
Abstract
The value of biomarkers, such as acetylcholinesterase and butyrylcholinesterase, for guiding perioperative patients suffering from postoperative delirium and/or (possibly related) postoperative cognitive dysfunction is unclear. Only recently have different biomarkers are being explored to assess postoperative delirium’s occurrence and/or course. The aim of this work is to investigate whether acetylcholinesterase and butyrylcholinesterase can help detect increased risks of the development and course of postoperative delirium in urological patients undergoing surgery. In total, 45 urology patients were screened. During five perioperative time points (meaning preoperative and postoperative), acetylcholinesterase or butyrylcholinesterase concentrations from serum were correlated with three perioperative postoperative delirium and two perioperative postoperative cognitive dysfunction investigations. Results showed neither a significant decline of either acetylcholinesterase or butyrylcholinesterase concentration before and after surgery, nor a significant correlation with postoperative delirium. Furthermore, significant postoperative cognitive dysfunction could not be detected in this perioperative urological collective.
Keywords
Introduction
Postoperative delirium (POD) is a socio-economic burden that occurs in all surgical disciplines, including urology, with increased morbidity, mortality, poor economic consequences and a an increased need for medical care (Leslie et al 2005, Leslie & Inouye 2011, Monk et al 2008, Steinmetz et al 2009). Higher cognitive functions such as memory, vigilance and goal-oriented problem-solving are often impaired in patients with POD, but are sometimes difficult to detect due to overwhelming problems such as attention deficits, disorientation and motor restlessness (in hyperactive/mixed type). Patients with postoperative cognitive dysfunction (POCD) present with memory deficits and long-lasting learning difficulties, usually in the absence of acute attention deficits (the cardinal symptom of POD). Although both share much similarity, there is an ongoing debate on whether POD and POCD are different phenotypes of the same disease (Deiner & Silverstein 2009) or whether they are completely different entities (Daiello et al 2019). While POD is relatively easy to be diagnosed using standardised procedures, such as the confusion assessment method (CAM) (Robinson & Eiseman 2008), POCD requires extended neuropsychological testing (Liu et al 2021). Besides very limited options of treatment for both diseases (Duning et al 2021, Pappa et al 2017, Zangl et al 2022), they are often underdiagnosed due to multiple factors (Iamaroon et al 2020).
Deficiencies in the cholinergic neurotransmission seem to be a likely source of the development of POD (Daiello et al 2019). Based on this assumption, various working groups have explored plasmatic esterase (acetylcholinesterase (AChE) and butyrylcholinesterase (BChE)) as bedside diagnostic tools for POD risk confirmation in a wide variety of surgical fields (Cerejeira et al 2011, John et al 2017, Plaschke et al 2017, Saldanha 2017). In this work, we investigated the feasibility of AChE and BChE concentrations in capillary serum for the diagnosis or predictor of POD after urological surgery. Furthermore, we analysed possible cross-associations between POD, POCD and serum cholinesterase. Consequently, it is an ongoing matter of debate whether serum biomarkers for the detection of POD (and POCD) are feasible for this purpose at all (Adam et al 2020, John et al 2017, Plaschke et al 2017, Stoicea et al 2014).
There is slight evidence for the consistency between POD and both cholinesterases in serum and cerebrospinal fluid (CSF) (Lin et al 2020). We assumed that the AChE/BChE concentrations in the CSF and serum are the same (Plaschke et al 2007). Furthermore, their concentrations just might predispose individuals at risk of the development of both diseases, either directly by altering the metabolism of relevant neurotransmitters (AChE) or indirectly by altering the metabolism of suspicious drugs, enabling the development of POD and POCD preoperatively (White et al 2005).
Therefore, this prospective observational study investigates the importance of cholinesterase activity in serum in urological patients in the perioperative phase with regard to the occurrence of POD and POCD for the first time.
Materials and methods
This investigation is a substudy of the CESARO project (Müller et al 2019). Here, we analyse only the urological patient population, which was operated in Munich (Ludwig-Maximilians-University Munich, Munich, Germany). The ethical commission signed the investigation afore (Ludwig-Maximilians-University Munich ethical board ref.: 558–13).
In total, 60 urologic patients were screened, of whom 45 (39 males and six females) finally participated. Nineteen patients (43.2%) suffered from prostate carcinoma, 18 (38.6%) from kidney tumours and two (4.5%) from renal pelvic disease. Inclusion criteria were the following: age at least 18 years, admission to post-anaesthesia care unit (PACU) or intensive care unit (ICU) after elective general anaesthesia, and scheduled inpatient treatment for at least 24 hours.
