
Abstract
Postoperative lingual nerve injury is a rare but serious complication following airway management and can lead to significant discomfort and disability. This literature review explores the aetiology, clinical presentation, management strategies and potential preventive measures for lingual nerve injuries associated with airway management during surgery. A search of PubMed, MEDLINE, EMBASE Science Direct, Cochrane library and Web of Science databases was done since inception to January 2024, including any observational studies and clinical trials describing patients diagnosed with lingual nerve injury following airway instrumentation. Multiple risk factors for lingual nerve injury were identified. Anaesthesia factors include difficulty with intubation and use of laryngeal mask airway. Surgical factors are long duration of operation and surgery of the head and neck. Patient factor includes female sex. Anaesthetists should proactively inform patients about the potential for this nerve injury and control modifiable risk factors to mitigate the risk of injury.
Key Phrases
- Lingual nerve injury is a complication following airway management during surgery.
- Lingual nerve injury commonly presents as tongue numbness and altered taste.
- Many risk factors for lingual nerve injury include the sex of the patient, airway device, type of surgery and length of surgery.
- Management of lingual nerve injury includes expectant management, medical management using anti-inflammatories and multidisciplinary management of long-term sequelae.
Introduction
The lingual nerve is the terminal branch of the mandibular division of the fifth cranial nerve. It provides taste sensation to the front two-thirds of the tongue and innervates the submandibular and sublingual glands (Fagan & Roy 2023). It is located under the roots of the third molar and on the inner surface of the mandible, making it vulnerable to injury (Laxton & Kipling 1996).
Lingual nerve neuropraxia commonly presents as tongue numbness and altered taste in the anterior two-thirds of the tongue (Su et al 2018). Due to its proximity to other cranial nerves, a lingual nerve injury may not be isolated and may present with hypoglossal, glossopharyngeal, or recurrent laryngeal nerve damage.
Airway management can also lead to lingual nerve injury, with factors such as inappropriate-sized laryngeal mask airway (LMA), multiple attempts, high pressure in laryngeal mask cuff and difficult intubation (Brimacombe et al 2005). High pressure in the supraglottic airway devices may compress or stretch the nerve at the tongue’s edge or the mandible’s inner surface near the third molar and causes nerve injury (Thiruvenkatarajan et al 2015).
In addition, numerous medical conditions have been considered as risk factors, such as ankylosing spondylitis, rheumatoid arthritis and calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly and telangiectasia (CREST) syndrome (Brimacombe et al 2005).
Limited literature exists on its incidence, risk factors, presentation and treatment beyond individual case reports. This review aims to consolidate available literature and compile evidence on the management of lingual nerve injury.
Search strategy
We conducted a review of the literature to evaluate the current trends in postoperative tongue numbness following airway management. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist is detailed in Figure 1.
