
Abstract
A novel synthetic haemabsorption column (Cytosorb™) has recently become commercially available. We describe its use in patients with overwhelming sepsis and consider the experience and evidence supporting its use. While Cytosorb haemabsorption is mechanistically distinct from other extracorporeal therapies in sepsis and appears effective in reducing inflammatory cytokines during sepsis, much of the basic science and clinical benefits remain unclear. Significant interactions including removal of antibiotics may be harmful and require further study. Suggestions for future research and how Cytosorb™ could be incorporated into practice are provided.
Case 1
A previously healthy patient in the 40 s was admitted with acute septic shock and multiple organ failure. Clinically and radiographically the cause was severe community acquired pneumonia with a lobar consolidative pattern and positive urine antigen testing for Streptococcus pneumoniae. The patient developed rapidly worsening multiple organ (cardiovascular, respiratory and renal) failure with prominent haemodynamic instability requiring high-dose infusions of norepinephrine, dobutamine and vasopressin and still only achieving systolic arterial pressures of 60–70 mm Hg. Bedside echocardiography demonstrated severe, global left ventricular dilatation and systolic failure with ejection fraction approximately 20%.
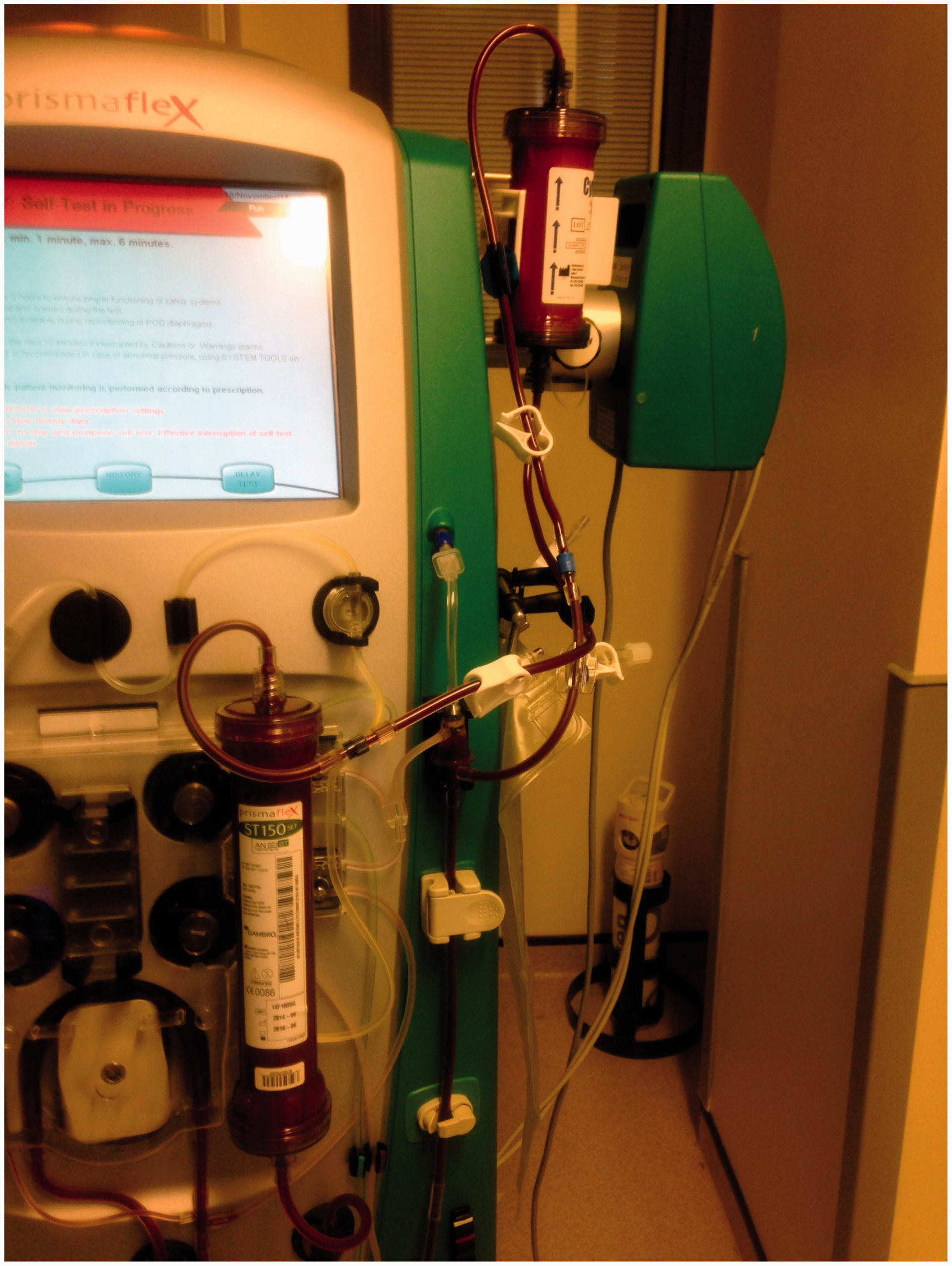
The patient was receiving maximal supportive care including continuous veno-venous haemodiafiltration (CVVHDF) for oligo-anuric acute renal failure and, in the face of refractory septic shock, the decision was made to add the Cytotosorb™ haemabsorption column into the return limb of the circuit (see Figures 1 and 2). He received our unit standard 1.8 l h−1 (approximately 25 ml kg−1 h−1) CVVHDF combined with blood pump speeds 200–300 ml min−1 as vascular access tolerated.
