
Abstract
Aim:
This study aimed to explore Australian health professionals’ perceptions and experiences regarding built environment planning for operating rooms.
Methods:
We conducted semi-structured interviews and a focus group using exploratory qualitative methods, involving 16 participants: anaesthetists, surgeons, nurses, theatre technicians and designers of operating rooms.
Findings:
Four core concerns of participants were analysed: Engagement, Respect & Collaboration; Foreseeing & Responding to Safety Concerns; Enhancing Design Planning to Minimise Internal & External Consequences; and Ambiguous Application of Standards in Operating Room Design Planning.
Conclusion:
Health professionals highlighted safety impacts related to patients and staff due to the built environment and emphasised the need for improved engagement, respect and collaboration in design processes. Consideration needs to be given to the lived experiences of health professionals in design planning to address safety concerns effectively. Hierarchies and cultural factors were identified as barriers to inclusive design processes.
Keywords
Key points
This research provides insights from end users related to the design of the built environment, highlighting the importance of collaborative design processes to create safer and more functional operating room (OR) environments.
The lack of transparency in design planning processes and the exclusion of end users resulted in missed opportunities to address safety concerns effectively, leading to feelings of disrespect among OR staff.
Conflicts arose from competing priorities between stakeholders, with decision-making often influenced by hierarchy, culture and politics rather than practical considerations or end-user needs.
OR staff raised safety concerns related to design proposals, emphasising the importance of addressing workflow challenges, minimising environmental risks and ensuring staff and patient safety through comprehensive design planning.
Introduction
The layout and design of operating room (OR) spaces significantly impact workflows, processes and the safe delivery of patient care. Studies have shown that the layout of the OR directly affects surgical performance, with disruptions arising from the positioning of equipment, furniture and fixed structures (Bayramzadeh et al 2018, Joseph et al 2019, Jurewicz et al 2020). The planning and design process for new healthcare environments develops across several stages with healthcare providers outlining users’ needs, care models and clinical programmes in a functional brief. Architects interpret the brief to develop an initial concept, which is refined into a detailed design. Construction follows the finalised design (Bernhardt et al 2022, New South Wales (NSW) Government 2024). The OR situated at the heart of operating suites must fulfil diverse requirements while adhering to regulatory standards (AusHFG 2018, Australian College of Perioperative Nurses (ACORN) 2020, Love & Steel 2022). The planning and design of OR spaces aimed at ensuring safe patient care represents a complex, critical and costly endeavour.
Well-designed hospital environments can increase staff effectiveness and satisfaction, reduce errors and infections, and decrease stress and injuries (Bernhardt et al 2022, Joseph et al 2019). Evidence-based design (EBD) research highlights the link between staff wellbeing, productivity, satisfaction and the physical environment of hospitals (Connellan et al 2013, Ulrich et al 2008). In recent years, a focus on optimising patient safety, improving surgical outcomes and enhancing efficiency has emphasised the importance of deliberate and strategic design within the OR environment (Allison et al 2021). Future OR design must be grounded in evidence, as various aspects of OR design have significant impacts on patient safety and staff performance (Joseph et al 2018, Neyens et al 2019). Through understanding the perspectives of health professionals working within ORs, this study seeks to inform decision-making in future OR environment design projects.
Literature review
A growing body of literature across health and architecture emphasises the need for EBD and interdisciplinary collaboration. Current strategies incorporate human factors and evaluation through simulation frameworks and post-occupancy evaluation, emphasising functionality, efficiency and safety including layout, lighting, ventilation and infection prevention measures (Brambilla & Coapolongo 2019, Ottosen Engebretson, & Etchegaray 2017, Shultz et al 2020, Torres-Landa et al 2018). Past research relating to users of the space and the physical environment within the OR have focused on user satisfaction, effectiveness of design communication and post-occupancy evaluation (Joseph et al 2019, Pomare et al 2021, Shultz et al 2020, Wingler et al 2018).
Overall, literature establishes the importance of integrating environmental considerations such as lighting and air quality and staff engagement into the design process of ORs, aiming to create safe, efficient and user-centred healthcare environments. Challenges persist in understanding the complex relationship between OR design and clinical outcomes. Catchpole and Alfred (2020) describe traditional evidence may not fully explain this relationship due to the complex, adaptive nature of surgery and the environment; research outcomes or efforts to understand design impacts lack direct correlations between OR design and clinical outcomes. While guidelines and design principles exist advocating for the inclusion of end users, there is a lack of emphasis on OR staff engagement in design planning within literature. Questions that need to be asked include ‘how are health professionals involved in designing ORs in Australia?’ and ‘how can safety be improved?’. There is a need for further research to guide OR design.
