Use of an Early-Goal-Directed therapy protocol did not improve outcome in patients with septic shock in comparison to a standard treatment protocol, or usual care based on physician judgement. Level of Evidence: 1B
Appraised by: G Evetts, K Birch
Citation: The ProCESS Investigators. A randomised trial of protocol-based care for early septic shock. N Engl J Med 2014;370:1683-1693
Lead author: Derek C Angus, angusdc@upmc.edu
Three-part clinical question:
Patients: Patients with a diagnosis of septic shock refractory to initial fluid resuscitation of 1000 ml.
Intervention: Patients were randomised to one of three groups: (a) Protocol-based early-goal-directed therapy (EGDT) (b) Standard protocol therapy (c) Usual care as directed by bedside physician.
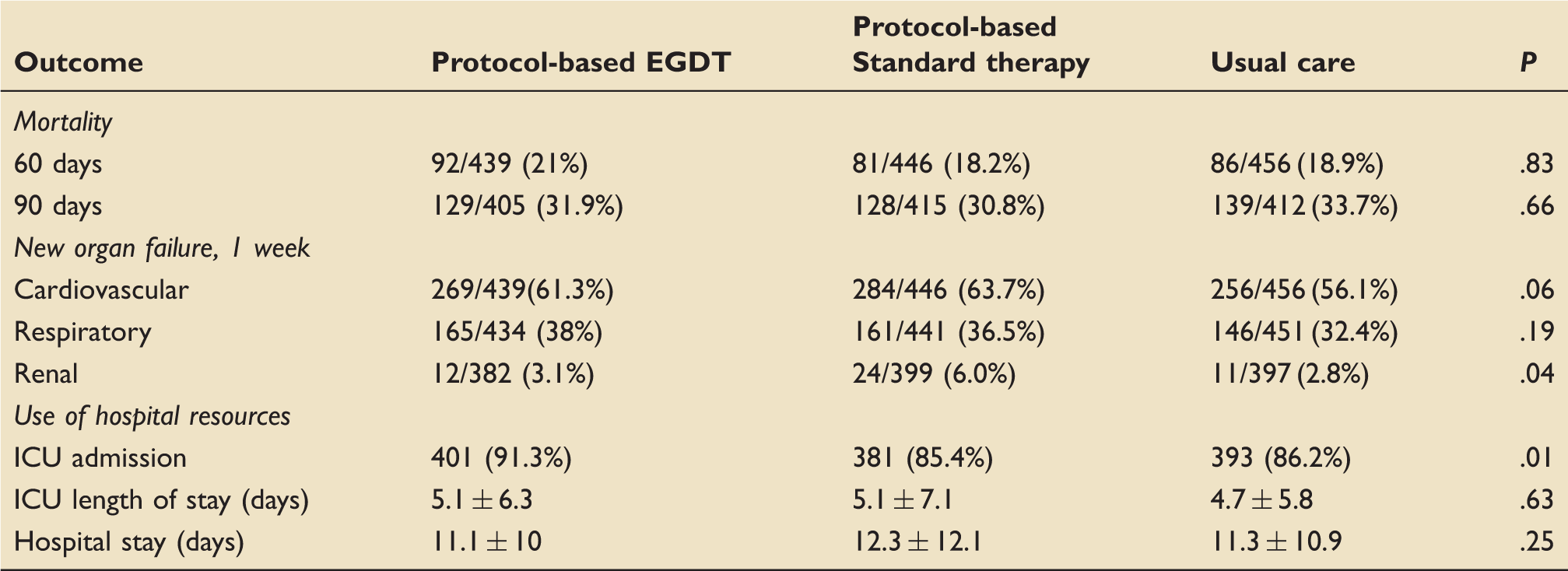
Outcomes: Primary outcome was 60 days in-hospital mortality. Secondary outcomes included mortality at 90 days and 1 year, a requirement for organ support, length of stay in intensive care and hospital, discharge disposition and any serious adverse events.
The study design: Prospective, randomised, multi-centre trial recruiting from 31 Emergency Departments (EDs) of tertiary teaching hospitals with > 40,000 yearly ED visits, who adhere to surviving sepsis campaign guidelines, use serum lactate as a screen for cryptogenic septic shock but do not routinely use central venous oxygen saturation (ScvO2) catheters or have a septic shock resuscitation bundle. Statistical analysis was conducted before unblinding.
