
Abstract
Context:
Open abdominal procedures under combined general and epidural anaesthesia are at high risk of thermal loss due to prolonged operating times and significant exposure of internal organs.
Setting and Design:
In this prospective observational study, the effects of short-duration prewarming were assessed in participants who underwent open abdominal procedures with combined epidural and general anaesthesia.
Methods and Materials:
A total of 72 patients were observed, with 36 receiving 15 min of prewarming before surgery and 36 receiving warming only during surgery. Core temperature (tympanic) was measured with an infrared thermometer both before prewarming and at the end of surgery. The incidence of postoperative hypothermia (core temperature <36 °C) and shivering was also recorded.
Statistical analysis:
Chi-square test, Student’s t test or Pearson χ² were used for comparisons between two groups.
Results:
The median temperature difference (baseline temperature – postoperative temperature) was lower in the prewarmed group (0.5 °C vs. 0.75 °C). The incidence of postoperative hypothermia and shivering was also lower in the prewarmed group than in the non-prewarmed group (22% vs. 50% and 5.56% vs. 25%, respectively).
Conclusion:
A 15-min prewarming protocol is associated with a lower incidence of postoperative hypothermia and shivering in patients who undergo major abdominal surgery under combined general and epidural anaesthesia.
Keywords
Introduction
Perioperative hypothermia, a decrease in core body temperature to <36 °C, is a frequent complication during major surgeries, especially open abdominal procedures (Becerra et al 2019, Kaufner et al 2019). Perioperative hypothermia may increase the risk of surgical site infections, delay wound healing, decrease coagulation and increase bleeding, leading to longer hospital stays and increased morbidity and costs (Lee et al 2020).
Patients receiving combined general and neuraxial anaesthesia are exposed to the highest risk of inadvertent perioperative hypothermia because the thermoregulatory depressant effects of each modality are additive. This combination profoundly lowers the core temperature threshold for vasoconstriction by a magnitude that approximates the sum of the individual effects of each anaesthetic technique. Furthermore, this dual impairment not only delays the activation of autonomic defences but also attenuates both the gain and maximal intensity of the vasoconstrictor response once it is finally initiated. Consequently, patients under combined anaesthesia cool to a significantly lower core temperature before any physiological defence is mounted, and once recruited, these defences are markedly less effective at preventing further heat loss compared to those under general anaesthesia alone (Sessler 2016).
Prewarming is the practice of actively warming patients before the induction of anaesthesia or neuraxial blockade. This intervention reduces the redistribution of heat from the core to the periphery, thereby lowering the risk of perioperative hypothermia (Van Duren 2022). It is especially important in patients undergoing major open abdominal surgery under combined general and epidural anaesthesia, where vasodilation and exposure markedly increase heat loss. Although 30–60 min of prewarming is often advised, this duration is logistically challenging in busy centres (time, space, staff, equipment), hindering routine adoption. A shorter protocol of 10–15 min is effective in selected settings (Horn et al 2016, Recio-Perez et al 2023, Uçak et al 2024), but its utility in patients undergoing major abdominal surgery with combined epidural and general anaesthesia has not been thoroughly investigated. Evaluating pragmatic, shorter durations may preserve much of the clinical benefit while improving feasibility and uptake.
Hence, we observed the impact of short-duration prewarming, of 15 min, on the postoperative core temperature and incidence of postoperative shivering in a real-world setting. The primary objective was to determine the mean change in core temperature from the preoperative baseline to arrival at the post-anaesthesia care unit (PACU). The secondary objectives were the postoperative incidence of hypothermia (<36 °C) and shivering.
Methods
This was a prospective observational study carried out in a 2000-bed tertiary care centre in southern India after the approval of the Institutional Ethics Committee (EC/NEW/INST/2021/1707) and registration with the Clinical Trials Registry India (CTRI/2024/07/070755). The study was conducted from July 2024 to February 2025. Written informed consent was obtained from all the participants. The STROBE guidelines were used to report the findings of the study.
Patients above the age of 18 years who underwent open abdominal surgery under combined epidural and general anaesthesia, with American Society of Anaesthesiologists – Physical Status (ASA PS) grades of I, II or III, were recruited for the study. The exclusion criteria were refusal of epidural analgesia, absence of intraoperative epidural infusion, emergency procedures, body mass index (BMI) <18 or >35 kg/m2 and the presence of sepsis, fever or hypothermia before surgery.