The Cytosorb column in use. The Cytosorb column incorporated into the return limb of a Prismaflex ST150 CVVHDF circuit.
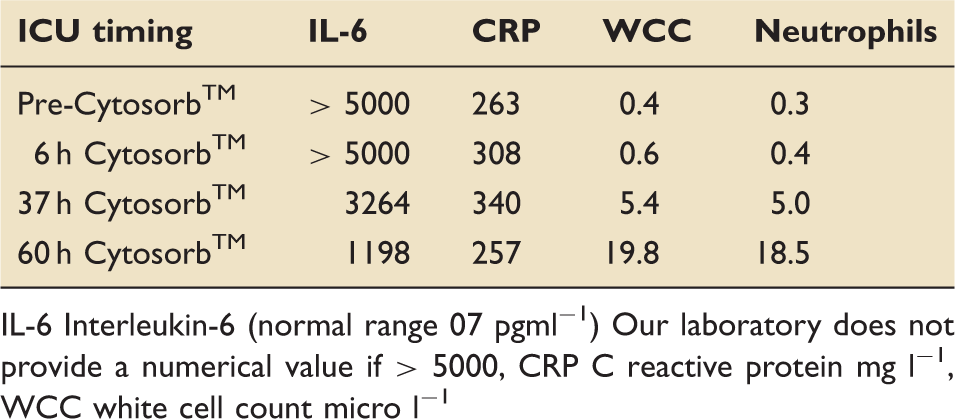
IL-6 Interleukin-6 (normal range 0–7 pgml−1) Our laboratory does not provide a numerical value if > 5000, CRP C reactive protein mg l−1, WCC white cell count micro l−1
At 60 h, the patient was no longer uraemic and CVVHDF was stopped as the filter clotted. Considering the marked improvement in haemodynamic condition and our lack of experience with Cytosorb™, therapy was discontinued; this was the same column throughout therapy without change.
The subsequent course was complicated by prolonged respiratory support via tracheostomy due to critical illness polyneuro(myo)pathy to ICU acquired weakness, but the patient was discharged to the ward and ultimately home in good health.
Case 2
A young patient in their 20s with a history of illicit intravenous drug abuse was admitted because of apparent community acquired pneumonia. Endocarditis was suspected on the basis of history, having been injecting low quality illicit drugs, probably contaminated with brick dust as a bulking agent. Transoesophageal echocardiography (TOE) confirmed a large vegetation attached at the ostium of the coronary sinus adjacent to the septal leaflet of the tricuspid valve, but with a competent valve. No organism was identified on blood cultures but the patient was receiving antimicrobial therapy for pneumonia when sampled.
The patient was managed supportively with mechanical ventilation and antibiotics but progressed to septic shock and acute renal failure requiring CVVHDF to control rising potassium. Vasoactive support was progressively increasing so the decision was made to include the Cytosorb™ column in the return limb of the Prismaflex circuit as described above.
Over the course of the next 6 h the clinical condition improved rapidly with reducing vasoactive infusions and ultimately the patient’s trachea was extubated at 72 h. The patient’s course was complicated by tricuspid regurgitation secondary to vegetations which ultimately required a tricuspid prosthetic valve replacement in another hospital. The patient recovered well after surgery and has been discharged home.
