
Abstract
Epidural analgesia is often considered cornerstone in multimodal analgesia when used in major surgeries. However, its role in managing acute postoperative pain in elderly patients is debatable because of its known potential complications. Furthermore, postoperative pain in elderly patients is under-treated because of complex comorbidities, and they are more prone to adverse events related to pain therapies. All systemic analgesic drugs have pharmacological limitations and precautions in elderly people. Recent meta-analyses showed that epidural analgesia provided better postoperative pain control compared to intravenous opioids. Interestingly, peripheral nerve blocks had no superior control of pain over epidural analgesia. In addition, epidural analgesia has shown to positively affect perioperative morbidities and mortalities, and reduce opioid-related side effects because of its non-analgesic effects on each organ system. When tailored in a specific multimodal approach, it shortens the intensive care and hospital stays. In conclusion, if complications are identified and treated early, and contraindications are ruled out, epidural analgesia can achieve sufficient postoperative pain management with insignificant adverse events in this population.
Introduction
While several studies exist that address the challenges of achieving good management of acute pain, few discuss this specifically in older people in the postoperative context. Despite its increased prevalence in elderly people, pain is undermanaged in the postoperative period, and inadequate therapy, with under-use of opioids, is common in this age group (Egbert et al 1990, McKeown 2015, Mcnicol et al 2015). This point is important because elderly people represent the fastest-growing segment of the world population especially in developed countries, and undergo surgery four times more than other age groups (Rooke et al 2002).
Elderly patients often suffer from diminished physiological reserve and chronic disease due to decreased organ function with ageing. Frailty is also common in this age group and is presented through different combinations of symptoms and signs including weakness, fatigue, mild cognitive changes, decreased balance, slowed motor skills and increased vulnerability to stressors (Walston et al 2006). Furthermore, age-related changes in pharmacology and physiology can affect postoperative pain management and increase the risk of adverse effects.
Regional anaesthesia and analgesia techniques, including epidural analgesia and peripheral nerve blockade, are widely used to achieve the best management of postoperative pain with minimum adverse effects. Several meta-analyses examined the role of epidural analgesia in postoperative pain control compared to other strategies. This review summarises limitations, benefits and current trends regarding the acute postoperative pain in elderly patients, with a focus on epidural opioids, compared to other modalities used to manage acute postoperative pain in elderly people.
Benefits versus risks of pain treatment in the elderly people
The elderly population is defined by the World Health Organization (WHO) as those older than 65 years. Moreover, they can be subdivided into three subgroups: ‘old–young’ (65–75 years), ‘old’ (75–85 years) and ‘very old’ (over 85 years)(Saleh 1993). Age-related physiological changes must be taken into consideration during the management of acute pain in elderly patients because they are individualised and progressive. Individuals only differ in their rate of onset (Macintyre & Upton 2003).
Anaesthetists must be capable of treating pain with awareness of the physiologic changes and comorbidities that are common in the elderly. They must also seek safety of different analgesic modalities, both pharmacologic and interventional, in balance with this age group’s peculiarities. Major areas of risk and their mechanisms of action are illustrated in Figure 1. These areas of risk are important to identify especially when trying to achieve adequate control of pain (McKeown 2015).
