
Abstract
We wish to report two issues that we recently identified following the insertion of a Bivona® (Smiths Medical, Ashford, UK) tracheostomy tube which developed recurrent leakage due to cuff deflation. In the first instance, the pilot balloon and cuff were both slowly deflating and required repeated re-inflation. In the second instance (with the same tube), the pilot balloon pressure was elevated, but the cuff continued to have a sizeable leak. On removal and examination of the tube, no structural damage was noted, but the cause for both incidents was identified.
The Bivona tracheostomy tube was surgically inserted, and the cuff balloon was initially inflated with air and a good seal was achieved. However, we found a gradual and consistent loss of cuff pressure leading to a loss of tidal volume. The cuff was then re-inflated with air via the pilot balloon and although this resolved the issue temporarily, the cuff leak recurred and the cuff pressure was checked and indicated to be less than 20 cmH2O. Assuming this could be due to tube migration, the adjustable flange clip was released and the tube was inserted 1 cm further down the stoma site and the clip was reconnected to its position.
The cuff was inflated with air; however, this manoeuvre did not resolve the issue of air leak; examination of the cuff pressure showed a pressure of between 80 and 90 cmH2O.
The Bivona tracheostomy tube was changed to a conventional size 9.0® Portex (Smiths Medical, Ashford, UK) tube and ventilation improved. Following the removal of the Bivona tracheostomy tube, we had a thorough examination of the tube and found no structural defect or damage to the tube. However, we did find the reasons for the initial cuff leak and the unexpected high cuff pressure.
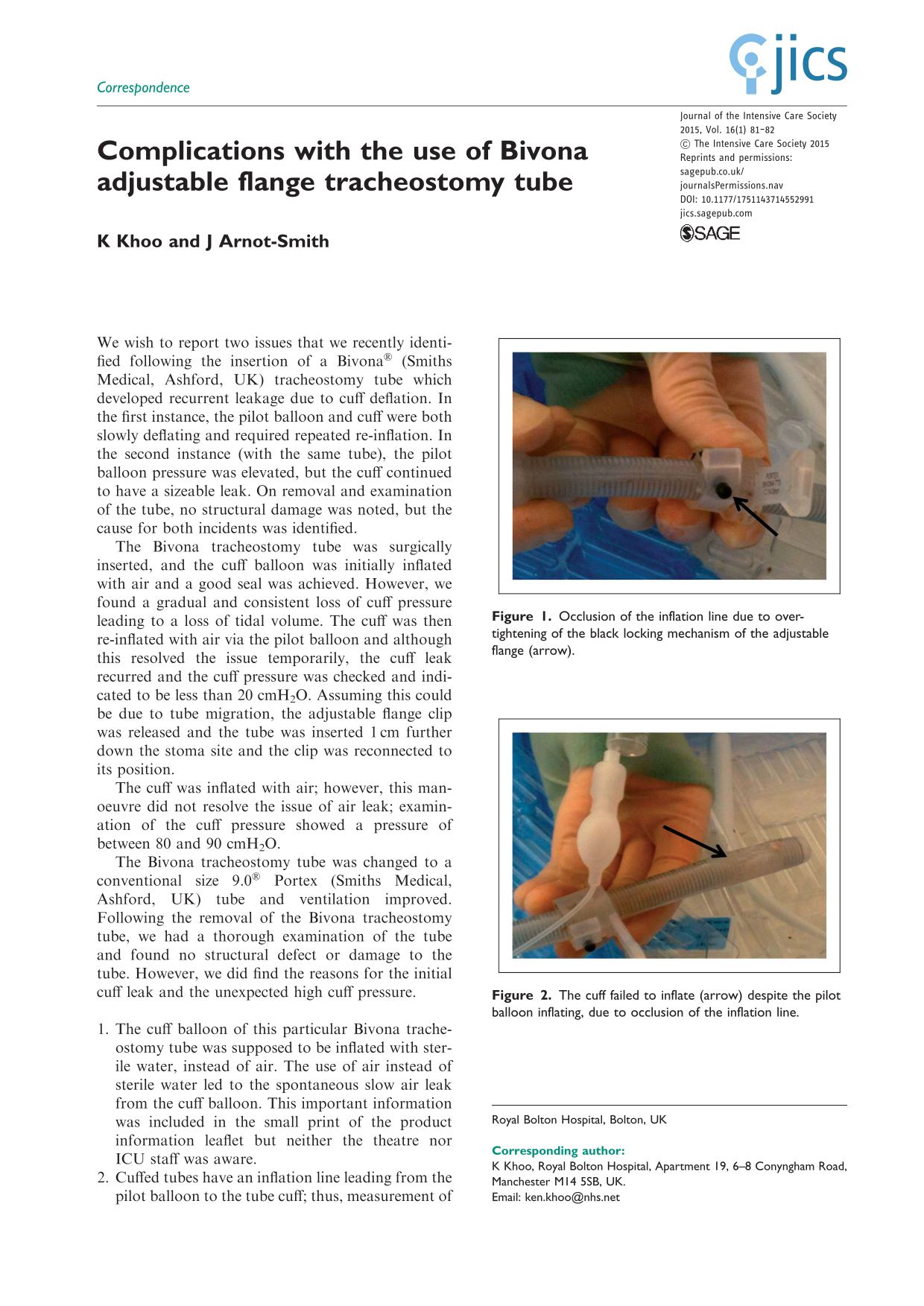
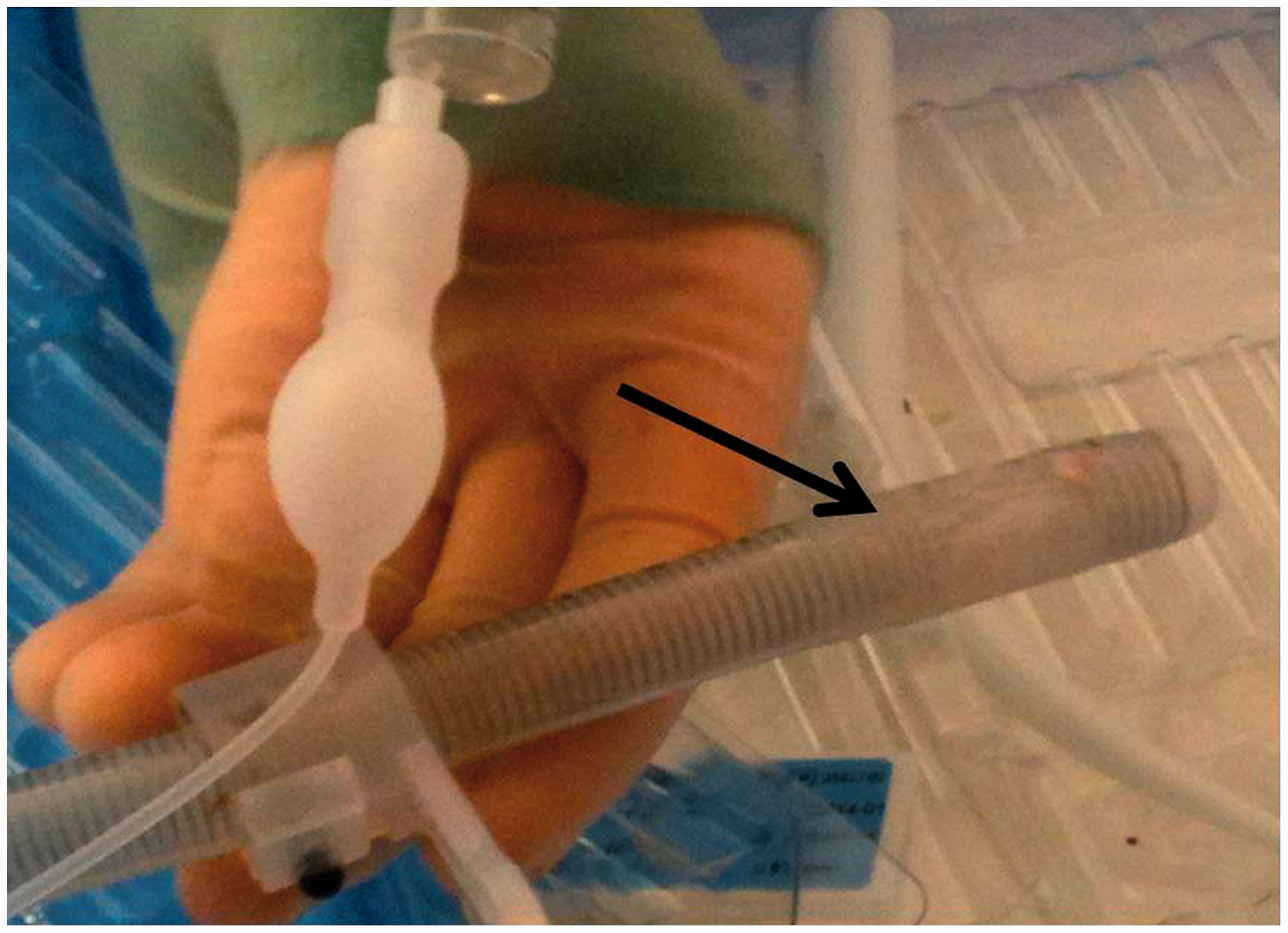
The cuff balloon of this particular Bivona tracheostomy tube was supposed to be inflated with sterile water, instead of air. The use of air instead of sterile water led to the spontaneous slow air leak from the cuff balloon. This important information was included in the small print of the product information leaflet but neither the theatre nor ICU staff was aware. Cuffed tubes have an inflation line leading from the pilot balloon to the tube cuff; thus, measurement of pressure in the pilot balloon should reflect the pressure in the cuff. The adjustable flange allows the flange to be adjusted up or down the shaft; we identified that inadvertent tightening can result in occlusion of the inflation line which can prevent cuff inflation despite high pressure readings being measured from the pilot balloon (Figure 1 and 2). This was most easily reproducible when the black locking mechanism was located directly over the inflation line.