Patients with a known pseudocholinesterase deficiency, acute psychiatric disorder with pharmacologic treatment, inability to understand German language, analphabetism and visual or hearing impairments were excluded from the study. Further exclusion criteria were lack of written informed consent, participation ability, accommodation in an institution on judicial or official order, emergency interventions and ambulant patients, lacking willingness to save and hand out data within the study. Patients were also excluded if they were an employee of one of the study centres or were included in an adjuvant therapy study at some point during CESARO (Müller et al 2019), or participated in a different clinical study (Figure 1).
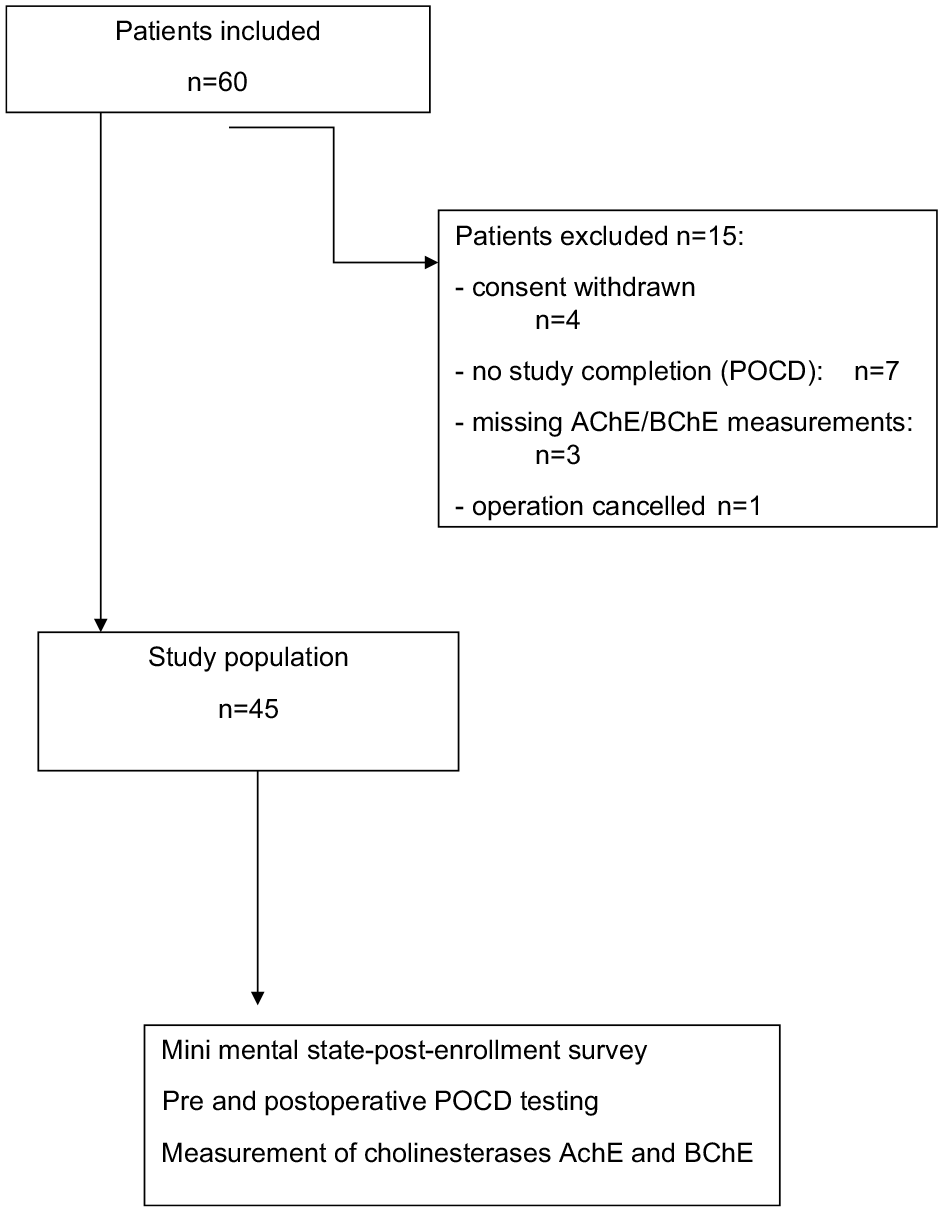
Flow diagram patient acquisition
The measurement of peripheral cholinesterase activity was performed as point-of-care testing using 10μL of capillary blood and a validated photometric test (ChE Check Mobile; Securetec Detektions-Systeme AG, Neubiberg, Germany). According to the instructions from the manufacturer, measurements were performed at five time points for each patient: at least one day prior to operation, shortly before anaesthesia induction, on admission to recovery room or PACU, on discharge from recovery room or PACU, one day after surgery and three days after surgery (see Figure 2).
