
Abstract
This study explored operating theatre nurses’ experiences of receiving feedback on intraoperatively acquired positioning-related injuries and organisational factors influencing these processes. A descriptive cross-sectional web-based survey was completed by 57 Swedish operating theatre nurses using a study-specific questionnaire grounded in patient-safety frameworks. Most respondents had encountered positioning-related injuries, yet structured feedback was uncommon: over half received feedback only occasionally, and one-third never received any. When incidents were reported, feedback was often infrequent or absent. Although feedback was rated highly important for clinical practice, reporting, and positioning safety, responsibility for providing it was perceived as unclear. Barriers included limited interdepartmental collaboration, unclear routines, and time constraints, whereas facilitators included cross-unit collaboration, defined feedback responsibilities, and leadership support. Some nurses reported resorting to impermissible access to patient records to obtain outcome information. The findings indicate a need for systematic, leadership-supported feedback structures that strengthen organisational learning, ensure legal compliance, and enhance perioperative patient safety.
Keywords
Introduction
Surgical procedures constitute a major component of global health care, with more than 300 million operations performed annually and a substantial share of preventable patient harm linked to perioperative care (World Health Organization (WHO) 2023). Even low-incidence complications can have considerable population-level impact due to the sheer volume of procedures. Positioning-related injuries, such as pressure injuries, nerve damage, and circulatory impairment, remain a persistent challenge, reflecting the heightened vulnerability of anaesthetised patients who cannot signal discomfort or adjust their position (Bentsen et al 2024, von Vogelsang et al 2019).
Perioperative practice is central to preventing positioning-related harm. Operating theatre (OT) nurses independently plan and implement evidence-based positioning strategies, maintain asepsis, and optimise physiological conditions across the surgical pathway (Riksföreningen för operationssjukvård (Rfop) 2020, Spruce 2017). Systematic preoperative risk assessment, vigilant intraoperative monitoring, and structured intraprofessional and interprofessional communication are essential. Interventions such as the WHO Surgical Safety Checklist have demonstrated reductions in complications and improved teamwork through clearer roles and shared mental models (Haynes et al 2009).
The OT is a complex, technology-dense environment where adverse events often arise from breakdowns in communication, inconsistent workflows, or competing task demands (Gillespie et al 2009). Increasing surgical complexity, including minimally invasive and robotic procedures, requires individualised positioning plans, repeated checks of patient alignment, and adaptation to limited visibility caused by draping and equipment (Bentsen et al 2024, Bjøro et al 2022). As many positioning-related injuries develop hours or days after the operation, the need for thorough documentation and anticipation of risk is critical (Usul & Dizer 2025).
Systems perspectives offer valuable frameworks for understanding the challenges highlighted in this study. Safety I and Safety II draw attention both to the prevention of errors and to the conditions that enable care to function safely under varying and often demanding circumstances (Hollnagel & Braithwaite 2013). Within these perspectives, feedback emerges as a central mechanism for learning, improvement, and professional development (Michl et al 2024). Effective feedback clarifies expectations, identifies emerging risks, and supports safer clinical practice, whereas feedback that is unclear, irregular, or poorly delivered can undermine motivation and hinder learning (Christina et al 2016). At an organisational level, feedback provided through incident-reporting systems contributes to quality-improvement efforts and strengthens a positive patient-safety culture (Glarcher & Vaismoradi 2025).
Given that positioning-related injuries occur in environments characterised by high interdependence and rapid task flow, feedback processes are particularly important. Yet, little is known about how OT nurses perceive, utilise, and integrate such feedback into their daily practice, indicating a need for further exploration of their experiences.
The aim of this study is to explore OT nurses’ experiences of receiving feedback on positioning-related injuries acquired intraoperatively with the following objectives:
How do OT nurses experience receiving feedback on intraoperatively acquired positioning-related injuries, and how clear is the responsibility for providing such feedback?
What are the sources, formats, and frequency of feedback that OT nurses receive regarding positioning-related injuries, and how do these factors influence their reporting practices?
Which organisational factors facilitate or hinder effective feedback processes related to positioning-related injuries, and how do OT nurses perceive the impact of feedback on their ability to work safely?
Methods
Study design
The study used a non-experimental descriptive cross-sectional design, conducted as a web-based survey.