The patients either received prewarming or did not receive prewarming on the basis of the availability of a forced air warmer and the adequacy of prewarming time without delaying operating room time, as decided by the consultant anaesthesiologist. If it were decided to prewarm the patient, then a standard warming protocol was initiated and continued for 15 min with a forced air warmer (3M™ Bair Hugger™ Model 775) set at 43 °C with a Bair Hugger blanket (3M™ Bair Hugger™ Blanket System). If the consultant decided not to prewarm, the patient was transferred to the operating room without receiving prewarming.
All patients received standard intraoperative warming measures after the induction of anaesthesia, in accordance with the standard operating procedures of our centre, thereby reducing potential confounding factors and effect modifiers. This included using a forced air warmer set at 43 °C through an upper body Bair Hugger blanket immediately after epidural catheter placement until the end of the surgery. All intravenous fluids were warmed through a fluid warmer set at 42 °C before infusion, and the warmed fluids were used for surgical site irrigation.
Data collection
All observations were conducted by the primary investigator, who was not involved in the patient’s anaesthetic management. Preoperatively, the baseline temperature was measured via a handheld infrared tympanic temperature device (Temperature Teller Plus GS-903). The clean probe was inserted into the ear canal by pulling the pinna up and back to straighten it, and the temperature displayed on the thermometer was recorded.
Details of intraoperative anaesthetic management, such as the epidural insertion level, drugs used, epidural infusion rate and surgical management, such as the duration of the surgery, level of incision and surgical irrigation fluids, if used, were documented from the anaesthetic chart. The duration of prewarming, if undertaken, was recorded. Intraoperative temperature trends at 15 and 30 min, followed by every hour and up to 3 h of the procedure, were also noted from the anaesthetic chart. The intraoperative core temperature was measured via a nasopharyngeal temperature probe (Bluepoint Medical Temperature Sensor AR 275 PA).
After completion of surgery, upon arrival at the PACU, core body temperature (tympanic) was recorded and then measured hourly for up to 6 h postoperatively. All PACU measurements used the same handheld infrared tympanic temperature device (Temperature Teller Plus GS-903) and the same technique as the baseline temperature measurement.
The sample size was based on the difference between two means with reference to Horn et al (2016). For a two-sample t test with 5% significance, effect size ≈0.5, 80% power and ~10% anticipated dropouts, the required size was 72 (36 per group) (Horn et al 2016).
The data collected were compiled in a Microsoft Excel spreadsheet, and statistical analysis was performed via Jamovi software (version 2.3.28). Descriptive statistics are presented as the means and standard deviations or medians and interquartile ranges for continuous variables and percentages for categorical variables. Student’s t test or the Pearson χ² test was used to compare baseline characteristics between the two groups. The chi-square test was used to obtain the p value for the secondary objective. A p value of <0.05 was considered to indicate statistical significance.
Results
A total of 80 patients were screened for eligibility and enrolled in the study. Forty patients received prewarming, whereas another 40 received no prewarming. In the prewarmed group, four patients were excluded: two patients who experienced epidural catheter placement failure and two patients who did not receive epidural infusion intraoperatively. In the non-prewarmed group, three of the patients were shifted to the intensive care unit due to prolonged surgery, whereas one patient did not receive an epidural infusion intraoperatively. After excluding four patients from the prewarmed group and four patients from the non-prewarmed group, a total of 72 patients completed the study and analysis, with 36 patients in each group, as shown in Figure 1.