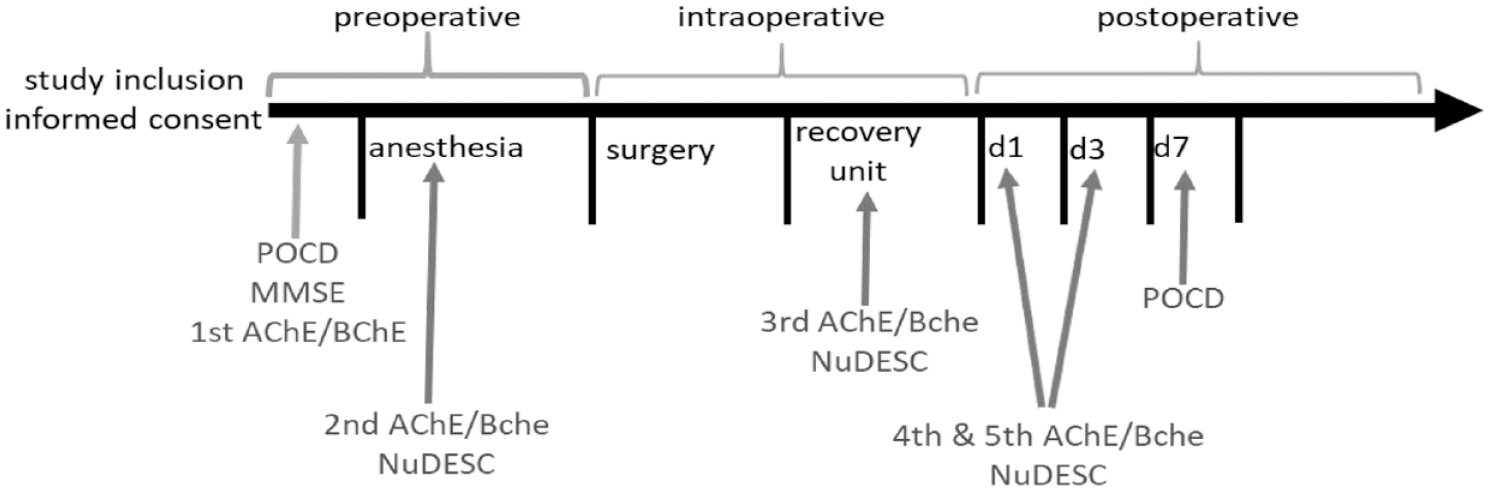
Pre, Intra and postoperative measuring points of postoperative cognitive dysfunction (POCD), Mini-Mental State Examination (MMSE), acetylcholinesterase (AChE), butyrylcholinesterase (BChE) and Nursing Delirium Scale (Nu-DESC) at days 1, 3 and 7: first, second and seventh postoperative day
According to the manufacturer’s specifications, the reference range for AChE was 26.7-50.9U/gHb and for BChE was 2300-7000U/L. To deal with missing values, we included three defined measurements (time points) into the analysis. An overview of the included measurements is listed below (Figure 2). Both AChE and BChE activities were quantified at the abovementioned five time points.
For detection of POD, Nursing Delirium Scale (Nu-DESC), as a highly validated diagnostic tool (Hargrave et al 2017), was done one day before the operation (baseline measurement), on the operation day before the induction of anaesthesia, in the recovery unit before discharge, and on the first and third postoperative days (Figure 2). Nu-DESC assesses five dimensions: orientation, behaviour, communication, illusion/hallucination and psychomotor retardation. The symptoms are rated on a 3-point scale, where a score of 2 or more cumulative points indicates delirium.
The neurocognitive testing battery for POCD confirmation consisted of the following:
(a) Verbal Learning Test (California VLBT): It is an instrument measuring episodic verbal learning and memory, and demonstrates sensitivity to a range of clinical conditions. In this study, patients performed four rounds of the test in the baseline survey and four rounds on the seventh postoperative day. According to international standards, every correctly remembered word was counted as 1 point (Kramer et al 2020).
(b) Stroop Colour Word Test (SCWT): It is a method for measuring the individual interference tendency in colour-word interference. If the content of the word matches the colour, the colour can be named more quickly; the other way round, it is naturally more difficult. The widely accepted limit for the SCWT is 40 correctly recognised items. Scores of 40 or less were scored as impairment of cognition, especially the decline in the perioperative course. Patients performed three rounds of the test in the baseline survey and three rounds on the seventh postoperative day (Scarpina & Tagini 2017).
