
Abstract
Purpose:
To identify all published data on the chemical, micro-organism and malignant cell contents of ultrasonic scalpel plume, if any, and on any clinical implications of the contents on patients and operating staff.
Methods:
Searches were conducted aiming to identify all published evidence on the chemical constituents, presence/absence of viable micro-organisms and malignant cells in ultrasonic scalpel plume. Attempts were made to source unpublished industry data.
Results:
There is evidence from human and in vitro studies of the presence of a range of harmful, and some human carcinogenic, chemicals within ultrasonic plume, mostly at very low concentrations. Any clinical relevance of this has not been studied. There is evidence from experimental studies of the presence of hepatitis virus, human coronavirus and human papillomavirus material within ultrasonic plume. Any clinical effect of this has not been studied. There is conflicting evidence from combined in vitro and mouse model studies of the presence of viable malignant cells within ultrasonic plume. Any clinical relevance of this has also not been studied.
Conclusion:
Overall, relatively little research into the plume has been published, and further study is required to more clearly delineate any potential risk to patients, surgeons and other theatre staff. Current safety recommendations are discussed.
Introduction
The ultrasonic scalpel is a concurrent cutting and haemostasis instrument used widely in surgery, particularly laparoscopic. Originally, it was reported the lack of surgical smoke production negated the need for any intraoperative aspiration or evacuation (Sherman & Davies 2000). However, mounting evidence of the risks of surgical smoke and lack of knowledge of ultrasonic plume has undermined this assumption. Aerosol emanating from an ultrasonic scalpel is technically not smoke as it does not result from burning (Fitzgerald et al 2012), and is variously described as a vapour or plume, although all of these terms are used interchangeably in the literature. ‘Plume’ will be used throughout this article. Currently, several devices are marketed – ultrasonic scalpels, shears, dissectors and scissors. Other specific ultrasonic devices – orthopaedic instruments for removing periprosthetic cement, bone cutting instruments, for example, piezoelectric, and dental ultrasonic instruments have a different mode of action and are not considered here.
Several previous reviews have examined the constituents of ‘surgical smoke’, although most focused on laser and electrocautery devices (Bigony 2007). A systematic review in 2013 did not locate any studies pertaining to ultrasonic devices (Mowbray et al 2013). Pierce et al (2011) produced an extensive systematic review of laser-generated air contaminants. Barrett and Garber (2003) included a review of evidence of the presence of viable cells and infection risk in ultrasonic plume, although a literature search strategy was not given. Fan et al (2009) produced a review of micro-organisms and cells but not specifically the chemical constituents of ultrasonic plume. Another review by Okoshi et al (2014) presented very few findings related to ultrasonic devices. Limchantra et al (2019) presented a narrative summary of some findings related to chemical constituents and viable cells.
A literature review specific to ultrasonic surgical instrument plume has not previously been published. Also, further important studies have been published since the aforementioned studies.
The rationale here is to conduct a literature review of the constituents of ultrasonic surgical instrument plume, gathering all known information (published and unpublished). Three specific parameters will be considered as follows:
Chemical constituents
Presence/absence of micro-organisms
Presence/absence of viable malignant cells.
Ultrasonic surgical devices were developed in the early 1990s and function based on production of ultrasonic waves at a frequency of around 55,500 Hz (Amaral 1994). It cuts by two mechanisms – rapid oscillations causing a reduction in tissue pressure and cellular swelling and lysis, and ‘power cutting’ by vibrations of the instrument blade. Coagulation occurs by protein denaturation via breaking of hydrogen bonds on the proteins by the high-frequency oscillations, and heat generated by friction. These mechanisms are different to electrosurgery and lasers, where more heat is generated.
Plume particle size has been quantified as 350–650nm (Ott et al 1998) and 68.5–994nm (Weld et al 2007), with concentration of 6.10 × 105 and 1.48 × 103 particles/cm3 for small and large particles, respectively (Weld et al 2007). Compared to bipolar, ultrasonics produce a similar concentration of small particles and 1.7 times the concentration of large particles. Monopolar produces smoke 721 times more concentrated than ultrasonics. The bimodal particle size represents small particles from nucleation of vaporised particles and larger ones from explosion and fragmentation of tissue. Plume generation is greater in ‘coagulation’ mode than ‘cut’ mode (Kim et al 2012).