The study patients: Inclusion criteria: Patients >18 years of age admitted to ED with a diagnosis of sepsis according to the physician with ≥2 systemic inflammatory response syndrome (SIRS) criteria and refractory hypotension (systolic <90) or lactate ≥4 despite 1000 ml fluid challenge in 30 min. All patients were enrolled within 2 h of detection of shock and within 12 h of admission.
Exclusion criteria: Patients with acute coronary syndrome, pulmonary oedema, status asthmaticus, major cardiac arrhythmia, gastrointestinal haemorrhage, seizures, drug overdose, burns, trauma, pregnancy, inter-hospital transfer, low CD4 count, and when treatment was considered futile.
Study groups: Each protocol was followed for 6 h post randomisation. Thereafter, care was left to the discretion of the responsible team.
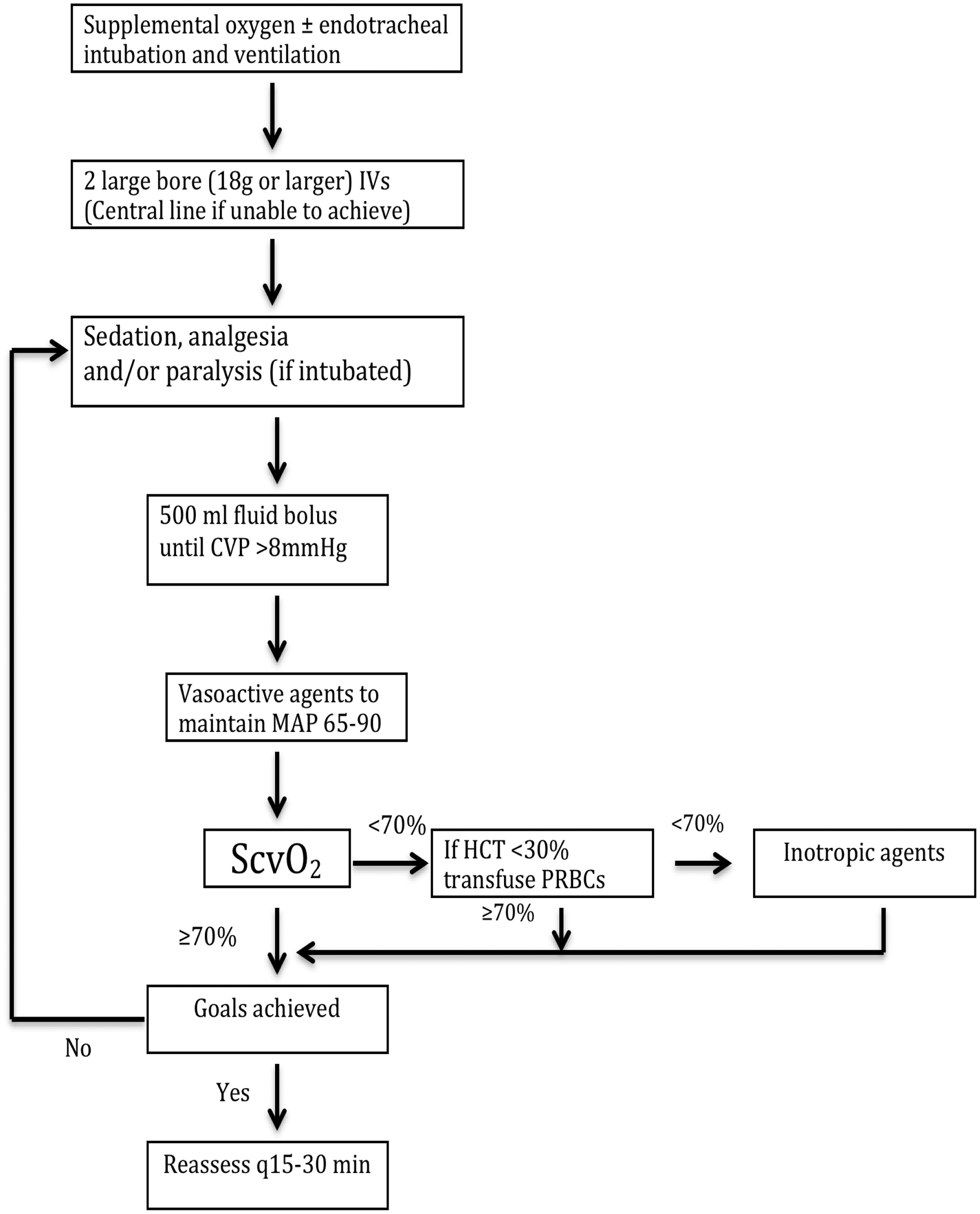
EGDT protocol group (439 patients): central venous saturation oximetry probe to target ScvO2 of 70% with fluid boluses, haematocrit optimization to 0.3 or inotropic agents (Figure 1).
