The use of vasopressin and steroids in addition to epinephrine during the resuscitation of patients suffering an in-hospital cardiac arrest is associated with an improved neurological outcome. Level of evidence: 1B (CEBM, RCT of good quality)
Appraised by: Johan Victor Rehnberg and Patrick Nee
Citation: Mentzelopoulos SD, Malachias S, Chamos S, et al. Vasopressin, steroids, and epinephrine and neurologically favorable survival after in-hospital cardiac arrest. JAMA 2013; 310:270–279.
Lead author: Spiros D Mentzelopoulis, smentzelopoulis@yahoo.com
Intervention and comparison: For the first five cycles of cardiopulmonary resuscitation (CPR), patients received either epinephrine/adrenaline (1 mg) with vasopressin (20 U) or epinephrine/adrenaline with saline placebo. Patients receiving vasopressin were also given a single dose of methylprednisolone (40 mg) during the first cycle, whilst controls received saline placebo. Patients with post-resuscitation shock at 4 h received stress-dose hydrocortisone (300 mg/d for ≤ 7 days and gradual taper) in the VSE (vasopressor-steroid-epinephrine) group or saline placebo in controls.
Outcomes: Return of spontaneous circulation (ROSC) for 20 min or longer, and survival to hospital discharge with favourable neurological recovery (Glasgow-Pittsburgh Cerebral Performance Category [GPCPC] score of 1 or 2).
Study design:
A multi-centre prospective, randomised, double-blind placebo-controlled trial.
Study patients:
Eligible: Adult patients suffering in-hospital, vasopressor-requiring cardiac arrest resuscitated according to European Resuscitation Council guidelines (2005).
Included: 268 patients.
Exclusion: Age younger than 18 years, terminal illness (i.e. life expectancy < 6 weeks) or do-not-resuscitate status, cardiac arrest due to exsanguination, cardiac arrest before hospital admission, treatment with intravenous steroids before arrest, previous enrolment in or exclusion from the same study.
Intervention group: 130 patients (146 randomised; 16 did not receive intervention as ROSC confirmed before study drug administered). Epinephrine/adrenaline (1 mg) plus vasopressin (20 IU), in pre-filled syringes, was administered between each cycle of CPR (cycle duration ∼ 3 min). Methylprednisolone (40 mg) was administered separately during the first cycle of CPR. Patients with post-resuscitation shock (mean arterial pressure, MAP, < 70) at 4 h received hydrocortisone in 100 ml of normal saline once daily (300 mg until the day of vasopressor cessation or day 8 post-arrest, and then dose reduced by 100 mg daily).
Control group: 138 patients (154 randomised; 16 did not receive intervention). Epinephrine/adrenaline (1 mg) plus saline placebo between each cycle of CPR, with saline placebo instead of methylprednislone during the first cycle of CPR. Patients with post-resuscitation shock at 4 h received 100 ml of normal saline once daily (any prescription of open-label hydrocortisone cancelled the experimental treatment).
Results:
Heterogeneity between the three centres was low for ROSC and neurologically favourable survival (I2 = 0.16 and 0, respectively).