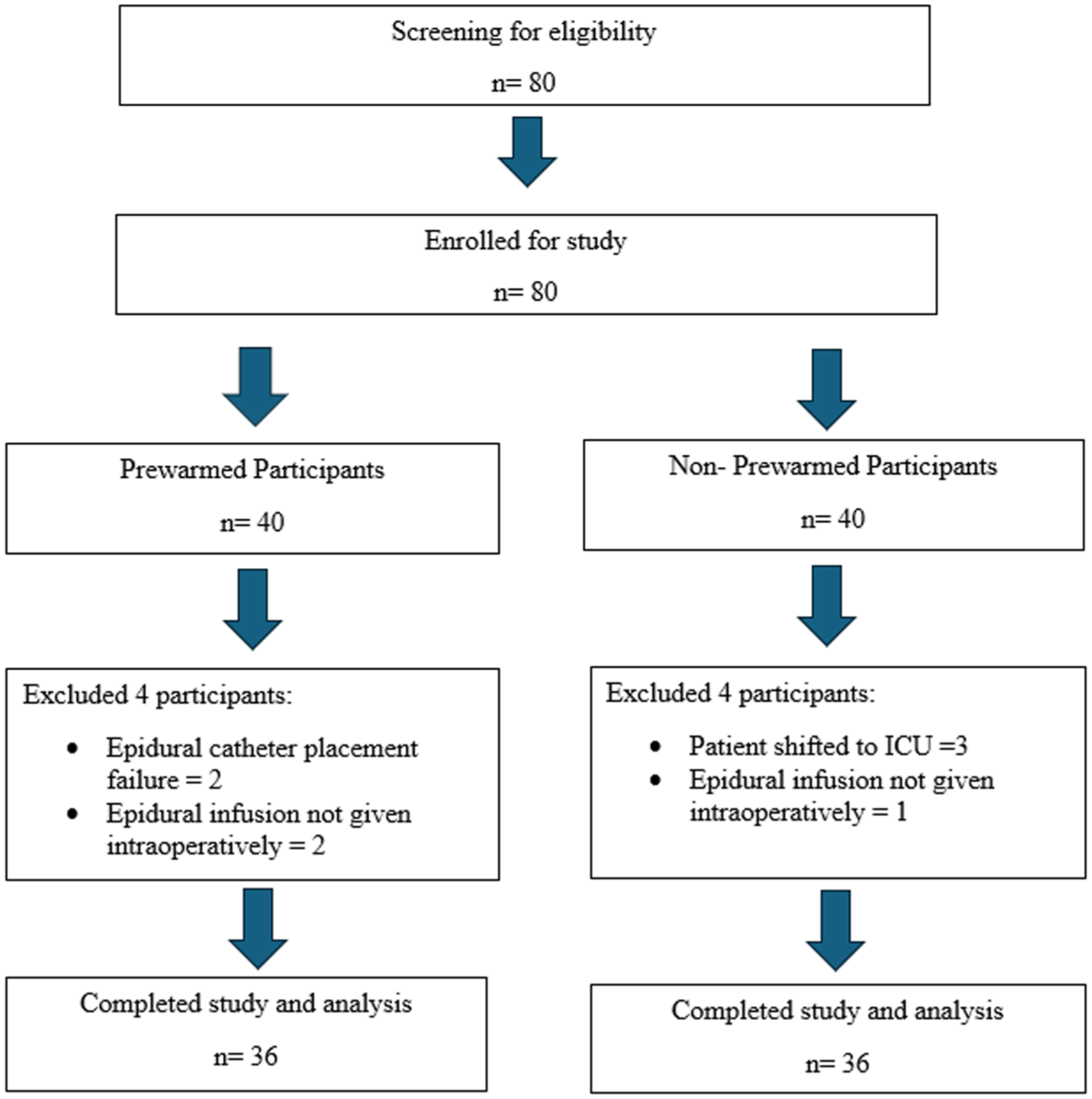
Patient flowchart (n = number of participants)
The two groups were comparable with respect to age, BMI, ASA status, duration of surgery, site of epidural insertion, rate of epidural infusion, type of surgery and temperature of the environment (Table 1). The prewarmed group included nine participants aged more than 60 years, whereas the non-prewarmed group included 12 participants. The duration of surgery ranged from 3 to 9 h in both groups, and the epidural infusion rate varied between 3 and 8 mL/h. Surgical procedures included pancreatectomies, hepatectomies, radical nephrectomies, cystectomies, cytoreductive surgeries, colectomies, anterior resections and exploratory laparotomies. When prewarming was performed, the mean duration of prewarming noted was 16.2 (2.3) min.
