
Abstract
Aim:
To explore the holistic nature of intraoperative nurse competence and its assessment methods.
Background:
Safe and effective nursing care in the intraoperative setting requires specialised knowledge, skills and attributes. Understanding what makes a competent intraoperative nurse and how to measure it is necessary to set professional expectations and inform future education initiatives.
Methods:
A scoping review of peer-reviewed studies published from 2009 was conducted following the Joanna Briggs Institute (JBI) methodology and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for scoping reviews guidelines.
Results:
Fifteen studies from eight different countries were included. Studies described similar competency domains, related to perioperative-specific technical skills and knowledge, and individual non-technical skills that enabled effective teamwork and collaboration. The Perceived Perioperative Competence Scale-Revised (PPCS-R) was the most frequently used assessment tool. Potential gaps in the competency domains included those related to patient assessment and cultural competence.
Conclusion:
Intraoperative nursing competence is complex and multidimensional, involving both technical and interpersonal capabilities. Challenges arise when assessing self-reported competence, and current approaches to measurement may need to expand their scope to ensure that competencies required for contemporary practice are adequately captured and measured.
Introduction
Organisations often use competency assessments to measure ongoing capability for practice and identify gaps in performance and educational needs of staff (Gillespie et al 2018). In the operating department setting, challenges such as the critical and vulnerable nature of patients, the high-pressure environment and the presence of multiple hazards, such as surgical smoke, sharps and biological hazards (Ugurlu et al 2015), necessitate competencies specific to this unique environment. Researchers have suggested that the combination of specialised knowledge, skills, attitudes and behaviours needed in this setting may extend far beyond the recognised specialised knowledge and traditional technical skills, encompassing a broader spectrum of cognitive, interpersonal and situational capabilities (Gillespie & Hamlin 2009, Sirevåg et al 2023, Uçak & Cebeci 2021).
Roles in the intraoperative environment are diverse, highly specialised and vary between countries, but they consistently involve comprehensive care and support throughout the patient’s perioperative journey. A multidisciplinary team, including surgeons, anaesthetists, nurses, operating department practitioners (ODPs), and other perioperative personnel, collaborates to deliver safe and effective intraoperative care. Within these varied teams, nurses play a pivotal role contributing to direct patient care, interdisciplinary coordination, management of advanced technologies, identification and escalation of safety concerns and maintaining vigilance and adaptability in response to shifting priorities (Nyberg et al 2024, 2021). Depending on their scope of practice, nurses may assist the surgeon within the sterile field, manage the operating room environment, support the surgical team, assist with anaesthesia administration, monitor the patient’s condition and respond to any intraoperative complications (Perioperative Care Collaborative 2017, Australian College of Operating Room Nurses (ACORN) 2023). These broad responsibilities highlight that nurses require a deep theoretical knowledge, alongside specific technical and cognitive capabilities, to navigate the complexities of patient care and the occupational hazards inherent in the operating room (Ugurlu et al 2015).
Despite efforts to clarify perioperative nursing competence, the field would benefit from further developing this conceptualisation. Given the complexity of the care provided and the environment in which it is performed, there is a pressing need to better understand what constitutes a competent perioperative nurse. While professional organisations may articulate professional standards and outline the scope of practice in this environment (ACORN 2023), perspectives on the characteristics of a competent nurse may differ owing to a lack of conceptual agreement.
In addition, during the COVID-19 pandemic, operating rooms underwent significant transformations in their operational practices, which may have influenced competency expectations and further highlighted the importance of formalising ‘implicit’ competencies. Although Gillespie and Hamlin (2009) made an important attempt to define perioperative nursing competence in their pivotal literature synthesis over a decade ago, their review highlighted the challenge of inconsistent definitions and conceptualisations. This uncertainty continues to contribute to challenges and variability in assessing and setting expectations for nurses and institutions (Uçak & Cebeci 2021). To address this gap, this study aimed to examine the latest literature on perioperative nurse competence, which may help provide conceptual clarity in the post-pandemic context.