Characteristics of plume spread are complex and multifactorial, in general linked with increasing cutting power (Schneider et al 2009). Velocity of emission increases with frequency and amplitude of blade oscillation. Straight blades generate largely a laminar plume emission of lesser width, whereas curved blades produce a turbulent emission of greater width, larger field and slower dissipation (up to two seconds) (Kim et al 2014). Ott et al (1998) recorded aerosol clearance time of 30–60 seconds for the immediate surgical area without evacuation use, and spread up to 40cm with the hook, 20cm with the ball and 10cm with the blade tips. Plume distribution was concentrated towards the concavity for the hook (with slight back-scatter), circumferentially for the ball and bilaterally for the blade tips. Up to 500,000 blood particles/litre were detected. Particle number varied with tissue type – being 17–23 times greater when cutting fatty versus lean tissue using the ball tip, and 11–20 times greater using the hook tip, a discrepancy also reported elsewhere (Schneider et al 2009).
Materials and methods
Institutional review board approval for this study was not required. Embase and MEDLINE databases were searched from their dates of inception to February 2022, as were the Cochrane Library and the Cochrane Central Register of Controlled Trials (CENTRAL) database. These databases were chosen to provide comprehensive representation of the available literature. The basic and operator search terms for MEDLINE are listed in Figure 1. No hand searching was undertaken. No language or publication date restrictions were applied.
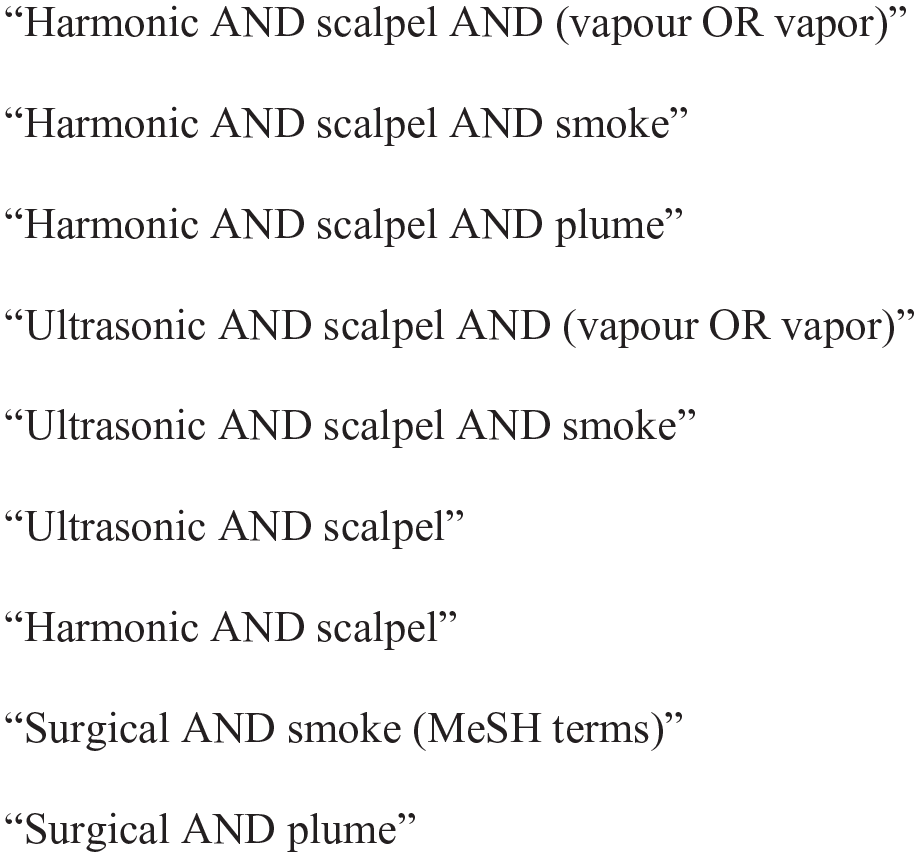
MEDLINE search terms
Two authors (BJS and SA) independently conducted searches. Plans were made for mediation by another author if disagreement, however, none occurred. The abstracts of all papers identified in the initial search were read, and those relevant to the study aims, or with unclear relevance, were read in full text. Many abstracts described ‘surgical smoke’ in their abstract where it was unclear whether ultrasonics had been used – all were read in full text. The references of all papers read in full text were cross-referenced for further studies. The search strategy was purposefully broad to maximise yield. Only plume-producing ultrasonic instruments were included. Those with no plume or non-ultrasonics – for example, laser and electrocautery – were excluded. Studies were accepted from any setting – experimental or clinical, any patient population, any specialty, any pathology either benign or malignant and any study type from case reports to randomised controlled trials, in recognition that much data will come from preclinical, small and in vitro studies.