(c) Concept Shifting Test (CST): This test measures attention, working memory performance and mental flexibility. It consists of five trials: during the first one, participants (CST digit) consecutively cancel out numbered circles. This is the individual’s reference time for psychomotor speed and attention. During the second test (CST letter), participants are asked to cancel out consecutively lettered circles. In the third trial (CST shift), participants are asked to cancel out numbered and lettered circles by alternating between the two sequences. The third trial serves as a measure for cognitive flexibility. In the last trial, participants are asked to cancel out consecutively empty circles. The average time in seconds to complete these two trials serves as an index of speed (Rundshagen et al 2014, Van der Elst et al 2006).
Those neuropsychological tests were chosen to offer the basic coverage of cognitive domains with just a short overlap and a short duration to perform (Liu et al 2021). POCD testing took place on the day before operation and on the seventh postoperative day. In addition, Mini-Mental State Examination (MMSE) was conducted to confirm and/or exclude already existing deficits before the operation (Liu et al 2021) (see Figure 2).
Statistical analysis
Statistical analysis was performed with SPSS 15.0 (IBM Statistics). After confirmation of normal distribution (with the Shapiro–Wilk test’s p-value >0.05), continuous data were displayed as mean and standard deviation (±SD). Correlation analysis was performed with Eta for nonlinear and Pearson’s r for linear association. Without normal distribution (with the Shapiro–Wilk test’s p-value <0.05), data were presented as median, and 25% and 75% quartile and further analysed with the Wilcoxon test. Descriptive statistics described frequencies and percentages for additional clinical and demographic parameters, including age, body mass index (BMI), duration of surgery, blood loss, length of hospital stay, complications and ‘physical status classification system’ (American Society of Anesthesiologists (ASA)). Correlations between AChE/BChE with POD and/or POCD were made with repeated-measures pairwise tests (analysis of variance (ANOVA)) (Burgess et al 2003). Eta correlation coefficient served as indicator for nonlinear associations. For further specifications, multivariate testing (with Pillai’s trace, Wilks’ lambda, Hotelling’s trace and Roy’s largest root) gained more detailed insights (Ateş et al 2019).
Results
Baseline parameters
The mean age of patients was 65.5 (±9.8) years. In all, 62.2% (n = 28) were scored 2 in the ASA classification system and 37.8% were scored 3 (n = 17). Patients had an average BMI of 27 (±3.9) kg/m2. The average duration of surgery was 138.6 (±79.6) minutes with a mean blood loss of 400 (±294) mL. The mean length of hospital stay was 10.5 (±4.3) days. The median MMSE value was 29 (min. 22; max. 30) (see Table 1).
Baseline parameters
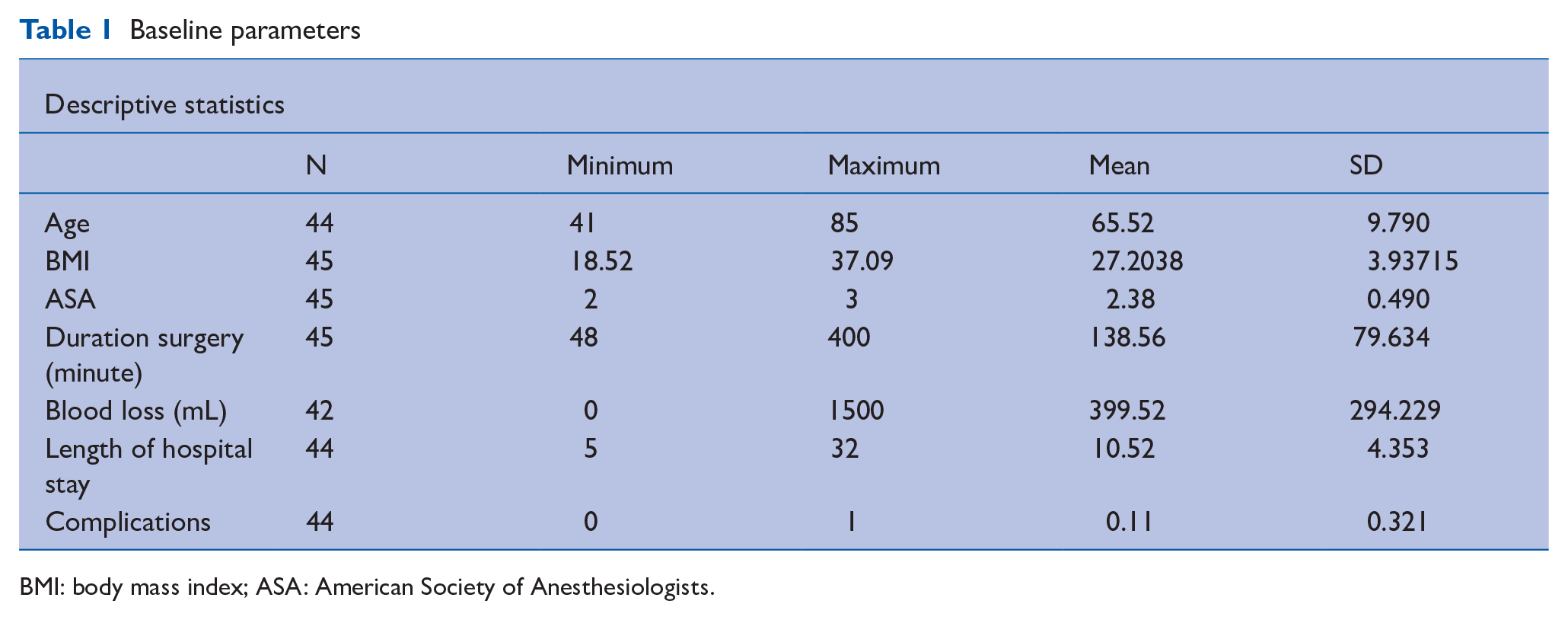
BMI: body mass index; ASA: American Society of Anesthesiologists.
