
Abstract

In critically ill patients, there was no significant difference in 28-day mortality in patients resuscitated with colloids compared to crystalloids. However 90-day mortality was significantly higher in the crystalloid group, Level of evidence: 1B (CEBM, RCT of good quality)
Patients: Adult patients accepted to the intensive care unit (ICU) requiring fluid resuscitation for acute hypovolaemia.
Intervention: Patients received either crystalloids (isotonic/hypertonic saline or any buffered solutions) or colloids (hypo-oncotic (e.g. gelatins, 4%/5% of albumin)) and hyper-oncotic (e.g. dextrans, hydroxyethyl starches and 20%/25% of albumin) solutions. Within each treatment group, investigators could use whichever fluids were available at their institution. The amount of fluid and duration of treatment were left at the discretion of the investigators within certain restrictions. These were that the daily total dose of hydroxyethyl starch could not exceed 30 ml/kg and investigators were required to follow any local regulatory agency recommendations governing use. Patients were subsequently managed exclusively within the fluid category to which they were randomised until ICU discharge. Exceptions were that regardless of treatment group, maintenance fluids were isotonic crystalloids and if physicians wished, they could administer albumin in response to demonstrated hypoalbuminemia (serum albumin <20 g/dL).
1. Primary outcome: Mortality at 28 days.
2. Secondary outcomes: Mortality at 90 days, ICU discharge and hospital discharge; number of days alive and not receiving renal replacement therapy, mechanical ventilation or vasopressor therapy; days without organ system failure (i.e. Sequential Organ Failure Assessment (SOFA) score <6); days not in the ICU/hospital.
3. Study design: International, multi-centre, prospective, parallel group, randomised clinical trial. The CRISTAL Trial was designed to test whether colloids altered mortality compared with crystalloids for fluid resuscitation in critically ill patients.
Eligibility: Adults who had not received fluids for resuscitation during their ICU stay and now required fluid resuscitation for acute hypovolaemia defined by a combination of:
Hypotension (systolic arterial pressure <90 mmHg, MAP <60, orthostatic hypotension, Delta pulse pressure of ≥13%. Evidence for low filling pressures and low cardiac index assessed invasively/non-invasively Signs of tissue hypoperfusion/hypoxia (≥2 of: GCS <12, mottled skin, UO <25 ml/h, CRT ≥3 s, arterial lactate >2, BUN >56 mg/dL, fractional excretion of sodium <1% The evidence (Control group = crystalloids; Experimental group = colloids). Notes: CER = control event rate, EER = experimental event rate, RRR = relative risk reduction, ARR = absolute risk reduction, NNT = number needed to treat.
Exclusion criteria: received fluid therapy in ICU, anaesthesia-related hypotension, advanced chronic liver disease, chronic renal failure, acute anaphylactic reaction, inherited coagulation disorders, had DNAR pregnant, burned >20% of body surface area, allergy to any study drug, refused consent, dehydrated, brain death/organ donor.
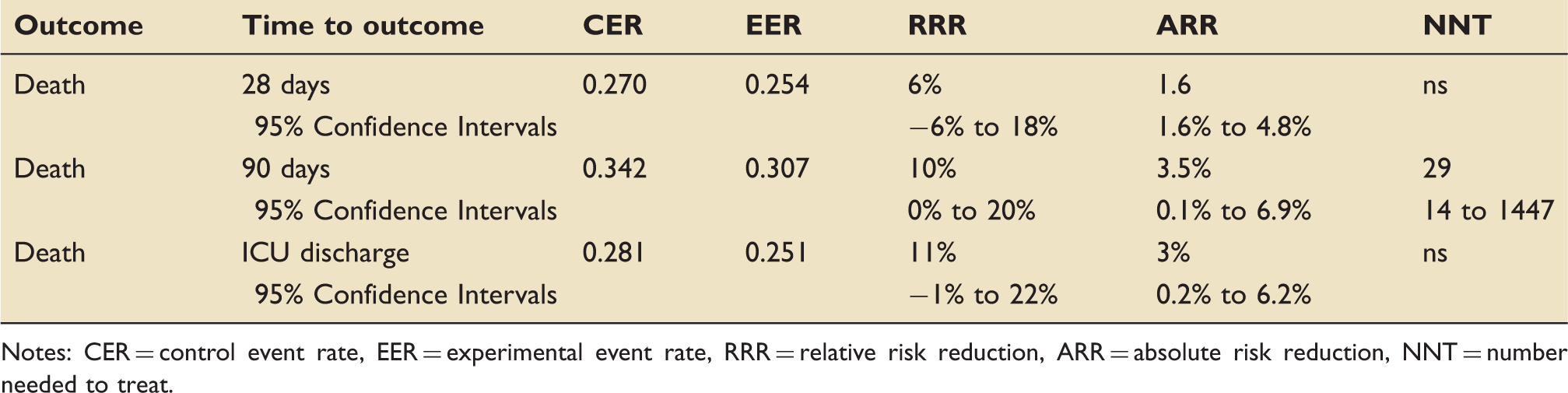
Do the methods allow accurate testing of the hypothesis? Yes. This was a large, international, multi-centred, computer-randomised, controlled trial. The only potential problems were that the clinicians were not blinded; however, the outcome assessors were which minimised the risk of assessment bias. Secondly, the extended recruitment period of nine years; however, this was not shown to modify the direction and size of estimates. Do the statistical tests correctly test the results to allow differentiation of statistically significant results? Yes. Are the conclusions valid in light of the results? Yes. The authors conclude that in ICU patients with hypovolaemia, the use of colloids compared with crystalloids did not result in a significant difference in 28–day mortality, and the results support this. However, within secondary outcomes, 90–day mortality was significantly higher with the use of crystalloids (p = 0.03). There were also significantly more days alive within 7 and 28 days without mechanical ventilation (p = .01/.01) and without vasopressor therapy (p = 0.04/0.03) in the colloid group. The authors offer three explanations for these results and feel further exploratory studies are required before conclusions are drawn. It is also worth noting that the trial was only powered to detect a 5% difference in risk of death at 28 days and therefore these secondary outcomes may not be statistically or clinically significant. Did results get omitted and why? Did the authors suggest areas of future research? Did they make recommendations based on the results and were they appropriate? Is the study relevant to my clinical practice? What level of evidence does this study represent? 1B
What grade of recommendation can I make on this result alone? What grade of recommendation can I make when this study is considered along with other available evidence? Should I change my practice because of these results? No. Considering the outcome of the study, there is no current evidence to change practice. Given that colloids are considerably more expensive than crystalloids, it is hard to see how their continued use can be justified over crystalloids. However, if a further study powered for 90-day mortality showed a statistically significant difference then one would strongly consider a change of practice if supported by other randomised controlled trials. Should I audit my current practice because of these results? No. Substantial numbers were required to demonstrate a statistical difference in the primary outcomes and local audit is therefore unlikely to be worthwhile.
Footnotes
Sarah Evans, Clinical Fellow, Intensive Care Unit, Northwick Park Hospital, Harrow, UK.