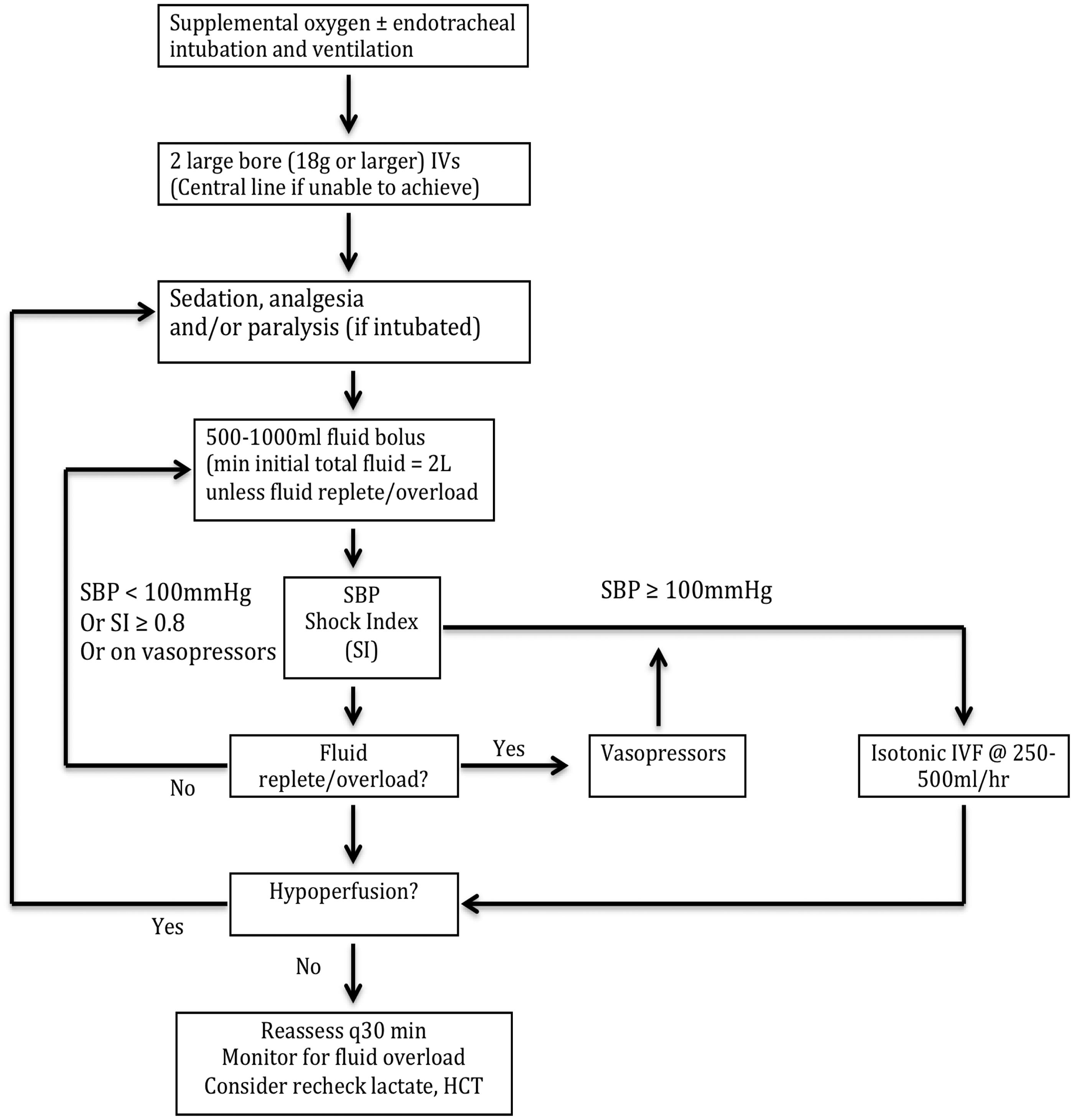
Standard protocol group (446 patients): peripheral access only, unless vasoactive agents were required or there was difficulty in obtaining intravenous access. Each protocol was followed for the first 6 h after randomisation (Figure 2).