Methodology
This study utilised a mixed-methods sequential design to investigate OR staff involvement in built environment design planning, with a focus on safety and function. Built environment design refers to physical construction elements, ambient features such as air quality, and interior design aspects such as furniture, signage and equipment (Bernhardt et al 2022, Ransolin et al 2022). This approach aligns with the research question because the perspectives of OR health professionals related to OR design planning are unknown. An exploratory sequential mixed-method design begins with a small qualitative study which informs the development of a quantitative survey tested with a larger sample (Creswell & Plano Clark 2017). This article presents the first phase of this study using Constructivist Grounded Theory (CGT) as a qualitative framework. The developing qualitative theory formed the foundation for a quantitative survey. Results are being compiled for integration into an overarching theoretical framework.
Grounded Theory (GT) emphasises data-driven analysis, constant comparison and theoretical sampling to develop theory, with CGT valuing new theory construction and process over static description (Charmaz 2006, Glaser & Strauss 1999). The resulting theory is grounded in social reality, shaped by individual and collective actions rather than external structures (Charmaz 2006). CGT was selected for this research due to its focus on generating theory from data, enabling the identification of factors that improve safety and function in OR design. Unlike other methodologies, CGT acknowledges the researcher’s subjectivity and encourages active participation in theory generation alongside participants. Integrating various data sources, CGT offers a comprehensive and practical approach to address the goals of this research in recognising diverse perspectives on safety and function. In addition, CGT aligns with the researcher’s constructivist and pragmatist worldviews, facilitating a thorough exploration of both intrinsic and extrinsic factors, providing a broader understanding compared to other methodologies such as phenomenology or ethnography (Charmaz 2006).
Methods
Conducted in two metropolitan tertiary public hospitals in South Australia in 2021, the research used purposive sampling to recruit participants from various health professional groups working within ORs to access participants possessing characteristics and experiences relevant to the research topic. Recruitment occurred through meetings, forums and flyers distributed within hospital settings. The study population were health professionals who had experienced working within a newly designed OR and those who had experienced redevelopment of existing ORs within an operating suite within the past five years in both public and private settings. Exclusion criteria applied to those not directly involved in intraoperative care.
