
Abstract
Background:
Over the last two decades, many elective procedures have transitioned to day-case surgery thanks to the introduction of ‘enhanced recovery’ protocols. Only recently has total hip arthroplasty been considered a candidate for day-case surgery, as it was once associated with significant pain, mobility impairment and prolonged postoperative recovery. The National Orthopaedic Hospital Cappagh became the first public hospital in Ireland to set up a day-case total hip arthroplasty service in June 2018, and since then has performed over 109 such cases.
Aims:
We outline our day-case total hip arthroplasty pathway, with specific focus on anaesthetic considerations. We report rates of failed discharge and readmission
Results:
We achieved successful same-day discharge in 90.8% of our first 109 cases. Readmission rate was 4.6%.
Conclusion:
Our experience of implementing a day-case total hip arthroplasty pathway was highly positive and congruent with expectations from the literature. With appropriate patient selection and education, day-case total hip arthroplasty is not just safe, but of benefit to both patients and healthcare systems.
Keywords
Introduction
Elective total hip arthroplasty (THA) is considered one of the most successful elective operations, combining low complication rates with excellent functional outcomes. The last two decades have seen a dramatic reduction in length of stay for nearly all elective operations, THA included, due to the introduction of ‘enhanced recovery after surgery’ programmes. Many elective operations have further transitioned to the day-case setting. Until recently, THA was not considered a candidate for day-case surgery due to the considerable pain, mobility impairment, potential medical comorbidities and complications often associated with a procedure of its magnitude. However, many international centres have shown that in well-selected patients, with a thorough multimodal recovery protocol, day-case THA can be performed safely and effectively, benefiting both patients and healthcare systems. Having performed Ireland’s first THA in 1969, the National Orthopaedic Hospital Cappagh (NOHC) became the first public hospital in Ireland to set up a day-case THA service in June 2018, and since then has performed more than 100 such cases.
We report our experience in implementing this pathway based on data drawn from our first consecutive 109 cases, highlighting key anaesthetic considerations and reasons for unsuccessful same-day discharge.
Methods
The NOHC performed Ireland’s first THA in 1969, for which the patient was admitted ten days in advance to undergo a period of isolation for infection precaution measures. Since then, the orthopaedic service has developed enormously, performing approximately 1600 arthroplasties per year, with a mean length of stay of 3.23 days for primary unilateral THA. In June 2018, the NOHC became the first public hospital on the island of Ireland to perform day-case THA, and at time of writing has now performed over 109 such cases.
We prospectively followed our first 109 consecutive day-case THAs, performed by a single surgeon at NOHC from June 2018 to February 2022. The study was approved by the local research and ethics committee (NOHC/2020/ETH/SH-CEO-282). All patients were enrolled on a comprehensive clinical pathway (Figure 1). Data collected included patient age, sex, American Society of Anesthesiology (ASA) score, same-day discharge status, surgical approach, operative time, estimated blood loss, surgical components used, postoperative complications and readmission status.
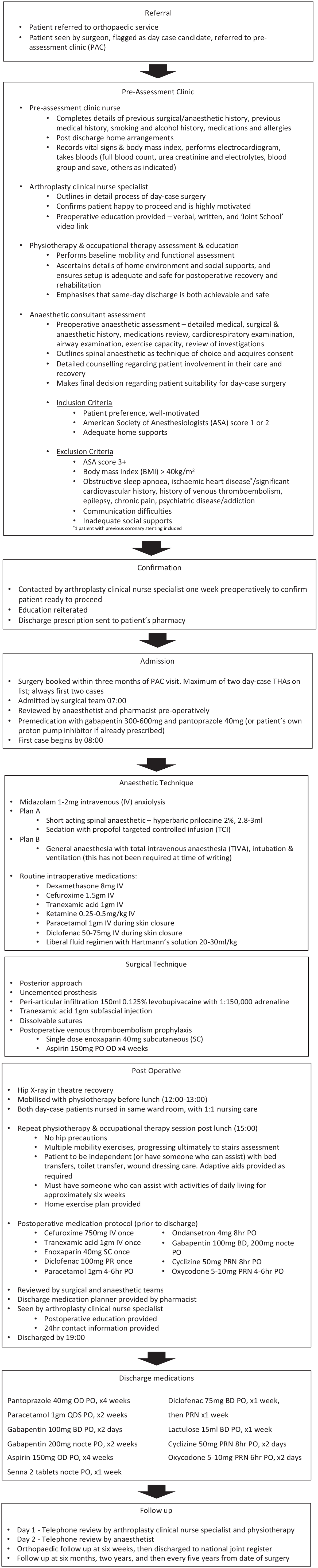
Summary of total hip arthroplasty clinical pathway
Results
Of the first 109 patients, 68 (62%) were male and 41 (38%) female. Mean age was 53 (±9.4); 46 (43%) were ASA score 1, 63 (57%) ASA score 2. Median operating time was 44 minutes and median estimated blood loss was 245ml (Table 1).
