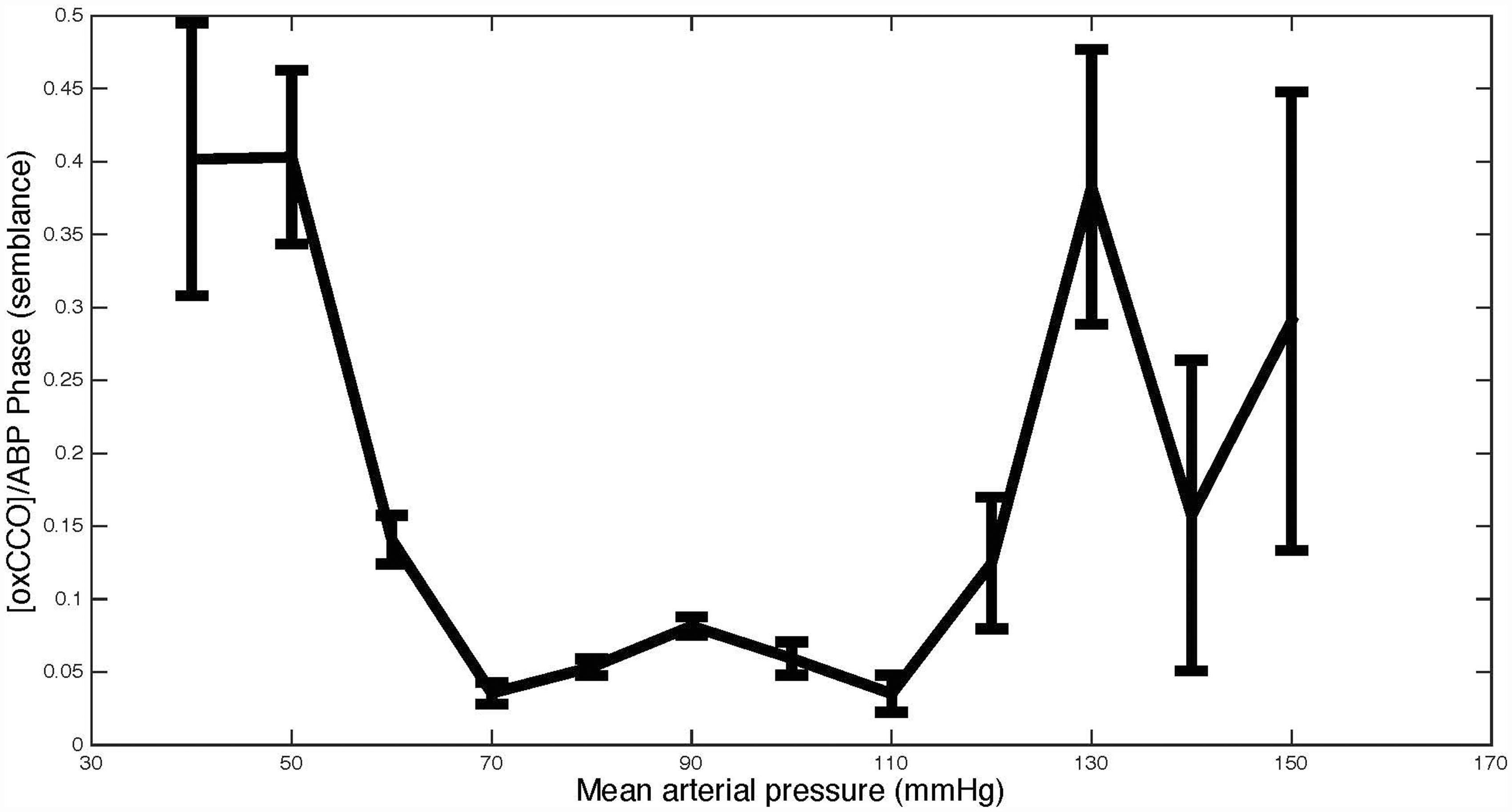
References
10R Cytochrome c oxidase: Evaluating the metabolic impact of impaired cerebral autoregulation
D Highton1, C Elwell2 and M Smit1,2
1Neurocritical Care, National Hospital for Neurology and Neurosurgery, London, UK
2Department of Medical Physics & Bioengineering, University College London, London, UK
Acute brain injury is associated with impaired cerebral autoregulation (CA). Continuous beside CA indices have been proposed as an adjunct to therapy. The mean velocity index (Mx) is an extensively validated index derived from correlation between transcranial Doppler flow velocity in the middle cerebral artery (TCD) and arterial blood pressure (ABP).1 Near-infrared spectroscopy (NIRS) is a non-invasive optical technique which can measure cerebral oxy/deoxy-haemoglobin and form the basis of Mx-style indices. Using a highly optimised in-house spectroscopy system a metabolic marker, the oxidation status of cytochrome c oxidase (oxCCO) – the terminal electron acceptor in the mitochondrial respiratory chain can be measured.2 The aim of this work is to measure the impact of impaired CA on [oxCCO]. We hypothesise that failure of CA will render [oxCCO] pressure passive potentially indicating flow-limited metabolism.
Following ethical approval and consent, patients with acute brain injury were recruited. Monitoring included TCD and broadband NIRS.2 CA indices were derived as previously described1 using a moving Pearson correlation coefficient: Mx (TCD, ABP), TOx (NIRS tissue oxygen saturation, ABP) and THx (NIRS total haemoglobin, ABP). A value >0.3 suggests impaired CA. [oxCCO] was analysed with respect to ABP using a wavelet measure of phase (semblance) between 0.1 Hz and 0.01 Hz. The Mx was compared using Pearson correlation.
Thirty-six patients were recruited (subarachnoid haemorrhage 21, traumatic brain injury 1 and intracranial haemorrhage 14). Mx correlated with [oxCCO]/ABP phase r = 0.34 p = 0.04, TOx r = 0.45 p < 0.01 and THx 0.40 p = 0.02. The figure illustrates the relationship between mean ABP and [oxCCO]/ABP phase. This suggests that ABP outside a well-defined ‘plateau’ region affects [oxCCO].
Our data suggest that impaired autoregulation is associated with pressure passive changes in [oxCCO]. This might reflect changes in mitochondrial oxygen delivery or its utilisation. Although further work is required to confirm these findings, [oxCCO] has considerable theoretical advantages over other methods of investigating the effects of CA as it reflects a metabolic endpoint.
Blood pressure thresholds for cytochrome c oxidation status (error bars, standard error mean).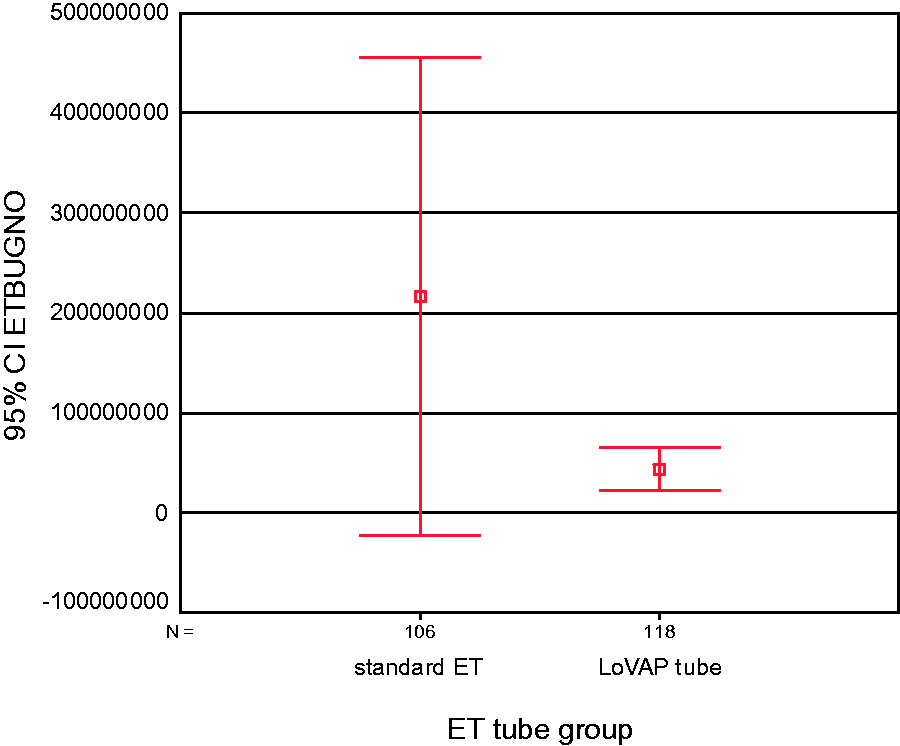
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EPSRC Grant (EP/K020315/1).
References
11R The moon, the madness, the myth? Lunar cycle and the incidence of delirium on the intensive care unit
S Berhane1, C Arrowsmith2, C Peters3 and SC Robert4
1Homerton University Hospital, London, England
2Emergency Medicine, Homerton University Hospital, London, England
3Intensive Care Medicine and Anaesthesia, Homerton University Hospital, London, England
4Intensive Care and Acute Medicine, Homerton University Hospital, London, England
Many health professionals believe that the lunar cycle has an effect on the incidence of psychiatric presentations to hospitals.1,2 Research has shown that the circalunar cycle can influence the subjective and objective quality of sleep3 and the incidence of psychiatric symptoms.4 However, more robust research largely involving emergency psychiatric presentations have failed to find any correlation.5 Thus far there has been no consistent association between lunar cycle and psychopathology. There have been no studies investigating whether circalunar rhythm has any effect on delirium (or psychiatric morbidity in general) in intensive care patients. The aim of this study was to examine whether there was any correlation between the incidence of delirium and the full moon.