There are a variety of adjustable flange tracheostomy tubes from different manufacturers in the market; some tracheostomy tubes use air for cuff inflation while others use sterile water. Our case highlights the importance of being vigilant and familiarising staff with the types of tubes used in their local hospital. It also highlights that adjusting the flange tracheostomy tubes such as these may cause problems with the locking mechanism, leading to occlusion of the inflation line, which runs along the outer tube shaft. This could lead to cuff balloon inflation failure and problems associated with it.
Occlusion of the inflation line due to over-tightening of the black locking mechanism of the adjustable flange (arrow). The cuff failed to inflate (arrow) despite the pilot balloon inflating, due to occlusion of the inflation line.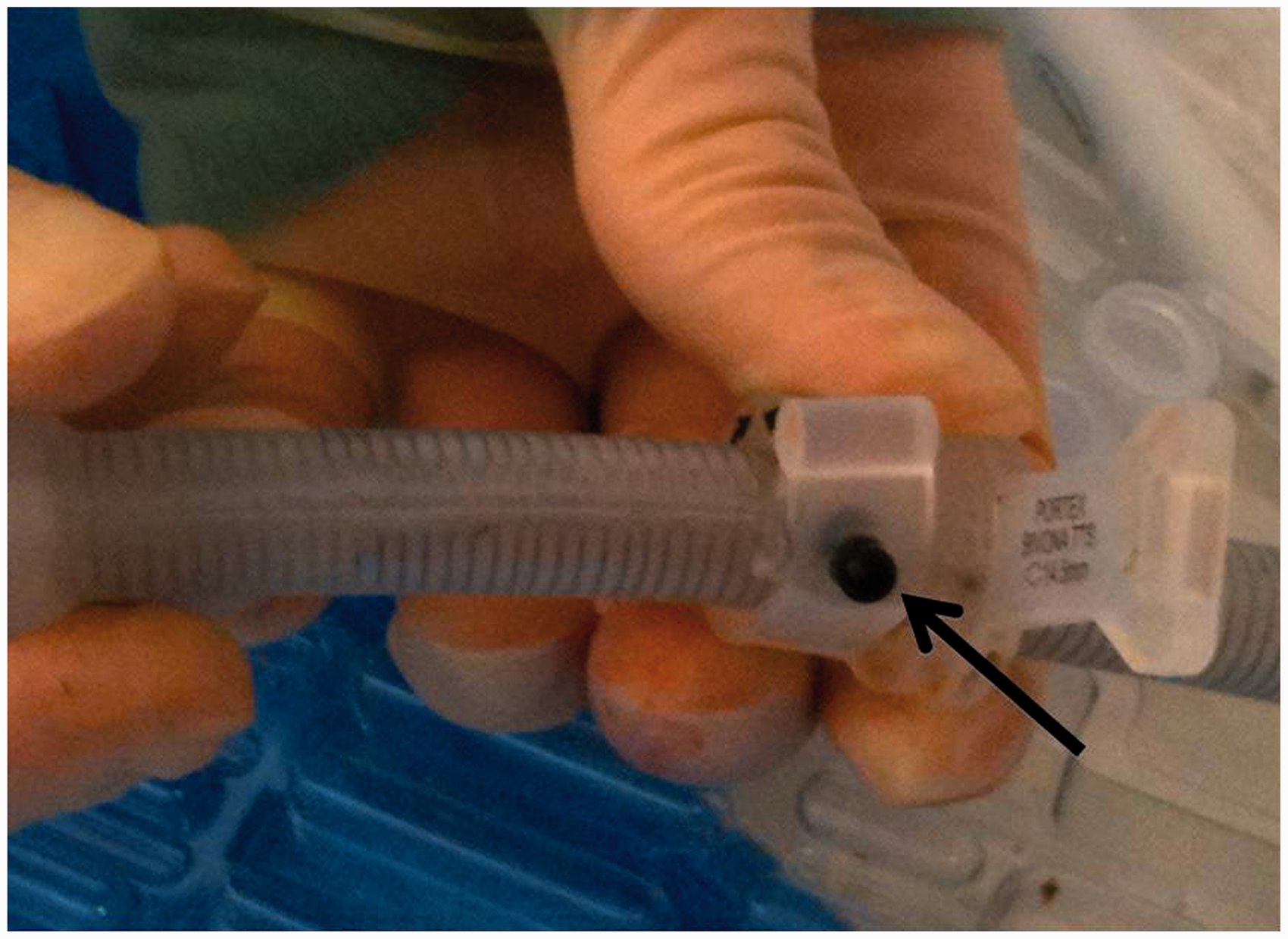
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.