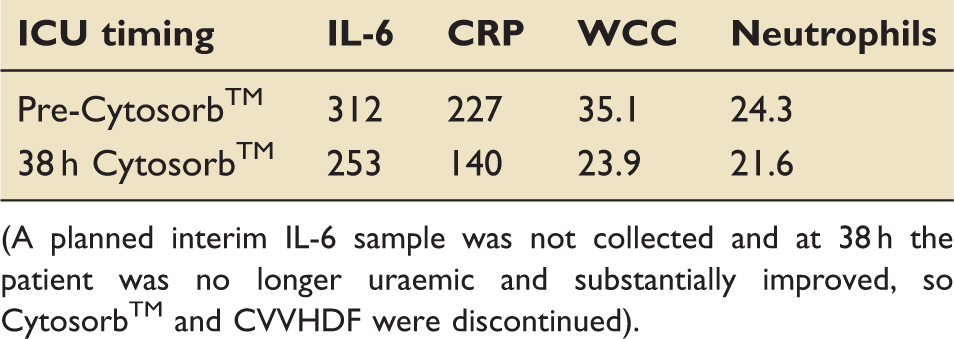
(A planned interim IL-6 sample was not collected and at 38 h the patient was no longer uraemic and substantially improved, so Cytosorb™ and CVVHDF were discontinued).
Discussion
These case reports appear to be among the first published uses of Cytosorb™ as an adjunct in managing sepsis. As Cytosorb™ is now commercially available in Europe, its introduction into clinical practice must occur in a controlled fashion, informed by clinical and surrogate outcomes.
Cytosorb (CytoSorbents Corporation; Monmouth Junction, NJ) is a novel synthetic haemabsorption column, which received CE approval in 2011 for the management of inflammatory conditions with elevated cytokine levels 1 and is currently the only CE-approved extracorporeal device marketed for inflammatory mediator removal. Cytosorb is currently marketed across the spectrum of inflammation including sepsis, cardiopulmonary bypass, pancreatitis and burns. 2
There is currently limited published data on the basic science and clinical experience of the device although CE marking centered upon (unpublished) findings from a small European trial of patients with acute respiratory distress syndrome (ARDS) complicating sepsis, where interleukin 6 (IL-6) blood concentrations in Cytosorb-treated patients were almost halved (49.1%) vs. standard care. To date, no clinical outcomes from this study have been published although promotional data suggest Cystosorb-treated patients had less deaths (0 vs. 62.5% control) and fewer patients required mechanical ventilation (33 vs. 88%) at 28 days. 3 Manufacturer data also suggest over 300 patient treatments to date with good tolerability and safety.2,3
The Cytosorb device is a relatively simple haemabsorption column consisting of a suspended column of beads of highly porous resin (polystyrene divinylbenzene PSDVB) covered with a biocompatible polyvinylpyrrolidone coating.
4