Patient and surgical characteristics from first 109 day-case total hip arthroplasties. Continuous variables are expressed as mean (SD) or median (IQR[range]). ASA, American Society of Anesthesiology; EBL, estimated blood loss
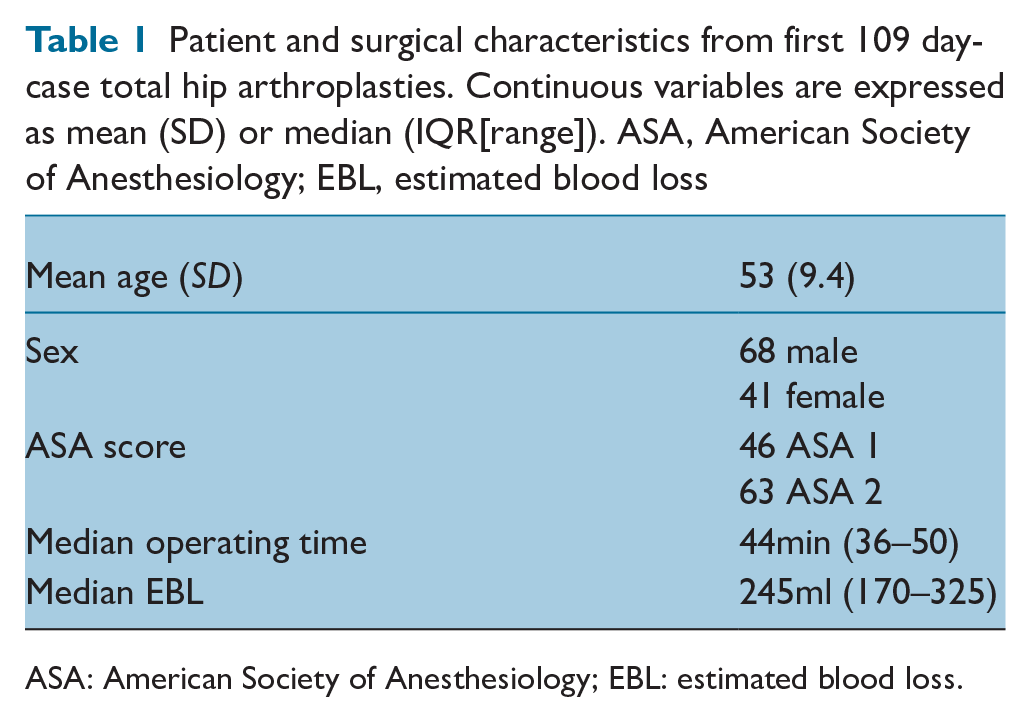
ASA: American Society of Anesthesiology; EBL: estimated blood loss.