The study was conducted over six months (January–June 2015) in an 11-bedded general intensive care unit. Data were collected using the three-day model, meaning that data were collected on the day of the full moon and new moon of each month and 24 h before and after that date (three days in total). In total, data over four new moon and four full moon cycles were collected. Delirium was assessed twice a day using the validated Confusion Assessment Method – Intensive Care (CAM-ICU). Patients who were too sedated to be assessed by CAM-ICU were excluded (65 patients in total) as were patients whose CAM-ICU score was not clearly documented (7).
Overall, 92 patients were included (54 during new moon and 38 during full moon). Background characteristics and interventions known to increase the risk of delirium were also collected. There was no significant difference in the baseline characteristics including mean age between the new moon and full moon group (58.6 vs. 58.8, respectively), gender (70% male vs. 71% male), Acute Physiology and Chronic Health Evaluation (APACHE) II scores (11 vs. 9) and pre-existing psychiatric history (31% vs. 26%). Sedative and psychotropic drugs used in the two groups were similar apart from the fact that patients in the full moon group received more benzodiazepines (0% vs. 10%) and more haloperidol (0% vs. 12%); however, there was no independent association between full moon and increased sedation overall.
There was no statistically significant independent association between the incidence of delirium during the new moon (CAM-ICU positive 20%) and the full moon group (CAM-ICU positive 14%). However, this was a relatively small study that was powered to detect only a large difference between the incidence of delirium at different stages of the lunar cycle. Our results are in keeping with larger studies outside of the intensive care setting reporting no association between the full moon and increased psychopathology.
In conclusion, our study found no association between the incidence of delirium and the full moon in intensive care patients. We hypothesise that the reason for the persistence of the belief that the full moon is associated with increased psychiatric morbidity is confirmation bias. This may explain why our patients received more sedative drugs during the full moon when compared to the new moon nights. Larger studies would be required to confirm these results.
References
12R Clinical sedation monitoring using a novel technology (Responsiveness Index): Clinical experience of patients enrolled in the DESIST clinical trial
EC Phillips1, J Antonelli1, K Kydonaki1, T Quasim2, J Ruddy3, A Davidson4, J Rutherford5, P Peltola6, MOK Särkelä6, K Uutela6, TS Walsh1 and for the Development and Evaluation of Strategies to Improve Sedation practice in inTensive care (DESIST) study investigators
1Anaesthetics, Critical Care and Pain Medicine, University of Edinburgh, Edinburgh, Scotland
2University Department of Anaesthetics, Glasgow University, Glasgow Royal Infirmary, Glasgow, Scotland
3Department of Anaesthetics, Monklands Hospital, NHS Lanarkshire, Scotland
4Department of Anaesthetics, Victoria Infirmary, NHS GGC, Glasgow, Scotland
5Department of Anaesthetics, Dumfries Hospital, NHS Dumfries and Galloway, Scotland
6GE Healthcare Finland Oy, Helsinki, Finland
Sedation strategies primarily aim to avoid over-sedation in intensive care units (ICUs), which is associated with adverse outcomes.1 We recently described a novel technology for continuously alerting bedside staff that deep sedation may be present – the Responsiveness Index (RI).2,3 RI uses facial electromyography to track patient arousals and was one of the quality improvement interventions used in the recently completed DESIST clinical trial (ClinicalTrials.gov NCT016344514). We describe the use of RI monitoring observed in the trial; this was the first use in routine clinical practice.
Four ICUs used RI monitoring, which was started following consent. Monitoring use was encouraged until patients were awake and/or extubated. Continuous RI data were presented as numeric values and traffic light colours: RI score 0–20, RED (high risk of deep sedation); 21–40, amber (intermediate risk); and 41–100, green (low risk). Following training, nurses were encouraged to reduce sedation in response to a red RI and aim for green RI values, but this was not linked to strict protocols.
Two-hundred and six patients received RI monitoring (range 26–90 across ICUs). RI data were not analysed for nine patients (six received neuromuscular paralysis, two advanced ventilator modes and one no data recorded); 197 patients’ data were analysed. The median (1st, 3rd quartile; min–max) time between intubation and starting monitoring was 21 h (11, 34; 0–103) and median duration of monitoring was 66 h (27, 139; 1–925). Monitoring continued until extubation in 32% of ICU survivors. The first RI recorded was red 59% (range 50–66% across ICUs), amber 12% (range 4–17%) and green 28% (range 25–38%). Among patients whose first RI was red, 16% never had a green RI; 68% of these were ICU non-survivors. For patients whose RI values did increase to the green range, the median time to first green RI was 9 h (4, 23; 1–103). Among all patients, the RI value was red for 35% of monitoring time (range 23–48% across ICUs), amber for 13% (range 11–13%) and green for 35% (range 30–42%). No RI data were recorded for a median 17% of monitoring time (range 8–29% across ICUs). The median longest recorded time with continuous red RI values was 7 h (3, 14; 0–69) and 70% of patients had ≥1 period of ≥4 h of sequential red RI values; sedatives were administered for 93% of these episodes. Among the patients in whom monitoring continued until extubation, the last recorded RI was red 10%, amber 17%, and green 74%. ICU non-survivors tended to have a higher prevalence of red RI values.
In this first description of RI monitoring during routine critical care, we found a high prevalence of red RI values consistent with deep sedation, despite encouraging nurses to adjust sedation to achieve higher RI values. The reasons for this are uncertain but could indicate a failure to fully use the RI technology as intended despite training and education. Our data suggest the technology has potential to reduce deep sedation, but further training and possibly a protocolised approach may be needed to maximise impact on clinical outcomes.
References
13R User experience of three interventions developed to improve sedation management in intensive care units: Concurrent qualitative study within the DESIST study
K Kydonaki1, J Hanley2, J Antonelli1, TS Walsh1 and for the Development and Evaluation of Strategies to Improve Sedation practice in inTensive care (DESIST) study investigators
1Anaesthetics, Critical Care and Pain Medicine, University of Edinburgh, Edinburgh, UK
2Research and Development Management, NHS Lothian, The Queens Medical Research Institute, Edinburgh, UK
Optimising sedation practice is part of patient-safety care bundles but is difficult to implement.1 Sub-optimum intensive care unit (ICU) sedation-analgesia management worsens patient outcomes and safety.2,3 The DESIST study developed novel ICU sedation-quality indicators and introduced and evaluated three interventions designed to improve sedation practice (ClinicalTrials.gov NCT01634451).3 In a cluster-randomised design, we randomised pairs of eight Scottish ICUs to four different combinations of these interventions, namely (a) enhanced education alone (2 ICUs), (b) education plus regular sedation quality feedback using process control methodology (2 ICUs), (c) education plus a novel sedation monitoring technology (Responsiveness Index (RI); (2 ICUs))4,5 and (d) all three interventions (2 ICUs). We collected pre- and post-intervention sedation-quality data for 90 weeks in all ICUs (45 weeks for each phase). We used action research for process evaluation of the intervention phase. We report here the experiences of ICU staff on the implementation and use of the three interventions.
An action research design was used. During implementation and intervention phases, one trained researcher (KK) used participant observation in each ICU in three distinct timelines to understand the uptake of interventions and subsequent changes in practice: beginning of intervention phase, midway of intervention phase and the end of intervention phase. We also conducted multi-professional focus groups in the final month of the intervention phase, in which participants reflected on intervention(s) uptake and the resultant changes to sedation practice. Field notes and transcripts were verbatim transcribed and entered in NVivo 10 software for qualitative analysis (QSR International, Ltd). An inductive comparative thematic analysis was conducted without a pre-defined theoretical framework to allow the in-depth exploration and understanding of the impact of interventions on sedation management. Data were compared by combination of interventions.
Among the three interventions, clinicians showed more preference towards the education package and the RI monitor and less towards the process feedback measures. The education package was informative and raised awareness of the various aspects of sedation management but was time consuming. The RI monitor was used as a prompt tool to consider deep sedation, but there was lack of understanding of the philosophy of the device (despite a training programme). The process measures stimulated some discussion about sedation practice but were considered difficult to understand and unreliable to stimulate a change of practice. At individual clinician level, raising awareness increased nurses’ autonomy in decision making. Changes in clinical practice that staff considered were the introduction or replacement of new assessment tools for pain, delirium and sedation level; reviewing the timing of the sedation hold; considering sleep promotion and pain management initiatives; introducing algorithms for delirium and agitation. Changes in the routine staff communication processes were taken into account to maintain consistency and provide clear guidance in decision making.
In conclusion, clinicians in all eight ICUs showed preference to interventions that were more approachable and meaningful to their daily clinical practice. The impact of the education and RI monitoring interventions seemed most relevant to the needs and current gaps in sedation practice.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Chief Scientist Office (CSO grant ref number: CSO/3/3), Scotland. The study was co-supported by GE Healthcare as part of the original application. GE Healthcare provided £200K of unrestricted support (through Edinburgh University) and also supplied the Responsiveness monitors and associated disposables used in the study.