Semi-structured interviews and a focus group were conducted with a total of 16 participants, including surgeons, anaesthetists, OR nurses, technicians and designers. Although focus groups with various roles were planned, time constraints limited participation, resulting in one focus group with two nurses. Another three people contacted the researcher to participate but were unable to attend.
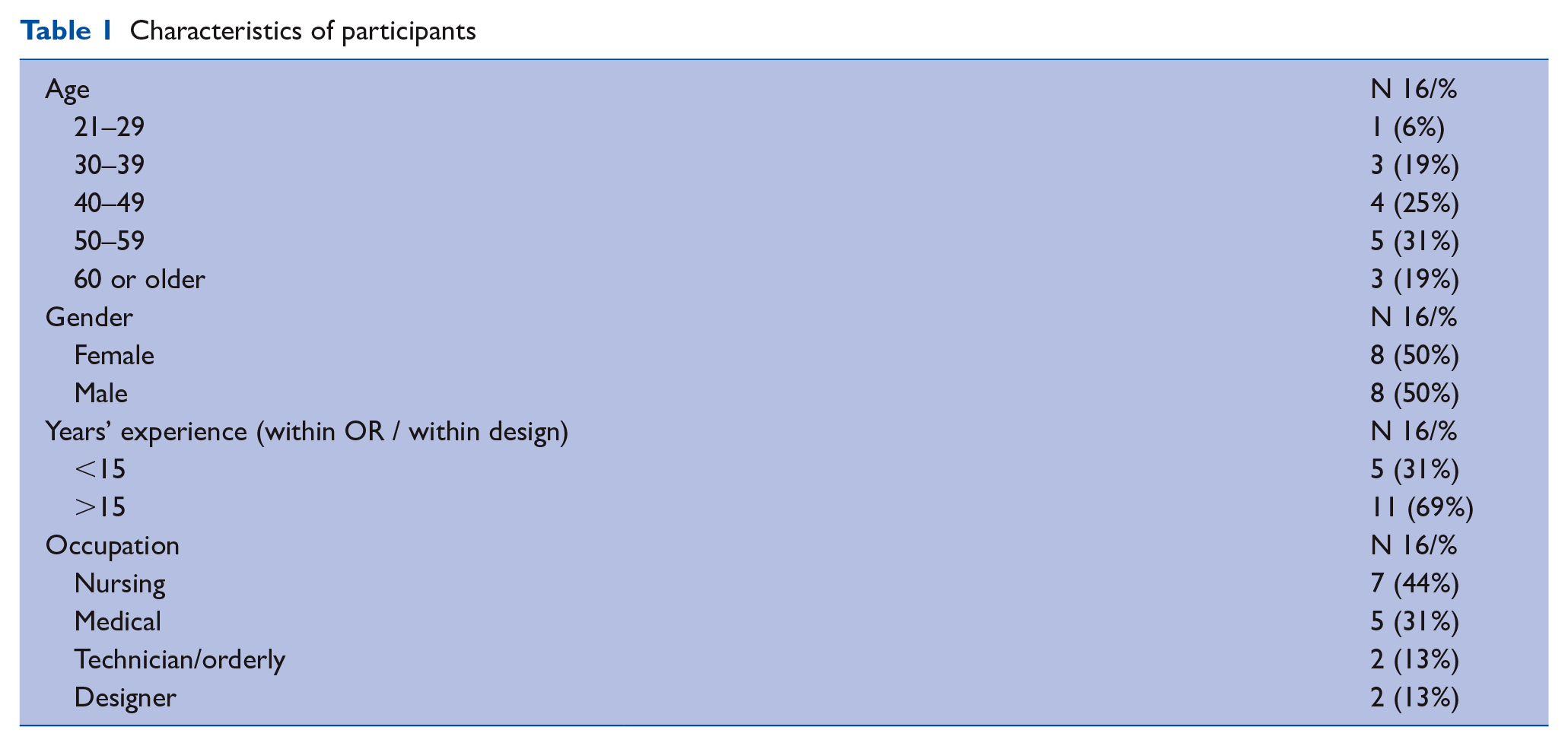
Interview questions derived from research aims and literature including design communication media used (Wingler et al 2018) guided data collection and analysis. Face-to-face interviews and focus group collected data on OR design elements, impact on safety within the OR and end user engagement in planning. Participants consented in writing to audio-recorded interviews and focus group with the principal researcher, ensuring a record of their perspectives. In total, 7.45 hours of audio recordings were transcribed and coded. Transcriptions were conducted by an independent service, and data were deidentified to protect privacy. Demographic data was collected (Table 1). The first author and principal researcher, experienced in qualitative interviews (Irwin et al 2018) and as an OR nurse, conducted data collection. Memo writing was undertaken by this researcher to assist analysis and theory building to inform theoretical sampling. Theoretical sampling continued until saturation was achieved, indicating no further insights from additional data related to emerging categories (Charmaz 2016).
Characteristics of participants
Ethics
Ethical approval for the research was obtained from both the research site ethics committee (CALHN 13748) and the university ethics committee (UoA H – 2020 – 34823).
Analysis
The research employed the constant comparative method, a core tenant of CGT, for data analysis (Charmaz 2016). Analysis starts as soon as possible and continues in parallel with data collection allowing for theoretical sampling and iterative refinement of categories (Charmaz 2016). Coding occurred in three stages: initial, focused and theoretical. Data collection and analysis occurred simultaneously as the researcher moved between coding, collecting data, memoing to identify gaps and then back to coding (Irwin et al 2024). Figure 1 demonstrates total codes and sequence of coding activities. Coding identified similarities and differences, with subsequent data collection guided by emerging categories and insights. NVivo for Mac (version 12) was utilised for managing data, with regular collaborative discussions among authors to ensure consistency in coding and analysis.