Attempts were made to access unpublished data from the major manufacturer of ultrasonic scalpel instruments, but these were unsuccessful. The nature of this subject’s literature is such that no quantitative synthesis or meta-analysis was possible, required or attempted.
Results
Eligible studies
In total, 3048 individual studies were located by the initial searches. Once 2035 duplicates were removed, 1013 studies were screened by abstract for inclusion. A total of 943 studies of those were excluded as clearly irrelevant. A total of 70 studies were read in full text, 40 studies excluded for not presenting original data, and 19 studies excluded as not including ultrasonic instruments. Three further studies were excluded as the level of detail on methodology could not confirm meeting inclusion criteria, leaving eight studies finally included. No additional studies were found from reading reference lists. The flow chart of these searches is shown in Figure 2, and study details are shown in Table 1.
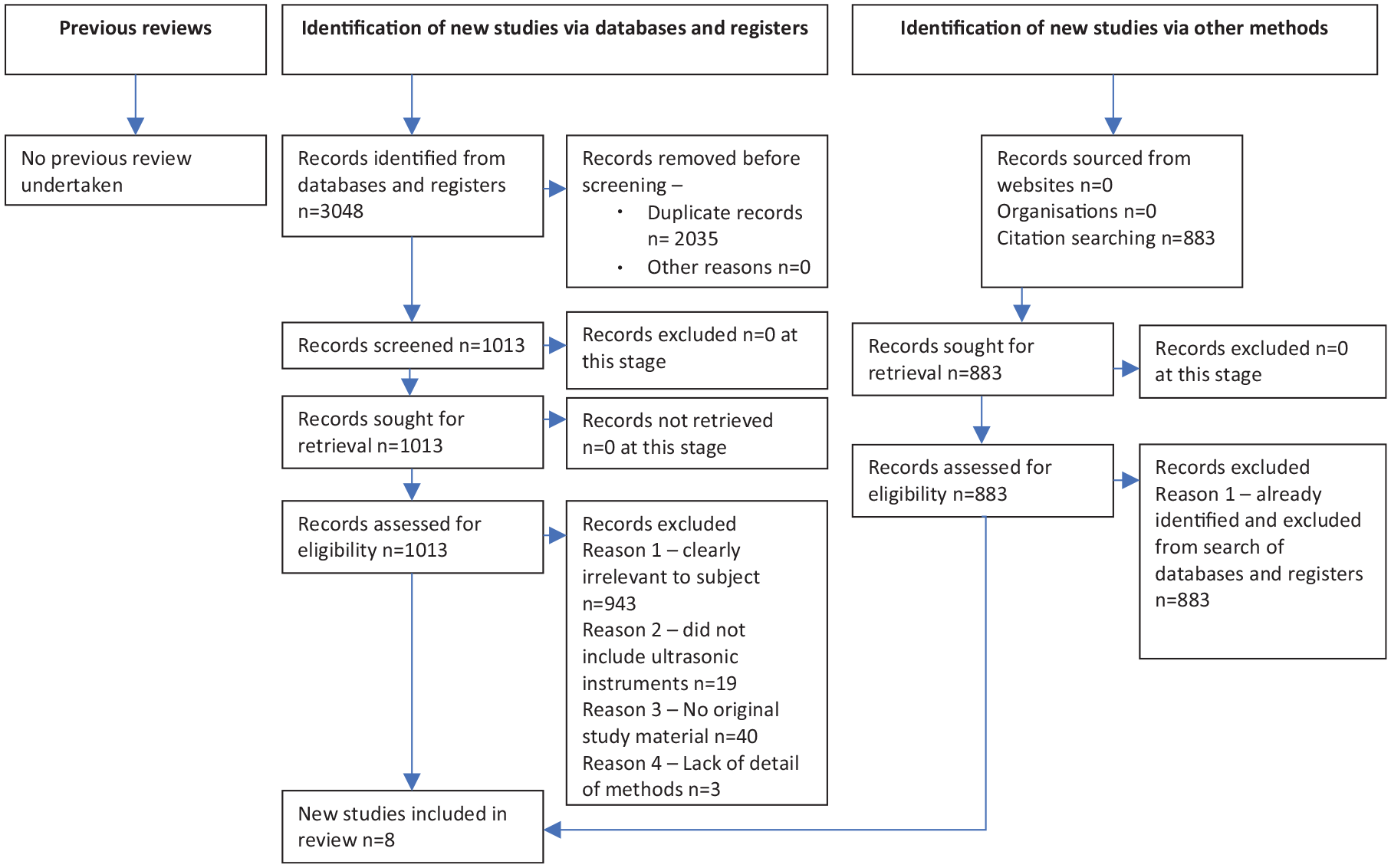
Flow chart of numbers of papers at each stage (PRISMA 2020)
Characteristics of included studies.