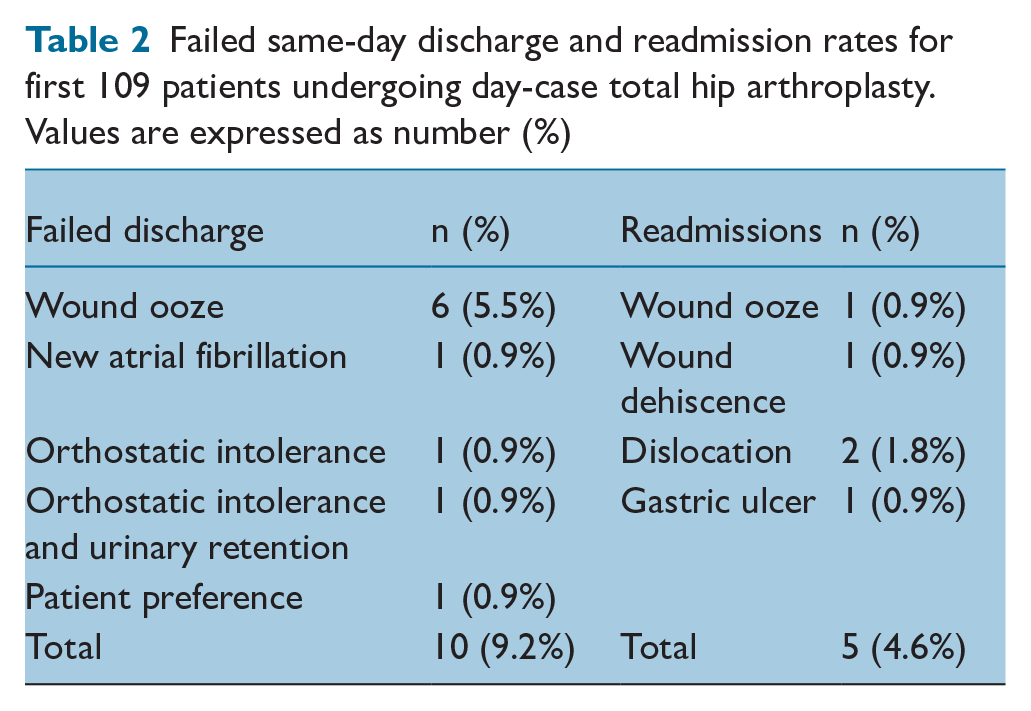
Successful same-day discharge was achieved in 90.8% of cases. The most common reason for failed discharge was wound ooze (60%). Readmission rate from date of first case to time of writing was 4.6% (Table 2).
Failed same-day discharge and readmission rates for first 109 patients undergoing day-case total hip arthroplasty. Values are expressed as number (%)
Discussion
The goal of successful same-day discharge following THA necessitates optimum patient selection and anaesthetic/surgical technique, alongside successful prevention and control of the undesirable postoperative pathophysiological responses such as pain, nausea, fatigue, weakness, orthostatic intolerance and cognitive dysfunction (Wainwright et al 2021). The same principles that underpin established enhanced recovery protocols are utilised to equal effect in day-case surgery, namely multimodal analgesia, early postoperative mobilisation and preoperative patient education with an emphasis on positive expectation for early discharge (Maempel et al 2016).
Patient selection and education
Younger patients (under 70 years) who have few or zero medical comorbidities, and are highly motivated to rehabilitate, are first identified as candidates for day-case surgery during consultation with the orthopaedic surgeon. Patients are then assessed at the preoperative assessment clinic (PAC) and deemed as either eligible or ineligible following detailed discussion with the consultant anaesthetist. The pre-assessment clinic is nurse-led with dedicated consultant anaesthetic oversight and involves detailed physiotherapy and occupational therapy assessments.