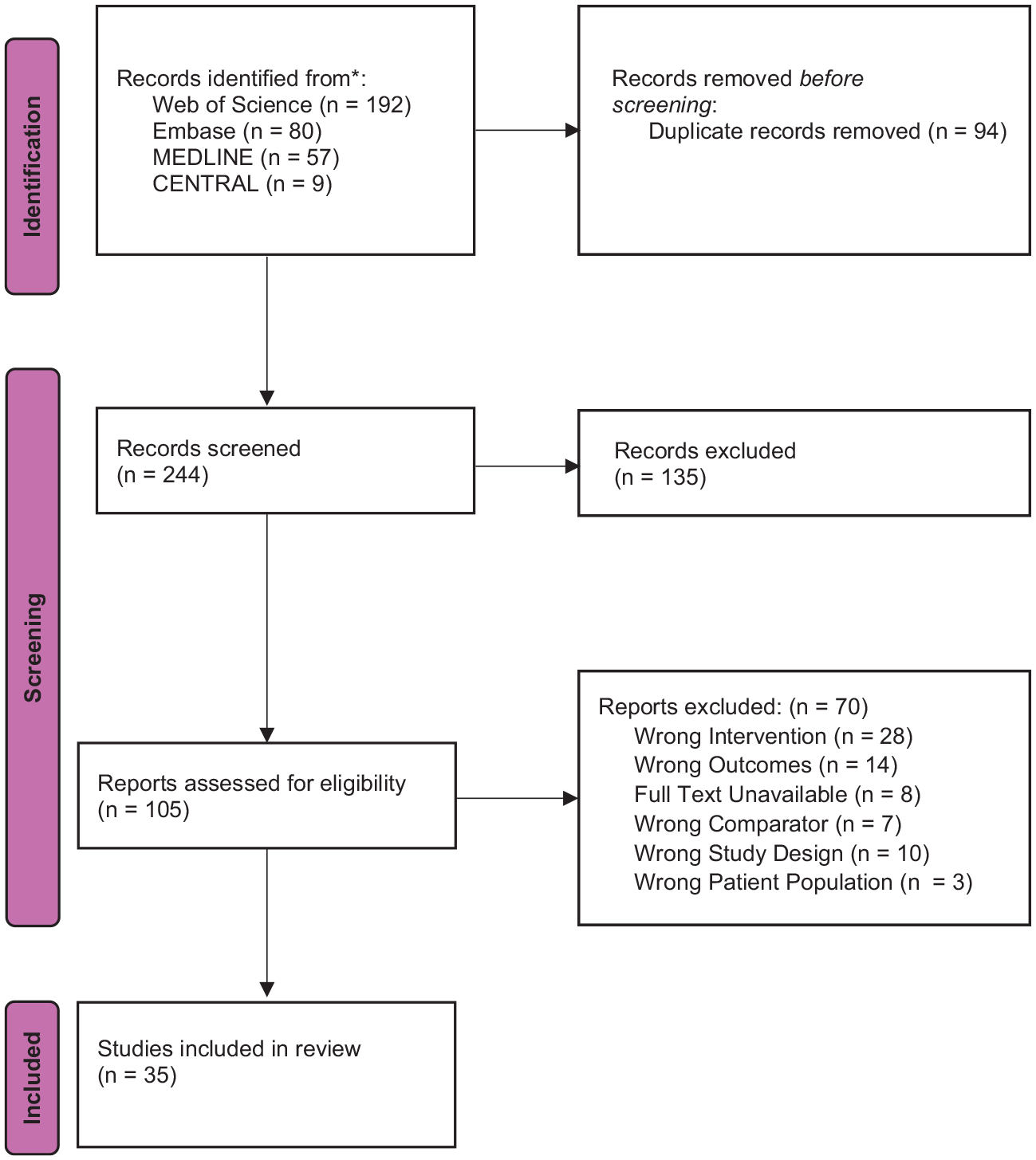
PRISMA flowchart summarising the process of article selection
A search of MEDLINE, EMBASE, Cochrane Library and Web of Science databases was performed for all literature until January 2024. The search terms were curated to identify literature discussing lingual nerve damage following airway management by intubation or laryngoscopy for surgical intervention. Detailed search terms to retrieve eligible studies were attached in an Appendix.
Inclusion criteria
We included literature discussing lingual nerve injury following airway management during surgical procedures. Observational studies, cohort studies, case reports, randomised control trials, clinical trials and multicentre studies were included. There were no restrictions placed on the publication year or geographical settings.
Exclusion criteria
Exclusion criteria included letters to editors, conference abstracts and commentaries. Any studies that were not presented in English or lacked available full text were excluded. We also excluded review articles, systematic reviews and meta-analyses.
Study selection
All the compiled literature from the databases was imported into Covidence. Automatic duplication checks were conducted by Covidence. Selected articles were screened by title and abstract, followed by a full-text assessment to ensure that these articles did indeed meet the eligibility criteria. Article selection was carried out by three independent reviewers with disagreements being resolved through a consensus decision. The PRISMA flowchart displays the number of studies included and excluded at each screening step (Figure 1).