Demographic data
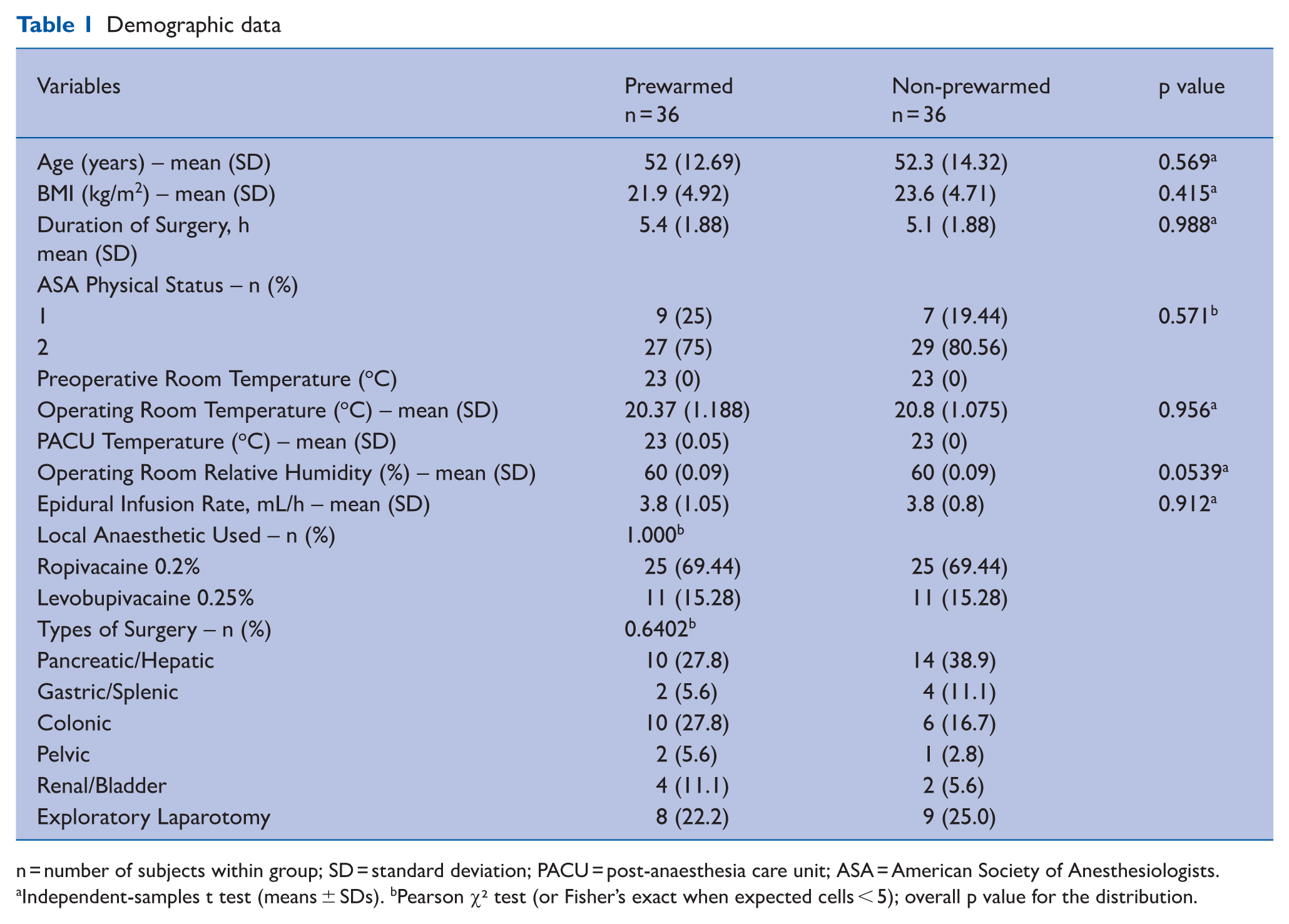
n = number of subjects within group; SD = standard deviation; PACU = post-anaesthesia care unit; ASA = American Society of Anesthesiologists.
Independent-samples t test (means ± SDs). bPearson χ² test (or Fisher’s exact when expected cells < 5); overall p value for the distribution.
The change in temperature during the perioperative period was calculated as the difference between the baseline temperature and the temperature recorded upon arrival at the PACU. The median temperature drop was 0.5 °C in the prewarmed group and 0.75 °C in the non-prewarmed group (Table 2). A Hodges–Lehmann median difference (non-prewarmed − prewarmed) of 0.2 °C was noted but may not be clinically significant.