The beads are 300–600 µm in diameter with density 1.02 g cm–3 and porosity 67.7%. The bead pores are 8–50 Angstrom units allowing adsorption for smaller molecules (< 50 kDa) and excluding larger proteins, e.g. albumin (70 kDa) or fibrinogen (340 kDa). Figure 3 demonstrates the appearance of the beads with electron microscopy of the inner pore structure.
Macroscopic appearance of Cytosorb beads and electron microscopy of heavily pore covered structure.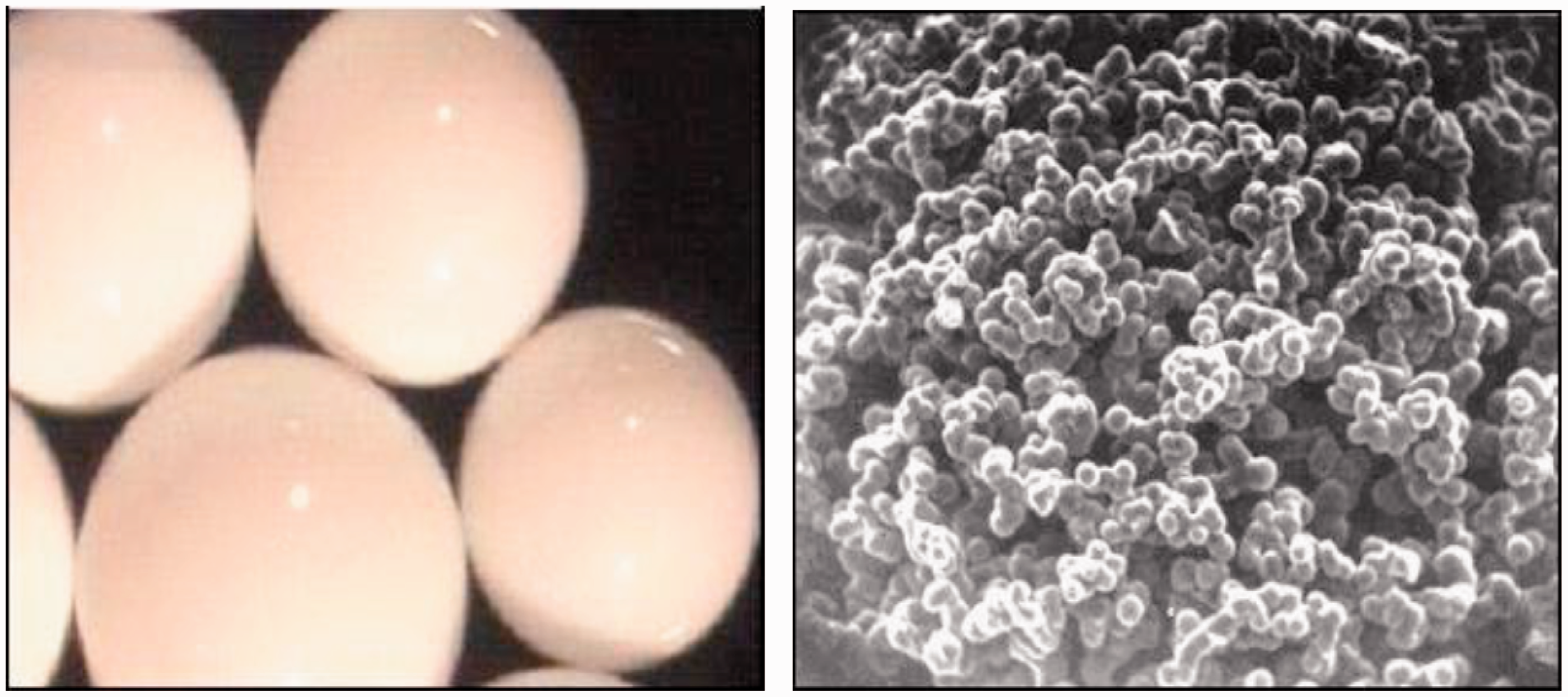
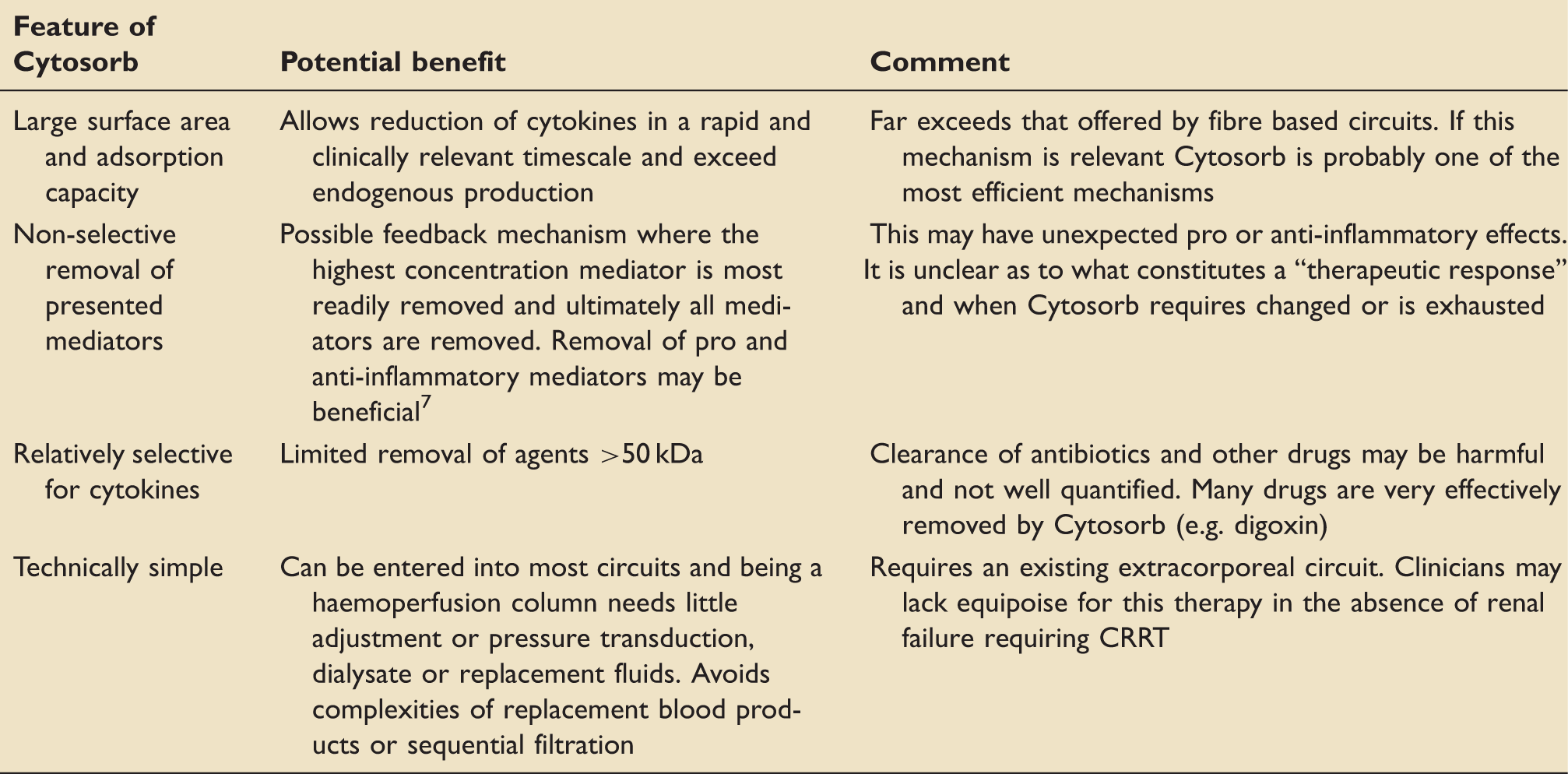
Consequently, while the Cytosorb column has an internal volume of 330 ml (equivalent to a standard carbonated drink can), the available surface area for mediator absorption is 850 m2g–1 (several football pitches equivalent) and far exceeds the surface area available from fibre technology as might be used in a standard diafiltration circuit (typically 0.5–2 m2g–1).
Basic science research describes refinement of bead size and structure to avoid haemolysis 4 while optimizing mediator absorption and in rat models achieved 50% removal of IL-6, IL-10 and TNF in septic rats at 1 h. 5
It is of note while IL-6 and Il-10 are relatively easily cleared, the TNF-alpha trimer (51 kDa composed of three units) clearance is significantly less. In a small volume horse blood model the absorption at 4 h was 100% for IL-1 and IL-8, 87% IL-6, 85% IL-10 and 55% TNF-alpha although in human use the reported reductions are considerably less and < 50%. 3
The sepsis syndromes are among the most common and lethal examples of uncontrolled inflammation and systemic inflammatory response syndrome (SIRS), and elevated levels of IL6 and IL-1 are associated with adverse survival. 6 However, the interplay of cytokine mediators is complex and some workers have demonstrated, perhaps counter intuitively, that persistently elevated “anti-inflammatory” mediators (e.g. IL-10) carry a worse prognosis than elevated “pro-inflammatory” mediators (e.g. IL-6). 