Data extraction
We extracted patient-related perioperative variables, such as age, sex, American Society of Anaesthesiologists (ASA) score, Mallampati (MP) score and comorbid diagnoses. We also extracted the type of airway management done, such as the use of endotracheal tube, LMA, cuffed oropharyngeal airway or laryngoscopy. In addition, the difficulty of intubation and size of the airway was noted. We extracted data regarding postoperative outcomes, such as presentation, time to onset and resolution of symptoms, investigations and treatments.
Results
After removing duplicates, our search yielded 244 articles to screen. Following title and abstract screening, we had 105 articles available for full-text literature. After eliminating 70 studies, we included 35 studies in our review.
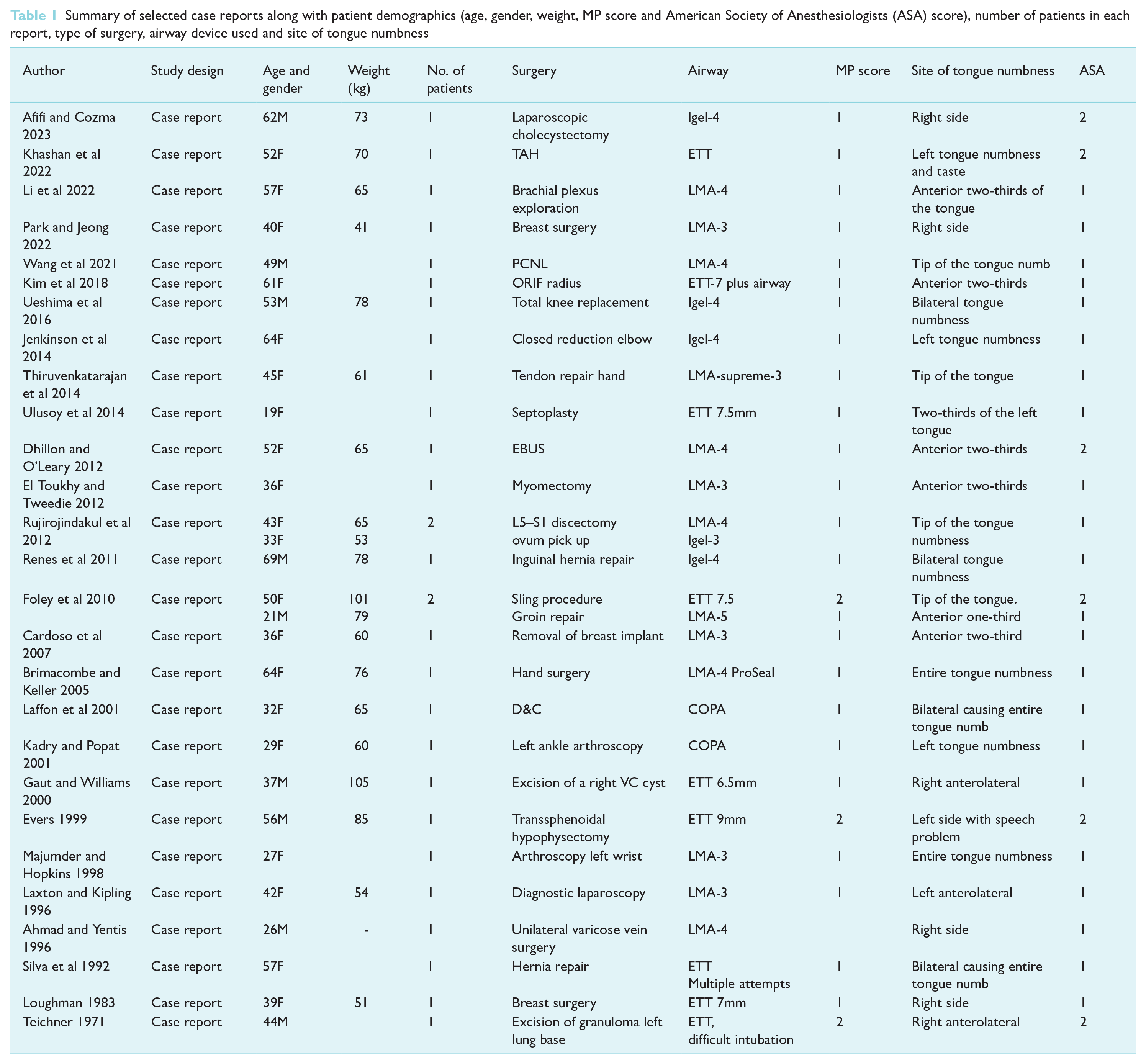
Our analysis identified 30 case reports that reported lingual nerve injury following airway management for 32 patients. Out of these, 21 patients had an LMA placed and 9 had an Endotracheal Tube (ETT) and 2 had Cuffed Oropharyngeal Airway (COPA)(Table 1).