The review
Research aim and design
This study aimed to explore the holistic nature of intraoperative nurse competence and its assessment methods. Given the lack of clarity on what constitutes perioperative nurse competence and the multiplicity of definitions, a scoping review was selected as the appropriate study design. Scoping reviews can be used to synthesise evidence and are useful for describing broader, less well-defined constructs, identifying knowledge gaps and surveying diverse research methodologies that are less amenable to systematic reviews, which often have more well-defined and structured questions (Peters et al 2022). We used a scoping review methodology to chart the current state of perioperative nurse competence literature from the time of Gillespie and Hamlin’s (2009) pivotal review.
Ethics statement
This study utilised existing literature and did not involve the collection of primary data; therefore, ethics approval was not required for this scoping review.
Search strategy
Following the PRISMA for Scoping Reviews (PRISMA-ScR) guidelines (Tricco et al 2018), we conducted comprehensive searches of electronic databases, including EBSCOhost, as well as databases such as Health Source, Medline, APA PsycArticles, Psychology and Behavioural Sciences Collection, APA PsycInfo, APA PsycTests and CINAHL Ultimate. In addition, Scopus, Science Direct and Ovid were also searched. Search terms included ‘competence’, ‘competency’, ‘nursing’, ‘perioperative’, ‘surgery’, ‘operating room’ and ‘operating theatre’. Truncation and wildcards were used to account for variations in word forms and spelling. Key terms were also searched for subject terms through EBSCO. Studies published in the English language from 2009 to 2025 were accessed to ensure adequate capture of the influential work conducted during this period. The search was conducted from November 2024 to January 2025.
Inclusion and exclusion criteria
The literature was included if it focused on the competence, collective knowledge, skills and attributes required to perform effectively and safely in the intraoperative environment. Articles identified as peer-reviewed primary research studies were included. Articles were excluded if they soley focused on professionals other than nurses, focused outside of the intraoperative setting (e.g. recovery or preoperative clinics), or solely on isolated skills or attributes.
Screening
One researcher searched the databases and identified studies that were collated and uploaded to Covidence (2023), which was used to manage the scoping review. Following the removal of duplicates, a pilot test of screening was conducted to ensure mutual understanding and consistency within the research team. Two reviewers subsequently screened titles and abstracts independently to determine their relevance to the inclusion criteria. Any discrepancies in study selection were resolved through discussion. Full-text articles were retrieved and independently systematically reviewed against the inclusion criteria by two reviewers. Any discrepancies in study selection were resolved through discussion. Reasons for exclusion at the full-text review stage were documented for transparency and clarity.
Data extraction
Data were extracted systematically to ensure the accurate collection of relevant information from each study. Two reviewers independently extracted data, cross-checking each other’s work for accuracy and resolving discrepancies through discussion to reach consensus. Extracted data included demographic characteristics of study participants, such as gender, age, professional background, years of experience in perioperative nursing and professional qualifications. Particular attention was given to how each study defined competence in the intraoperative setting, as definitions varied across sources. In addition, the review captured the specific components of competence identified in the literature, including both technical and non-technical skills. The assessment tools used in the studies were also examined, with attention to the methods employed to evaluate competence.
Data analysis and presentation
The extracted data were analysed using basic descriptive techniques to describe the assessment tools used in the studies and the components of competence that they assessed. The results were reported as counts and percentages. This review did not assess the quality of the articles or evaluate their risk of bias, as guided by the scoping review methodology (Peters et al 2022). The findings are therefore presented as a narrative summary to help the field mature in relation to future research in this context.
Results
Database searches identified 1638 records. After duplicates were removed, the titles and abstracts of 1488 records were screened. Of those, a total of 61 records were identified for full-text screening. Forty-six articles were excluded, and a total of 15 studies were included in the review (Figure 1).