7 The poorly regulated inflammatory “storm” of sepsis has been reviewed extensively elsewhere.8,9 Despite decades of basic science and clinical research, it remains unclear how absolute or relative concentrations, or timing of interactions of inflammatory mediators effects the evolution of inflammation and ultimately how manipulation of these mediators may become therapeutic options. Furthermore, complex interactions between inflammation, endogenous anti-inflammatory processes, coagulation and platelets, and the vascular glycocalyx suggest manipulating cytokines may only offer a partial therapy. It is a recurring theme that most “anti-inflammatory” therapies have failed in robust evaluation despite encouraging initial results including drotrecogin alfa, 10 tifacogin, 11 high and low dose corticosteroids,12–14 intravenous immunoglobulin, 15 antithrombin III, 16 statins17,18 and most workers feel our understanding of manipulating inflammation has moved beyond the “magic bullet” single intervention.
Intriguingly, murine anti-TNF (afelimomab) demonstrated small increases in survival in patients with elevated IL-6. 19 The accompanying editorial emphasizes appropriate patient selection to ensure therapeutic efficacy (in this case IL-6 levels) and it seems misplaced to expect all patients with “elevated cytokines” to benefit from any given anti-inflammatory therapy including Cytosorb™. 20
Conventional extracorporeal therapies in sepsis offering “blood purification” have been generally disappointing. A recent systematic review of high-volume CVVHDF in sepsis suggest extracorporeal therapies in acute kidney injury (AKI) should focus on alternatives to diafiltration and that the technique is mechanistically unlikely to deliver improved outcomes, beyond managing uraemia and acute kidney failure. 21 Most mediator clearance during CVVHDF is an adsorption phenomenon with relatively little convective or diffusive clearance 22 and consequently, the relatively low fibre density and high endogenous turnover mean most commercial CVVHDF circuits achieve modest and transient reductions in cytokines, ultimately becoming saturated.