Changes in core temperature (°C) from baseline to PACU arrival

n = Number of subjects in a particular group. IQR = Interquartile range; PACU = post-anaesthesia care unit.
The maximum difference was observed immediately postinduction [MD of +0.4], as expected (Table 3).
Trends of perioperative core body temperature in prewarmed and non-prewarmed patients
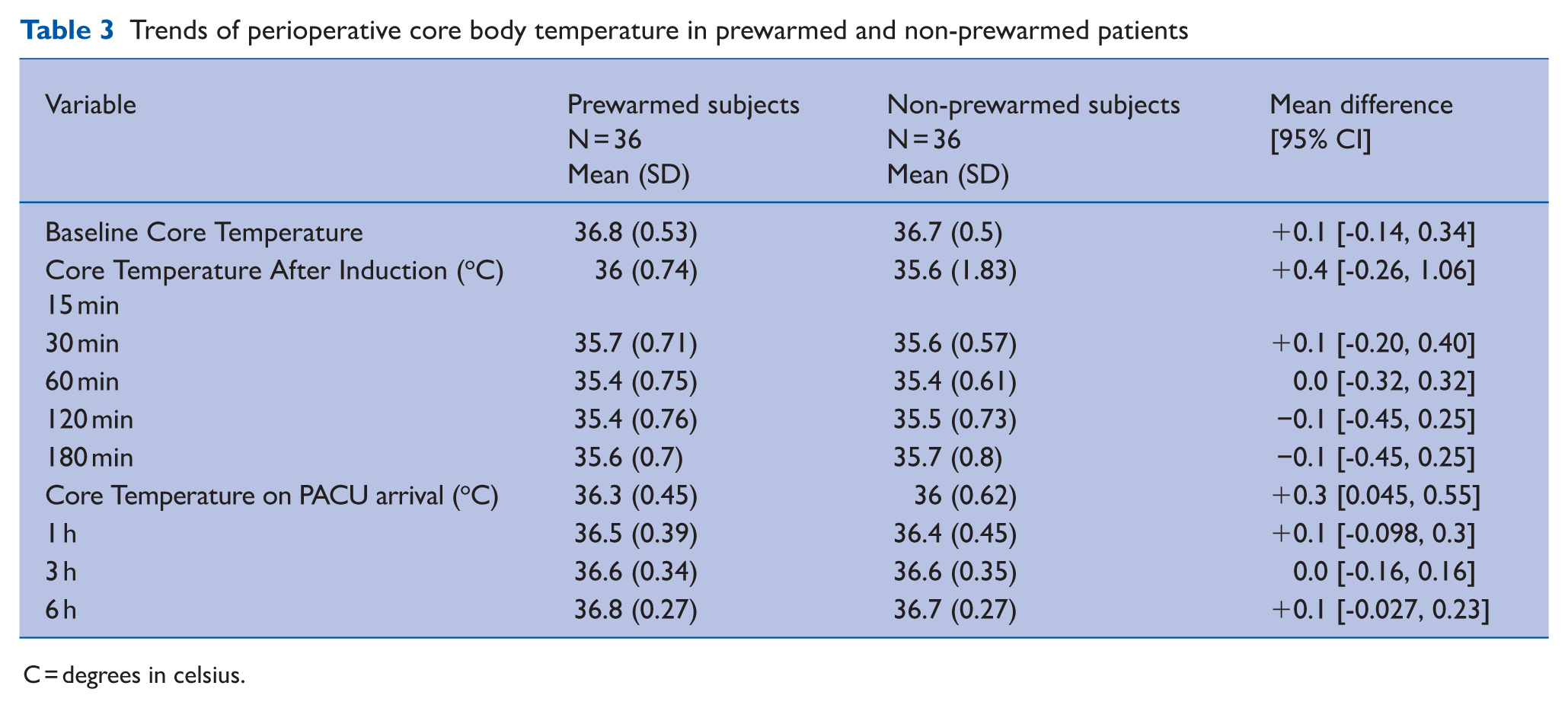
C = degrees in celsius.