Both the protocol groups were cared for by the same trained and dedicated physician-led team. Adherence to study protocols was monitored by external study staff using a flow chart examining physiological goals and actions in attempt to achieve them.
Usual care group (456 patients): This was left to the discretion of a non-study clinician.
Results - see tables overleaf.
EBM Questions
Do the methods allow accurate testing of the hypothesis? Yes. This was a multi-centre, randomized, comparison of protocols against a non-standardised approach. The same team provided care to the patients randomised to the protocolised care arms, but a separate non-study team provided care to the usual care group in order to minimise any operator bias. Study physicians could not be blinded, but data analysis was performed by blinded study personnel. Adherence to protocols was monitored by study staff using an adherence flowchart for each protocol arm.
Do the statistical tests correctly test the results to allow differentiation of statistically significant results? Yes. Data were analysed on an intention-to-treat principle. The investigators tested sequentially whether protocol-based resuscitation (EGDT or standard-based therapy) was superior to usual care, and then whether protocol-based EGDT was superior to protocol-based standard therapy. Power calculation based upon 80% to detect a mortality reduction of 6–7% gave a sample size of 1950 patients. This assumed a mortality of 30–46% in the usual care group based on the similar study by Rivers et al.1 However, analysis before 1300 patients showed a lower than expected mortality of 20% which was also consistent with another study.2 Recalculation gave a sample size of 1350 for the same power. Primary outcome of 60-day mortality was tested using Fisher’s exact test. In case of test site variability, secondary analysis included a linear mixed model, which allowed for any effect of study site. For all other secondary outcomes, Fisher’s exact test was used for categorical outcomes and analysis of variance for continuous variables. Cumulative Kaplan-Meier mortality curves to display between-group differences were constructed. Breslow-Day tests assessed interactions between treatment assignment and subgroups such as age, sex, infective source, lactate levels, etc. Subgroup analysis based on Acute Physiology and Chronic Health Evaluation (APACHE) II score, baseline serum lactate levels and time from shock detection to randomization was also performed using logistical regression to test for correlation.
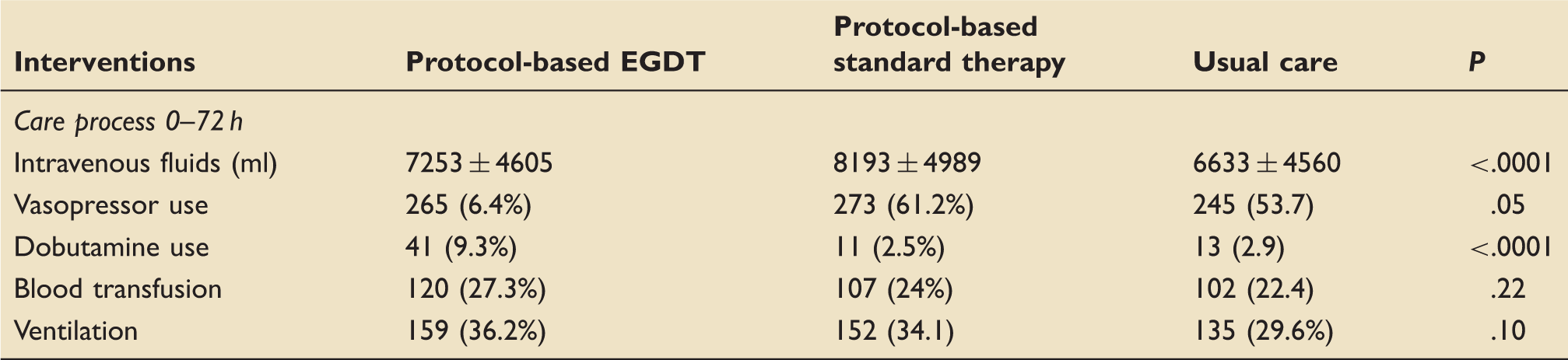
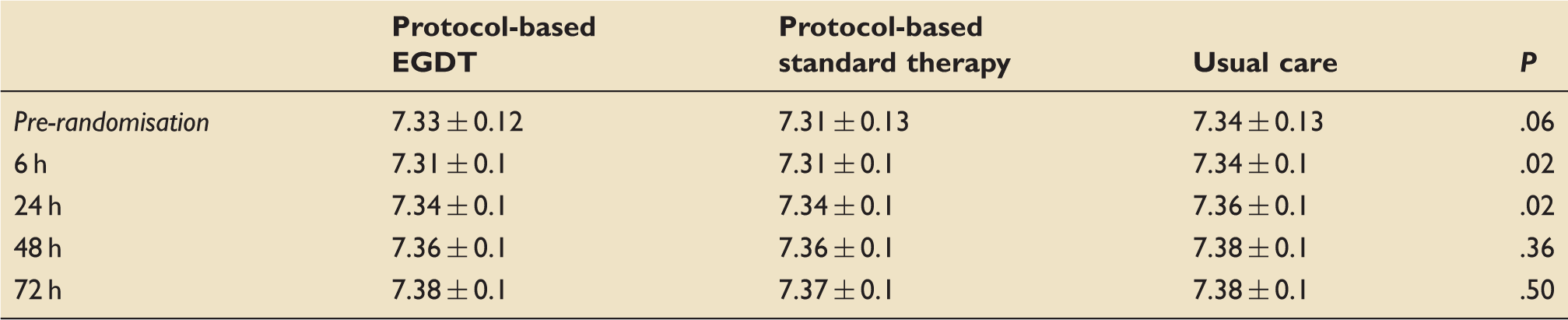