References
14R SoundEar devices passively reduce ambient sound in critical care
NR Plummer, J Baldwin and S Laha
Critical Care Unit, Lancashire Teaching Hospitals NHS Foundation Trust, Preston, UK
Histogram of background sound levels before (blue) and after (green) the SoundEar III device’s visual sound warnings were turned on.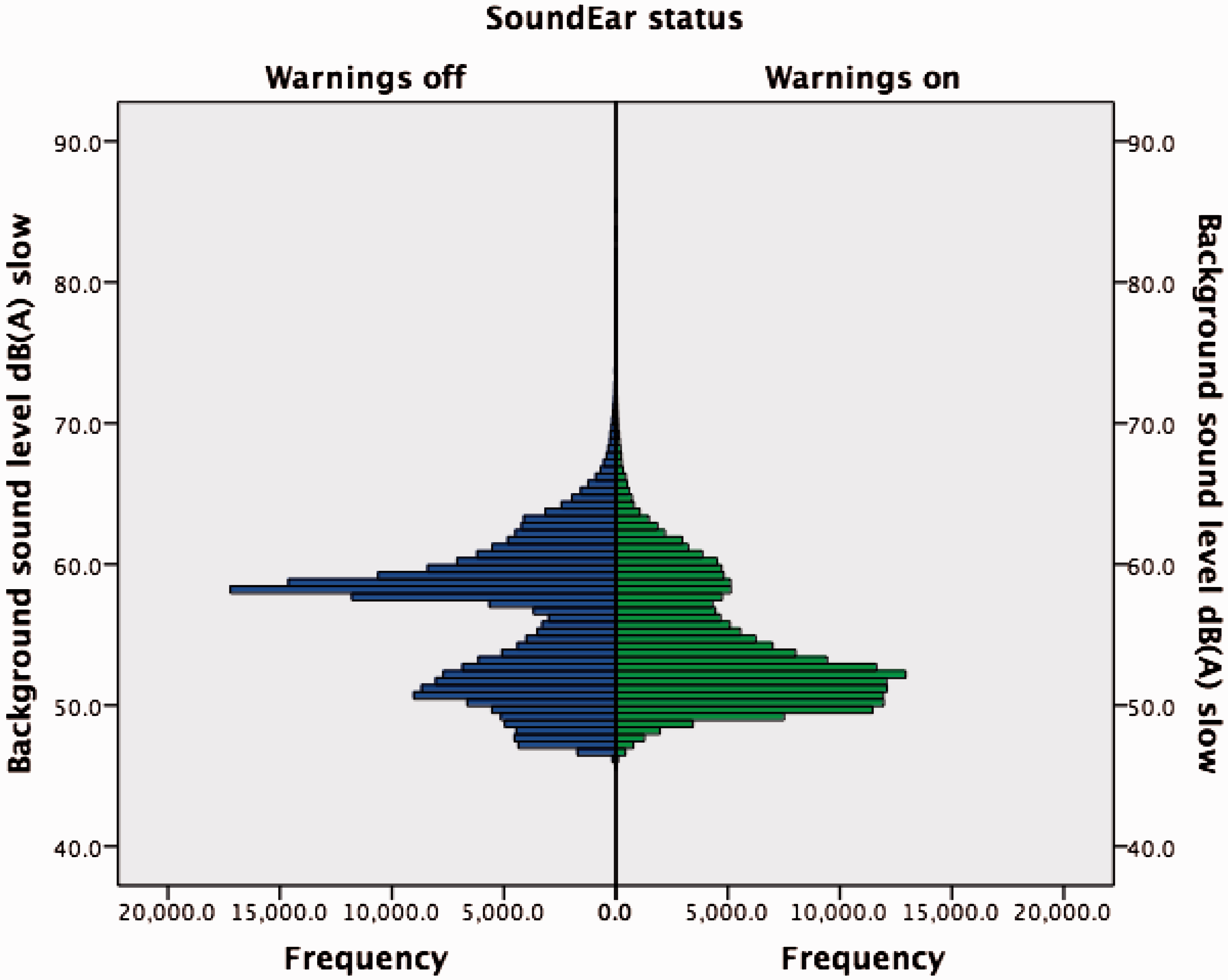
Acknowledgements
Registered with Lancashire Teaching Hospitals NHS Foundation Trust Department of Research and Innovation. Ethical approval was waived. SoundEar III devices were provided free of charge by SoundEar A/S (Birkerød, Denmark), with explicit agreement to publish results regardless of positive or negative findings.
References
15R Noises in the intensive care unit
Julie L Darbyshire1, Emma Jeffs1, Sarah Vollam1, Lisa Hinton2 and J Duncan Young1,2
1Nuffield Department of Clinical Neurosciences, University of Oxford University, Oxford, UK
2Health Experiences Research Group, University of Oxford, Oxford, UK
3Adult Intensive Care Unit, Oxford University Hospitals NHS Trust, Oxford, UK
Noise levels in intensive care units (ICUs) are about as loud as the dining room of a busy restaurant.1 This high background noise is likely to contribute to abnormal sleep and increase the incidence of ICU-acquired delirium. Patients who suffer from delirium in hospital have longer stays and more health problems after they return home.2 Disrupted sleep is common in the ICU and may be associated with delirium.3
The SILENCE portfolio of studies aims to identify the major sources of noise in the intensive care unit, confirm viable measures for sleep and delirium and implement a feasible noise reduction strategy that can be formally tested in a future large-scale randomised controlled trial.
For this noise identification study, two qualitative researchers independently conducted observations in four ICUs in the Oxford University Hospital NHS Trust. Observation sessions lasted from 2 to 12 h and were completed during the day and overnight, both during the week and at weekends. Sound pressure levels (SPL) were recorded using portable sound level monitors which were calibrated before and after use.
A total of 35 h of observations were completed in the two general adult ICUs with shorter comparison sessions in the neonatal unit (6 h) and adult neuro-ICU (3 h). Activity, particularly at staff handover periods and when preparing patients for transfer, and alarms were identified as the primary sources of noise. Several occurrences of ‘alarm blindness’ were witnessed. Supportive infrastructure in the neonatal unit has been introduced as a response to the potentially damaging effects of noise. Illuminated signs are in use and privacy screens encourage foot traffic away from the patient cots.
Where lighting levels were higher overnight, it was also noticeably louder. Most visitors were quiet but some seemed to have poor health literacy and were disruptive. Staff chat was predominantly focused on patient care but not exclusively. Where staff had formed friendships, it was more likely that colleagues would silence alarms for patients other than their own.
Concurrent SPL monitoring confirmed that levels are still much higher than the World Health Organization recommended limit of 30 dBA. Subjective reflection on the environmental noise levels at times contradicted the objective SPL measure.
Noise levels in the ICU remain elevated. Much of the noise is generated from alarms which are not silenced, and general activity. Alerting signs raise awareness of noise but do not achieve a lower SPL. Post-observation discussion with staff and patients has led to the development of an alarms management policy and the introduction of simple environmental changes such as switching metal bins for plastic. We are also developing new teaching materials designed to raise awareness of the effects of noise. Additional suggestions for future work included re-assessment of night-time illumination practices, integrated alarm systems, noise cancellation and concentrated care areas.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The National Institute for Health Research ‘Research for Patient Benefit’ programme funds the SILENCE research project at the University of Oxford and Oxford University Hospitals NHS Trust.