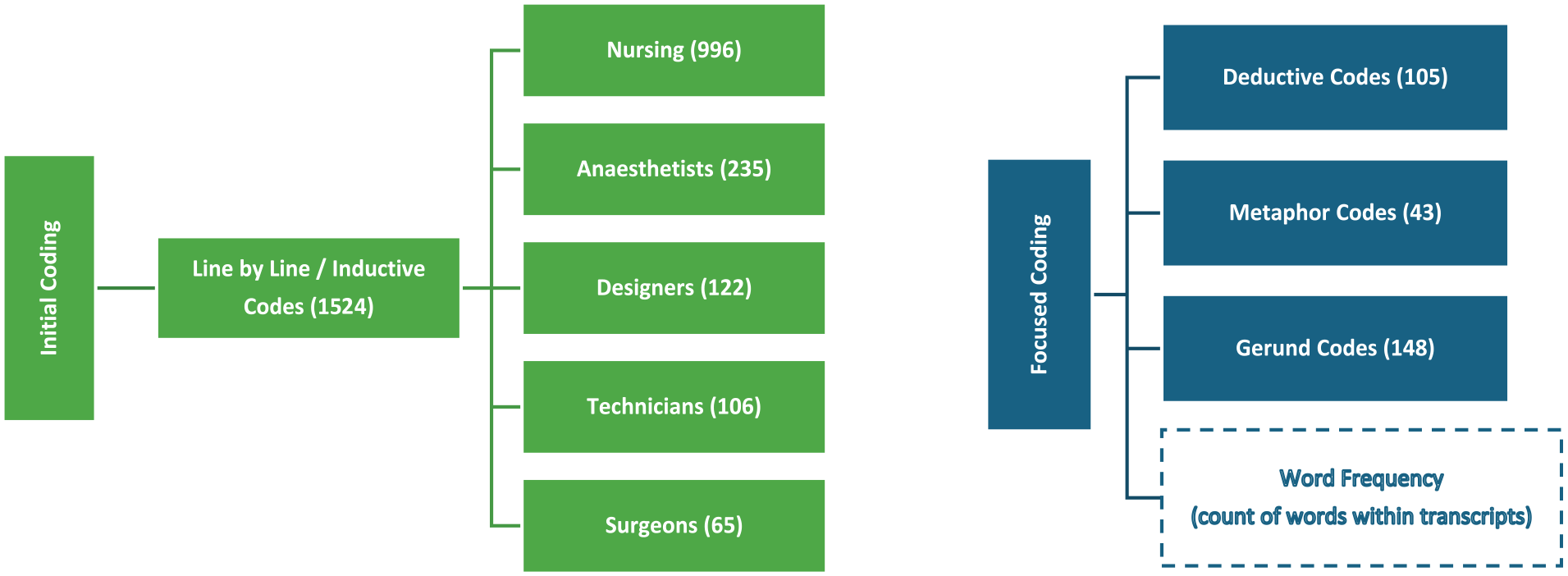
Total codes and process
Additional interview questions were informed by ongoing data analysis, particularly regarding perspectives on design communication media during planning. It emerged end users did not understand the processes involved in design planning and described experiencing conflict in design user groups. Ethics approvals were subsequently updated to include the recruitment of designers who offered valuable perspectives on design impacts and engagement processes.
A list of design factors related to ORs, drawn from the literature review, served as prompts to stimulate discussion and further explore design elements and their impacts during interviews and focus group. The list included various aspects of OR design, including layout, size, air quality, temperature, patient and staff movement, workflow, waste management, surgical instrumentation and equipment, as well as the relative locations of individual spaces adjoining the ORs and between different zones (eg: restricted, or non-restricted zones). As participants naturally referenced these factors during descriptions of their experiences, it served as a guide for the principal researcher post-interview, aiding in memoing. The list functioned as a valuable tool for organising and analysing data collected.
The actions observed during analysis when coding gerunds revealed the effect of the design on the users of OR spaces and linked the concerns of OR staff and designers with specific impacts for surgical patients and staff (Irwin et al 2024). Word frequency queries and data observation techniques were used to confirm codes and identify theoretical significance, including the exploration of metaphors and analogies used by participants to describe their concerns (Bernard et al 2017). Memos were utilised to capture data abstractions and identify relationships between categories (Charmaz 2016). A memo was completed by the principal researcher immediately following interview, each coding activity and when confirming theoretical concepts. In preparing to code data, memos were undertaken capturing preconceived ideas and identified bias of the principal researcher.
Results
Comprehensive analysis of rich data exploring OR staff experiences resulted in four qualitative concepts, as shown in Figure 2. CGT encourages the development of theoretical concepts rather than themes which may be too rigid in development of a theory (Charmaz 2016). These concepts reflect the core concerns of OR staff, encompassing engagement in design planning and working within the space. Participants detailed work dynamics, emphasising design considerations and safety implications for patients and staff.