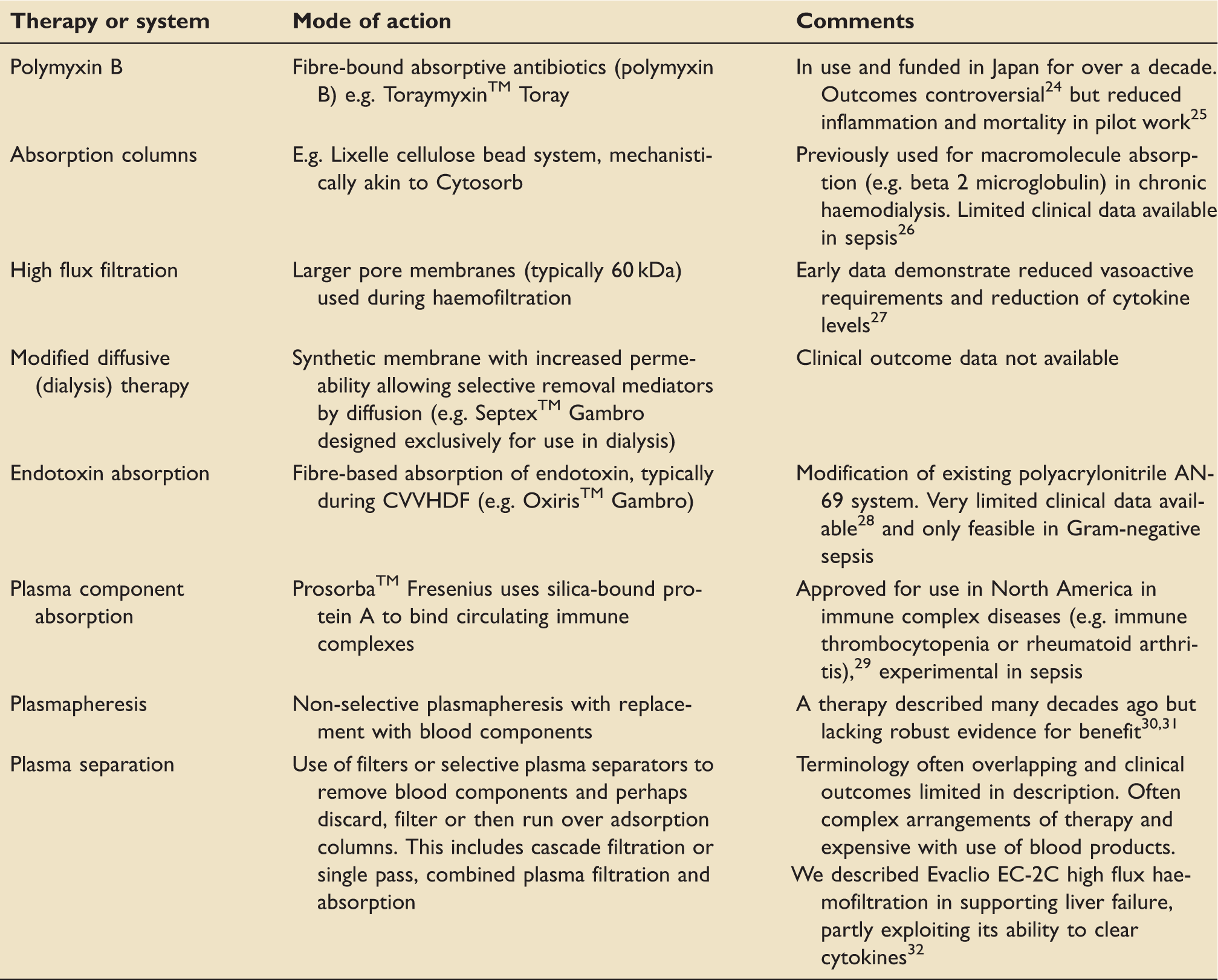
Extracorporeal therapies for sepsis, beyond the CVVHDF circuit, are relatively limited, certainly in the UK, and some alternative examples to Cytosorb™ are considered below and have been reviewed elsewhere. 23
As UK-trained clinicians this has been our first clinical experience using assays of IL-6 during sepsis, and anecdotally this is typical. Neither case demonstrated a rapid response during Cytosorb™ and the pattern was one of “gradual improvement” over hours; definitively ascribing causality is premature. The timescale for IL-6 results in Derby was several days and consequently no management decisions were based upon IL-6 and in all other aspects “standard care” was delivered. C reactive protein (25 kDa), white cells and temperature all appeared to lag behind IL-6 responses by 24–48 h, the significance of which is unclear. We do not routinely measure procalcitonin (13 kDa) but kinetics use of this marker or C reactive protein in tracking therapeutic success during CVVHDF and Cytosorb may be significantly altered and requires evaluation.