Incidence of POD
Seven patients (15.6%) suffered from delirium in the postoperative period, whereas 38 (84.4%) did not.
Perioperative course of neurocognitive (POCD) testing
Thirty-two patients had a worse performance in postoperative VLBTs, and only two were better postoperatively (four were equal). Patients got significantly worse in the VLBT in the perioperative course (z-value = −4.4; p = 0.000).
Post and preoperative differences in SCWT were almost equal: 20 patients performed worse and 22 better (one tie) postoperatively. In consequence, there was no statistical difference (z-value = −0.013; p = 0.99).
Comparable results were found with CST: post and preoperative differences were negative in 17 patients and positive in 22 patients (without tie). In consequence, there was no statistical difference (z-value = −0.998; p = 0.318) (see Table 2).
Results of neurocognitive testing
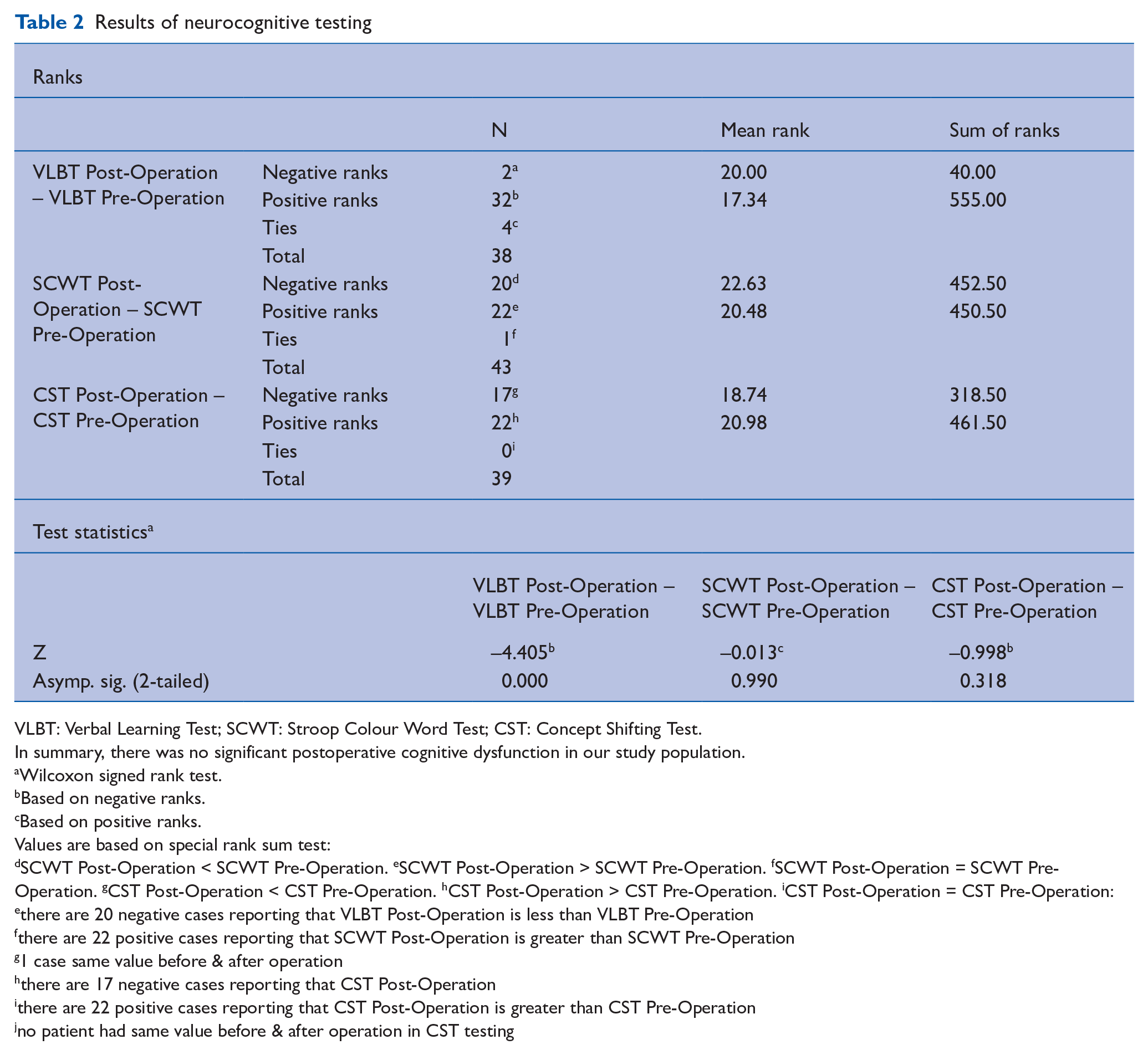
VLBT: Verbal Learning Test; SCWT: Stroop Colour Word Test; CST: Concept Shifting Test.
In summary, there was no significant postoperative cognitive dysfunction in our study population.
Wilcoxon signed rank test.
Based on negative ranks.
Based on positive ranks.