Setting and sample
The study used a non-probability sampling strategy combining convenience and snowball sampling, a common approach when no formal register of the target population exists (Polit & Beck 2021). Convenience sampling targeted easily accessible OT nurses, while snowball sampling allowed included participants to recruit additional colleagues, thereby broadening the sample and increasing variation. Recruitment took place through closed, profession-specific Facebook groups for Swedish OT nurses, where participation was anonymous, voluntary, and self-selected, limiting independent verification of professional identity. Informed consent and confirmation of inclusion criteria were obtained through a mandatory checkbox in the survey. The sample included OT nurses from county, regional, and private hospitals in Sweden and varied in gender, professional experience, employment form, and working hours. Inclusion criteria required licensed OT nurses with current clinical practice and experience caring for anaesthetised patients with neuromuscular blockade sufficient to eliminate autonomous movement for at least 1 hour.
Data collection
Description of instrument: Data were collected through a digital questionnaire, an efficient method for reaching a geographically dispersed sample within a limited timeframe (Henricson 2023). Because no existing instrument fully matched the study aim, a study-specific survey was developed, informed by established and psychometrically tested tools (Supplemental Material 1). The Patient Safety Competence Scale (PEPSS) guided the construction of items related to feedback, responsibility, and motivation to report adverse events (Ginsburg et al 2012), while the Swedish version of the Hospital Survey on Patient Safety Culture (S-HSOPSC) informed questions addressing organisational factors and feedback structures (Hedsköld et al 2013). Questions were not copied but developed independently based on the instruments’ conceptual frameworks, a recognised strategy when designing new questionnaires (Polit & Beck 2021).
Content validity was enhanced through expert review by two OT nurse doctoral students, including one specialist in positioning-related injuries, and face validity was assessed by two experienced OT nurses who evaluated clarity, relevance, and estimated completion time. Their feedback informed revisions to improve comprehensibility and analytic usefulness (Henricson 2023). Reliability was supported through a clear layout, logical structure, and standardised response formats, and a technical review ensured functionality prior to launch. The final questionnaire contained 7 demographic items and 13 study-specific questions. Frequencies, clarity, and perceived importance were measured using ordinal Likert-type scales (Joshi et al 2015), and the combination of closed and open items enabled both quantitative and qualitative analyses.
Data collection was carried out over a 2-week period (21 November–5 December 2025) with three distribution rounds to increase visibility and response rates. The questionnaire was distributed through the profession-specific Facebook group and via personal contacts, and participants could respond either through a QR code or a generic survey link.
Data analysis
The analysis was conducted using descriptive statistics, an appropriate method for summarising and clarifying patterns and variations in the data (Polit & Beck 2021). Categorical variables were analysed using frequencies and percentages. Multiple-choice items were summarised by counting occurrences and calculating the percentage for each response option. For Likert-type-scale items, mean values were calculated on a five-point scale, enabling an overview of respondents’ experiences and attitudes. The results were visualised in tables and figures to highlight key patterns.
Ethical considerations
The study adhered to the principles of the Declaration of Helsinki (World Medical Association (WMA) 2024), ensuring respect for participants, protection from harm, and fairness. Participants received written information about the study’s purpose, procedures, anonymity, voluntariness, and the right to withdraw, and informed consent was obtained through a mandatory confirmation in the digital survey. Anonymity was maintained by avoiding the collection of identifiable information or technical metadata.
Data were stored securely on password-protected devices and deleted after the study ended. Participants’ rights, anonymity, and voluntary participation were safeguarded throughout. In line with the Swedish Ethics Review Act (SFS 2003:460), the study did not require ethical approval, as it did not involve sensitive personal data, health information linked to identifiable individuals, or any physical or psychological intervention.
Results
Participants
A total of 57 respondents were included in the study, the majority of whom were women (91%, n = 52). Among the respondents, 83% (n = 47) worked full-time, defined as a 90%–100% employment rate. Most were employed at regional or university hospitals (84%, n = 48). The respondents had varying levels of professional experience, with the largest proportion having worked as OT nurses for 16 years or more (33%, n = 19). In total, 61% (n = 35) had been in the profession for 8 years or longer (Table 1). The respondents reported working across several surgical specialities, with the most common being general surgery, orthopaedic surgery, and gynaecological surgery/obstetrics. All respondents reported the supine position as the most commonly used positioning method in clinical practice (100%, n = 57). In addition, the lateral position was reported by 54% (n = 31), the lithotomy position by 39% (n = 22), and the prone position by 30% (n = 17).