References
16R An improved classifier for mortality prediction in adult critical care admissions
A Shenfield1, M Rodrigues1, D Valentine2, D Liu2 and J Moreno-Cuesta2
1Sheffield Hallam University, Sheffield, UK
2North Middlesex University Hospital, London, UK
ROC Curves with Pointwise Confidence Bounds.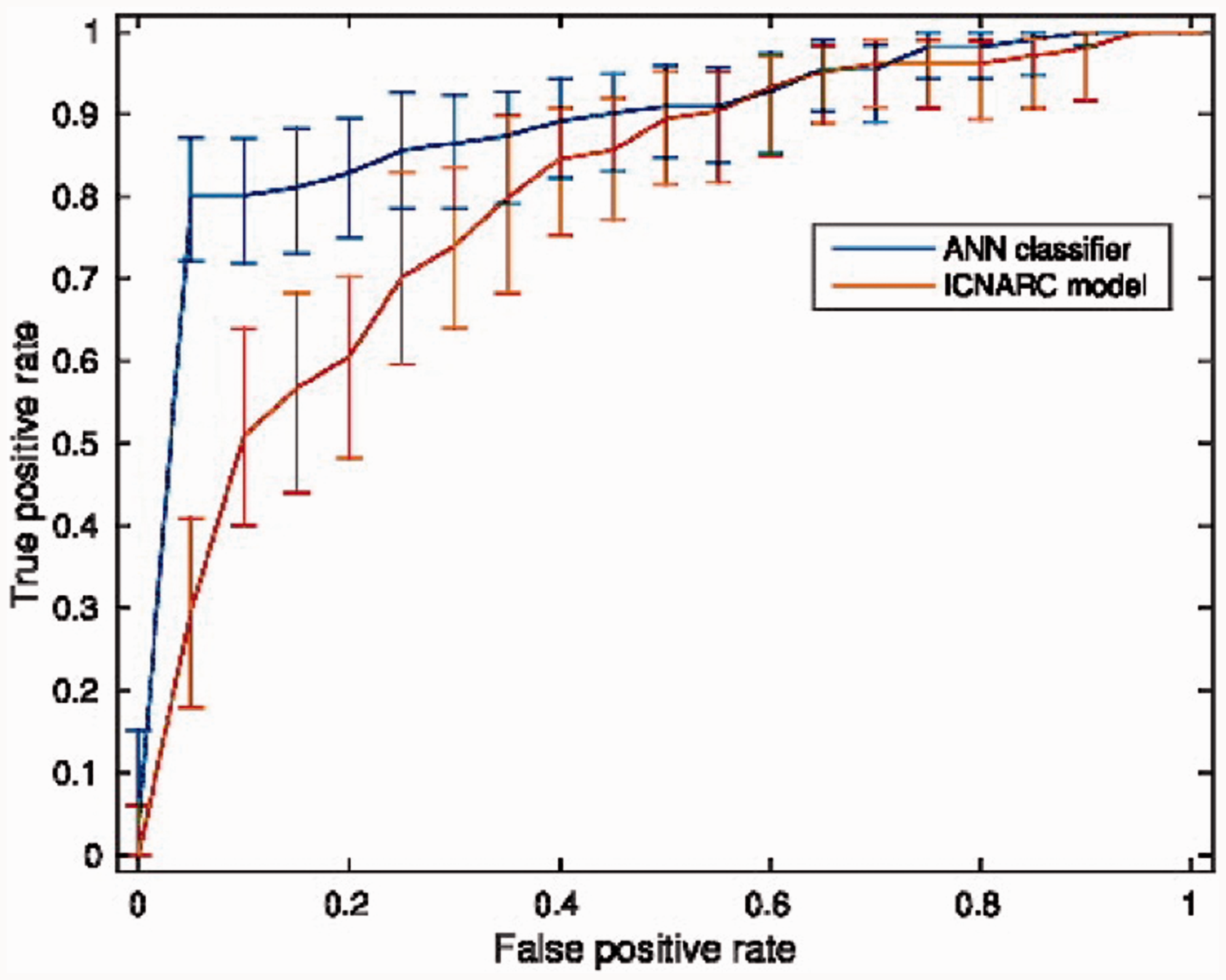
Reference
17R A study of the impact of alcohol on admissions to a large Welsh intensive care unit
Ceri Battle1, Morgan Pengelly2, Karen James1, Abigail Clayton1 and Craig Jerwood1
1Critical Care Unit, Morriston Hospital, Swansea, UK
2College of Medicine, University of Otago, Otago, New Zealand
The harmful use of alcohol has led to 3.3 million deaths each year worldwide, which represents 5.9% of all deaths.1 Alcohol-related deaths rates were significantly higher in Wales than in England in 2012, with 18.0 compared to 14.7 per 100,000, respectively.2 Social deprivation is reported to influence alcohol-related mortality. The alcohol-related mortality rate in the most deprived communities of Wales was 22.0 per 100,000 in 2002–2006, more than three times higher than the least deprived areas.3 We undertook a prospective evaluation of the impact of alcohol-attributable admissions to an intensive care unit (ICU) in a major tertiary centre in Wales.
Data collection was completed from 20 November 2014 until 31 December 2014. Re-admissions to ICU during the same hospital stay were excluded. Ethical approval was not required (Wales REC 6). Each consecutive admission was prospectively screened for direct or indirect alcohol associations (defined as alcohol-attributable admissions) according to pre-determined definitions based on the ICD-10 criteria, outlined in a similar study.4 The Ward-Watcher database (Critical Care Audit Limited, Ilkley, UK) was used to obtain patient outcomes.
Using the patient’s postcode, a deprivation code was assigned using the Welsh Index of Multiple Deprivation (2011).5 Eight domains of deprivation are included and each domain is made up of a number of indicators. The income domain indicator was used as a marker of deprivation in this study as it is an absolute score which provides the percentage of those living in the area receiving income related benefits and has an extremely high correlation with the overall deprivation index.5
Patients’ characteristics for admission to ICU, attributable and non-attributable to alcohol.
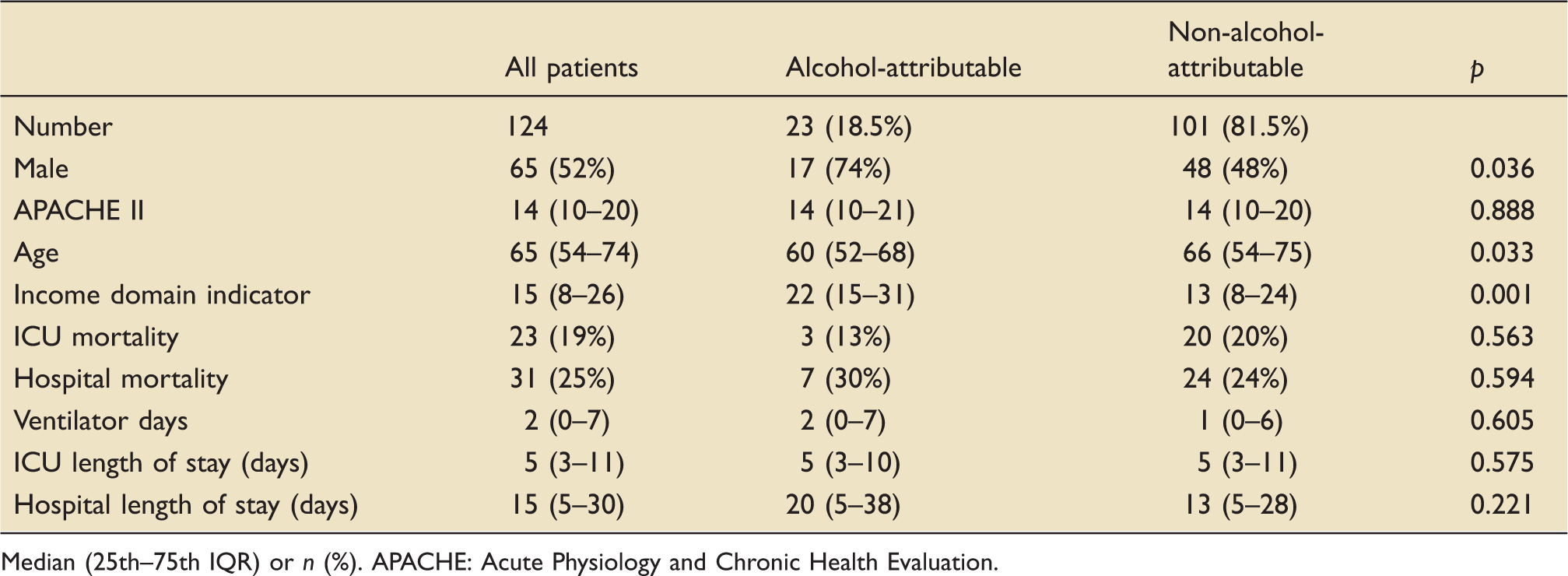
Median (25th–75th IQR) or n (%). APACHE: Acute Physiology and Chronic Health Evaluation.
In this study, we identified that almost a fifth of admissions were due to alcohol-attributable conditions. ICU mortality for alcohol-attributable admissions in our study was 13%, compared to a similar result of 18% in a recent Scottish study.4 Previous research has reported alcohol-related admissions are more likely to be male patients and younger compared with those without alcohol-related disease.4 The results of this study supported these findings. This study demonstrated that patients admitted to the ICU of a Welsh tertiary centre with alcohol-attributable conditions are significantly more likely to live in an area with higher social deprivation.
References
18R Visiting in intensive care: A survey of UK units
KS Deacon, JL Mitchell and LG Mould
University of Wolverhampton, UK
Intensive care units (ICUs) are stressful for both patients and relatives and when visiting is restricted relatives anxiety levels are increased.1 Relatives can experience feelings of helplessness and a lack of control, and these are reduced if allowed to visit more and help care for the patient.2 Patients have reported remembering their families visiting them in the ICU and that this helped them to feel secure, less alone and gave them the courage to fight.3 One previous survey of UK ICU visiting practices has been carried out which established that 80% of units had some level of restriction on visiting hours; within this, 80% of units allowed 4 h or more per day1. The current survey aimed to build on this data to establish what the range and average visiting time allowed is within UK ICUs, along with further questions on visiting policy and the influencing factors.
A survey was designed to provide answers on four specific questions: whether the unit has a written visiting policy, what the permitted visiting times are, the number of visitors allowed at one time and whether children are allowed to visit. Following each of these set questions, a free text box was provided to enable respondents to also comment on the factors that had influenced the decisions in each area. A final box was provided at the end of the survey for writing any further comments relating to visiting in their units.
The survey was posted to the lead nurse at 341 UK ICUs, which included 34 paediatric or neonatal units. A list of UK ICUs was obtained from the Intensive Care Society (ICS) and cross-referenced with a second list provided by the Intensive Care National Audit and Research Centre (ICNARC). Completed surveys were received from 166 units (48.7%). Analysis of these data will provide descriptive statistics to summarise responses to the set questions. Separate analysis of paediatric and neonatal unit data will allow for comparison with adult units. Alongside this a narrative summary of the influencing factors described and the further comments will be provided with illustrative quotes.
Having obtained data on visiting practices from just under half of UK ICUs the results of this survey will allow for an informed discussion of what current visiting practices are within UK ICUs and the factors the influence these practices.
References
19R Team perceptions of risk and safety: A qualitative study of ICU staffing
D D’Lima, E Murray and S Brett
Imperial College Healthcare NHS Trust, London, UK
Safety concerns have prompted an increasingly regulatory focus on intensive care unit (ICU) staffing, yet there is limited literature on the factors that ICU teams perceive to be relevant to safe team working and minimising staffing risks.