Summary of selected case reports along with patient demographics (age, gender, weight, MP score and American Society of Anesthesiologists (ASA) score), number of patients in each report, type of surgery, airway device used and site of tongue numbness
Presentation of injury
Patients predominantly reported symptoms of loss of sensation in the anterior two-thirds of the tongue or taste disturbances either hours after surgery or at most 24 hours after the operation (Table 2). Patients may also suffer from an unpleasant taste of metal, old cheese, or ammonia. At times, they may encounter difficulty with word pronunciation (Hillerup 2007).
Summary of case reports selected along with surgical factors (type of surgery, duration, patient position), site of tongue numbness, onset and duration of symptoms, and interventions used
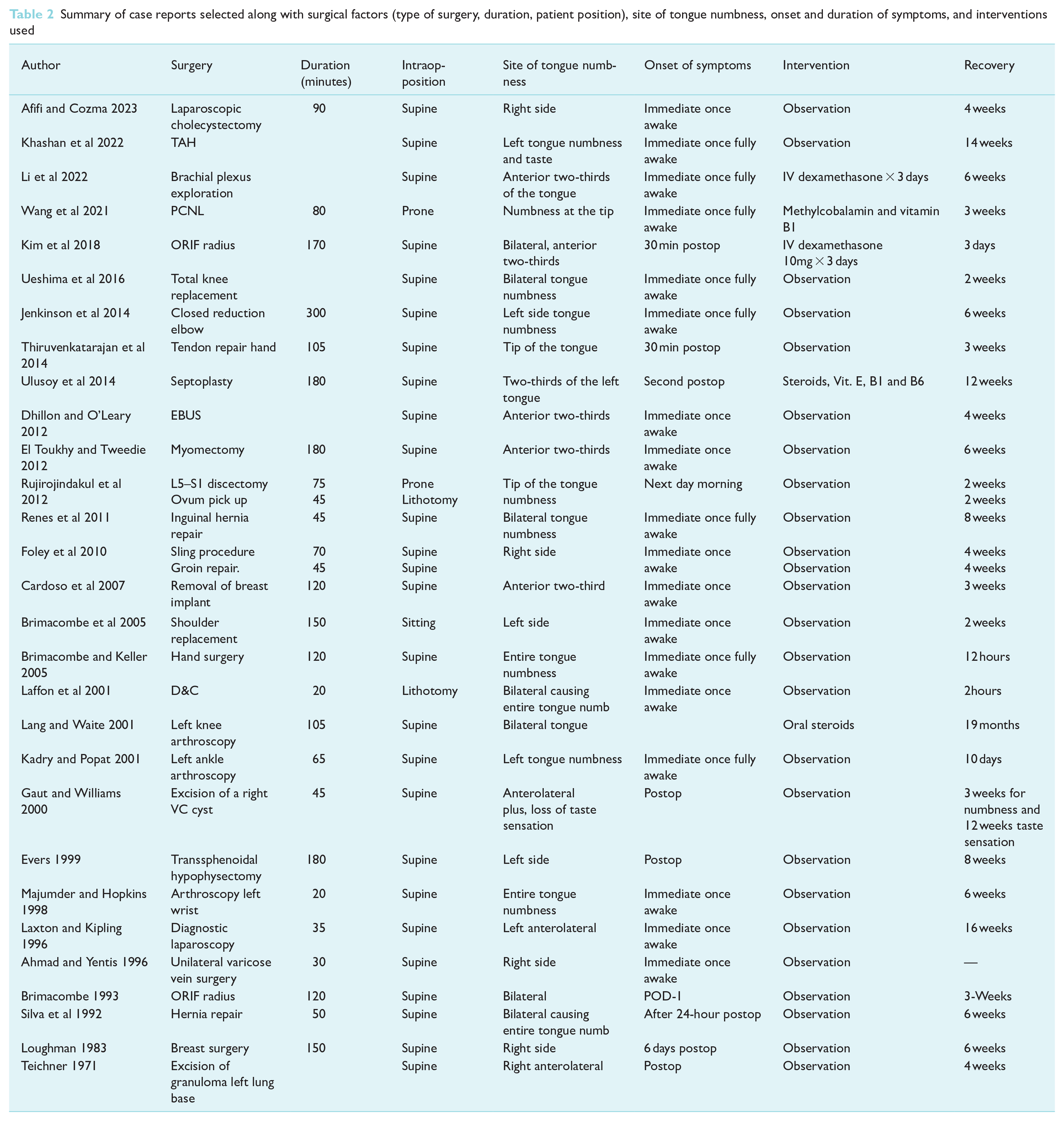
There is significant variability in the time until resolution of symptoms. Laffon et al (2001) reported a patient who resolved symptoms 2 hours post operation, while Lang and Waite (2001) reported their patient to be symptomatic 19 months after the surgery.
The majority of lingual nerve injuries were unilateral, seven reported to be left-sided, five right-sided, and the remainder not specified. However, among the 32 patients reported, 7 of them presented with bilateral lingual nerve injury and 3 presented with combined lingual nerve injury with glossopharyngeal, hypoglossal and inferior alveolar nerve injury (n = 1 for each). Furthermore, of the nine bilateral verbal nerve injuries, four of which were reported following ETT, with the five remaining being following LMA use.
Risk factors for lingual nerve injury
Several studies/case reports have identified factors that increase the risk of lingual nerve injury during surgery.