Values are based on special rank sum test: dSCWT Post-Operation < SCWT Pre-Operation. eSCWT Post-Operation > SCWT Pre-Operation. fSCWT Post-Operation = SCWT Pre-Operation. gCST Post-Operation < CST Pre-Operation. hCST Post-Operation > CST Pre-Operation. iCST Post-Operation = CST Pre-Operation: ethere are 20 negative cases reporting that VLBT Post-Operation is less than VLBT Pre-Operation fthere are 22 positive cases reporting that SCWT Post-Operation is greater than SCWT Pre-Operation g1 case same value before & after operation hthere are 17 negative cases reporting that CST Post-Operation ithere are 22 positive cases reporting that CST Post-Operation is greater than CST Pre-Operation jno patient had same value before & after operation in CST testing
Perioperative course of AChE/BChE concentrations
The difference between AChE before (mean 84.9 ± 12.1) and after operation (120.8 ± 14.6) is significant (n = 45; p = 0.000). BChE before (1533.5 ± 228.6) and after operation (1822.4 ± 271.7) is less, but still significantly different (n = 45; p = 0.004) (see Table 3).
Paired-samples test preoperative and postoperative cholinesterases
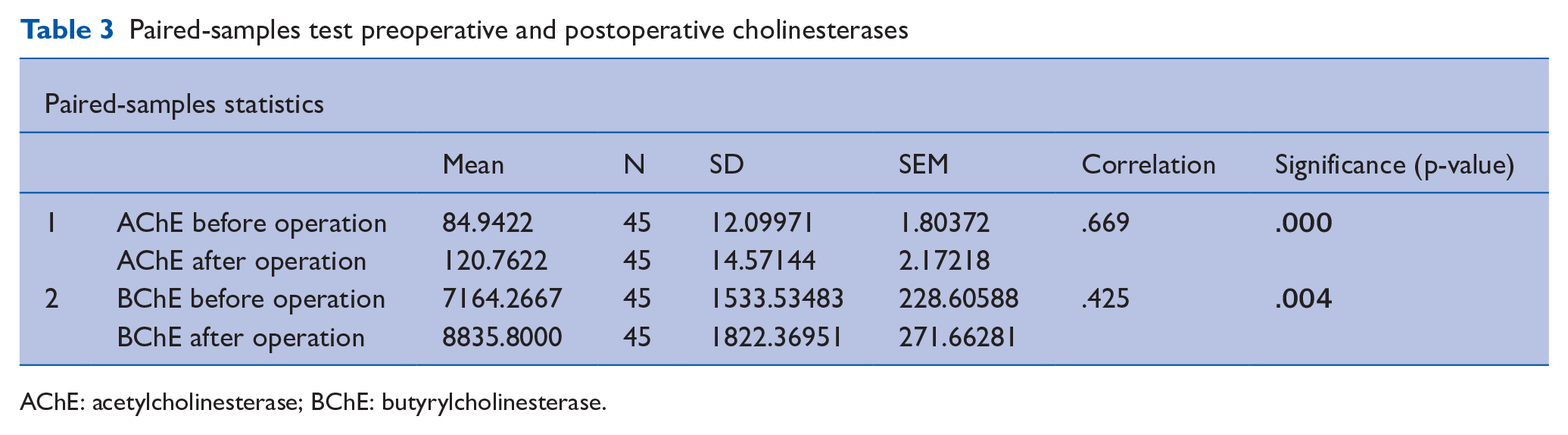
AChE: acetylcholinesterase; BChE: butyrylcholinesterase.