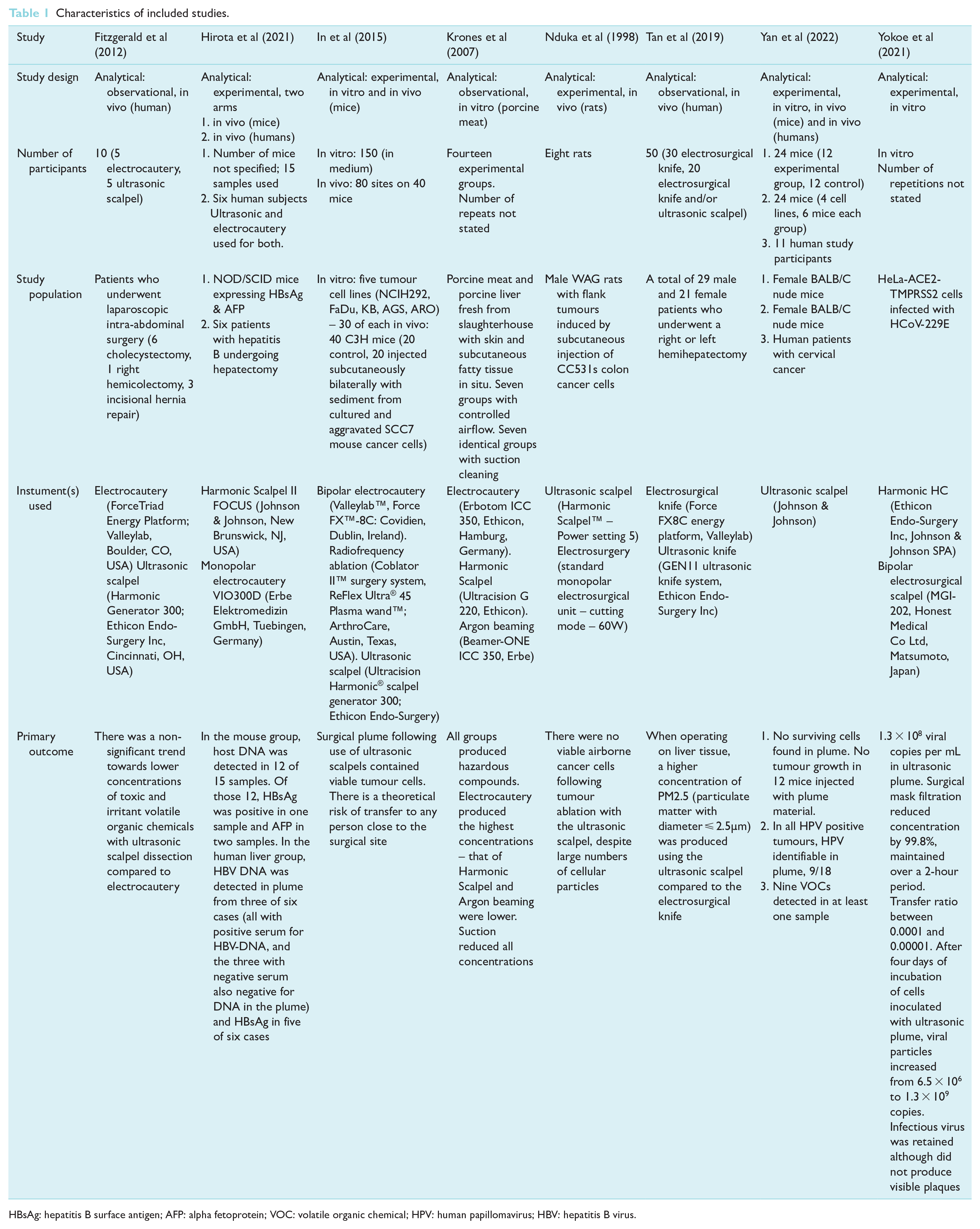
HBsAg: hepatitis B surface antigen; AFP: alpha fetoprotein; VOC: volatile organic chemical; HPV: human papillomavirus; HBV: hepatitis B virus.