Demographic characteristics

Frequency and type of feedback provided
Regarding feedback related to positioning-related injuries, just over half of the respondents reported that they had only occasionally received feedback on an injury in which they were involved (54%, n = 31), while 32% (n = 18) stated that they had never received any feedback. When respondents reported a suspected or confirmed positioning-related injury, feedback was described as infrequent (28%, n = 16) or entirely absent (40%, n = 23) (Figure 1).
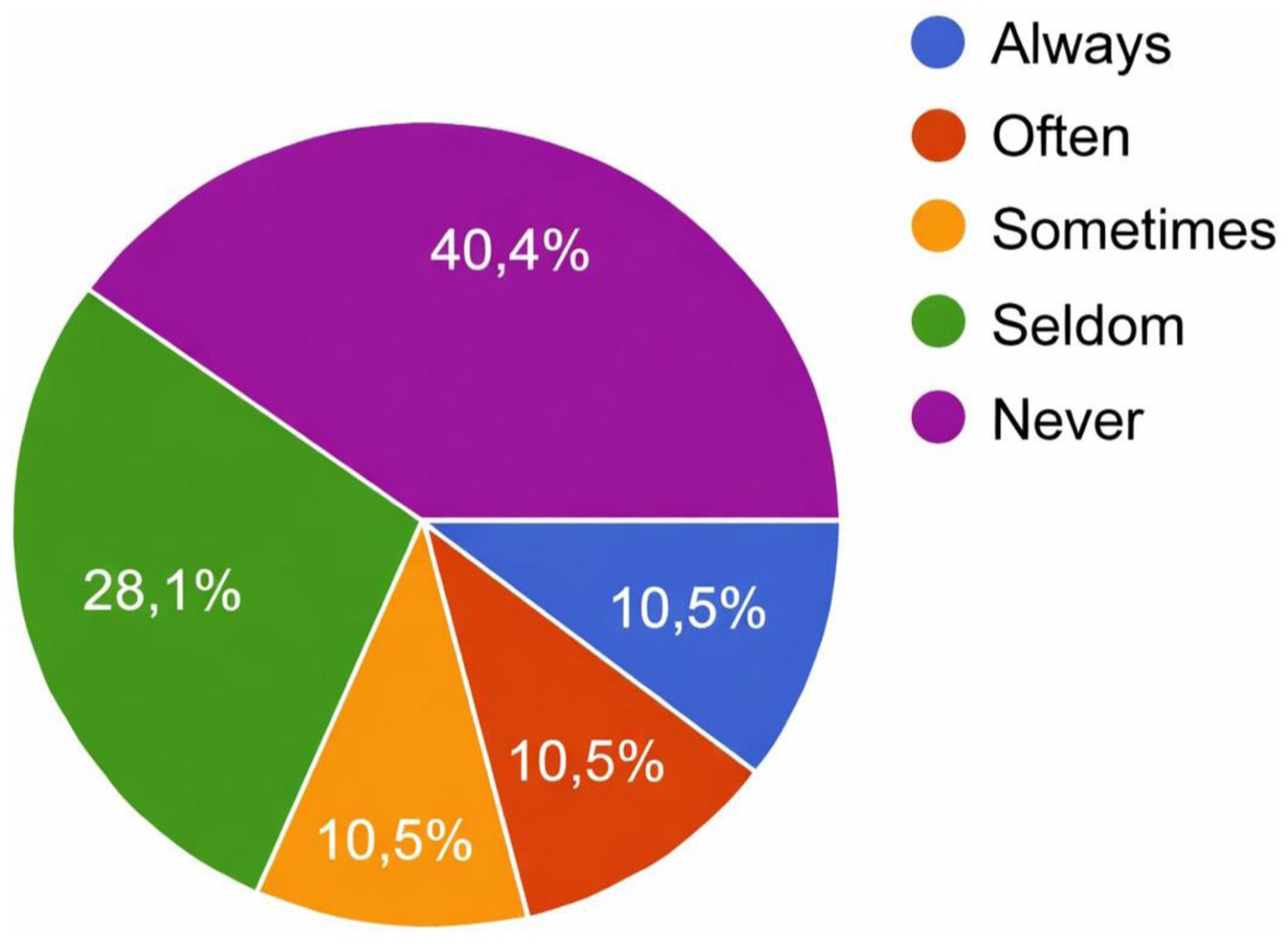
How often do you receive feedback when you have suspected, documented, and reported a positioning-related injury?