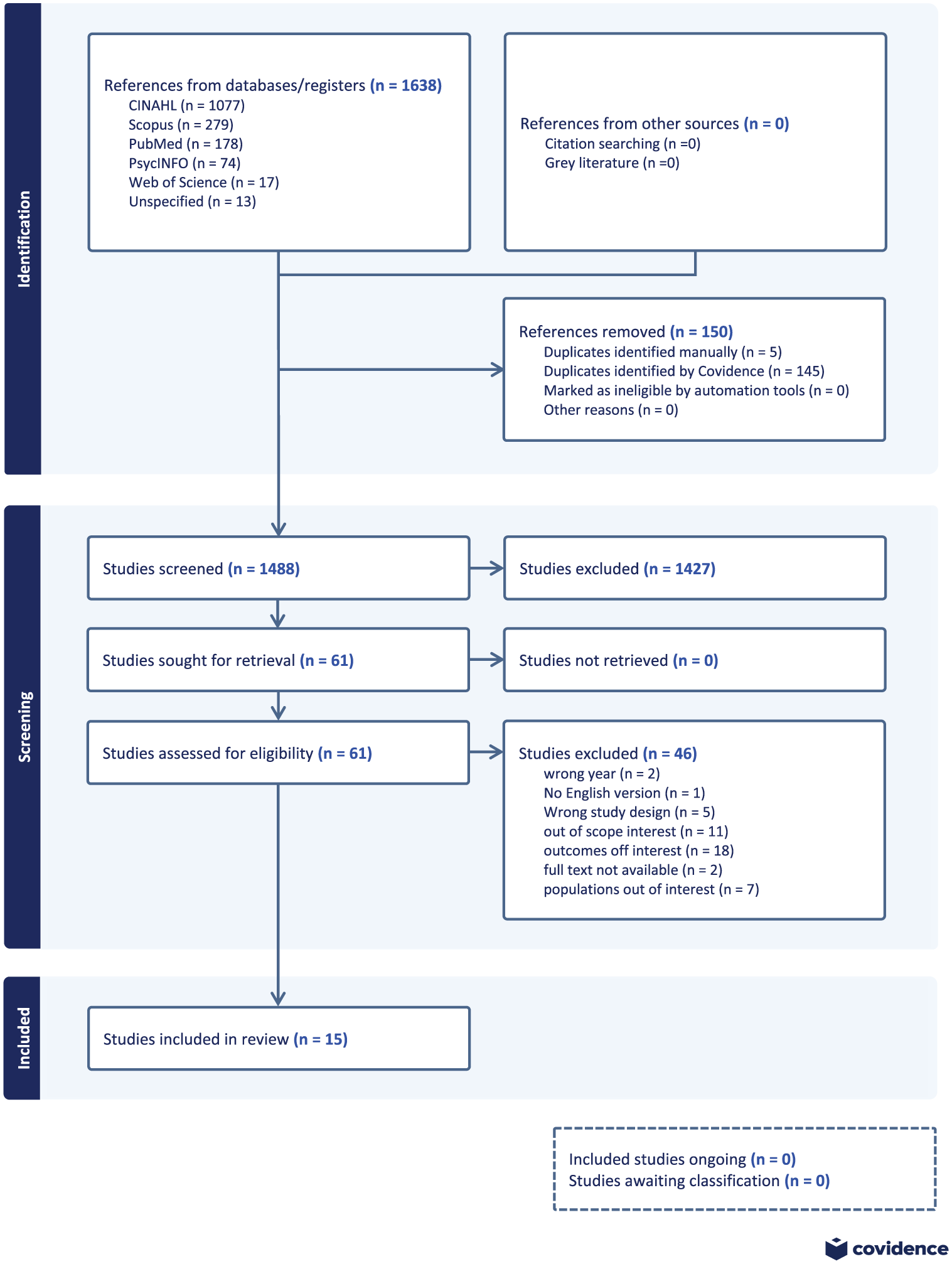
PRISMA flow diagram
Characteristics of included studies
Table 1 provides a summary of the study characteristics and findings. The 15 included studies were conducted across various countries, including Australia, Canada, Scotland, the United States, Sweden, China, Turkey and Finland, and employed a range of methods and methodologies, including qualitative focus groups, cross-sectional surveys and mixed-method approaches.