Chemical constituents
Fitzgerald et al (2012) collected peritoneal cavity gas during five laparoscopic procedures using electrocautery and five using an ultrasonic Harmonic Scalpel (Ethicon Endo-Surgery Inc, Cincinnati, OH, USA), and compared with cigarette smoke and city air (Nottingham, UK). Diathermy was not used. Of the volatile organic chemicals (VOCs) tested for, the following were detected in the Harmonic Scalpel group (see also Table 2): benzene, ethylbenzene, styrene, toluene, heptane and methylpropene. Of these, one is classified as carcinogenic to humans (benzene), two as possible carcinogens (ethylbenzene and styrene), one not classifiable and two as harmful on contact/inhalation/ingestion IARC (1988). Concentration of styrene was similar in the Harmonic Scalpel and electrocautery groups. The others were all lower in the Harmonic Scalpel group, although the difference was not statistically significant. All concentrations except methylpropene were significantly lower than cigarette smoke, but no differences from city air. Other chemicals not detected were as follows: decene, ethenylmethylbenzene, furfural, acetylene, ethylene, 13-butadiene, methyl thiocyanate, propanenitrile and carbon disulphide. As a laparoscopic study, concentrations could be higher than open procedures.
Chemical constituents of ultrasonic scalpel plume
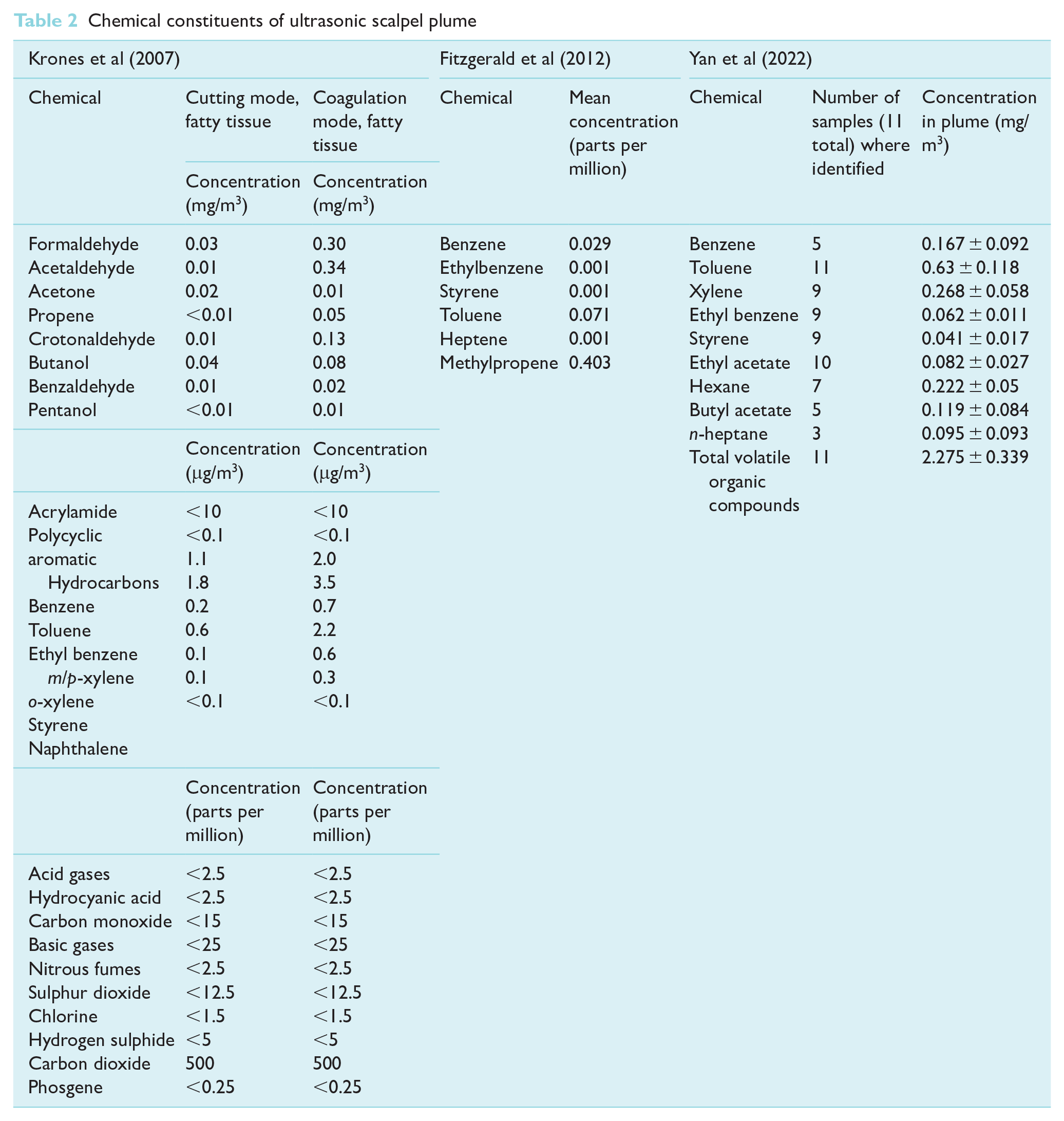
Krones et al (2007) performed in vitro tests on porcine meat and liver comparing 20 minutes of electrocautery, Ultracision G 220 (Ethicon, Hamburg, Germany) and combined electrocautery and argon beaming. Gas samples were collected from 50cm distance, with and without suction. A range of aldehydes, VOC and inorganic gases were detected (Table 1). Concentrations of all chemicals were substantially reduced by suction; however, all were still detectable and VOC consistently lower for the ultrasonic group. However, aldehydes were similar, and inorganic gases were similar between the groups when used on fatty tissue.