The perceived importance of feedback for clinical practice was rated with a mean score of M = 4.93 on a five-point scale. The importance of feedback for reporting willingness and for patient safety during positioning was rated at M = 4.53 and M = 4.53, respectively. In contrast, the clarity of responsibility for providing feedback received a considerably lower mean rating of M = 2.04.
Two main approaches were identified for how OT nurses follow up on a patient’s condition when feedback on a suspected positioning-related injury was lacking: direct contact with other health care personnel and review of the patient’s medical record.
Barriers and challenges to feedback
The respondents identified several organisational barriers to feedback (multiple-choice item). The most frequently reported ones were insufficient collaboration between units within the care pathway (68%, n = 39), unclear routines or responsibilities (63%, n = 36), and lack of time (56%, n = 32) (Figure 2).
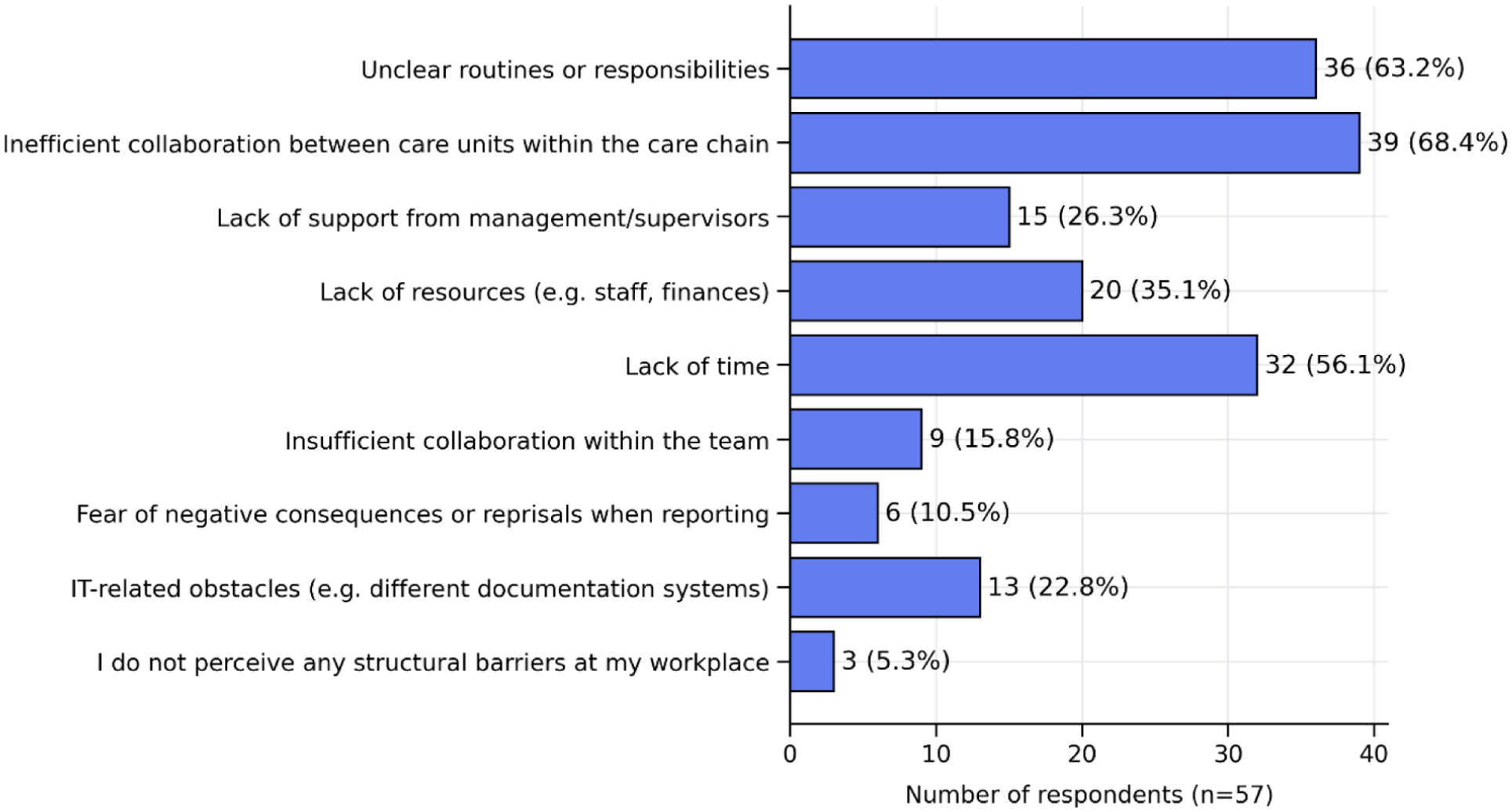
Barriers and challenges to feedback
Factors promoting feedback
Several factors were identified as important for supporting an effective feedback process. The most frequently reported facilitators included efficient collaboration between units across the care pathway (88%, n = 50), clearly defined responsibility for providing feedback following reported injuries (84%, n = 48), and managerial support reflected in a safety-oriented organisational culture (65%, n = 37) (Figure 3).
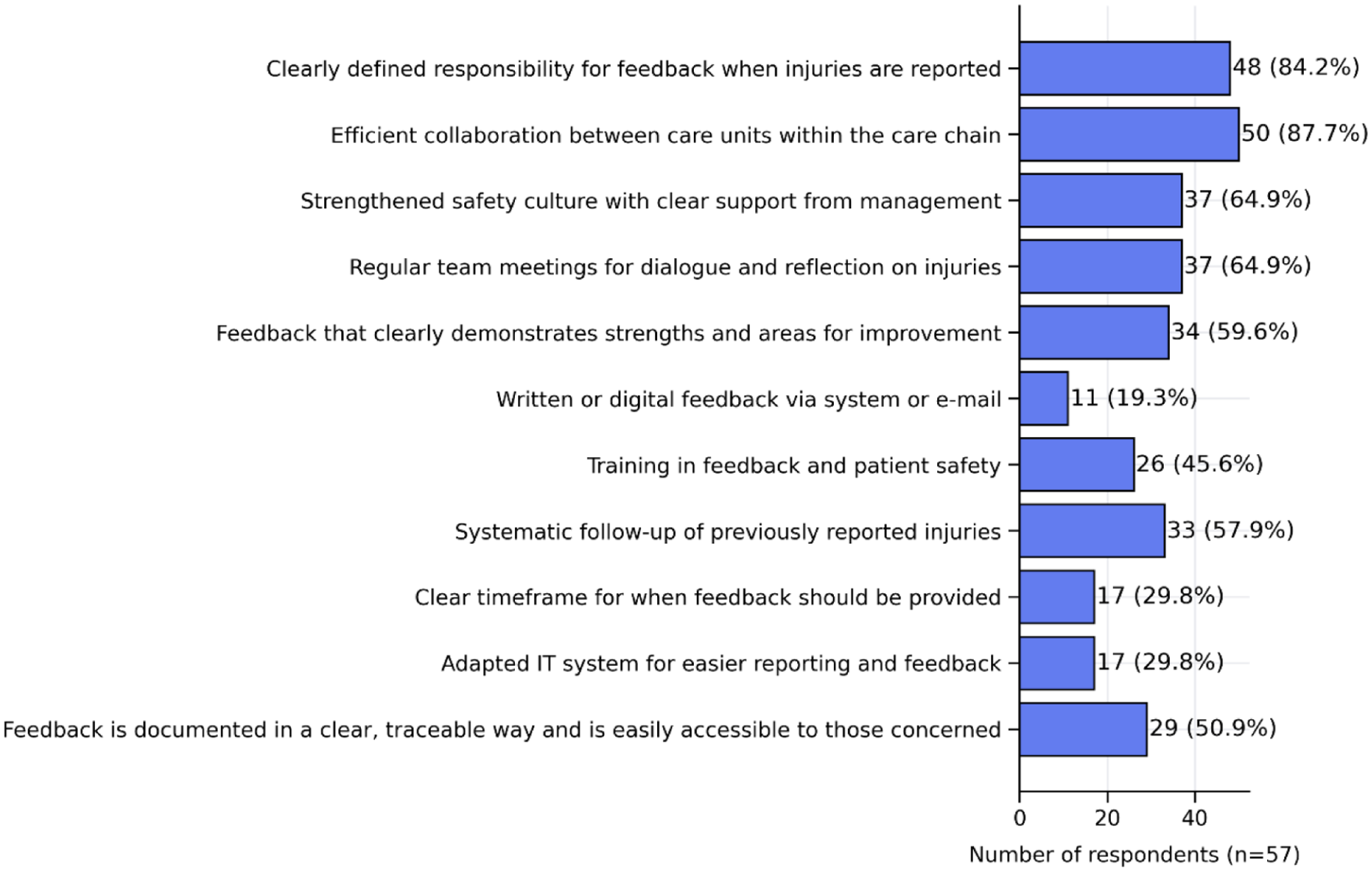
Factors promoting feedback
Discussion
This study highlights a pronounced gap between the importance attributed to feedback and its limited availability in perioperative practice. Although most OT nurses reported experience with positioning-related injuries, structured feedback after incident reporting was uncommon. This aligns with