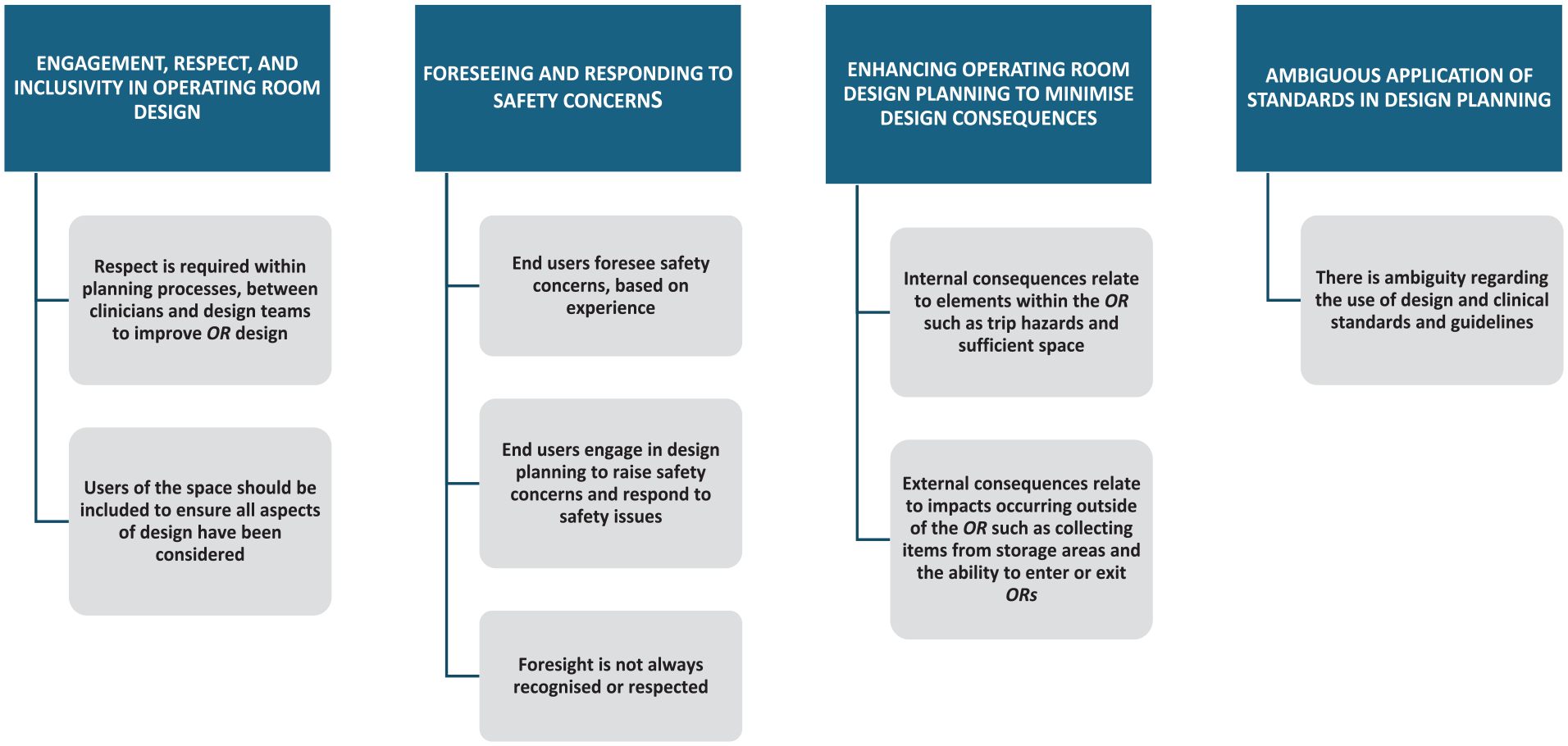
Concepts reflecting core concerns related to operating room built environment design and safety
Engagement, respect and inclusivity in operating room design
Respectful engagement in planning and a level of inclusivity for OR staff that was meaningful was a key insight from participant perspectives. Health professionals and designers described the relationships between end users and the OR space as well as the relationships in design planning with design teams, managers, colleagues and the broader context of healthcare. Participants described that new technology that may be integrated into a new design and explained how the built environment affected their ability to provide care. They cited examples of effective and ineffective designs, illustrating the complexity of OR work dynamics and the challenges in creating suitable and safe spaces due to technology, workflow and team interactions. One such challenge is incorporating relevant health professionals in design planning. An architect drew on an analogy comparing the process of healthcare design to the familiar experience of ordering a takeout meal at home:
How frustrating is that when it’s just you and your partner? Then it gets even worse when you’ve got you and your kids. Now we’re ordering takeout for an entire hospital, with something like 300 plus people involved representing 1500 people . . . it’s an absolute nightmare sometimes. (P15, Architect)
Hidden work and unheard voices
The process of design planning was hidden from health professionals, who lacked understanding of the design planning process, including involvement, components and decision-makers. Even those involved in developing design briefs or user groups noted hidden aspects, remaining uninformed or ‘in the dark’ (P10, Anaesthetist). Uncertainties about roles included in design planning and hidden aspects, such as budget for staffing, equipment and finishes, were evident. Nurses highlighted being asked for feedback after decisions were made, missing the chance to identify safety concerns initially. Managers and design teams sought feedback on how nurses could address design-induced workarounds:
It was more about ‘How can we make this work?’ . . . more about fitting the design rather than getting input into how things were designed. (P5, Nurse)
Not being heard was interpreted during theoretical coding as a lack of respect. An anaesthetist described being involved in a user group raising concerns and was subsequently removed from the design planning user group:
It was made clear that my opinions . . . were contrary to the belief of the management . . . when I started to voice my criticism too strong, I was uninvited to further meetings. (P10, Anaesthetist)
Conflicting priorities
Health professionals were conflicted about the position they find themselves in due to design planning and working within the healthcare system. Describing the dual nature of conflict, health professionals wanted to contribute to design but were unheard or excluded. If included, there was a desire or pressure to get the design right. Expressions like ‘They never listen anyway’ (P8, Nurse) illustrate the perceived inevitability of conflict and disrespect in both design planning and healthcare. Designers cautioned against involving too many people in user groups, citing potential problems due to numerous opinions and conflicting priorities:
Each department will have their own focus or priority, and they’re not necessarily as cognisant of the conflicting information that you’ll get between them . . . it’s always . . . a difficult balance. (P15, Architect)
Hierarchy, culture and politics impacting decision-making
Decision making in design planning may be political and specific design elements can be biased towards health professional roles. A designer cited the placement of a master clock in the OR, related to which role needed immediate visual access to the clock, dictating its location in the space. A decision was required from the health service regarding which medical role this element should be biased towards. This designer also described an example of a post anaesthetic space, questioning if the design should be biased to the way work is undertaken by nurses or anaesthetists:
Who do you bias the room towards, the one who’s using it most often or the one who’s most . . . [sighs] I’m trying to be delicate with my words, but the most important in the room? (P15, Architect)
Surgeons emphasised the political nature of decision-making, highlighting how critical aspects of functionality might be overlooked during the process:
Politicians and people who are making decisions getting advice from bureaucrats and non-clinicians . . . and often overriding the recommendations of the clinicians. (P14, Surgeon)
Medical staff were described as asserting more influence in decision-making compared to other health professionals. In the private sector, a nurse observed reduced medical staff involvement, making the design process seem easier. Health professionals emphasised the importance of involving end-users in the design planning process. When asked about the stakeholders who should participate in OR design planning, an anaesthetist elaborated:
I think everyone working there . . . what I’ve realised also with Covid is how essential each part of our team is to the whole . . . and if you leave one out it . . . it just doesn’t work. (P11, Anaesthetist)
Foreseeing and responding to safety concerns
Health professionals described raising safety concerns related to proposed designs with colleagues, managers and design teams when contributing within user groups however missed opportunities in design planning are evident. Not engaging users of the OR space, asking nurses to develop suitable workflows once the space had been constructed and not considering specific elements were identified as missed opportunities to improve built environment design.
Poorly performing workflows and environmental impacts
The primary safety concern within the OR revolved around access to essential support, clinicians and critical equipment for both patients and staff. Nurses described the importance of access to emergency equipment:
Accessibility . . . is really important both from a staff and patient safety issue, because if it’s too far away . . . you’re increasing the amount of time before a patient gets access to the treatment they need. (P5, Nurse)
Delays in accessing necessary items can prolong patient anaesthesia time and jeopardise patient outcomes. Participants highlighted the risks associated with long distances within the operating suite, which can lead to delays and compromise patient safety:
[Distance] is extremely important . . . where the distances are so great . . . you might wait 20 minutes for something to arrive, . . . which is a huge waste of theatre time and money . . . and obviously dangerous. (P12, Surgeon) Distance has been a huge thing that’s made it . . . really hard to work in. (P9, Nurse)
Travelling long distances in emergency situations posed challenges in providing immediate support critical for patient outcomes. An anaesthetist stressed the time taken to access ORs created risk:
we’ve had near-misses . . . we put patients at risk by . . . that distance. (P10, Anaesthetist)
Challenges stemming from the built environment impact workflow performance and staff safety, with concerns ranging from trip hazards to excessive noise levels due to materials used affecting communication and increasing staff fatigue:
They still have a lot of noise problems . . . the anaesthetic rooms are very noisy . . . which makes communication with the patient difficult there. (P4, Anaesthetist)
Doors were described as causing staff injury, delays in entry and exit of the space, impacting patient dignity/privacy if a door opens to an external space and is visible to those passing through corridors or other areas and a threat to the aseptic environment. Instances of injuries, such as broken fingers and caught limbs, as well as equipment damage, were described due to heavy doors with automatic sensors:
We’ve had minor injuries . . . broken fingers. (P10, Anaesthetist) You sometimes risk contaminating a field because . . . you’re right by the thoroughfare . . . the doors are opening and closing in the middle of the procedure. So, they’re not maintaining airflow. (P3, Nurse)
The desire to create flexibility within the design, while considering future technology and space required, was described as ‘future proofing’ and was considered important not only to build a sufficient space but acknowledging cost, service provision and adaptability implications.