The aim of our qualitative interview study was to (i) examine the human factors that teams perceive to be relevant to safe staffing and (ii) identify practice improvements based on the factors to minimise risk and improve safety.
Forty-five semi-structured interviews were conducted with three core professional groups (nurses, doctors and physiotherapists) across three adult ICU units within one NHS trust. The qualitative interview data were analysed by a research psychologist. An initial framework of high level themes was developed based on the experiences of interviewers, discussion with clinical leads, the relevant literature and outcomes of initial coding exercises. This framework was then applied deductively across the dataset. In parallel to this approach, additional themes and sub-themes were identified inductively throughout the process of analysis. The framework was continuously discussed and iterated with input from clinical team members as the analysis progressed.
An overarching finding was the importance of achieving a dynamic balance within and across teams, patients and the hospital. Individuals and teams identified the need to exercise judgement and work resiliently in order to manage this balance, rather than relying on regulation and quotas (i.e. simply matching a certain amount or type of patients to a certain amount or type of staff). A set of related findings were identified. Interviewees’ views of the clinical status of patients did not necessarily fit established staff/patient ratios. For example, a Level 3 patient may need more physical support, but a Level 2 patient may need more combined psychological and physical support. Individuals had their own personalised perception of how to categorise the acuity of their patients and this developed with experience. A further finding was that interviewees’ views on what makes a good team were not necessarily objective. It seemed that people who are realistic (i.e. persevere to deliver ‘good enough’ care despite difficulties) were favoured as optimal team members over optimists (i.e. those people who tried to consistently perform at a high standard based on a value driven approach). We found that differing perspectives and priorities were identified across the professional groups, possibly reflecting professional roles and training. For example, where the accountability of the individual/team ends (i.e. at the unit or beyond) varied according to professional roles and seniority. Coping mechanisms were demonstrated where (particularly junior) staff focused in on the unit or individual patient and chose not to take on the responsibility of critically ill patients beyond the unit. This was demonstrated through both physical and mental separation from additional patient workload.
The results suggest the importance of team and unit dynamics, over regulation, to achieve a well-functioning unit. Resilience skills, such as working flexibly and optimal team utilisation, could be achieved through scenario-based team training, to encourage different professional groups to create and work towards shared priorities.
20R Abstract not available
21R A case note analysis of the reasons for early unplanned acute hospital re-admissions among adult ICU survivors
D Nassif1, N Jones1, E Donaghy2, L Salisbury3, P Ramsay3, N Lone1,3 and T Walsh1,3
1Department of Critical Care, Royal Infirmary Edinburgh, Edinburgh, Scotland
2Centre of Population Health Sciences, University of Edinburgh, Edinburgh, Scotland
3Critical Care Medicine, University of Edinburgh, Edinburgh, Scotland
Increasing numbers of adult intensive care unit (ICU) patients survive to hospital discharge. Recent research demonstrated a 23% re-admission rate to acute hospital beds within 90 days of discharge.1 The reasons for unplanned re-admission are uncertain but could indicate a system failure; it has been shown, for example, that few patients receive structured rehabilitation despite their complex physical and psychological needs.2 We undertook a case note review informed by a literature review of known drivers of unplanned hospital admission. We included patients who participated in a recently published randomised controlled trial of hospital-based rehabilitation, where local records indicated unplanned hospital re-admission within 90 days of hospital discharge.3
Our literature review was used to develop a preliminary explanatory matrix. In addition to medical indications (e.g. clinical deterioration), other factors included multi-morbidity, polypharmacy, social deprivation, socio-demographics, rurality, social support and substance misuse. We used this matrix to conduct a medical case note analysis, extracting data onto the different fields to categorise contributory factors.
Presence of known drivers of hospital re-admission.
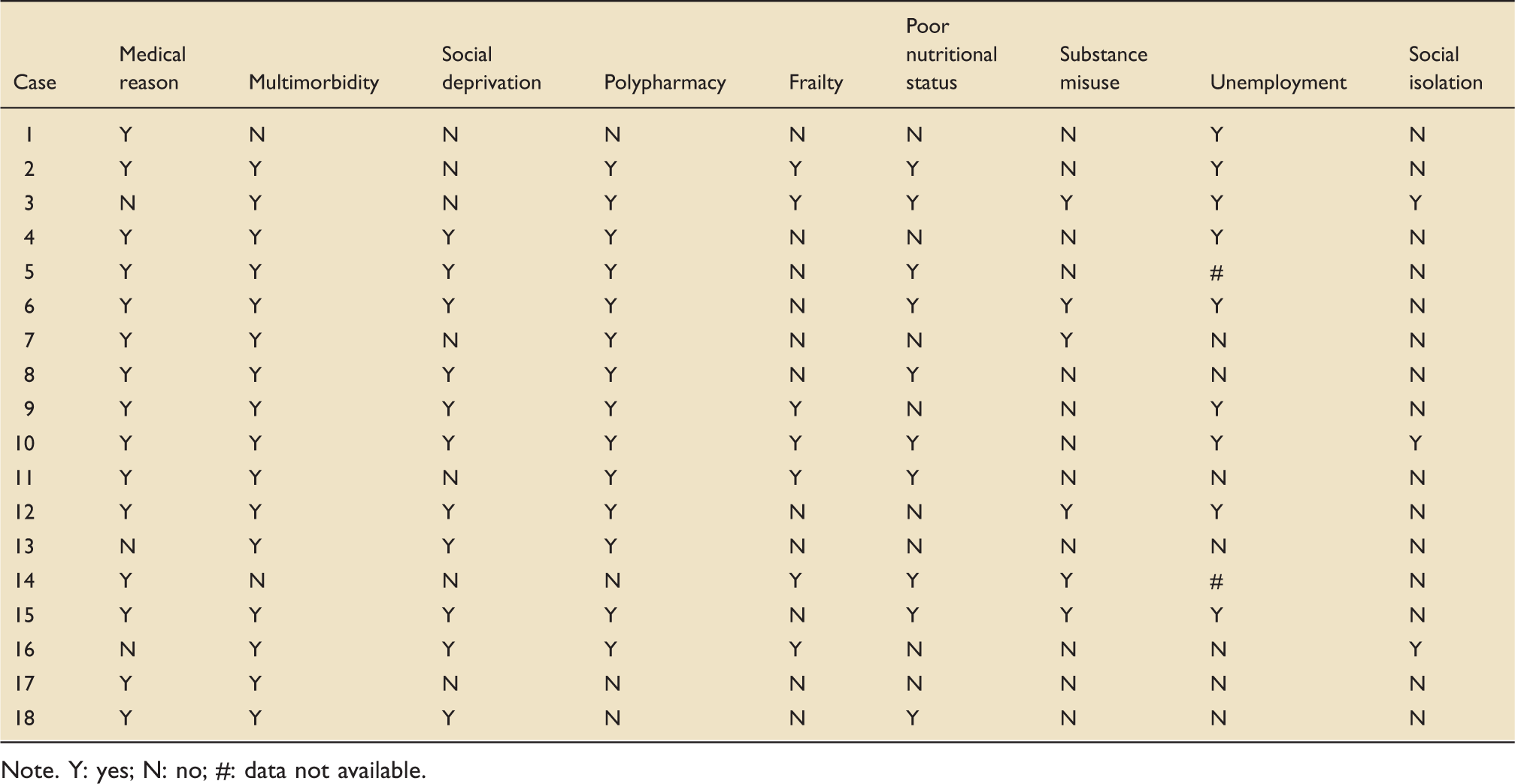
Note. Y: yes; N: no; #: data not available.
We found that most patients (15/18, 83%) had three or more documented physical co-morbidities and nine (50%) had documented psychological co-morbidities. Polypharmacy was highly prevalent (14/18, 78%), with 10 patients (55%) on high-risk medication (e.g. warfarin, insulin, immunosuppressants).
The Scottish Index of Multiple Deprivation (SIMD) score indicated that 10 patients (55%) were resident in the most deprived areas of the region (quintiles 1–2). Almost half lived alone with no social support, and a third had significant alcohol or substance misuse.
Our case note review demonstrates that a significant proportion of ICU survivors requiring unplanned acute hospital re-admission have significant pre-existing physical and psychological morbidity, and complex social issues including social deprivation, social isolation and alcohol and substance abuse. These data suggest that multiple factors other than the medical condition leading to ICU admission are relevant to unplanned re-admission, and by inference the recovery process towards independence. Our findings support the development of targeted interventions across health and social care that might anticipate need and be implemented both before and after hospital discharge.
Author Note
D Nassif and N Jones are Joint first authors.
References
22R Abstract not available
23R Direct monitoring of physical activity in critical care: Feasibility, tolerability and validity of the ActivPAL accelerometer
G Atkins, D McWilliams and C Snelson
University Hospitals Birmingham NHS Foundation Trust, Queen Elizabeth Hospital Birmingham, Birmingham, UK
Transitions between positions.

Percentage agreement between ActivPAL and video observation.