Are the conclusions valid in light of the results? Yes. Baseline characteristics between the groups were not significantly different in terms of demographics, source of sepsis, APACHE II score, serum lactate, or time to randomization. Adherence to protocols was high, with only 11.9% and 4.4% patients being non-adherent in the EGDT and standard-therapy groups, respectively. Treatment in terms of intravenous fluid volume, vasoactive drug usage and blood transfusion was not significantly different in the 6–72 h period. Use of antibiotics, glucocorticoids, and activated protein C was also not significant between the groups. However, it is worth noting that at 6 h the average pH values in the protocol-based groups were significantly lower than the usual care group at 7.1 and 7.4, respectively (Table 4). This could imply increased severity of sepsis in those groups. This theory might be supported by the fact that significantly more patients in the EGDT group were admitted to an intensive care unit (Table 1).
Did results get omitted and why? Yes. Ten patients withdrew their consent from the study, leaving 1341 patients in the analysis.
Did the author suggest any further areas for research? No. However, the authors do comment on the study’s inability to examine what aspects of the very early stages of a patient’s care may have on outcomes in sepsis.
Did they make recommendations based on the results and were they appropriate? No. No specific recommendations were made, but the authors declared that if patients with sepsis are identified early and received antibiotics in addition to other non-resuscitative aspects of care promptly, then there was no advantage in using a protocol-based resuscitation using central venous monitoring.
Is the study relevant to my clinical practice? Yes. The patients in the study are fully representative of UK patients with septic shock. EGDT using ScvO2 has been part of fluid resuscitation in sepsis along with other patient cohorts for over 10 years, based on papers such as the Rivers study,1 and Shoemaker.3 The surviving sepsis campaign guidelines recommended use of ScvO2, and thus it is considered best practice. This paper calls in to question the positive impact this has on patient outcome.
What level of evidence does the study represent? 1B. The study design and testing of adherence to study protocol, together with correct and interim power analysis make this a good quality study.
What grade of recommendation can I make on this result alone? A
What grade of recommendation can I make when this study is considered along with other available evidence? A. The recent ARISE trial4 of similar design and quality yielded similar findings. The early study by Rivers et al.1 had a higher mortality rate, was single-centred and had other possible confounding issues. The ProMISe trial,5 a third trial of this nature will supply further evidence on the use of EGDT for sepsis.