Design teams may not be reflective of end users
All OR staff roles noted that design teams often lack representation from end users, leading to gaps in understanding current workflows and challenges faced in the OR. This lack of representation results in decisions made by management or senior clinicians who may not be familiar with the intricacies of day-to-day operations within the OR environment. Health professionals stressed the importance of including individuals with firsthand experience working in ORs during the design process to ensure that the design reflects the needs and realities of end users:
I think sometimes the teams that are chosen from management, rather than trying to involve more people on the floor . . . those that’ve worked in multiple theatres . . . across different . . . countries, or different types of hospitals. (P6, Nurse)
A surgeon elaborated on the planning process for newly designed ORs aimed at minimising risk associated with intraoperative chemotherapy. The plans involved incorporating control rooms to enable staff to avoid exposure. A surgeon noted that this risk was particularly concerning within current ORs:
They’re doing that complex chemotherapy stuff which is highly toxic . . . in an area where they don’t have control of the airflow, because it’s coming into my theatre . . . [laughs] So, does that make me nervous? Yes! [laughs]. (P14, Surgeon)
Health professionals emphasise the importance of involving relevant stakeholders in the planning process to address safety concerns effectively. Nurses identified if given the opportunity to be involved, safety concerns would be raised based on lived experience. An anaesthetist highlighted how the shape of the OR and location of doors and airflow can affect the orientation of the operating table, demonstrating the complexity of design decisions:
With all the intentions we had in how to set up each different theatre, then the surgical teams moving into them then decided otherwise . . . and made some things not work as we intended. (P11, Anaesthetist)
Factors like power point access, door functionality and space flexibility contribute to unintended outcomes, including insufficient storage and disrupted workflows. A nurse emphasised the gap between theoretical design concepts and practical functionality, highlighting common challenges in design implementation:
I think there’s a lot of things that you think sound really good and will work really well in theory but, when you put it into practice, sometimes it’s not as functional as you’d like it to be. (P5, Nurse)
Enhancing operating room design planning to minimise internal and external consequences
This concept outlines elements to consider across different dimensions related to patient safety, physical space, staff safety, building structure and engagement in design planning. Internal consequences relate to elements within the OR such as trip hazards and sufficient space, while impacts occurring outside of the OR are due to external factors such as collecting items from storage areas and the ability to enter or exit ORs.
Minimising design consequences
The dimension of patient safety within the OR included factors relating to access and proximity to critical items and support, adequate storage, reducing door openings to minimise contamination risks, exposure to infectious substances or harmful agents, maintaining unobstructed pathways for smooth movement, continuous monitoring of patient condition and safety measures throughout surgical procedures:
My biggest concern with staff safety is obstacles in the way. (P7, Technician)
Trip hazards, ergonomics, manual handling and equipment placement contribute to pathway obstructions caused by wires and cords, impacting all dimensions. The importance of considering staff safety and the OR environment in door design to mitigate risks and ensure staff safety was clear:
The wiring on the floor is crazy . . . we’ve got to put black mats to cover them . . . so no-one trips . . . that's what we have to do because the booms are in the wrong places. (P13, Technician)
Enhancing planning processes
Health professionals advocated for enhanced communication to improve OR design stressing the importance of managers explaining design choices and providing visual aids to foster staff understanding and involvement in the process:
The hardest thing about anything that involves building and design is having an understanding of what a space looks like, a space feels like, once you’re in it. (P5, Nurse)
A surgeon highlighted requesting with designers, an alternative design communication media to assist with planning through virtual reality (VR) and how this may have supported clinicians in design planning, such as assisting time poor clinicians to contribute and enabling an understanding of how staff movement to provide care was impacted. This request for support was not provided due to cost:
‘In terms of seeing whether, like, the theatre lights are too high or too low, whether they’re going to fit in terms of where the beds are, whether there’s room for anaesthetic equipment and things, to me that’s hard to do in two dimensions’ . . . ‘We’ve asked about virtual reality . . . but been told it’s too hard’. (P14, Surgeon)
A planner recalled a project where a full-scale mock-up failed to identify issues with lighting and equipment height. The effectiveness of the mock-up highlighted the challenge of incorporating lessons learned when critical functional aspects were overlooked by both designers and end users.