References
24R Mapping physical activity in critically ill patients in a UK intensive care unit: A prospective observational service study
J Mortimore1,2, J Rose3, N Hart1,4,5, S Berney3,6,7 and B Connolly1,4,5
1Lane Fox Clinical Respiratory Physiology Research Unit, St. Thomas’ Hospital, Guy’s & St. Thomas’ NHS Foundation Trust, London, UK
2Department of Physiotherapy, King’s College London, London, UK
3Physiotherapy Department, Austin Health, Melbourne, Australia
4Guy’s & St. Thomas’ NHS Foundation Trust and King’s College London NIHR Biomedical Research Centre, London, UK
5Division of Asthma, Allergy and Lung Biology, King’s College London, London, UK
6Institute of Breathing and Sleep, Austin Health, Melbourne, Australia
7Physiotherapy Department, University of Melbourne, Australia
Early mobilisation (EM) of critically ill patients in the intensive care unit (ICU) is advocated to mitigate against peripheral skeletal muscle wasting and weakness occurring during the illness course. Improvements in patient- and clinical-centred outcomes have been demonstrated with this approach. However, recent international datasets have highlighted poor implementation of EM into routine practice,–3 with patients spending significant proportions of the day in bed, alone and participating in little or no physical activity.4 To date, there are few published data regarding EM practice and physical activity levels of patients in UK ICUs.
The aim of the current study was therefore to prospectively characterise the profile of physical activity undertaken by critically ill patients in a UK ICU.
A single-centre, prospective observational study (HRA classification ‘service evaluation’, www.hra-decisiontools.org.uk/research/uk) utilising the technique of behavioural mapping was conducted in the 30-bedded adult tertiary referral ICU of a large, university teaching hospital between June and July 2015. Patients who had been invasively mechanically ventilated for more than 48 h and who were likely to remain in the ICU for a further 24-h period were included. Throughout the course of a full day (0830–2000), patients were observed for 1 out of every 10 min. During each observation, data on the location of the patient, persons present at the bedside and highest level of physical activity performed were recorded.
Forty-two patients were included: M:F 22:20, mean (SD) age 59.4 (15.0) years, SOFA at ICU admission 13.1 (3.5), medical admission diagnosis 32/42 (76.2%) in whom 2646 observations were collected over eight non-consecutive days (6 weekdays, 2 weekend days). On the day of observation, at a median (IQR) ICU length of stay of 7.9 (4.3–12.7) days, 31 patients were invasively mechanically ventilated with endotracheal tubes in situ, 4 were in receipt of extracorporeal membrane oxygenation therapy, 12 had inotropic support in situ and 18 were heavily sedated.
Summary of location, activity level and people present for the whole cohort and according to ventilation and sedation status.
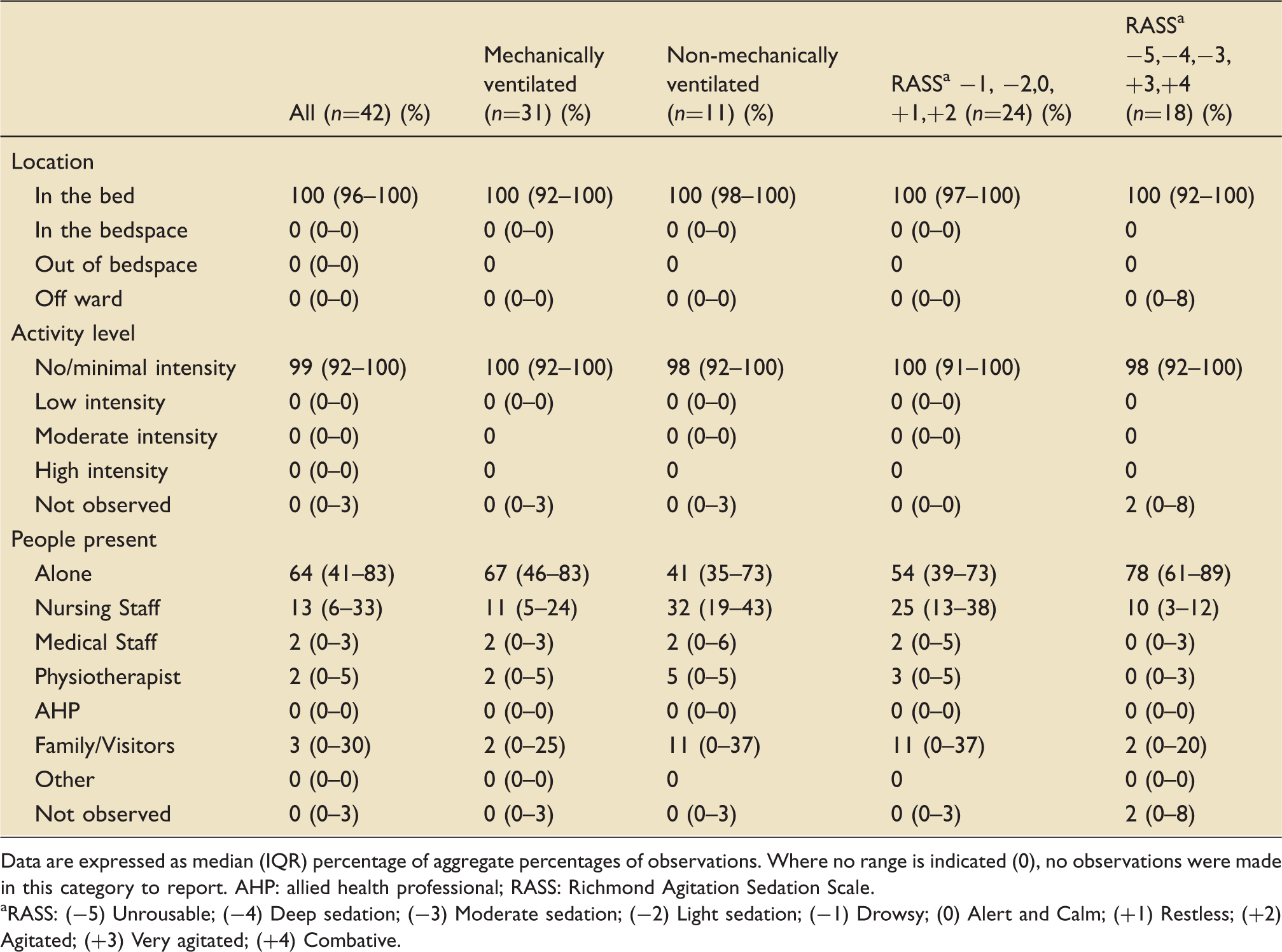
Data are expressed as median (IQR) percentage of aggregate percentages of observations. Where no range is indicated (0), no observations were made in this category to report. AHP: allied health professional; RASS: Richmond Agitation Sedation Scale.
RASS: (−5) Unrousable; (−4) Deep sedation; (−3) Moderate sedation; (−2) Light sedation; (−1) Drowsy; (0) Alert and Calm; (+1) Restless; (+2) Agitated; (+3) Very agitated; (+4) Combative.
These low physical activity levels in the majority of this cohort of ICU patients, who spent up to two-thirds of the day alone, highlight the potential for greater integration of physical activity into clinical management.
References
25R Can verbal encouragement and self-reported patient motivation predict active participation in physiotherapy on critical care?
CA Lawrence1,2, F Lorencatto2 and JJ Francis2
1Barts Health NHS Trust, London, UK
2School of Health Sciences, City University London, London, UK
Critical illness is systemic in nature and subsequent complications include global deconditioning, muscle wasting and decreased health-related quality of life.1 The prevalence and magnitude of these complications mean that rehabilitation is essential throughout the critical care continuum.1 ‘Rehabilitation’ refers to early movement, exercise and mobility. The ideal duration of each rehabilitation session remains undetermined and patient tolerability of treatment is under-researched.
The wider literature suggests patient motivation, self-efficacy and health beliefs can impact on participation in rehabilitation in outpatient physiotherapy settings.–4 However, it is unclear whether this translates to an inpatient environment. Routine physiotherapy in this setting is based on assumptions that patient motivation and verbal encouragement from physiotherapists may influence patients’ persistence during rehabilitation sessions. Therefore, the aim of this study was to identify whether self-reported patient motivation and extent of verbal encouragement given by physiotherapists during rehabilitation are predictors of duration of patients’ active participation in physiotherapy on critical care.
Patients were recruited at three hospitals. Between May and July 2015, all patients requiring critical care for >48 h, receiving physiotherapy, were invited to participate. A total of 31 patients participated (mean age = 60.61, range: 18-88 years), 15 males (48%) and 16 females (52%). The lead author observed a rehabilitation session and measured the length of time (minutes/seconds) of active patient participation in physiotherapy. Criteria for judging the start and end of active participation were decided following a small validation study. Participants were asked to complete a structured interview, conducted using four sub-scales from the intrinsic motivation inventory (IMI)5 and they indicated their agreement with statements about the session using a Likert scale (1 = not at all true, 7 = very true). Coefficient alpha (α) was computed to assess internal consistency reliability of the subscales. The physiotherapist and participant were also asked to report the amount of verbal encouragement given (1 = no encouragement, 7 = extreme encouragement).
The IMI subscale of interest/enjoyment (α=0.85) demonstrated good internal consistency in this patient group. It is considered to be the self-report measure of intrinsic motivation5 (median [IQR] = 5.71 [6–7]). The value/usefulness subscale suggested that patients felt physiotherapy was important to their recovery (median [IQR] = 7 [7–7]); however, limited variance meant it was not appropriate to use in subsequent analyses. There was also limited variation in amount of verbal encouragement as reported by the patient (median [IQR] = 7 [6–7]) compared with the physiotherapist (median [IQR] = 5 [3–6]).