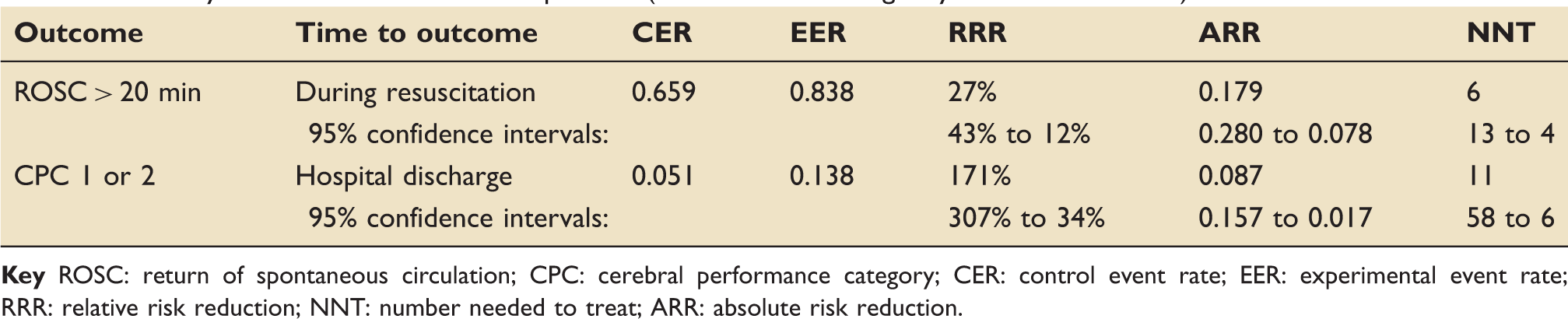
The VSE group had higher probability of ROSC for 20 min or longer and was more likely to survive to hospital discharge with a favourable neurological recovery (Table 1).
Primary outcome measures for all patients (ROSC and neurologically favourable survival).
Outcome
Time to outcome
CER
EER
RRR
ARR
NNT
ROSC > 20 min
During resuscitation
0.659
0.838
27%
0.179
6
95% confidence intervals:
43% to 12%
0.280 to 0.078
13 to 4
CPC 1 or 2
Hospital discharge
0.051
0.138
171%
0.087
11
95% confidence intervals:
307% to 34%
0.157 to 0.017
58 to 6
Key ROSC: return of spontaneous circulation; CPC: cerebral performance category; CER: control event rate; EER: experimental event rate; RRR: relative risk reduction; NNT: number needed to treat; ARR: absolute risk reduction.
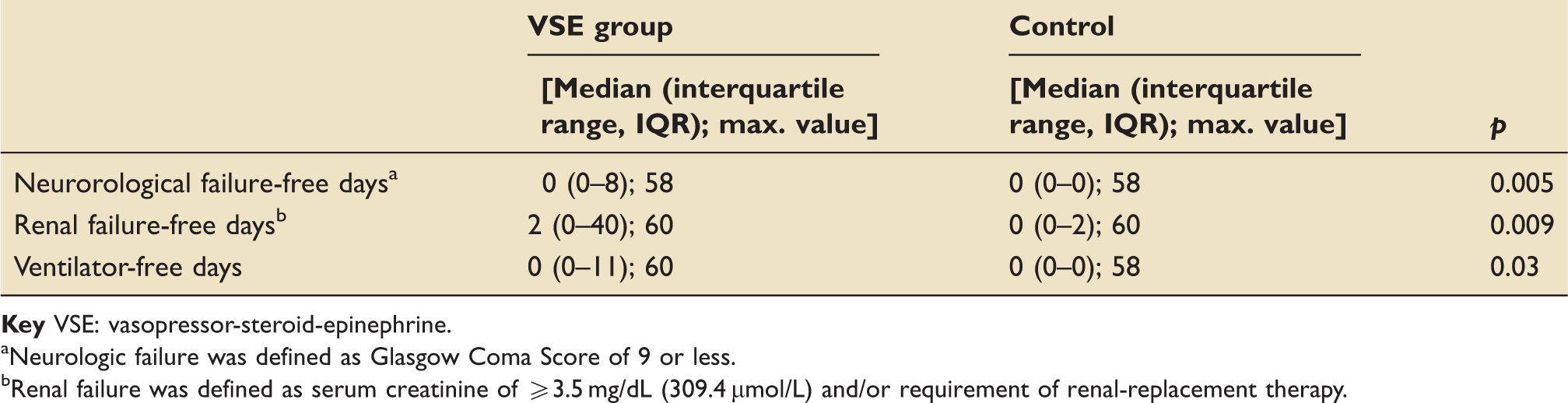
Compared with controls, VSE patients had significantly more neurological and renal failure-free days and more ventilator-free days (Table 2), as well as improved haemodynamics and central venous oxygen saturations.