Ambiguous application of clinical standards in operating room design
Standards, including building codes and health facility guidelines, heavily influence OR built environment design. While some guidelines, like the Australasian Health Facility Guidelines (AusHFG 2018), can be adjusted to suit practical needs or consider future requirements, others are non-negotiable. Building standards were described as the domain of architects and designers with relevant knowledge, while adherence to clinical standards was described as the responsibility of healthcare providers involved in design planning:
All the Australian health ones . . . and then there’d be all the operating theatre, ACORN standards . . . everything from electrical safety to manual handling. I mean, the list would be extensive. (P6, Nurse) The disconnect between the architects who are saying ‘Well, this is the standard’, and then the clinicians saying ‘Well, that’s . . . that’s great, but that’s not gonna work’ . . . we found that, looking at a space, we could say for sure . . . ‘This is a standard, but it’s not gonna work for us’. (P1, Nurse)
Discussion
The importance of respect and collaboration between health professionals and designers to foster meaningful engagement and inclusivity in the planning phase was a core concern within this CGT study. While design planning processes may not be fully understood by end users, the consequences of poorly considered design are felt within the OR, compromising patient workflows and care. Health professionals seek to influence safety within the OR space, emphasising the importance of considering specific safety elements through engaging end-users in design planning. OR staff, as end users, offer invaluable insights based on their lived experiences in providing care. Their perspectives on safety, function and priorities differ according to their roles and activities in the OR. However, hierarchical and cultural dynamics in healthcare organisations can hinder effective design communication and collaboration. This emphasised design planning must strike a balance between the diverse needs and preferences of stakeholders, recognising that accommodating every individual requirement is unrealistic. Health professionals lack clarity about the integration of standards into OR design planning, leading to potential challenges in meeting regulatory requirements.
Research highlights a gap between architects’ designs and end-user preferences, emphasising the importance of understanding discrepancies in healthcare practices (Elf et al 2017), with studies advocating for EBD tools to align with actual work practices (Machry et al 2020, Ransolin et al 2022). Communicating with end users, evaluating design choices and ensuring options for engagement are available may promote contribution to planning processes. Results highlight the significance of enhancing OR design planning to minimise both internal and external consequences. This involves optimising the layout, functionality and safety features of ORs to mitigate risks to patients, staff and the surrounding environment. Elements within the OR are interconnected and influence each other with adequate storage, efficient layout and reducing distance between ORs and adjacent areas being crucial considerations within OR design planning. Involving experienced health professionals in OR design planning is crucial to account for the intricacies of the environment, including clinical complexity and safety concerns. Considering the underlying intentions of a design may help mitigate unintended consequences that can arise from design decisions.
Limitations of the study
Study limitations include focusing on one Australian state and conducting research during the COVID-19 pandemic in two metropolitan hospitals, impacting access to busy health professionals. The participant numbers may not fully represent colleagues’ perspectives. Exploring medical and nursing roles across surgical specialities could offer more nuanced insights. Findings may not be generalisable due to variations in OR environments and cultural factors; however, these findings serve to guide future OR design engagement, highlighting specific concerns of health professionals working within ORs. Future research incorporating perspectives of patients, administrators and facility managers could enrich understanding of OR design dynamics and contribute to comprehensive solutions.
Implications for practice
To address shortcomings in OR design and minimise safety risks, there is a need for greater engagement, respect and collaboration between health professionals and design teams.
To ensure that OR designs meet the needs and preferences of those who work in these spaces, it is essential to include the lived experiences and insights of OR staff in design planning.
Involving OR end users in design planning helps to incorporate their insights and preferences and promotes a more collaborative approach to OR design.
Design outcomes should balance the needs of patients, staff and operational requirements.
Conclusion
The findings of this research highlight the intricate relationship between design planning and the practical realities of work and provision of care occurring within the OR. This study emphasises the need for respectful engagement and inclusivity of OR staff in the design planning process. Participants stressed that meaningful involvement throughout the process is essential to effectively address safety concerns and ensure the practicality of design choices.
The categories of hidden work and unheard voices reveal significant gaps in communication and transparency within design planning. OR professionals often felt excluded from crucial decision-making processes, which led to frustration and missed opportunities to proactively address safety and functionality concerns prior to the build. In addition, conflicting priorities among different stakeholders emerged as a major challenge. These tensions impacted collaborative efforts and compromised the final design’s suitability for daily operational needs.
The critical importance of anticipating and addressing safety concerns within OR design was emphasised. Issues such as insufficient space, inadequate workflow design and safety hazards were identified as significant challenges impacting both staff and patient outcomes.
Overall, the research highlights the imperative for a more inclusive, transparent and collaborative approach to OR design planning. By prioritising the perspectives and experiences of end-users and integrating these insights into the design process, healthcare facilities can better align physical environments with operational needs. This alignment may ultimately enhance safety, efficiency and overall quality of care in OR settings. Future research and practice should continue to explore these principles to foster optimal OR environments that support both staff wellbeing and patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.