The use of a restrictive red-cell transfusion strategy in adult ICU patients with septic shock resulted in similar rates of mortality, life-support requirements and ischaemic events compared to a liberal transfusion strategy, but resulted in significantly fewer blood transfusions. Level of evidence: 1B (CEBM, RCT of good quality).
Appraised by: Liam P Scott
Citation: Holst LB, Hasse N, Wetterslev J, et al. for the TRISS Trial Group and the Scandinavian Critical Care Trials Group. Lower versus higher haemoglobin threshold for transfusion in septic shock. N Engl J Med 2014; 371: 1381–1391.
Lead author: Lars B Holst, lars.broksoe.holst@regionh.dk
Three part clinical question:
Patients: Adult patients in the intensive care unit (ICU) with septic shock and haemoglobin (Hb) ≤9 g/dl.
Intervention: Patients were randomly assigned to either a lower threshold (Hb ≤7 g/dl, ‘restrictive’) or higher threshold (Hb ≤9 g/dl, ‘liberal’) transfusion strategy; they were given single cross-matched units of leucodepleted red blood cells to achieve the assigned transfusion threshold.
Outcomes: Primary outcome was mortality rate at 90 days post-randomisation. Secondary outcomes included the requirement for life support (renal replacement therapy, mechanical ventilation, inotropic support) at days 5, 14 and 28; the occurrence of serious adverse reactions; number of days alive without life support at 90 days and days alive outside of hospital at 90 days.
Study design: International, multi-centre, parallel-group, prospective randomised trial.
Study patients:Inclusion criteria: Adult patients with septic shock and Hb ≤9 g/dl, presenting to 32 Scandinavian ICUs over a two-year period. Exclusion criteria: Patients who declined transfusion or for whom consent could not be obtained, prior adverse reaction to a blood transfusion, patients who had already received a transfusion during the current ICU admission or those with acute coronary syndromes, active haemorrhage or acute brain injury. One thousand two hundred and twenty-four patients were assessed for eligibility and 1005 underwent randomisation; five were subsequently excluded.
Study groups: Five hundred and three patients were randomly assigned to the lower threshold, ‘restrictive’ group and 497 patients were assigned to the higher threshold, ‘liberal’ group. Patients were transfused single cross-matched units of leucodepleted red cells once their measured haemoglobin had reached the assigned thresholds. Haemoglobin levels were reassessed within 3 h of transfusion or prior to commencing a further transfusion.
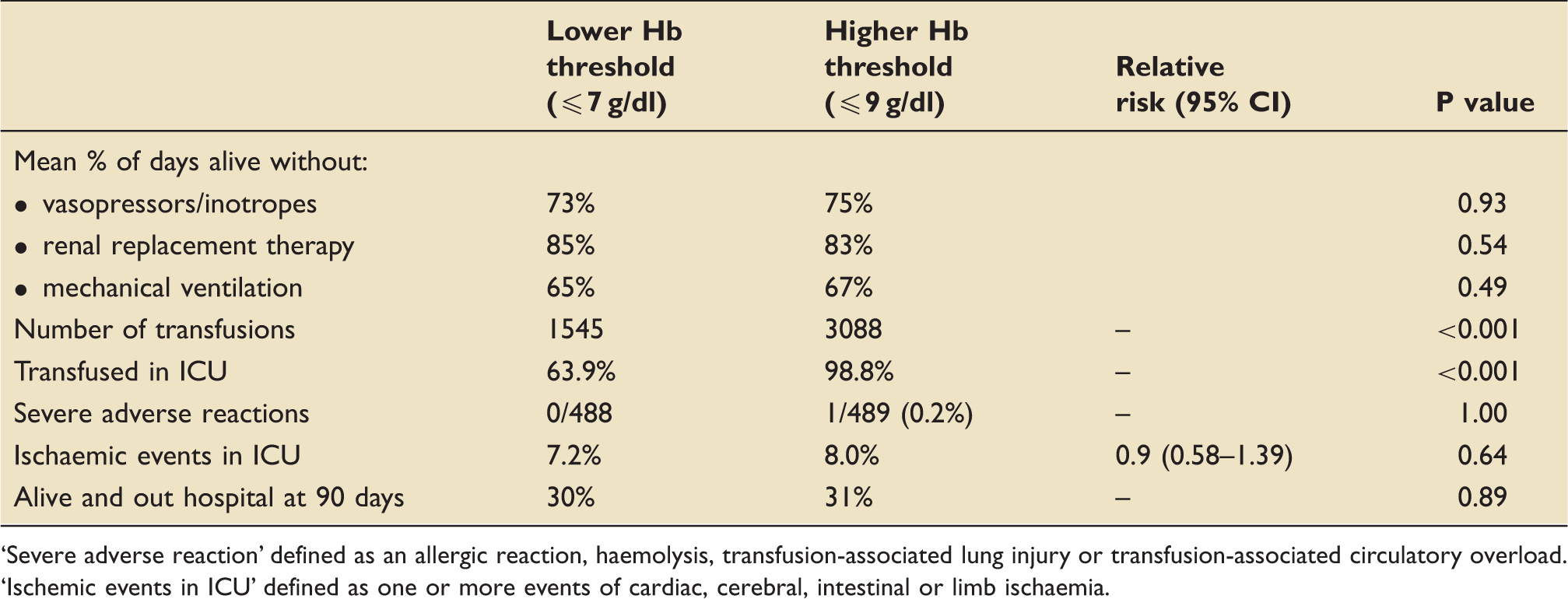
The results: (see Table 1). There was no significant difference in 90-day mortality when using a restrictive transfusion threshold compared to a liberal threshold. For secondary outcomes (see Table 2), there was no significant difference in days alive without life support, ischaemic events or severe adverse reactions. When using a restrictive transfusion threshold, there was a significant reduction in both the number of transfusions administered and the proportion of patients transfused in the ICU.