Tan et al (2019) performed comparative tests of airborne concentration of PM2.5, a fine particulate matter with diameter <2.5µm and considered a major constituent of air pollution associated with serious pulmonary and cardiovascular effects. Surgical plume from 30 patients undergoing hemihepatectomy with electrosurgery alone was compared with 20 patients where electrosurgery and ultrasonic knife (GEN11 ultrasonic knife system, Ethicon Endo-Surgery Inc) were used. A PM2.5 detector was positioned 5cm from the surgeon’s nose at nose height. The concentration was approximately double in the ultrasonic and electrosurgery group compared to electrosurgery alone (531μg/m3 vs. 280μg/m3, respectively), comparable to a serious pollution state. Liver, muscle and adipose tissues produced different PM2.5 concentrations.
Yan et al (2022) studied the chemical contents of surgical smoke collected during laparoscopic hysterectomy in 11 human cervical cancer patients. Bipolar electrocoagulation was also used. A total of 20 VOCs were tested for by sorbent adsorption and thermal deposition, of which nine were detected, although only toluene was detected in all samples (see Table 2). In comparison with US standards from the National Institute for Occupational Safety and Health (NIOSH) levels of benzene, toluene, xylene and total VOC exceeded the indoor safety standard. Cytotoxicity was tested by assays of two cell lines cultured in smoke-filtered medium, compared with control. In one cell line, there was no significant difference in growth at 24 and 48 hours; however, viability was inhibited at 72 hours in the smoke arm compared to control. In the second cell line, viability was significantly decreased at 24, 48 and 72 hours.
Micro-organisms
Hirota et al (2021) performed ultrasonic scalpel instrumentation on induced tumours in mice producing hepatitis B surface antigen (HBsAg) and alpha fetoprotein (AFP), and excised liver specimens from six humans infected with hepatitis B virus (HBV). HBsAg and AFP levels were measured in collected plume with chemiluminescence enzyme assay and HBV DNA and host genetic material with real-time polymerase chain reaction (PCR). In the mouse group, host DNA was detected in 12 of 15 samples. Of those 12, HBsAg was positive in one and AFP in two. In the human liver group, HBV DNA was detected in plume from three of six cases (all with positive serum for HBV-DNA, and the three with negative serum also negative for DNA in the plume) and HBsAg in five of six cases. Whether this material represents viable virus was not studied.
Yokoe et al (2021) instrumented cell cultures infected with human coronavirus 229E, with Harmonic Scalpel (Ethicon Endo-Surgery Inc) or electrosurgical bipolar scalpel (MGI-202, Honest Medical Co Ltd, Matsumoto, Japan) and collected plume by passing it into culture medium, which was then sampled for virus. Within the ultrasonic group, 1mL of medium contained 1.3 × 108 RNA viral copies, compared to 6.3 × 107 in the electrosurgery group. Further experiments filtered this smoke through a surgical mask graded as an efficacy of ⩾98% in filtering particles over 3µm in diameter (YM-1, HOGY Medical, Tokyo, Japan). Filtration reduced viral copies in the ultrasonic group by 99.80%. When repeated after two hours of cycled aspiration, the number of viral copies was not significantly different at 0, 60 and 120 minutes, indicating persistent effective mask filtration. Tests were also conducted on samples containing varying concentrations of RNA/mL. The transfer ratio was between 0.0001 and 0.00001. Below 2.3 × 106 RNA copies/mL, no RNA was detectable in the aspirated material. Finally, coronavirus infectivity was tested by inoculation of cell plates with medium containing smoke. In samples containing less than 1.3 × 108 copies/mL, no cytopathic effect was observed suggesting considerably reduced infectivity. After four days of incubation, viral copies increased 200-fold (although not generating visible plaques), whereas the electrosurgery group saw a 5000-fold reduction. This could indicate much higher viral survival within ultrasonic plume as compared to that of electrosurgery, although minimal infectivity was shown.