Our two cases demonstrate very similar clinical syndromes (i.e. overwhelming sepsis) with subsequent multiple organ failure but markedly different IL-6 profiles, i.e. one peak concentration in excess of 5000 pgml−1 and one in 300–400 pgml−1 range. Whilst the latter remains grossly elevated (normal range < 7 pg ml−1) it was associated with an identical clinical picture and reinforces the concept that absolute cytokine levels may not be the most important factor and relative concentrations or timing may be equally important. Defining the indications for Cytosorb™ based upon concentrations of cytokines is currently unfounded and raises the question whether patients with lower levels of Il-6 are likely to be Cytosorb™ “non-responders”. Currently, the indications for therapy remain “elevated cytokines” and this risks large costs and potential adverse risk/benefit profiles. Furthermore, the column has a finite lifespan and will become saturated; it is unclear how long a column can last and when it should be changed with case reports citing 6 h and the manufacturer suggesting 24–36 h. Our own further experience has been to pragmatically replace Cytosorb™ columns after 24 hours, or when CVVHDF filter set requires changing. Whether a saturated column can be identified by a failure to clear IL-6 is unknown. Furthermore, if a CVVHDF circuit fails in use this can be changed relatively easily at under £100; loss of Cytosorb™ reflects closer to £1000 and would absolutely require a stable and established extracorporeal circuit to be viable.
If the Cytosorb is to be evaluated with equipoise in clinical trials these data must be complete and recognise complex drug distribution and elimination kinetics during CVVHDF. The absorption of vasoactives by Cytosorb, and in particular catecholamines, is theoretically low because of polar hydroxyl moieties, despite their small molecular size (personal communication, David Scullard, Linc Medical) but this requires quantitative assessment. In principle, most albumin-bound substances will bind to Cytosorb. While this could theoretically be attractive (e.g. removal of bilirubin in liver failure) and indeed while the beads share some similarity to other extracorporeal systems (e.g. molecular adsorbent recirculating system MARS™, Gambro), the effects here could also be harmful, e.g. removing hormones and nutrients.
A relatively unexplored application is the use of Cytosorb in treating drug toxicity where in vitro work suggests good rates of clearance of several drugs and it could prove an alternative to charcoal haemoperfusion in the future. While human model data remain lacking, in principle the removal of some drugs is potentially highly efficient and could be useful, e.g. in overdose. Drugs with >80% removal in an in vitro model after 120 min include vancomycin, teicoplanin, digoxin, tacrolimus, valproate, phenobarbital, carbamazepine and phenytoin and 60% removal of cyclosporine. 34
The Cytosorb column currently costs approximately £1000 although this will reflect commercial usage. It is not currently included in UK critical care commissioning agreements.
A suggested way forward with Cytosorb
Currently, the Cytosorb column has CE marking but is not Food and Drug Administration (FDA)-approved in the United States of America and its use is largely restricted to Europe. Germany has perhaps the greatest anecdotal experiences but the European Sepsis Trial remains unpublished. 3 Many of the challenges in safely and effectively introducing Cytosorb into practice are common to all new medical technologies.
Our use of the device has been on a compassionate basis where patients have failed to respond to standard care but this carries inherent bias in selecting unwell patients later in their disease who are less likely to survive and negate a potential useful therapeutic effect. Conversely, routine use risks adverse outcomes and the impact of an extracorporeal circuit and may be directly harmful. It is a relatively expensive therapy. We feel unable, based on our experiences, to form an opinion over risk vs. benefit with the device and believe most clinicians will reach this point.
We believe it is premature to run a definitive trial and that further research is needed before this is attempted. Fundamental issues requiring addressing include
Indications, contraindications for use. It remains unclear whether elevated biomarkers (e.g. IL-6) are sufficient to identify likely responders or whether clinical features or disease acuity (e.g. APACHE II) are better. Conversely, whether benefit is related to absolute IL-6 level is unclear, e.g. does peak level > 5000 suggest better therapeutic efficacy than 300? How is therapeutic efficacy defined? It is not adequate to simply demonstrate reduction in biomarkers and this must be linked to robust clinical endpoints from other sepsis studies including mortality, organ support requirements, length of stay.10–14 When should Cytosorb therapy stop? It is unknown whether a falling biomarker indicates success in stopping inflammation and the improvement may be sustained by ongoing care (e.g. antibiotics) or whether markers (e.g. IL-6) need reducing to very low levels. The latter approach might be harmful in inducing immunosuppression and possible later adverse events (e.g. secondary infection).