earlier research demonstrating that insufficient feedback undermines reporting motivation, restricts learning, and limits the development of safer practices (Christina et al 2016, Michl et al 2024). Furthermore, limited documentation and follow-up have been shown to obscure early signs of preventable complications, such as limb symptoms following robotic procedures (Ramírez Johansson & von Vogelsang 2019).
In the absence of formal feedback systems, many respondents described taking individual initiatives, most notably reviewing patient records after surgery or contacting colleagues in the care pathway. These actions reflect strong professional engagement, yet they also expose serious legal and ethical conflicts. According to the Swedish Patient Data Act, only health care professionals directly involved in a patient’s care are permitted to access medical records; retrospective review for ‘personal follow-up’ is not legally permissible. Several respondents nevertheless reported that this was the only available way to obtain feedback, underscoring the extent to which the organisation fails to provide lawful and reliable mechanisms for learning. The reliance on individual initiatives such as informal follow-up and retrospective chart review reflects patterns described in previous research. Clark et al (2025) report that health care staff routinely engage in workarounds when organisational systems are insufficient, often navigating tensions between professional responsibility and regulatory constraints. Similarly, in this study, nurses’ actions, although motivated by a desire to ensure patient safety, resulted in legally problematic practices that indicate a lack of system-level support for structured and lawful feedback processes.