Characteristics of included studies
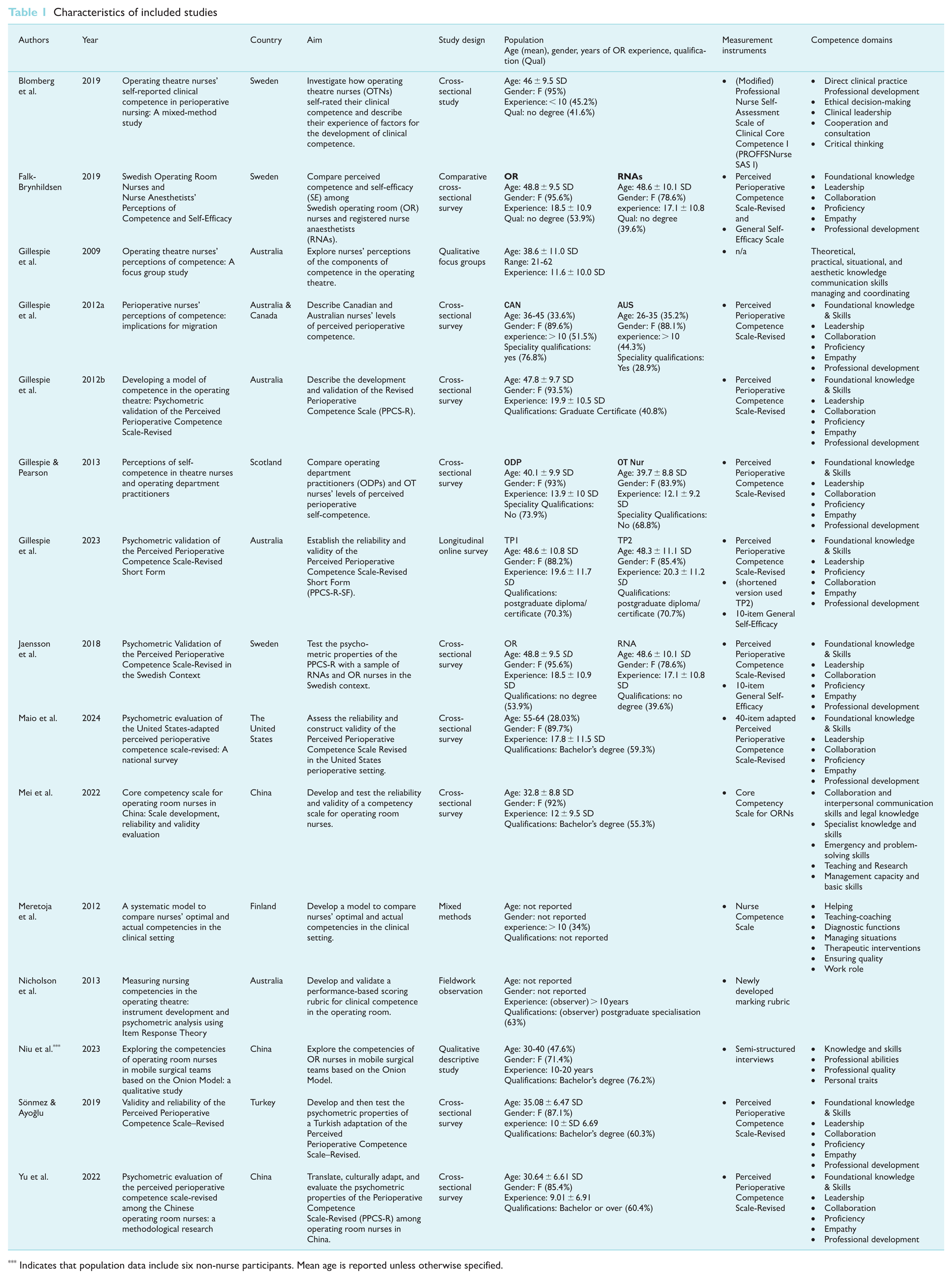
Indicates that population data include six non-nurse participants. Mean age is reported unless otherwise specified.
Characteristics of participants in included studies
The reporting of participant characteristics varied considerably between studies, and not all studies reported age, gender, perioperative nursing experience or qualifications. In studies where demographics were reported, the age range was from 21 to over 60 years, with the mean age ranging from 30.64 ± 6.61 SD to 48.8 ± 9.5 SD years. Participants were mainly female, with over 10 years of professional experience, and held either a bachelor’s degree or a professional diploma in nursing. Most samples were recruited from credentialing or professional associations.