14
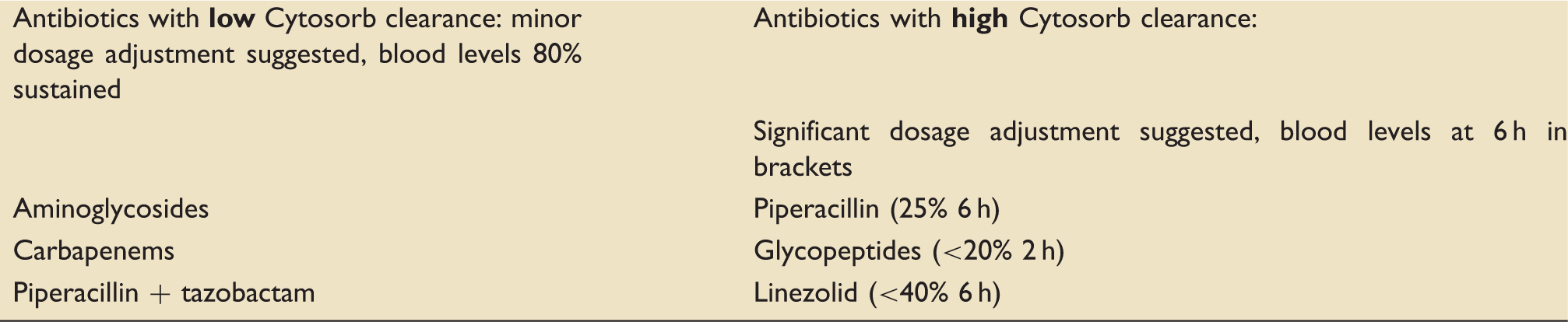
If clinical endpoints are used which ones, e.g. is success falling vasoactive infusions or their discontinuation? Should Cytosorb be used as an independent extracorporeal therapy in the absence of a need for such a therapy? All treated patients in Derby have also had AKI requiring CVVHDF; is it beneficial to commence therapy and indeed could Cytosorb prevent renal failure? Does Cytosorb therapy reduce or extend CVVHDF filter set lifespan, and does adsorbance column position in the circuit e.g. pre- or post- filter affect performance of Cytosorb or filter? Unintended consequences. Cystosorb™ therapy has many implications common to an extracorporeal circuit but also affects drug kinetics (especially antibiotics) and will affect albumin-bound substances, e.g. hormones or toxins (e.g. bilirubin) in largely unstudied ways. This may demonstrate unwanted effects, e.g. sub-therapeutic antibiotic concentrations but could also open the way to novel applications, e.g. support in liver failure or treating drug toxicity demands further evaluation.
The evaluation and use of Cytosorb illustrate the discrepancies between the approval process for drugs and medical devices and it is unlikely a drug with such potent and multiple modes of action would have got to market on the basis of an unpublished cohort study, and post-marketing surveillance would be much more intense and robust. Pragmatically we suggest
Clinicians engage with the manufacturer registry and submit their data. All uses of the device should be recorded by clinicians and representative data kept to inform future investigations. Pressure is placed on the manufacturer to make the findings of European Sepsis Trial available and ideally published in peer reviewed journal and engagement continued calling for all registry and trial data to be fully disclosed. Full compliance with local incident reporting and national surveillance schemes (e.g. the UK MHRA). A cohort study is undertaken to define basic science (e.g. IL-6 profiles and correlation to clinical events) typical set duration and safety. A pilot study is run using a theoretical primary end point, i.e. clearance of IL-6 and “proof of principle”.
Once these data are available, it should be possible to determine whether equipoise is appropriate 35 and if an adequately powered prospective, randomized clinical trial should be undertaken utilizing specific clinical endpoints in conjunction with biomarkers, once they have been more completely evaluated and described. What is not a sustainable future is for an invasively delivered therapy that significantly interferes with the inflammatory process of sepsis to be commercially available and applied to patients with minimal robust and published data on efficacy or safety.
Footnotes
Acknowledgement
The authors thank Dr Julia Forsythe, Consultant Biochemist, Royal Derby Hospital (support IL-6 assays).
Consent
Both patients were treated acutely with the assent of next of kin. Upon recovery, both patients provided signed consent for publication in peer reviewed journal, discussed in the presence of their next of kin.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The UK distributor (Linc Medical) supplied the Cytosorb columns used in these patients and provided technical support during their use (David Scullard). Our unit has since purchased Cytosorb columns for clinical use at retail prices. The authors have no prior experience with Cytosorb, and received no financial support, directly or otherwise from Linc Medical or Cytosorbents. In collecting scientific material for this manuscript, discussions have been held with Linc Medical and representatives of Cytosorb including Dr Philip Chan, Medical Director.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.