AChE/BChE concentrations and POD
Total (meaning preoperative and postoperative values taken together) AChE concentrations were not significantly associated with the occurrence of POD (Pearson coefficient = –0.013; p = 0.93; n = 45), as well as total BChE concentrations (Pearson coefficient = 0.012; p = 0.94; n = 45).
Furthermore, the analysis of individual AChE/BChE time point concentrations (each five preoperative and postoperative time points) did not show significant association with POD: based on results from Eta correlation, we observed no significant correlation, and the strengths of correlation along the significant values were >0.05 (see Table 4).
Upper half: Eta correlation of five individual preoperative and postoperative cholinesterases and their association with delirium
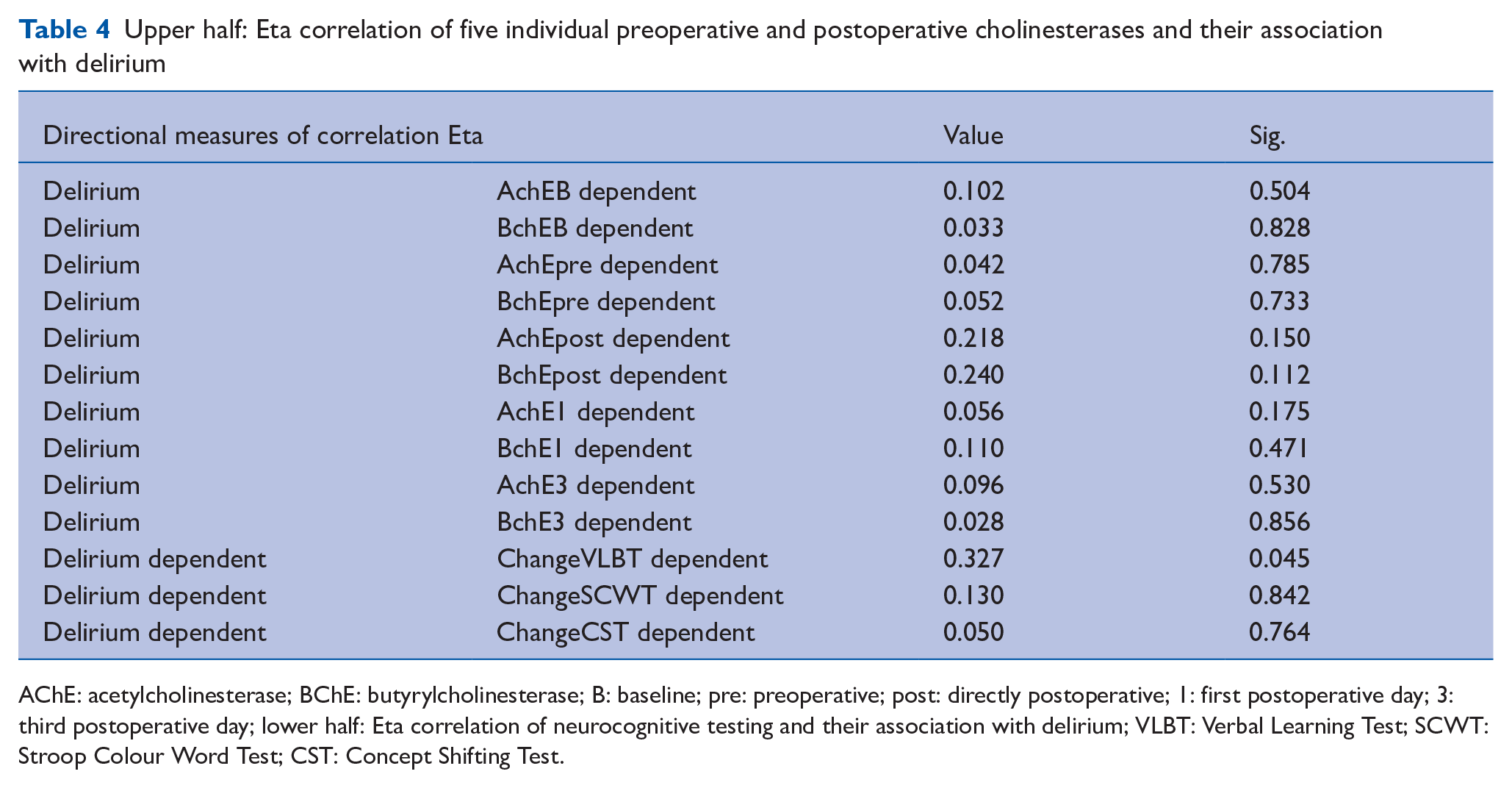
AChE: acetylcholinesterase; BChE: butyrylcholinesterase; B: baseline; pre: preoperative; post: directly postoperative; 1: first postoperative day; 3: third postoperative day; lower half: Eta correlation of neurocognitive testing and their association with delirium; VLBT: Verbal Learning Test; SCWT: Stroop Colour Word Test; CST: Concept Shifting Test.