Su et al’s (2018) retrospective case–control study highlighted that head and neck operations significantly increase the risk of postoperative lingual nerve injury.
Ozdamar et al (2019) demonstrated that longer operation durations were a significant risk factor for lingual nerve injury. Tessema et al’s (2006) review in micro laryngoscopy cases also linked operations lasting more than 1 hour to higher incidences of tongue paresthesia and dysgeusia, likely resulting from lingual nerve injury.
Ozdamar et al’s (2019) findings showcased that experiencing difficulties during intubation was a major risk factor for lingual nerve injury.
Su et al (2018) noted that younger and healthier patients had a higher risk of neuropraxia. However, Tessema et al (2006) and Ozdamar et al (2019) did not find age a significant risk factor for tongue symptoms or lingual nerve injury.
Tessema et al (2006) and Ozdamar et al (2019) studies found gender-based disparities. Female patients, according to these studies, were more prone to lingual nerve injuries post-surgery (Ozdamar et al 2019, Tessema et al 2006) Ozdamar et al (2019) specifically demonstrated a higher complication rate in females following suspension laryngoscopy.
Ozdamar et al (2019) indicated that MP score, BMI and preoperative diagnosis were not significant predictors of lingual nerve injury.
Tan et al’s (2010) evaluation of LMA in 100 patients reported only one case of lingual nerve injury. However, most case reports linking LMA use to neuropraxia suggest a potential association.
This comprehensive overview of various studies provides a nuanced understanding of the multifactorial nature of lingual nerve injury, attributing it to surgery type, operative time, intubation difficulties, patient demographics (age and sex) and potential correlations with using LMA.