A relative risk (RR) of less than 1 indicates that prewarming was associated with a reduced risk of postoperative hypothermia and shivering. Both outcomes were significantly different between groups, with p values <0.05 (Table 4).
Association between PACU hypothermia and shivering
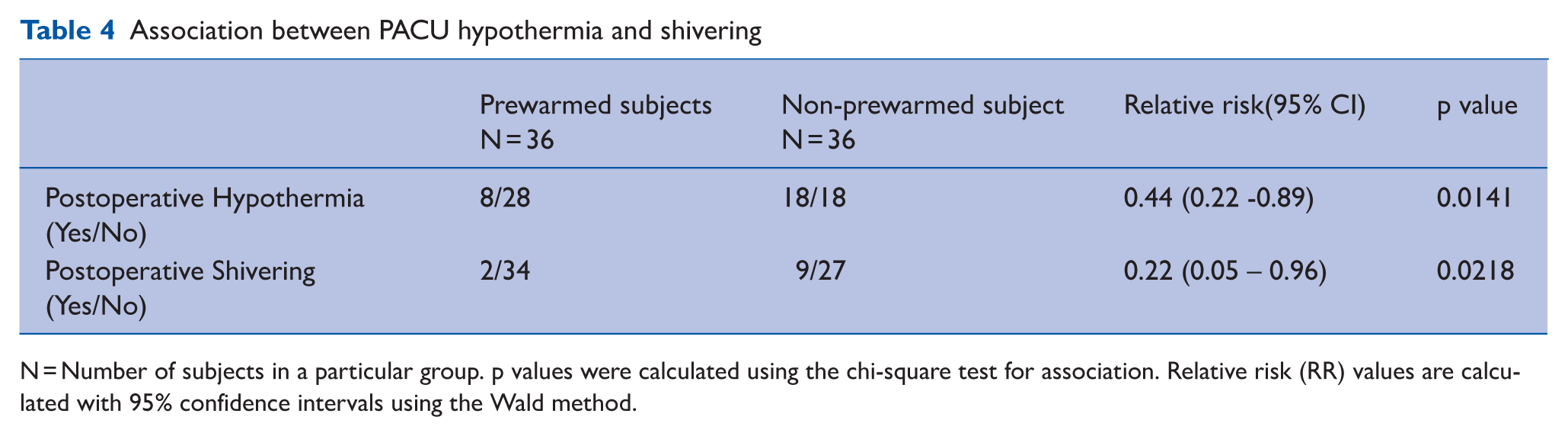
N = Number of subjects in a particular group. p values were calculated using the chi-square test for association. Relative risk (RR) values are calculated with 95% confidence intervals using the Wald method.
Discussion
In this prospective observational study, prewarming patients for 15 min before the placement of an epidural catheter and the induction of general anaesthesia was associated with a smaller perioperative drop in core temperature and a lower incidence of both hypothermia (<36 °C) and shivering postoperatively.
Multiple systematic reviews and meta-analyses have demonstrated the effectiveness of prewarming in reducing perioperative hypothermia across various surgical procedures (Madrid et al 2016, Uçak et al 2024). Clinical guidelines, including those from the German Society of Anaesthesiology and Intensive Care Medicine and the National Institute for Health and Care Excellence (NICE), recommend the use of prewarming as a standard practice, ideally for 30–60 min before surgery (Grote et al 2018, NICE 2008, Sessler 2016). However, routine implementation is often constrained by time, staff and equipment shortages. A study from Germany reported only 13%–20% compliance with prewarming protocols (Gabriel et al 2019). Pragmatic strategies, such as shorter prewarming durations or cowarming, may be a path to balance efficacy and feasibility. Short-duration prewarming protocols have shown benefits in selected settings. For example, Horn et al (2012) demonstrated the benefit of ⩾10 min of prewarming in patients undergoing a short duration of surgery (<90 min) under general anaesthesia and 15 min of prewarming in patients undergoing caesarean section under epidural anaesthesia (Horn et al 2002), where it reduced postoperative hypothermia and shivering. Similar benefits have been reported under spinal anaesthesia and during laparoscopic gynaecological surgery (Lee et al 2020, Recio-Perez et al 2023).