Although several authors (Meneghini et al 2017, Sher et al 2017) have developed risk screening tools in this context, there is no current agreed consensus on patient eligibility criteria. Major comorbidities noted in the literature to increase the risk of postoperative complications include age > 80 years, cardiovascular disease, pulmonary disease, uncontrolled diabetes, coagulopathy, body mass index (BMI) > 40, chronic steroid use and albumin deficiency/malnutrition (Sher et al 2017, Thompson et al 2021). Based on extensive experience in joint arthroplasty, the pre-assessment service considers the following criteria acceptable for patient eligibility: patient preference for same-day discharge; age < 70 years; ASA score 1 or 2; BMI < 40; adequate home supports; residing within a one-hour drive of the hospital; and no barriers to communication. Exclusion criteria include obstructive sleep apnoea; congestive heart failure; arrhythmia; history of venous thromboembolism; significant psychiatric disease including addiction; chronic pain or long-term opioid consumption; chronic steroid use; and poor social supports.
Preoperative patient education is of paramount importance in allaying patient apprehension, as well as achieving realistic patient expectations. We use a multidisciplinary approach to patient education, with input from the consultant surgeon and anaesthetist, arthroplasty clinical nurse specialist, physiotherapy, occupational therapy and pharmacist. A key member of the team is the arthroplasty clinical nurse specialist, who coordinates and guides the patient on their journey from referral to discharge. Every member of the team emphasises the importance of a positive mindset and ensures the patient is physically and psychologically prepared for an active role in their recovery.
Anaesthetic technique
The goal of successful ambulatory surgery places significant demand on anaesthetic technique. Key priorities include rapid onset/offset of anaesthesia, rapid recovery of strength, reflexes, mobility and micturition and a balance of adequate analgesia with minimal nausea, vomiting or sedation. In the setting of THA, neuraxial anaesthesia is considered the anaesthetic technique of choice (Memtsoudis et al 2019); however, historically this has not been considered a good option for ambulatory surgery due to concerns regarding residual motor blockade and urinary retention. Conversely, neuraxial anaesthesia obviates the need for intraoperative opioids (which reduces postoperative nausea and vomiting), has minimal impact on pulmonary physiology and allows a faster return to oral intake. We use hyperbaric prilocaine 2% which exhibits many ideal properties, namely a rapid onset and offset, low incidence of transient neurological symptoms, rapid return of bladder function and a block suitable for operations up to 90 minutes without the need for adjuvants (Boublik et al 2016, Rattenberry et al 2019).
Surgical considerations
A posterior surgical approach (non-piriformis tendon sparing) is used with emphasis on minimising both surgical duration and blood loss. An uncemented prosthesis is used as standard; however, cement may be used if bone quality is poor. The implant system used was either Accolade® II/Trident® (Stryker Corporation, Kalamazoo, MI, USA) or ACTIS™/PINNACLE® (DePuy Synthes, Warsaw, IN, USA). A periarticular injection of 150ml 0.125% levobupivacaine with 1:150,000 adrenaline is given prior to closure with dissolvable sutures (therefore, patient does not need to return for skin clip removal). Following a high early incidence of postoperative wound ooze, a subfascial injection of tranexamic acid 1gm was introduced in addition to the 1gm given intravenously.
Immediate rehabilitation
Early postoperative rehabilitation begins as soon as the patient is alert, clinically stable and has full return of motor function. However, it is only achievable when pain, nausea, sedation and orthostatic intolerance are controlled. To address these issues, we aim to minimise blood loss through excellent surgical technique and use of tranexamic acid, employ a liberal fluid strategy, use preemptive anti-emetics and – arguable most importantly – use a multimodal analgesic regimen.
Uncontrolled pain is one of the main barriers to discharge from hospital, and the importance of an adequate multimodal analgesia regimen cannot be overstated. We use preemptive analgesia, beginning with a preoperative dose of gabapentin on admission to the day ward. Intraoperatively, all patients receive 8mg intravenous (IV) dexamethasone; 0.25–0.5mg/kg IV ketamine; and 1gm IV paracetamol and 50–75mg IV diclofenac during closure, provided there are no contraindications. Postoperatively, the patient receives a standardised prescription of regular oral paracetamol, regular gabapentin, a single dose of rectal diclofenac followed by a regular non-steroidal anti-inflammatory drug (NSAID), and as-required oxycodone. The patient leaves with a standardised discharge prescription that has been provided and dispensed in advance. None of the day-case THA patients thus far have failed discharge due to unmanageable pain.