Even from a legal and organisational standpoint, structured feedback is essential. Health care providers are obligated to ensure systematic patient safety work, in which structured feedback is a fundamental component. The absence of structured feedback processes therefore constitutes an ethical, legal, and professional concern at the system level, where organisational shortcomings risk limiting OT nurses’ ability to act in accordance with their professional responsibility. This stands in contrast to the International Council of Nurses (ICN) Code of Ethics, which emphasises nurses’ duty to promote patient safety, prevent harm, and contribute to continuous quality improvement (International Council of Nurses (ICN) 2021).
Safety I and Safety II perspectives
Integrating the findings with Safety I and Safety II perspectives further clarifies the implications of the current feedback deficit. From a Safety I perspective, feedback serves as a reactive mechanism for learning from adverse events and near misses. When most respondents reported ‘seldom’ or ‘never’ receiving feedback on reported incidents, opportunities for traditional incident-driven learning were lost.
A Safety II perspective broadens the understanding of feedback by also recognising the need to learn from what routinely goes well. OT nurses continuously adapt to procedural variation, limited visibility due to draping, and patient-specific anatomical challenges. However, these successful adaptations remain largely invisible without systematic feedback mechanisms. Positive, proactive learning, such as highlighting competent positioning decisions or effective risk-mitigating teamwork, therefore remains underdeveloped. This is consistent with prior work demonstrating that feedback which includes both risk identification and recognition of successful practice strengthens professional development and psychological wellbeing (Michl et al 2024) and can be formalised through excellence-based reporting systems (Plunkett et al 2015).