Patients who undergo major abdominal procedures under combined general and epidural anaesthesia are at the highest risk to inadvertent perioperative hypothermia and may benefit the most from active warming strategies (Sessler 2016), justifying our focus on this cohort. Rosenkilde et al (2025) investigated the effect of prewarming in a population akin to ours and reported a postoperative hypothermia incidence of 33% in the non-prewarmed group compared with 6% in the prewarmed group following approximately 50 min of prewarming. The more pronounced effect observed in their study is likely attributable to the longer duration of prewarming. Horn et al (2016) reported that 15 min of prewarming after epidural insertion reduced the incidence of postoperative hypothermia from 72% to 6% in patients who underwent laparoscopic abdominal surgery. Kaufner et al (2019) evaluated the effectiveness of prewarming during epidural insertion via forced air warming (Bair Paws) and reported a smaller temperature decrease in the prewarmed group (−0.35 °C vs. −0.9 °C), although the exact duration of prewarming was not mentioned. Together with our findings, these reports support the clinical utility of a short duration of prewarming in higher-risk settings.
The physiological rationale for these findings has been studied previously. Under anaesthesia, core body temperature changes typically follow three phases: an initial redistribution phase due to anaesthesia-mediated vasodilation, a linear phase of temperature decline, over 2–3 h as heat loss exceeds production, and a plateau phase, where vasoconstriction limits further losses and a balance is reached between heat loss and heat generation (Ramaswamy 2025). Prewarming increases the peripheral heat content, narrows the core–periphery temperature gradient and blunts the redistribution drop. At high settings, 30 min of prewarming can add approximately 69 kcal of peripheral heat, which is approximately 1.5 times the heat typically lost during the redistribution phase (47 kcal) (Becerra et al 2019). This may explain why even a short duration of prewarming can offer measurable thermoregulatory benefits.
Our study provides real-world evidence of the benefits of a shorter duration of prewarming in patients undergoing major abdominal surgery. Further randomised control trials in such high-risk populations can confirm these associations and examine the effects of prewarming on other outcomes linked to intraoperative normothermia, such as surgical site infections, perioperative bleeding and recovery metrics.
This study has certain limitations that must be acknowledged. First, this was a prospective observational study in which allocation to the prewarmed group was based on the availability of a forced air warming device and logistical feasibility, as determined by the attending anaesthesiologist. Although this non-randomised approach introduces the possibility of selection bias, it mirrors real-world clinical decision-making and provides valuable insight into the effectiveness of short-duration prewarming in routine practice. Second, core body temperature is measured via a tympanic thermometer – a non-invasive method that is inherently technique dependent. This method was selected to increase patient comfort while conscious, and efforts were made to minimise measurement variability through the use of a standardised measurement technique and a single trained observer for all readings.
Finally, the modest sample size and short follow-up period may limit the generalisability of the findings and preclude the detection of more subtle effects or delayed outcomes. Future studies employing randomised controlled designs with larger sample sizes and extended follow-up are warranted to confirm and expand upon these findings.
Conclusion
In adults undergoing major abdominal surgery with combined general and epidural anaesthesia, a 15-min prewarming protocol was associated with a smaller perioperative decrease in core temperature and lower incidences of postoperative hypothermia and shivering. Given its brevity and feasibility, we support implementing at least 15 min of prewarming when resources allow, specifically in major open abdominal surgeries. Because these data are observational, confirmatory randomised trials are warranted before mandating universal adoption.
Footnotes
Acknowledgements
We would like to acknowledge the Department of Anaesthesia, Kasturba Medical College, Manipal, for helping with planning and providing resources.
Author contributions
AKS: Conceptualisation, methodology, data collection and analysis, manuscript writing.
SKN: Conceptualisation, methodology, data collection and analysis, manuscript review and editing.
BDA: Methodology, manuscript review and editing.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval and informed consent statement
This study was carried out in Kasturba Medical College and Hospital, Manipal, after approval of Institutional Research Committee (IRC) on January 25, 2024, followed by approval of Institutional Ethics Committee 2 (IEC 2) on April 13, 2024, (EC/NEW/INST/2021/1707), and registration at Clinical trials registry India (CTRI/2024/07/070755) on July 16, 2024. Patient declaration of consent statement: Informed consent was obtained from all the participants before enrolling them into the study. Participants identity has been kept confidential.