Yan et al (2022) performed ultrasonic scalpel instrumentation of tumours induced in 24 mice with four human cervical cancer cells. Three cell lines were human papillomavirus (HPV) positive and one negative. In all 18 cases involving HPV positive tumours, HPV was detectable in surgical smoke by PCR and flow fluorescence hybridisation. HPV detection was negative in all cases in the mice with HPV negative tumours. To test infectivity, an HPV negative cervical cancer cell line was cultured in medium filtered with smoke from each HPV positive cell line group for 72 hours, then in normal culture for a further 72 hours. HPV positivity was found in 6/6, 3/6 and 6/6 of the samples for each of the three cell lines at 72 hours, and 4/6, 2/6 and 3/6, respectively, after the further 72 hours culture. This gives a total of 15/18 HPV positive at 72 hours, and 9/18 positive at 144 hours.
Malignant cells
In et al (2015) manipulated five tumour cell lines with radiofrequency ablation, electrocautery or Harmonic Scalpel (Ethicon Endo-Surgery Inc) and collected smoke from 5 to 10cm distance. Collected smoke was transferred to a culture medium and DNA genotyping conducted if cellular proliferation observed. Each cell line experiment was replicated five times. Harmonic Scalpel plume collected from 5cm cultured viable cells in all 25 experiments but from 10cm in only two. No viable cells in the radiofrequency ablation or electrosurgery groups. DNA genotyping revealed cultured cells to be identical to the instrumented cell lines.
An in vivo arm inoculated the same smoke into the bilateral lower back of 20 mice and compared with 20 controls. This demonstrated tumour growth at 16 out of 40 injected sites in the experimental group at two weeks, with histology demonstrating malignant features.
Nduka et al (1998) investigated the morphology and viability of in vivo aerosolised tumour cells with the use of Harmonic Scalpel (Ethicon Endo-Surgery Inc) on induced tumours in rats. This showed large quantities of cellular debris in the plume (>1 × 107 cell debris/mL) on light and electron microscopy, mainly subcellular amorphous aggregates but with ‘very few’ that on the basis of size could be morphologically intact cells. No viable cells were demonstrated on Trypan blue staining, and no growth observed after one week of culture.
Yan et al (2022) instrumented tumours in mice induced with human cervical cell cancer cells, using the Harmonic Scalpel (Ethicon Endo-Surgery Inc). Microscopy of smoke samples with haematoxylin and eosin and Papanicolaou stains showed large quantities of cellular debris, several morphological intact epithelioid cells but no viable malignant cells. Trypan blue staining suggested these epithelioid cells were non-viable. Culture of smoke samples for two and five days showed no growth. Inoculation of surgical smoke material into the hind limbs of 12 mice and observation for three months showed no tumour development.
Discussion
Ultrasonic scalpel plume contains a wide range of chemicals including known human carcinogens; however, determining the level of risk posed to patients and operating staff is complex. All are predominantly a risk via inhalation (HSE 2020). Exposure is determined by many factors, including the device and usage, operated tissues, proximity to the device, ventilation, use of personal protective equipment (PPE) and smoke evacuation.
In the UK Control of Substances Hazardous to Health (COSHH), regulations legally oblige employers to protect workers from exposure to hazardous substances by not exceeding workplace exposure limits (WELs). Limits are defined by the UK Health and Safety Executive (HSE) and quoted as time-weighted averages – equivalent to a concentration in parts per million (ppm) over continuous periods of exposure of either eight hours or 15 minutes. Cross-referencing data on chemical concentrations from papers found here with UK WEL from January 2020 (HSE 2020) gives some idea of risk although with several caveats. WEL is based on a continuous exposure, whereas in surgery plume, it is largely non-continuous. Also, most studies analysed plume collected close to the instrument. Plume will be more dispersed at the surgeon’s nose position and factors like ventilation and smoke evacuation will have a significant influence. In general, for the chemicals with a defined WEL, the detected concentration was much lower than the 8-hour WEL. For example, styrene was detected at 0.001 ppm (Fitzgerald et al 2012), some five orders of magnitude lower than the 8-hour WEL of 100ppm. Some measurements were closer to the WEL – carbon monoxide was measured at <15ppm (Krones et al 2007), with an 8-hour WEL at 20ppm. Three exceeded WEL – sulphur dioxide at <12.5ppm (Fitzgerald et al 2012) with 8-hour WEL at 0.5ppm, chlorine at <1.5ppm with WEL at 0.5ppm and phosgene at <0.25ppm with 8-hour WEL at 0.02ppm. These findings surely warrant further study. None of the studies investigated any clinical effect.