Safety
As this is an observational study, it is not possible to draw conclusions regarding the safety of day-case THA. In our first 109 cases, we achieved successful same-day discharge in 90.8% and a readmission rate of 4.6%. As Goyal et al (2017) note, successful discharge rate varies considerably between studies, ranging from 36% to 100%. Most studies report a success rate of 75%, with orthostatic intolerance being the main reason for impaired early discharge in the remaining 25%. Of the ten unsuccessful discharges in this study, six were due to wound ooze, two due to orthostatic intolerance, one due to new-onset atrial fibrillation and one due to patient preference.
Multiple studies have attempted to compare complication and readmission rates between outpatient and inpatient THA; however, it is important to remember that many of these suffer from selection bias. The selection criteria for day-case THA necessitates that patients are younger, fitter, less obese, have fewer comorbidities and are highly motivated to partake in early rehabilitation. Similarly in our day-case cohort, the mean age was 53 and 42% were ASA 1, with the remainder ASA 2. Randomised controlled trials (Goyal et al 2017) and propensity-matched studies (Gromov et al 2019, Rosinsky et al 2020) which aim to eliminate this bias have not shown an increase in complication or readmission rates in the day-case setting. Rosinsky et al (2020) retrospectively compared 91 patients who underwent day-case THA with a propensity-matched inpatient THA group during the same time period and found improved patient-reported outcomes at two years, and no differences between the groups regarding complications, emergency department visits or readmissions. Other cohort studies have shown significantly lower 90-day complication rates in day-case THAs versus inpatient counterparts (Thompson et al 2021). In one such study, Gromov et al (2019) reported 6% 90-day readmission rate in the outpatient cohort versus 4% in the inpatient cohort. The authors conclude that the risk of serious complications in the early postoperative period is very low in patients who could be deemed eligible for day-case surgery. A recent meta-analysis by Bordoni et al (2020) comprising eight studies and 66,971 THA patients (one RCT and seven comparative studies) found the baseline rate of complications (4.7%) and readmissions (2.9%) was not increased in those who underwent same-day discharge. Due to the small number of studies included, and with low-level comparative trials affected by selection bias, the quality of evidence is ‘very low.’ Apart from complication and readmission rates, the optimal surgical technique and patient selection strategy have yet to be elucidated in the literature.
From our experience, the safety profile compares favourably with data from the National Orthopaedic Register and international literature. Although there was an initial high incidence of postoperative wound ooze (accounting for 60% of failed discharges), this incidence dropped markedly following the introduction of an additional dose of subfascial tranexamic acid. There were two episodes of postoperative THA dislocation, both occurring at day 14. At time of writing, we have zero incidence of venous thromboembolism.
Cost
In 2021, the mean length of stay for inpatient primary unilateral THA was 3.23 days. While both day-case and inpatient THA incur the same cost on the day of surgery, each postoperative day spent in hospital costs a further €1,100. Therefore, for each THA that went home on the day of surgery, approximately €2,200 was saved. In 2021, there were 46 successful same-day discharge THAs, amounting to savings of €101,200 for that year.
Conclusion
The benefits of day-case THA are numerous and include enhanced patient satisfaction due to being able to recover in their own home, improved sleep and return to normal diet and improved engagement in rehabilitation exercises. We also hypothesise that there is a decreased use of postoperative opioids due to an enhanced patient self-perception of being fit, healthy and motivated to rehabilitate, which can become lost in the inpatient setting. Finally, though not the primary incentive, it is estimated that each day-case THA saves the healthcare system €2,200 compared with an average inpatient stay. Areas of further interest include comparison with an inpatient control group and elucidation of optimal patient selection criteria.
In summary, our experience of implementing a day-case THA pathway at NOHC has been highly positive and congruent with expectations based on the literature. With appropriate patient selection and education, day-case THA is both safe and beneficial to patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.