Approaches to the assessment of competence
Five tools were identified across the included studies to assess perioperative nurses’ competence. The most commonly used was the Perceived Perioperative Competence Scale-Revised, which was adopted or adapted in nine studies (Gillespie et al 2012a, 2012b, 2023, Gillespie & Pearson 2013; Falk-Brynhildsen et al 2019, Jaensson et al 2018, Maio et al 2024, Sönmez & Ayoğlu 2019, Yu et al 2022). Other tools included observational rubrics (n = 1; Nicholson et al 2013), a modified Professional Nurse Self-Assessment Scale of Clinical Core Competence (n = 1; Blomberg et al 2019), the Core Competency Scale for ORNs (n = 1; Mei et al 2022) and the Nurse Competence Scale (n = 1; Meretoja and Koponen 2012).
Competence domains
In Table 1, the conceptual labels used by authors to categorise competency domains are shown. Studies broadly identified the need for: (1) individual knowledge and skills, categorised as: foundational knowledge and skills (n = 9), theoretical, practical, situational and aesthetic knowledge (n = 1), specialist knowledge and skills (n = 1), knowledge and skills (n = 1); emergency and problem-solving skills (n = 1), critical thinking (n = 1), ethical decision making (n = 1); (2) team-based skills, such as leadership and management (n = 12), collaboration, consultation and cooperation (n = 12); (3) personal attributes, including empathy (n = 10) and (4) the ability to develop oneself and others (n = 11).
Discussion
Intraoperative nurse competence has been broadly described in the literature in terms of the context-specific skills, knowledge and attributes required to practice in the unique operating environment, as well as more generic competencies applicable across various health care settings. While no uniform definition of intraoperative nurse competence was identified, we did observe similarities between the categories of competence, suggesting nurses need to possess similar technical and non-technical capabilities to be considered competent in this specialised field. Despite studies being conducted in various countries and several using different competency assessment frameworks, there appeared to be some general agreement on the competencies needed for nurses to practice safely and effectively in the intraoperative setting.
Contextualised knowledge and skills, teamwork abilities, leadership and self-development were noted as important domains across the reviewed studies; however, the direct assessment of technical proficiency was not prominent. Despite the recognition that perioperative nurses require specialised psychomotor technical skills (Gillespie et al 2009, Nicholson et al 2013), existing frameworks address these inconsistently. While, the PPCS-R, includes the domains titled ‘Foundational knowledge and skills’ and ‘Proficiency’ (Gillespie et al 2012b), analysis of individual items suggests these domains primarily reflect procedural knowledge, organisational acumen, or cognitive and situational skills, rather than hands-on technical capabilities. Gillespie and Pearson (2013), in a subsequent study, characterise the ‘Foundational knowledge and skills’ domain as encompassing beginning technical skills, such as knowledge of instruments and procedures, but stop short of including technical proficiency. Similarly, Maio et al (2024) describe this domain in terms of technical skills, linking it to knowledge of instruments and procedures, rather than to the mastery of technical psychomotor skills. In contrast, Falk-Brynhildsen et al (2019) adopted a version of the PPCS-R that removed the word ‘skills’ from the competency domain title altogether, potentially reflecting a conceptual shift in how this domain is understood and operationalised.
Technical proficiency did appear to be more directly examined in some competency frameworks, such as the Professional Nurse Self-Assessment Scale of Clinical Core Competence I, used by Blomberg et al (2019). This scale was first developed and validated in long-term and home care contexts in Norway and includes questions that target the nurses’ direct clinical practice, such as ‘I utilize medical equipment in an appropriate and accurate manner’ (Finnbakk et al 2015). However, given Blomberg et al (2019) report modifying the tool, acknowledging that not all items from the original scale were relevant to the perioperative context, it is difficult to determine whether these technical domains remained the same in the modified version.
Non-technical skills related to individual performance emerged consistently as a competency domain across all studies. Gillespie et al (2009) identified empathy and situational awareness from their analysis of focus group interviews with perioperative nurses as important domains, which subsequently informed the development of the PPCS-R. Similarly, other studies also identified the importance of critical thinking and person-centredness (Blomberg et al 2019, Mei et al 2022), although not always described as such.