Correlation between POD and POCD
Based on the results from the Eta correlation, only VLBT changes have weak (but significant) correlation with POD (p < 0.05). However, there is no significant correlation between SCWT/CST values and POD (see Table 4).
Discussion
Cholinesterases (AChE/BChE) play a crucial role in the fine adjustment of excitatory neurotransmitter acetylcholine, which is necessary for higher central nervous functions, such as attention, awareness, orientation and goal-oriented thinking (Müller et al 2019, Plaschke et al 2007, Saldanha 2017). Disturbances of this fine balance may occur during operations due to different factors, such as anaesthetic medications, (ie, benzodiazepines), direct anticholinergic drugs (ie, atropine) and the surgical stress response (which is centrally regulated in the hypothalamus). The cholinesterase, as a regulator of acetylcholine concentrations, may therefore play a crucial role in the development of postoperative cognitive peculiarities, such as POD and POCD. In this study, we investigated serum cholinesterase concentrations (AChE/BChE) for the correlation with either POD or POCD as bedside measurement in a urological collective for the first time.
This investigation included 45 patients undergoing urological operations. Comparable to other working groups dealing with urological patients (Gani et al 2013, Leotsakos et al 2019), seven patients (15.6%) suffered from POD. It is well known that in other surgical specialties, particularly those with more serious systemic diseases, such as cardiac surgery (Iamaroon et al 2020, John et al 2017) and surgeries in patients with severe vascular disease (Brzezinski-Sinai 2021), the incidence of POD is much higher.
Both AChE and BChE concentrations increased significantly in our urological collective postoperatively. Most publications that analyse the occurrence of POD indicate a decrease in cholinesterase after surgery (Cerejeira et al 2011, John et al 2017) in which either lower or comparable cholinesterase concentrations were associated with POD. The absence of significant POD diseases and the postoperatively increased cholinesterase concentrations speaks for a causal imbalance of acetylcholine in the central nervous system, but is of course not proof. This finding may be due to the rather low invasiveness (laparoscopy, transurethral surgery) of urological interventions, as demonstrated by short surgery durations, low blood loss and short hospital stay. It appears that the invasiveness of surgical interventions is associated with a postoperative increase in cholinesterase (John et al 2017, Lin et al 2020, Plaschke et al 2017). This phenomenon can possibly be attributed to a more extensive regeneration phase, which is regulated by the parasympathetic nervous system and consequently higher cholinesterase activities to break down the vegetative transmitter acetylcholine (Fitzgerald et al 2021).
Our testing battery for POCD confirmation showed only significant worse results in VLBT, not in SCWT and CST, meaning that there was no evidence for significant POCD occurrence in comparison with other study groups (Rundshagen 2014). In consequence, due to the absence of POCD, it could not be further compared with both POD and AChE/BChE concentrations.
Limitations
A limitation of the present work is the fact that a rather small collective of only 45 patients could be examined. It must be noted that the work is a sub-collective of the ‘CESARO’ work (Müller et al 2019) and unfortunately could not be achieved with the available means and possibilities.
It should also be noted that the evidence for a clear correlation between serum and cerebrospinal fluid cholinesterase is rather low, but was the best possible method for this purpose (Lin et al 2020, Plaschke et al 2007).
Conclusion
This work is the first attempt to find relationships between cholinesterase concentrations, POD and POCD in a urological and postoperative patient population. Further work will be needed in the future to show whether cholinesterase is suitable as a risk marker and therapy companion for patients with impaired postoperative cognitive performance.
Footnotes
Availability of data and materials
The data set that was created during the study is publicly available on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Contributorship
VvD conceptualised the study, designed the study and supervised the data collection. QZ wrote the manuscript and analysed the data. BS did the laboratory analysis and field work. SD critically reviewed the manuscript and developed the final version. VvD and BS were involved in the development of the study protocol. All authors commented on the manuscript and approved the final version.
Data sharing
Data available on request.