Preliminary analysis was conducted using Spearman’s Rho correlation. There was no significant relationship between length of active participation and the following variables: mean score for interest/enjoyment (r(31) = −0.06, p = 0.74), verbal encouragement (patient) (r(31) = −0.17, p = 0.36) or verbal encouragement (physiotherapist) (r(31) = 0.29, p = 0.11).
In this relatively small cohort of patients, results suggest that preconceptions about motivation, encouragement and participation in physiotherapy may not be applicable in the critical care setting. However, the study highlighted difficulties with the measurement of constructs such as verbal encouragement and value/usefulness in this setting. Therefore, further research is needed to explore other potential patient barriers to participating in rehabilitation on critical care.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted in part fulfilment of a Master of Research Clinical Research award, which was funded by the National Institute of Health Research.
References
26R Abstract not available
27R Abstract not available
28R The effect of bed percussion vibration therapy on airflow in mechanically ventilated patients with severe respiratory failure
K Morris1,2, L Osman1,2, A Wilson2 and E Main2
1Department of Physiotherapy, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
2Institute of Child Heath, University College London, London, UK
Patients with severe respiratory failure (SRF) require mechanical ventilation which is associated with impaired mucociliary clearance.1 Airway clearance techniques (ACTs), including manual chest wall vibration (CWV) and hyperinflation are interventions which aim to expel secretions by increasing airway expiratory airflow bias.2 Critical thresholds of peak inspiratory flow to peak expiratory flow ratio (PIF:PEF) of <0.9 or an absolute difference in PIF-PEF of >17 l/min are reported to promote cephalad expulsion of mucus.3,4 Bed percussion vibration therapy (BPVT) is a modality, whereby a patient’s mattress delivers percussion and vibration. Manufacturers promote this modality as aiding secretion clearance; however, its effectiveness is yet to be determined. This study aimed to investigate the effectiveness of BPVT as an ACT by measuring airflow bias in mechanically ventilated patients with SRF.
This is a prospective, observational study. Patients admitted to a large inner-city hospital critical care unit were screened for eligibility. Patients included were on an SRF pathway, mechanically ventilated and nursed on the Total Care Bed® (Hill-Rom, IN, USA). Patient consent/consultee declaration was obtained, and ethical approval was granted by the local ethics committee (14/EE/0106). Primary outcomes were PIF:PEF and PIF-PEF difference, measured over three time periods: before, during and after BPVT. BPVT was applied for 15 min: 5 min percussion at 5 Hz followed by 10 min vibration at 13 Hz. Airflow was measured via a flowmeter inserted in to patients’ ventilator circuits. Physiological variables were recorded in parallel. Differences in primary outcomes were assessed using Wilcoxon signed-rank tests, significance reported at p < 0.05.
Group characteristics and primary variables.
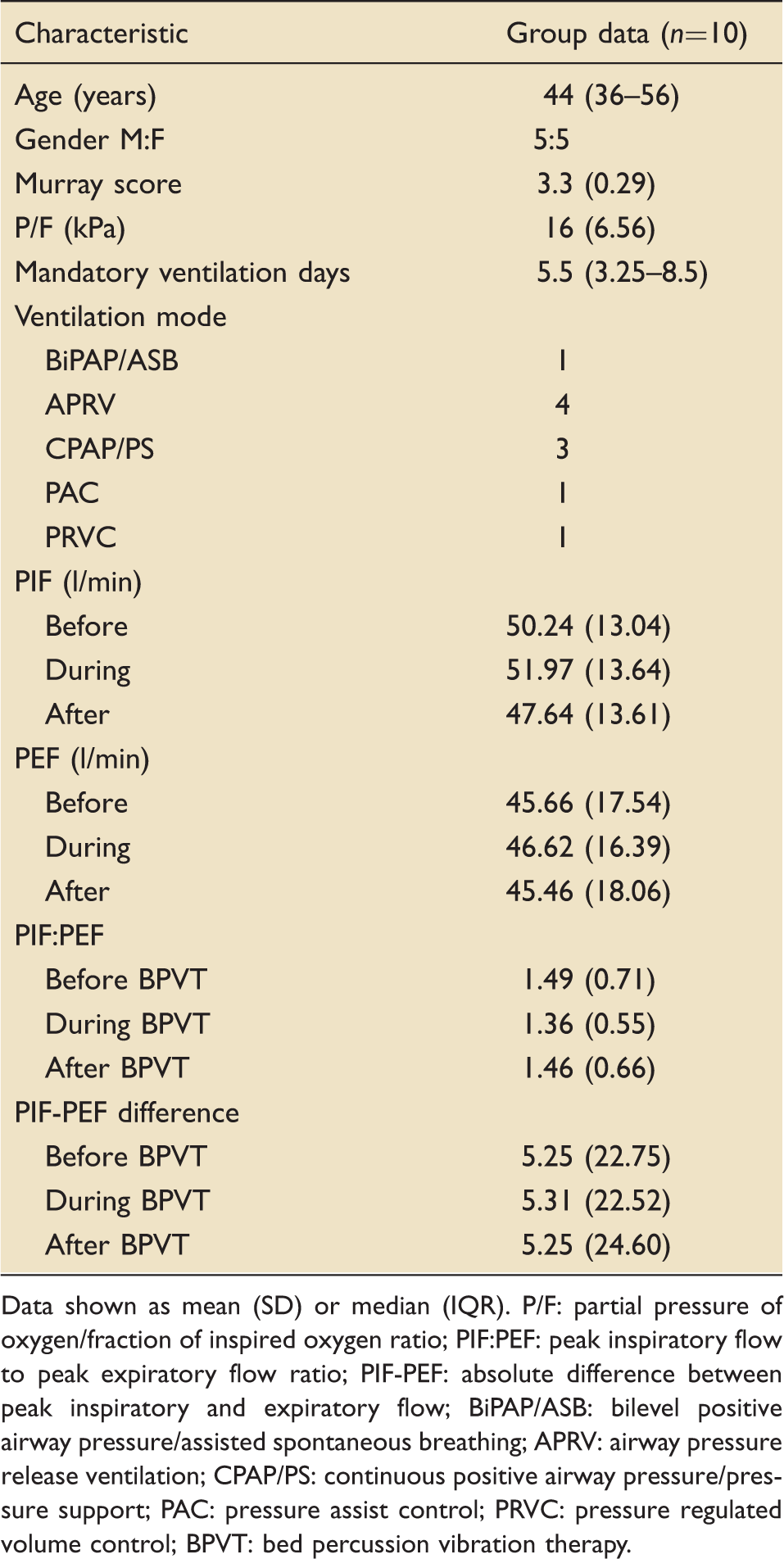
Data shown as mean (SD) or median (IQR). P/F: partial pressure of oxygen/fraction of inspired oxygen ratio; PIF:PEF: peak inspiratory flow to peak expiratory flow ratio; PIF-PEF: absolute difference between peak inspiratory and expiratory flow; BiPAP/ASB: bilevel positive airway pressure/assisted spontaneous breathing; APRV: airway pressure release ventilation; CPAP/PS: continuous positive airway pressure/pressure support; PAC: pressure assist control; PRVC: pressure regulated volume control; BPVT: bed percussion vibration therapy.
In this small heterogeneous group of patients with SRF, PIF:PEF and PIF-PEF differences did not meet critical thresholds to promote mucus expulsion during BPVT. Unlike physiotherapy CWV techniques, BPVT is applied without the presence of an opposing force. Manual CWV apply compressive forces downwards through the chest wall with the patient against a surface. The absence of any opposing force during BPVT may result in reduced transfer of chest wall forces to changes in airflow within the airways. The role of BPVT as an ACT in those with SRF has yet to be determined, further research is required in larger, defined populations, including evaluation of the forces applied and their effects on airflow within the airways.
References
29R Mortality in critically ill non-surgical patients with pre-existing pulmonary hypertension
KB Bauchmuller1, Y Arunan1, R Condliffe2, C Billings2 and GH Mills1
1Department of Anaesthesia and Critical Care, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK
2National Pulmonary Hypertension Service, Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK
Pulmonary hypertension (PH) is an uncommon yet life-limiting condition that has been associated with a poor prognosis. Recent changes in our understanding of its pathophysiology have led to novel therapeutic strategies.1 However, there is limited data on outcome of patients with PH requiring admission to an intensive care unit (ICU).2
We conducted a retrospective observational study of patients with PH admitted to the ICU in a UK national pulmonary hypertension referral centre for non-surgical conditions between April 2000 and July 2014. Data on patient characteristics, admission details, physiological and biochemical parameters as well as treatment modalities throughout the ICU stay were collected from our critical care electronic patient record system (Metavision) and the PH unit clinical database. ICU-specific therapies and their association with hospital survival were assessed using logistic regression analysis using SPSS. Results are expressed as median (range) and odds ratios (OR) with 95% confidence intervals (CI).
Therapeutic modalities associated with hospital survival.