Beyond individual performance, all studies that described their domains of competence also recognised the importance of team-based non-technical competencies, such as leadership, cooperation, coordination, and supporting others. These findings are supported by recent research suggesting that team-based non-technical skills are a critical factor for improving patient safety in the OR. For example, effective team-based communication and coordination have been reported to reduce surgical errors, improve workflow efficiency, and enhance situational awareness across the surgical team (Sinyard et al 2022, Weller et al 2024). These competencies are especially vital in high-stakes, fast-paced environments like the OR, where timely collaboration and shared mental models can directly impact patient outcomes (Attawet et al 2025). Considering a core tenet of nursing is to keep patients safe from harm (White et al 2025), it follows that any competency assessment would include those skills known to promote patient safety.
The complexity of intraoperative nurse competence likely contributes to the challenge of developing valid and reliable scales that adequately reflect the breadth and depth of required competencies while ensuring the assessment is manageable in length (Swan et al 2023). In this review, the response rate reported in individual studies was frequently below 50%. Longer surveys may increase responder fatigue and contribute to low response rates, careless responses and incompletions, while shorter surveys may inadequately capture the breadth of competencies required to be considered competent.
Considering this tension, some competency domains may have been forgone in lieu of areas deemed more relevant. For example, despite being emphasised in nursing professional frameworks (Nursing and Midwifery Board of Australia (NMBA) 2016), studies did not always explicitly assess less visible competencies related to cultural competence, moral judgement, values and ethics. While Blomberg et al (2019) specified the inclusion of ethical decision-making in their assessment of clinical competence, few others made this explicit.
Other competency areas related to patient assessment were also less prominent across the studies. Blomberg et al (2019), for instance, highlighted removing questions related to the clinical assessment of the patient’s diagnosis from their framework, considering such questions irrelevant in the perioperative setting. While the reviewed studies were conducted across different countries, and differences in performance expectations may exist, professional nursing perioperative bodies often refer to the importance of patient assessment. In Australia, for instance, the widely adopted ACORN standard for perioperative nursing emphasises the importance of patient assessment throughout. For example, nurses are expected to continually and collaboratively monitor and assess the patients’ condition and wellbeing (ACORN 2023).
The lack of complete visibility into the frameworks used across the included studies raises the possibility that these less visible items were, in fact, embedded in other domains or labelled differently. Previous work, however, has hypothesised that the over-reliance on previous frameworks, such as crew resource management (CRM), may limit the field’s understanding of the full scope of non-technical skills performed by nurses in the OR (Sirevåg et al 2023), which may explain why some domains were less visible. While it is worth considering whether these competencies were absent or merely integrated into other domains, the consequence of not making them explicit could mean that their importance to practice is underestimated.
The majority of studies used competency self-assessment tools to understand perioperative nurse competence. One of the challenges with this approach is, in fact, that the onus of deciding competence appears to lie with the individual in a self-assessment approach. Research has shown that an individual’s ability to accurately assess their level of capability is imperfect and often leads to biased perceptions of one’s abilities (Carter & Dunning 2008, Ehrlinger et al 2008). Dunning et al (2004) argue, for instance, that students’ self-assessment of competence often shows only marginal agreement with mentors’ and teachers’ assessments. Elsewhere in the health care domain, neither medical students’ nor physicians’ perceived competence has been found to be strongly related to more objective forms of measurement (Davis et al 2006, Lai & Teng 2011). In this review, only one study coupled the self-assessment of competence with an external assessment of actual competence. Meretoja and Koponen (2012) reported on the process of developing a threshold for optimal competencies using the Nurse Competence Scale and found that nurses’ self-assessed competence and their managers’ assessed competence levels were significantly lower than the expert’s optimal competency threshold. Although Sönmez and Ayoğlu (2019) suggest that the PPCS-R can be used by nurse managers to assess performance and guide professional development, this appears to depart from the original scale’s intended use as a self-assessment tool.