Studies on laser smoke demonstrated presence of HPV, Staphylococcus, Neisseria and Corynebacterium (Capizzi et al 1998), and HPV transmission to a surgeon using laser has been confirmed (Hallmo & Naess 1991). Concern for microorganism transmission within ultrasonic plume is theorised as more likely than laser and electrocautery devices due to the plume having higher water content, larger particles (Barrett & Garber 2003), lower temperature (Ziegler et al 1998), no burning process (Champault et al 1997) and fairly wide scatter (Ott et al 1998). Low temperature surgical aerosol has been shown experimentally (not with ultrasonic instruments) to contain viable human immunodeficiency virus (HIV) (Johnson & Robinson 1991). Two studies investigating presence of hepatitis virus material in ‘ultrasonic dissector’ irrigation fluid were excluded due to lack of detail of the instrument used and methods (Higashi et al 1994, Matsumata et al 1991) and the equipment differing from modern instruments. In the last two years, studies have identified HBV DNA and HBsAg (although whether this represented viable virus was not tested) and coronavirus 229E (although minimal infectivity in terms of cytopathic effect was observed) in ultrasonic plume, and transfer of HPV via plume.
The presence of viable cells within surgical smoke has been long-debated. Viable cells have been isolated from laser (Hoye et al 1967, Ziegler et al 1998) and laparoscopic electrosurgery smoke (Champault et al 1997, Fletcher et al 1999). Others found morphologically intact but non-viable cells (Oosterhuis et al 1982). A brief preliminary study by Nahhas (1991) was not included here which performed Papanicolaou staining of mist debris from surgeons’ goggles after instrumenting ovarian tumours and demonstrated ‘numerous fresh, intact and possibly viable tumour cells’. No further details were given. This review found conflicting evidence from animal studies and no human studies. The clinical relevance of this is currently unknown with no evidence of harm.
PPE, evacuation devices and filters on laparoscopic instruments can help protect theatre staff (Hahn et al 2017). The UK Health and Safety Executive (2012) conducted a literature review but made virtually no mention of ultrasonic devices. Smoke evacuation devices are known to be effective (Krones et al 2007, Ott et al 1998). High volume suction built in to a diathermy tip is very effective at reducing smoke levels detected at surgeon mask position (Pillinger et al 2003), which could be used for ultrasonic instruments. Smoke evacuation with pump intake and exhaust filters are recommended for laser surgery (MHRA 2015), held within 5cm of the surgical field (Georgesen & Lipner 2018). Standard surgical masks have been shown to be ‘absolutely ineffective’ at preventing ingress of toxic volatile chemicals from surgical smoke (Kocher et al 2019). Highly efficient seal-tight respirator facemasks are recommended where smoke is generated (Georgesen & Lipner 2018, Li et al 2020). Yokoe et al (2021) found high-grade surgical masks to be extremely effective at filtering human coronavirus particles in an experimental study. In a systematic review on PPE for surgical smoke, Georgesen & Lipner (2018) found no evidence on eye protection, but advised it for all surgeons. Further study is required of any risk to patients, surgeons and other theatre staff posed by plume. It appears likely the SARS-CoV-2 (COVID-19) pandemic has magnified awareness of these issues.
Limitations of this study include the small volume of literature available. The studies have heterogeneous design, study population and procedure type, using instruments by different manufacturers. Combining such studies in a literature review was deemed appropriate in this case, as no meta-analysis was possible and result synthesis would be narrative, and for the purpose of finding all available evidence. Some of the studies present experimental data with uncertain clinical significance. It is considered the search strategy was sufficiently robust that very few important studies would be missed.
Conclusion
Ultrasonic plume contains harmful chemicals, some carcinogenic. These are mostly, but not always, well below WEL and much reduced by effective evacuation and surgical masks. Any risk from these constituents has not been studied in a surgery context. There is some experimental evidence of presence of hepatitis virus, coronavirus and HPV material within plume but with no human studies. There is conflicting evidence from experimental studies of the presence of viable malignant cells but again no human studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.