Primary outcomes.
Outcome
Time to outcome
CER
EER
RRR
ARR
NNT
Death
90 days
0.450
0.430
4%
2%
ns
95% confidence intervals:
−9 to 18%
−4.2 to 8.2%
ARR: absolute risk reduction; CER: control event rate (higher Hb group); EER: experimental event rate (lower Hb); NNT: number needed to treat; ns: not significant; RRR: relative risk reduction.
Secondary outcomes.
Lower Hb threshold (≤7 g/dl)
Higher Hb threshold (≤9 g/dl)
Relative risk (95% CI)
P value
Mean % of days alive without:
• vasopressors/inotropes
73%
75%
0.93
• renal replacement therapy
85%
83%
0.54
• mechanical ventilation
65%
67%
0.49
Number of transfusions
1545
3088
–
<0.001
Transfused in ICU
63.9%
98.8%
–
<0.001
Severe adverse reactions
0/488
1/489 (0.2%)
–
1.00
Ischaemic events in ICU
7.2%
8.0%
0.9 (0.58–1.39)
0.64
Alive and out hospital at 90 days
30%
31%
–
0.89
‘Severe adverse reaction’ defined as an allergic reaction, haemolysis, transfusion-associated lung injury or transfusion-associated circulatory overload.
‘Ischemic events in ICU’ defined as one or more events of cardiac, cerebral, intestinal or limb ischaemia.
EBM questions:
Do the methods allow accurate testing of the hypothesis?Yes. This was a large multi-centre, computer-randomised, pragmatic clinical trial. All treatment decisions other than transfusion thresholds were at the discretion of the treating clinicians. The outcomes assessor and trial statistician were blinded to study group allocations, although it was impractical to do so for the treating clinicians.
Do the statistical tests correctly test the results to allow differentiation of statistically significant results?Yes. The authors calculated 1000 patients would be needed to provide an 80% power to detect a 9% absolute reduction in mortality after 90 days in the lower threshold group. These calculations were based upon the 45% mortality and 20% relative risk reduction seen in the restrictive group in the similar TRICC trial.1 The recruitment target was achieved.
Are the conclusions valid in light of the results?Yes. The study demonstrated there was no significant difference in mortality rates at 90 days when using a restrictive compared to a liberal transfusion strategy. This effect was confirmed by the intention-to-treat and per-protocol analysis, and remained consistent across a range of pre-specified subgroups. The majority of patients screened for eligibility underwent randomisation, the two groups had very similar baseline characteristics after allocation and data were available from 99.3% of patients for the primary outcome analysis.
Did results get omitted and why?Yes. Sixty-two patients discontinued the study (38 in the lower threshold group, 24 in the higher threshold group), predominantly at the patients’ or their surrogates’ request. This data wasn’t used for analysis of secondary outcomes but was still available (except for two patients) for analysis of the primary outcome. It is worth noting there were significantly more protocol violations in the lower threshold group compared to the higher threshold group (5.9% versus 2.2%, p = 0.004), suggesting more patients in the restrictive group were transfused at a higher level than intended. However, this had no effect on outcomes in the per-protocol analysis.
Did the authors suggest any further areas of research?Yes. The study specifically excluded patients with active cardiac ischaemia, as have other similar studies. The authors note that further research is needed to assess the safety of lower transfusion thresholds in these patients.
Did they make any recommendations based on the results and are they appropriate?No. The authors make no specific recommendations.
Is the study relevant to my clinical practice?Yes. The patients enrolled are representative of many adult patients presenting with septic shock to both academic and non-academic centres throughout the UK. The current Surviving Sepsis guidelines2 recommend that after resolution of initial hypoperfusion blood transfusions should be instigated once Hb ≤7 g/dl (to target a range of 7–9 g/dl). However, during the initial resuscitation transfusion practice has historically been guided by the River’s trial,3 which promotes a liberal transfusion strategy (target haematocrit 30%, approximately 9–10 g/dl). This present study has ramifications for patient safety, resource allocation and cost efficiency. It demonstrates that a restrictive transfusion strategy, applied through all phases of the critical care management of septic shock, does not affect mortality whilst reducing the overall number of blood transfusions.
What level of evidence does this study represent?1B. A good quality RCT.
What grade of recommendation can I make on this result alone?A
What grade of recommendation can I make when this study is considered along with other available evidence?A. This trial concurs with several other high-quality studies from critical care, medicine and surgery which suggest a restrictive transfusion threshold is safe in a variety of patient populations (excluding those with active cardiac ischaemia).
Should I change my practice because of these results?Probably not. It is likely that most hospital transfusion policies in the UK already promote a lower haemoglobin threshold for transfusion – although until the present study the rationale for doing so in septic shock had yet to demonstrated.
Should I audit my practice because of these results?No. No specific audit is suggested by this study.
Footnotes
Appraised by:
References
1.
HebertPCWellsGBlajchmamMA. A multicentre, randomised controlled clinical trial of transfusion requirements in critical care. N Engl J Med1999; 340: 409–417.
2.
DellingerRPLevyMMRhodesA. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock – 2012. Crit Care Med2013; 41: 580–637.
3.
RiversENguyenBHavstadS. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med2001; 345: 1368–1377.