Social desirability response bias is another challenge with self-reported measures of capability. Individuals’ desire to portray themselves positively can lead responders to answer questions based on a false belief about themselves, or they may actively answer incorrectly to conform to a preconceived notion of what is considered an acceptable response (Van de Mortel 2008). While this may contribute to a distorted understanding of perceived competence levels, it can also mask potential issues with the scale design. High internal consistency may reflect response patterns rather than item coherence, potentially inflating reliability estimates. These concerns are particularly salient in studies reporting high test–retest reliability (Sönmez & Ayoğlu 2019) or in those that report skewed results, where responders select the highest possible rating across subdomains (Gillespie et al 2012a, Maio et al 2024, Sönmez & Ayoğlu 2019). These response patterns may in part reflect social desirability bias or response style effects rather than purely objective self-assessment. Some studies acknowledge the presence of positively skewed distributions and potential ceiling effects (Gillespie et al 2012a, Maio et al 2024), and they interpret results with thoughtful caution, advocating for further testing of these measures in more heterogeneous samples.
Gillespie et al (2012b), the developers of the widely adopted PPCS, have also acknowledged that there are critics of the value of competence self-assessment tools. However, they argue that despite limitations, their tool is helpful for self-reflection and a useful support for performance development reviews. Notably, ratings of perceived competence using the PPCR tend to correspond to years of experience in Australian, Canadian, UK and Swedish nurses, at least up to the 10-year point (Gillespie et al 2018). Conversely, the correlation between level of competence and academic degree was not always consistent. Falk-Brynhildsen et al (2019) found no correlation between academic degree and any of the six subscales of the PPCS-R, and Blomberg et al (2019) reported that nurses with a master’s level qualification rated themselves the lowest in some domains, for example, clinical leadership.
While the PPCS-R was the most frequently used scale in the reviewed studies, some authors report the development of alternatives to better capture contextual nuances of perioperative nursing in their settings. For example, Mei et al (2022) developed a five-domain 36-question scale to assess perioperative nurse competence in China. The scale demonstrated promising psychometric properties, with acceptable reliability and validity. However, the authors also recognised opportunities for further refinement, noting that the high Cronbach’s α of 0.97 may suggest conceptual overlap or item redundancy, a concern supported by the confirmatory factor analysis, which indicated only moderate model fit.
Conclusion and recommendations
This scoping review focused on identifying how intraoperative nurse competence has been conceptualised and measured holistically, examining both its components and the assessment tools used to measure it. The findings revealed that, although not clearly defined, intraoperative nursing competence, as a holistic concept, has been measured using a variety of assessment tools that focus on both technical and non-technical skills of intraoperative nurses. Although the tools used throughout the literature provide a foundation for assessing competence, some gaps were identified, particularly in cultural competence, suggesting they may not completely reflect contemporary nursing practice. Given that some of these tools were developed over a decade ago, they may need to be revised and updated to reflect modern-day practices.
Strengths and limitations
This study provides a broad overview of intraoperative nurse competence as a holistic construct, along with the assessment methods reported in the literature. The strengths of this study include the use of the JBI framework and PRISMA-ScR guidelines to inform the development, execution and reporting of the scoping review, the use of a comprehensive search strategy that enabled the identification of a wide range of peer-reviewed studies and the use of two researchers to independently review and extract study data. Conversely, several limitations need to be noted. First, we only included English-language publications, which may have resulted in relevant research published in other languages being excluded. Second, despite a rigorous search strategy, some eligible studies may have not been identified if the authors used alternative terminology. Third, much of the included literature focused on nurses affiliated with professional organisations, which may limit the generalisability of the findings. Finally, while this review focused specifically on registered nurses in the perioperative setting, we acknowledge that in the United Kingdom and other countries, the intraoperative workforce includes a range of professionals, including ODPs. As such, the findings may not reflect the breadth of competencies required by other professionals, and future reviews may wish to explore this to develop a more comprehensive understanding of the perioperative workforce.
Footnotes
Author Contributions
PS, JA, EC: Study design.
PS, JA: Data collection.
PS, JA, EC, KC: Data analysis.
PS, JA, EC, KC: Manuscript writing.
PS, JA, EC, KC: Critical revisions for important intellectual content.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.