Should I change my practice because of these results? No. Both ProCESS, and ARISE showed overall mortality rates to be substantially lower than in the original Rivers study. This is possibly due to the surviving sepsis campaign generating increased awareness, diagnosis and early treatment of septic shock with appropriate antibiotics and fluid resuscitation. This would suggest that the ‘early’ part of EGDT is the important component, and that current day standard ‘accepted care’ of sepsis gave no worse outcome than goal-directed therapy. The surviving sepsis campaign intends to issue a statement based on the results of the three trials after they are published.
Should I audit my practice because of these results? Possibly. Central venous catheters (CVC) are associated with a degree of morbidity and therefore their use must be justified. Sole use of CVCs for monitoring ScvO2 could therefore be considered unnecessary and not best practice.
Selected outcomes of the three groups.
Outcome
Protocol-based EGDT
Protocol-based Standard therapy
Usual care
P
Mortality
60 days
92/439 (21%)
81/446 (18.2%)
86/456 (18.9%)
.83
90 days
129/405 (31.9%)
128/415 (30.8%)
139/412 (33.7%)
.66
New organ failure, 1 week
Cardiovascular
269/439(61.3%)
284/446 (63.7%)
256/456 (56.1%)
.06
Respiratory
165/434 (38%)
161/441 (36.5%)
146/451 (32.4%)
.19
Renal
12/382 (3.1%)
24/399 (6.0%)
11/397 (2.8%)
.04
Use of hospital resources
ICU admission
401 (91.3%)
381 (85.4%)
393 (86.2%)
.01
ICU length of stay (days)
5.1 ± 6.3
5.1 ± 7.1
4.7 ± 5.8
.63
Hospital stay (days)
11.1 ± 10
12.3 ± 12.1
11.3 ± 10.9
.25
Main intervention frequency in the three groups.
Interventions
Protocol-based EGDT
Protocol-based standard therapy
Usual care
P
Care process 0–72 h
Intravenous fluids (ml)
7253 ± 4605
8193 ± 4989
6633 ± 4560
<.0001
Vasopressor use
265 (6.4%)
273 (61.2%)
245 (53.7)
.05
Dobutamine use
41 (9.3%)
11 (2.5%)
13 (2.9)
<.0001
Blood transfusion
120 (27.3%)
107 (24%)
102 (22.4)
.22
Ventilation
159 (36.2%)
152 (34.1)
135 (29.6%)
.10
Fluid resuscitation volumes at various time points in the study (mls).
Protocol-based EGDT
Protocol-based Standard therapy
Usual care
P
Pre-randomisation
2254 ± 1472
2226 ± 1363
2083 ± 1405
.15
0–6 h
2805 ± 1957
3285 ± 1743
2279 ± 1881
<.0001
6–72 h
4458 ± 3878
4918 ± 4308
4354 ± 3882
.8
0–72 h
7253 ± 4605
8193 ± 4989
6633 ± 4560
<.0001
Average pH of subjects at different time points in each study group.
Protocol-based EGDT
Protocol-based standard therapy
Usual care
P
Pre-randomisation
7.33 ± 0.12
7.31 ± 0.13
7.34 ± 0.13
.06
6 h
7.31 ± 0.1
7.31 ± 0.1
7.34 ± 0.1
.02
24 h
7.34 ± 0.1
7.34 ± 0.1
7.36 ± 0.1
.02
48 h
7.36 ± 0.1
7.36 ± 0.1
7.38 ± 0.1
.36
72 h
7.38 ± 0.1
7.37 ± 0.1
7.38 ± 0.1
.50
Protocol for early goal-directed therapy (EGDT).
Protocol for standard care.
Footnotes
Appraised by:
George E Evetts MRCP FRCA, Speciality Trainee year 6, Anaesthesia & Intensive Care, Imperial College School of Anaesthsia
george.evetts@gmail.com
Kristina Birch MRCP FRCA FFICM, Consultant in Anaesthesia and Intensive Care Medicine, North Bristol NHS Trust
References
1.
RiversE. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl JMedi2001; 345: 1368–1377.
2.
JonesAE. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA2010; 303: 739–746.
3.
ShoemakerWC. Sequence of physiologic patterns in surgical septic shock. Crit Care Med1993; 21: 1876–1889.
4.
The ARISE Investigators. Goal-directed resuscitation for patients with early septic shock. N Engl J Med2014; 371(16): 1496–1506.
5.
PowerGS. The protocolised management in sepsis (ProMISe) trial statistical analysis plan. Crit Care Resusc2013; 15: 311–317.