Organ failure-free days in post-resuscitation shock groups.
Neurologic failure was defined as Glasgow Coma Score of 9 or less.
Renal failure was defined as serum creatinine of ≥3.5 mg/dL (309.4 µmol/L) and/or requirement of renal-replacement therapy.
At 4-h post-ROSC, 76 of 86 surviving VSE patients and 73 of 76 surviving controls had post-resuscitation shock. When compared to shocked control patients who received placebo, shocked VSE patients who received stress-dose hydrocortisone had a higher probability of survival to hospital discharge with a favourable neurological recovery (Table 3).
Neurological outcome in survivors still alive at 4 h with post-resuscitation shock; defined as new post-arrest circulatory failure or post-arrest need for 50% or greater increase in any vasopressor/inotropic support targeted to MAP > 70 mmHg.
Outcome
Time to outcome
CER
EER
RRR
ARR
NNT
CPC 1 or 2
Hospital discharge
0.082
0.211
157%
0.129
8
95% confidence intervals:
293% to 22%
0.240 to 0.018
56 to 4
Key VSE group received stress-dose hydrocortisone and controls received saline placebo. MAP: mean arterial pressure; CER: control event rate; EER: experimental event rate; RRR: relative risk reduction; NNT: number needed to treat; ARR: absolute risk reduction.
EBM questions:
1. Do the methods allow accurate testing of the hypothesis?Yes. This was a well-designed, double-blinded RCT.
2. Do the statistical tests correctly test the results to allow differentiation of statistically significant result?Yes.
3. Are the conclusions valid in light of the results?Yes. This was appropriately powered for the primary outcomes (based on estimated survival benefit from 4% to 15%; the preliminary study showed a survival benefit for favourable neurological recovery of 15% compared with 4% in controls), and although there was more than one primary outcome – increasing the chances of a single positive result – both were positive. However, as the VSE and post-arrest shock/stress-dose hydrocortisone protocol was applied as a bundle, it is not possible to quantify the effect of any individual component on survival to discharge with favourable neurological recovery.
4. Did results get omitted, and why?No.
5. Did the authors suggest areas of further research?Yes. The specific effect of post-arrest hydrocortisone alone on neurologically intact survival.1 Although studies looking at the effect of corticosteroids on organ dysfunction in sepsis suggest potential for benefit in the post-arrest syndrome, this and the preliminary study by the same group are the only human randomised trials investigating corticosteroid use after ROSC. Further work, possibly using multi-arm intervention groups, is required to differentiate the relative effects of each part of the VSE bindle on survival.
6. Did they make any recommendations based on the results and were they appropriate?No. No specific recommendations were made.
7. Is the study relevant to my clinical practice?Yes. But only in selected patients (i.e. adult in-hospital cardiac arrest and refractory post-resuscitation shock at 4 h). Notably, there were no recorded defibrillations in the study group despite nearly 17% of patients in each arm having VF/VT, suggesting that resuscitation must have deviated from current guidelines in at least some cases.
8. What level of evidence does this study represent?1B. Individual RCT with narrow confidence intervals.
9. What grade of recommendations can I make on this result alone?B. Extrapolated from Level 1 evidence.
10. What grade of recommendations can I make when this study is considered along with other available evidence?B. The only other study looking at this combined treatment bundle is the preliminary single-centre RCT conducted by the same group (2009).2
11. Should I change my practice because of these results?Maybe. Ideally these results should be validated by another group as well as studies to look at the individual effects of each component of the VSE protocol.
12. Should I audit my current practice because of these results?No.
Footnotes
References
1.
Mentzelopoulos S, Malachias S, Chamos C, et al. Vasopressin, steroids, and epinephrine and neurologically favorable survival after in-hospital cardiac arrest: a randomised clinical trial. JAMA 2013; 310: 270–279.
2.
MentzelopoulosSDZakynthinosSGTzoufiM. Vasopressin, epinephrine, and corticosteroids for in-hospital cardiac arrest. Arch Intern Med2009; 169: 15–24.