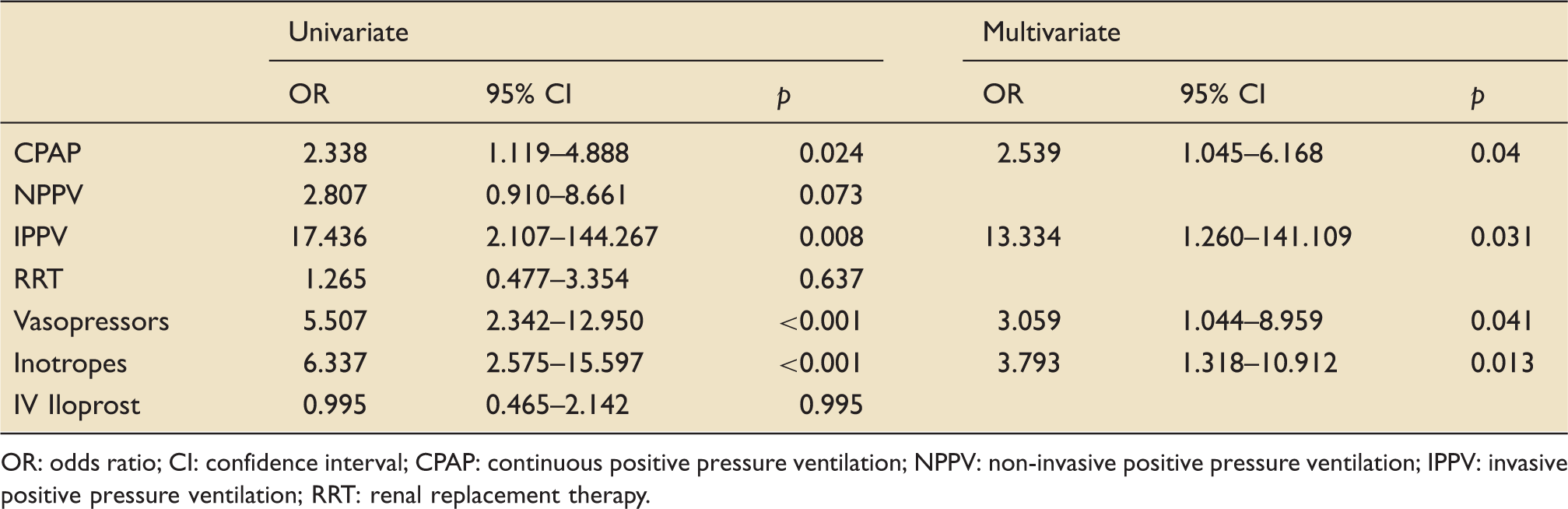
OR: odds ratio; CI: confidence interval; CPAP: continuous positive pressure ventilation; NPPV: non-invasive positive pressure ventilation; IPPV: invasive positive pressure ventilation; RRT: renal replacement therapy.
Overall, roughly two-thirds of patients with pre-existing PH admitted to ICU survived to hospital discharge. Invasive ventilation was associated with a dismal survival rate. The need for CPAP as well as haemodynamic support represented independent predictors of hospital mortality whereas renal replacement therapy did not. This may reflect the ability to tightly regulate fluid status thereby optimising preload of a compromised right ventricle.
References
30R Computational modelling of oxygen delivery in acute respiratory distress syndrome: Optimising positive end-expiratory pressure
M Chikhani1, A Das2, M Haque1, W Wang2, O Cole1, DG Bates2 and JG Hardman1
1Anaesthesia and Critical Care, Division of Clinical Neuroscience, University of Nottingham, UK
2School of Engineering, University of Warwick, UK
During mechanical ventilation, positive end-expiratory pressure (PEEP) is applied to the lungs of patients with acute respiratory distress syndrome (ARDS) to prevent collapse of open but unstable alveoli and to recruit collapsed alveoli.1 PEEP has the potential to impair cardiac output. Despite finding a consistent improvement in oxygenation and lung compliance, few studies have demonstrated a survival benefit associated with the application of high PEEP (i.e. >10 cm H2O) in ARDS.2 The reduction in cardiac output may outweigh the benefit of improved arterial oxygenation and alveolar mechanics by causing an overall reduction in oxygen delivery (DO2). Disease and patient heterogeneity makes the issue difficult to study in vivo, making this an ideal opportunity for high-fidelity modelling studies investigating the effects of PEEP in ARDS.
Graph showing modelled oxygen delivery in millilitres per minute (left hand axis) with PEEP (dark bars) and mean airway pressure (light bars) in cmH2O (right hand axis) during a time-based PEEP trial. Each line corresponds to a virtual patient.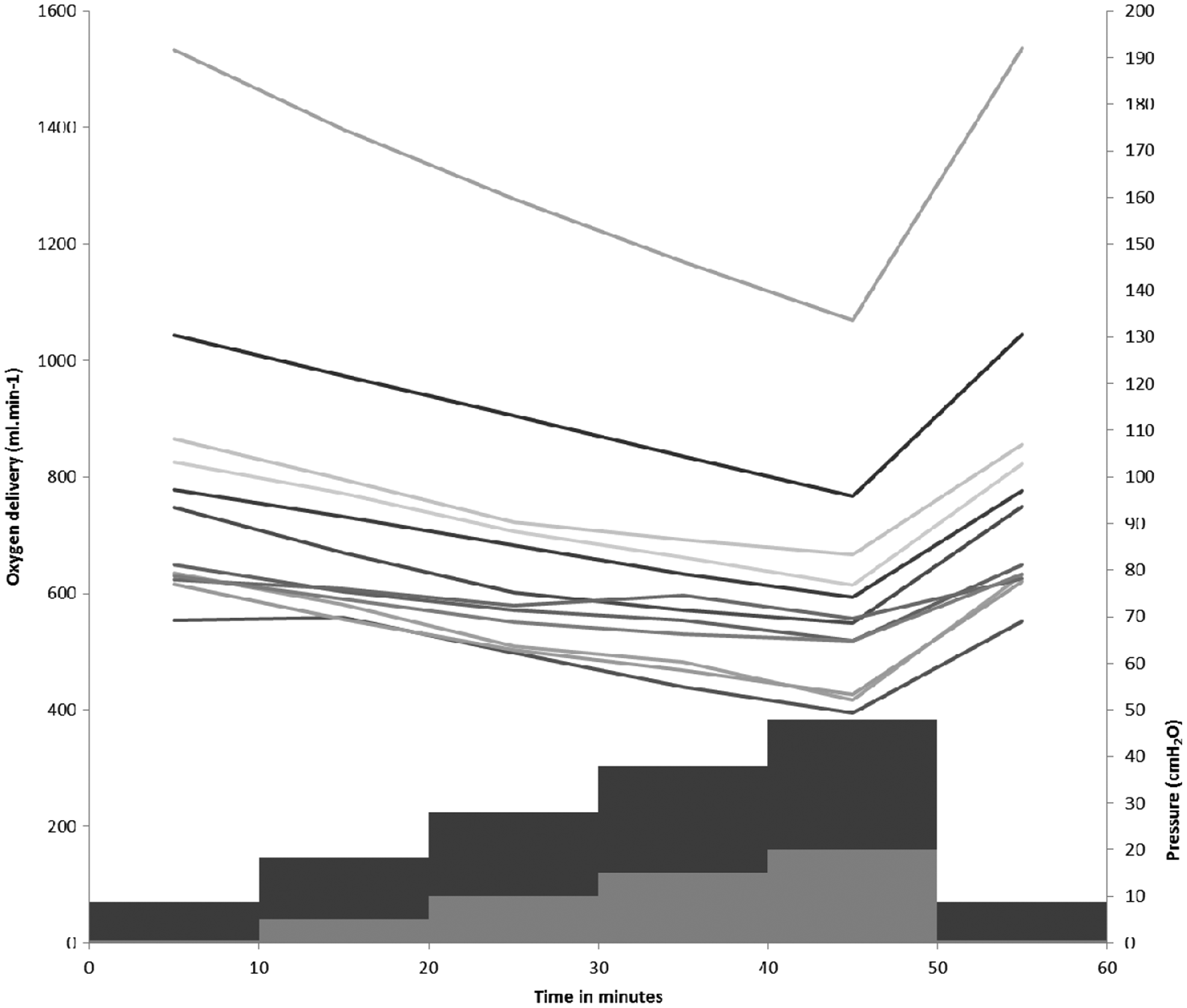
The Interdisciplinary Collaboration in Systems Medicine (ICSM)-integrated pulmonary and cardiovascular model was developed as a bespoke multi-organ, multi-scalar pathophysiological model. It is based on the widely validated Nottingham Physiology Simulator.3 The modelling includes a multi-chamber contractile cardiac model, dynamic alveolar behaviour and pulsatile blood flow. The model was matched to historical data to create nine virtual patients with various cardiovascular states and ARDS severity. These virtual patients underwent pulmonary ventilation using lung-protective techniques and were subjected to an incremental PEEP trial (10 min at each value of PEEP: 0, 5, 10, 15, 20 cm H2O), before returning to zero PEEP at the final setting.
In silico data describing alveolar gas exchange, cardiac output and alveolar dynamics were recorded. Cardiac output reduced and while oxygenation improved in every modelled patient at every increment in PEEP, although the rate of change in each of these varied between patients and between PEEP levels. Figure 1 illustrates the relationship between PEEP, mean airway pressure and DO2.
Using high-fidelity simulation, we have demonstrated the potential for oxygen delivery to reduce in response to the incremental increase in PEEP even in the context of an apparent improvement in gas exchange. The reduction in DO2 was most apparent in simulated patients with less severe gas exchange defect.
The observed fall in DO2 is of particular importance in the context of routine monitoring of oxygenation but not cardiac output – potentially leading to a misleading impression of clinical therapeutic benefit with increasing airway pressure. We hypothesise that the clinically observed improvement in oxygenation during PEEP may be offset by a reduction in organ perfusion, and that this might account for the failure to demonstrate any survival benefit of high-PEEP ventilation strategies in patients with ARDS.