Treatment of injury
In most of the case reports, expectant management was instituted. However, in five case reports, anti-inflammatory medication was used (Kim et al 2018, Lang & Waite 2001, Li et al 2022, Park & Jeong 2022, Tan et al 2010). Dexamethasone was administered at varying doses for 3 days in three of the reports (Kim et al 2018, Li et al 2022, Tan et al 2010). Park and Jeong (2022) used prednisolone for 3 days, gradually reducing the dosage by half daily. Lang and Waite (2001) also used oral steroids, but no specific details were provided. Apart from anti-inflammatory medication, Ulusoy et al (2014) and Wang et al (2021) reported the use of other vitamins, such as Vitamin E, B1 and B6 as supplements for their patients. In the Ulusoy et al’s (2014) case presentation, the patient developed anxiety and depression-like symptoms due to social isolation from their diagnosis. Patient care involved prescribing an Selective Serotonin Reuptake Inhibitor (SSRI), which was discontinued after 12 weeks.
Discussion
Our review contributes to the existing body of evidence, highlighting an association between LMA use and lingual nerve neuropraxia. We identify significant risk factors for lingual nerve injury, emphasising female sex, extended operations, head and neck procedures, and difficulty with intubation. However, the data remain inconclusive on whether BMI, MP score and age contribute to neuropraxia.
Evidence suggests a higher risk of lingual nerve injury in females, potentially attributed to smaller jaw sizes and mouth openings (Tojyo et al 2019). Nevertheless, conflicting views on the anatomical location of lingual nerve injury exist (Mendes et al 2014). Difficulty with intubation and prolonged operations predictably increase the risk, with multiple intubation attempts causing repeated trauma and extended operations exerting more pressure on the nerve.
Our review shows that head and neck procedures are also associated with high risk for lingual nerve injury which may be due to increased airway congestion, pressure and potential airway dislodgement. Although BMI and MP scores theoretically affect airway size and intubation difficulty, limited studies warrant further investigation into their role as contributors.
We were limited in the number of studies assessing BMI and MP score as risk factors for lingual nerve injury. Theoretically, BMI and MP scores can indeed influence the airway anatomy, potentially contributing to difficulties during intubation. Larger BMI often correlates with increased adipose tissue around the neck and throat, potentially complicating airway management. Similarly, a higher MP score suggests increased oropharyngeal tissue that could obstruct the airway, making intubation more challenging. While these factors intuitively suggest a potential association with lingual nerve injury due to their impact on airway characteristics, the limited number of studies exploring this relationship does highlight a gap in the current understanding. Future investigations that delve deeper into these factors could provide valuable insights into their direct impact on lingual nerve injury during airway management
One of our review limitations is focusing solely on lingual nerve injuries related to airway management. Dental procedures and inferior alveolar blocks are indeed well recognised as common causes of lingual nerve injury. Procedures, particularly those involving wisdom tooth extraction or other oral surgeries, and inferior alveolar nerve blocks are acknowledged sources of lingual nerve injury. These procedures involve closer proximity to the lingual nerve and thus pose inherent risks. Therefore, a larger scope is necessary to better understand all forms of lingual nerve injury.
Taken together, the size of the LMA/supraglottic airway device should be chosen appropriately, generally based on patient weight. Upsizing the LMA/supraglottic airway device should be considered if cuff volume or pressure exceeds the recommended limit. Use of a cuff inflator with pressure measurement may also mitigate over-inflation. For intubation, appropriate patient positioning, attention to laryngoscopy technique and low threshold to switch to alternative airway adjuncts may avoid unnecessary pressure exerted on the soft tissue by the laryngoscopist.
In summary, it is important to note that lingual nerve injury can occur as a postoperative complication of airway management. To ensure that patients are fully informed about the risks associated with airway management, it is crucial to include lingual nerve neuropraxia as a potential complication that may arise. Anaesthetists play a vital role in communicating these risks and providing reassurance in case of complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.