Organisational, ethical, and legal implications
The organisational barriers identified in this study, unclear routines, time constraints, and limited interdepartmental collaboration, indicate that the lack of feedback is rooted not in individual behaviour but in systemic shortcomings. When feedback is informal or individually initiated, learning becomes fragmented and seldom contributes to broader organisational improvement (Glarcher & Vaismoradi 2025). The respondents’ accounts reflect this pattern: learning does occur, but in isolation and often through methods that conflict with both ethical standards and legal requirements. Several OT nurses reported resorting to legally impermissible practices, such as accessing patient records without a care-related mandate, solely to obtain outcome information. This underscores the severity of the system failure; nurses feel compelled to break the law in order to fulfil what they perceive as their professional and ethical responsibility.
The resulting tension is ethically significant. Nurses described uncertainty and feelings of inadequacy, suggesting the presence of ethical stress. A lack of feedback has been linked to such experiences, as clinicians struggle to uphold the principles of beneficence and non-maleficence without adequate information about the consequences of their actions (Beauchamp & Childress 2013, Michl et al 2024). When organisations fail to provide lawful, structured feedback mechanisms, OT nurses are placed in an untenable position where meeting ethical obligations means violating regulatory constraints, highlighting an urgent need for system-level reform.
Strengths and limitations
A key strength of this study is its national reach, achieved through broad digital recruitment that increased variation in professional backgrounds and organisational settings and enriched the understanding of OT nurses’ experiences. The high internal data quality, with no missing responses, strengthens the reliability of the findings. Moreover, the questionnaire, developed from established patient safety frameworks and refined through expert review, provides strong content validity within the study’s scope.
However, the use of non-probability sampling through social media and snowball recruitment introduces selection bias and limits generalisability (Lehdonvirta et al 2021). The low numeric response rate increases the risk that participants differ systematically from non-respondents. Self-reported data may also be affected by recall bias and social desirability. In addition, the questionnaire lacks full psychometric validation, and reliability cannot be empirically confirmed without test–retest procedures. Finally, recruitment via open links and the short data-collection period pose further methodological constraints (Lehdonvirta et al 2021).
Conclusion
Taken together, the findings show that OT nurses frequently encounter positioning-related injuries but rarely receive structured feedback despite its importance for patient safety, learning, and professional development. The lack of clear routines, defined responsibilities, and cross-unit collaboration limits prevention efforts and weakens the safety culture, while the absence of organisational feedback systems places nurses in ethically and legally vulnerable situations.
Feedback therefore emerges as both a professional necessity and an ethical–legal requirement in perioperative practice. To ensure safe and sustainable practice, organisations need systematic, leadership-supported feedback structures that support learning from both adverse events and everyday successful practice. Such systems would enhance patient safety, strengthen OT nurses’ professional agency, reduce ethical stress, and improve quality and resilience across the perioperative workflow.
Supplemental Material
sj-docx-1-ppj-10.1177_17504589261450077 – Supplemental material for Operating theatre nurses’ experiences of feedback on intraoperatively acquired pressure injuries related to surgical positioning: A descriptive survey study
Supplemental material, sj-docx-1-ppj-10.1177_17504589261450077 for Operating theatre nurses’ experiences of feedback on intraoperatively acquired pressure injuries related to surgical positioning: A descriptive survey study by Matilda Thunmarker, Lubava Jasnopolski and Ami Fagerdahl in Journal of Perioperative Practice
Footnotes
Author contributions
MT and LJ were responsible for data collection and for the development of the questionnaire. MT, LJ, and AF contributed to the conception and design of the study and participated in all other aspects of the research process. AF drafted the first version of the manuscript. All authors critically revised the manuscript and approved the final version. AF holds overall responsibility for the work. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
The study adhered to the principles of the Declaration of Helsinki, ensuring respect for participants, protection from harm, and fairness. Participants received written information about the study’s purpose, procedures, anonymity, voluntariness, and the right to withdraw, and informed consent was obtained through a mandatory confirmation in the digital survey. Anonymity was maintained by avoiding the collection of identifiable information or technical metadata. In line with the Swedish Ethics Review Act (SFS 2003:460), the study did not require ethical approval, as it did not involve sensitive personal data, health information linked to identifiable individuals, or any physical or psychological intervention.
Consent for publication
Not applicable.
Data availability statement
The data are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.