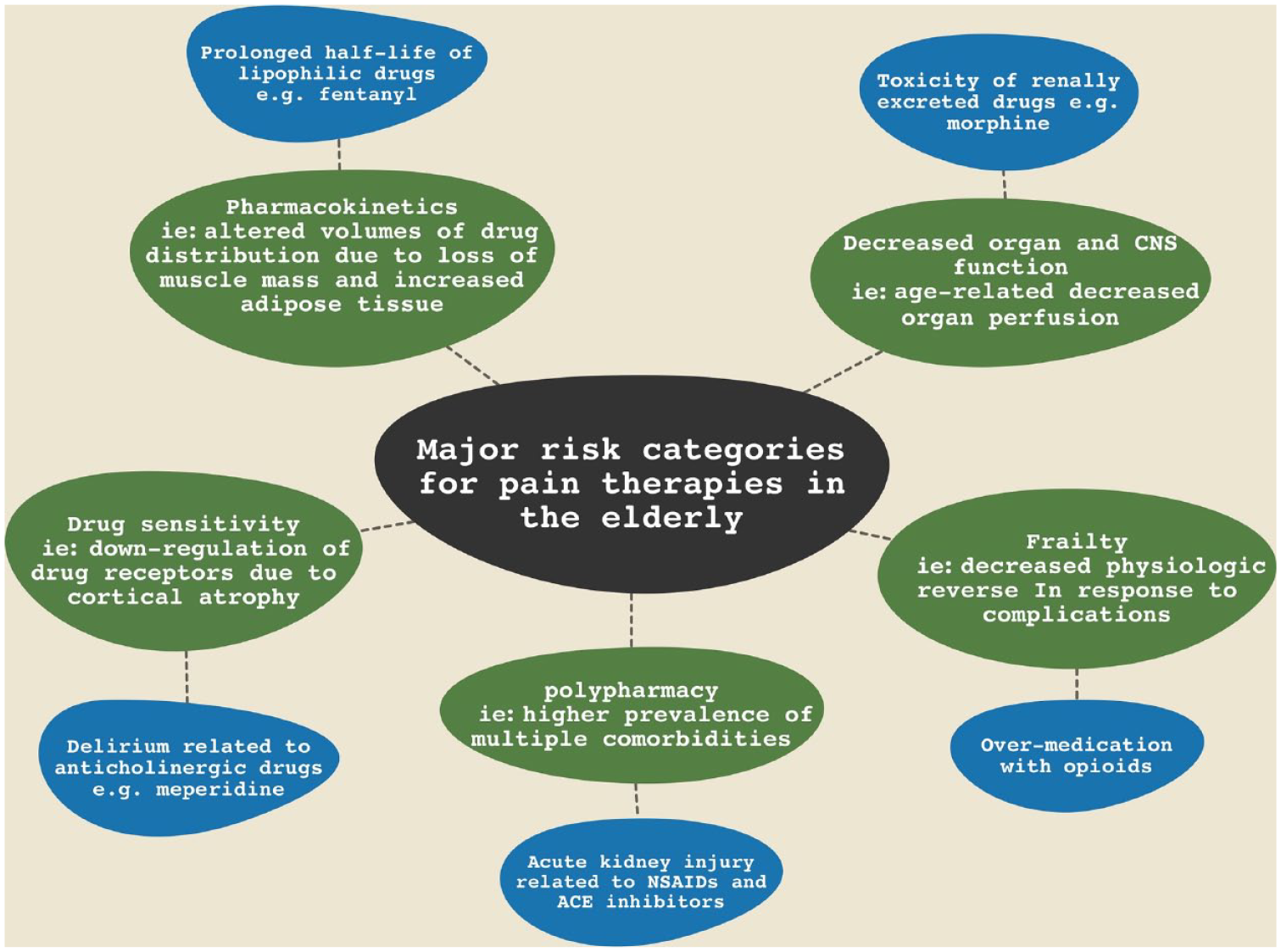
Risk categories for pain therapies in the elderly
Adequate analgesia contributes to many beneficial postoperative outcomes such as decreased cardiopulmonary adverse effects, shorter hospital stays, smoother rehabilitation, less readmissions and lower incidence of chronic pain syndromes. Therefore, it can be even more beneficial in an elderly patient who is already at higher risk for nosocomial complications (eg: delirium) or who has ongoing functional limitations or issues with chronic pain (Falzone et al 2013).
Compared to younger patients inadequate pain control can cause myocardial infarction due to increased heart rate, risks are high. If the pain control is not adequate, the risk of myocardial infarction increases due to increased heart rate, blood pressure and myocardial oxygen demand. Also, this may extend to regional impairment of ventilation, shallow respiration and impaired cough reflexes which can lead to atelectasis, infection, hypoxemia and even respiratory failure, especially after thoracic or upper abdominal surgeries. Uncontrolled pain can also induce or worsen ileus which increases the duration and cost of hospital stay (Cook & Rooke 2003).
For the elderly, the advantages of adequate pain treatment with minimal side effects can significantly enhance the postoperative recovery in a positive way.
Physiological changes in elderly patients and the limitations of pain treatment
When dealing with unwanted adverse effects of drugs, physiological reserves and compensatory mechanisms are limited in older people compared to younger populations.
Regarding the cardiovascular system, hypovolemia and impaired sympathetic response can occur following regional anaesthesia and analgesia which may be dangerous if it was not properly anticipated by use of lower doses of, preferably, morphine alone or with low doses of local anaesthetics for pain treatment in this age group. Reduced hepatic blood flow may lead to a 25% up to 40% decrease in morphine clearance with high extraction ratio across the liver. A higher peak arterial concentration of IV morphine could be expected if the cardiac output decreased up to 20% (Androw 2003).
The pulmonary system is also affected by ageing in the form of decreased sensitivity of the respiratory centres to hypoxia and hypercapnia, diminished cough, increased anteroposterior diameter due to ossification of costal cartilages and calcification of the joints of the ribs, and higher incidence of obstructive sleep apnea. Consequently, performing regional anaesthesia or analgesia would be anatomically difficult. The incidence of complications such as pneumonia and atelectasis is disproportionately higher in this age group. Also, the risk of hypoxemia and morphine overdosage is increased which requires oxygen and slow titration of the morphine dosage, respectively (Connoly 2003, Cook & Rooke 2003).
Elderly people are at a higher risk of kidney disease, meaning that their response to maintain normal homeostasis is slower. Moreover, the glomerular filtration rate (GFR) and tubular excretion and reabsorption are decreased, as well as metabolism and clearance of medications and metabolites, for example, morphine. Therefore, creatine clearance is the most reliable method to determine GFR (Cook & Rooke 2003, Epstein 1996).
Regarding the digestive system, gastric prostaglandins, bicarbonate and nonparietal fluid decrease with age. In addition, helicobacter pylori infestation and constipation are common in the elderly. Therefore, they are more prone to mucosal damage from nonsteroidal anti-inflammatory drugs (NSAIDs). Drugs such as anticholinergic, dopaminergic drugs and opioids often worsen constipation (James 2003).
Regarding decreased body mass and a change in plasma proteins that occurs with ageing, the total body water reduced, while adipose tissue increases. Consequently, the distribution and redistribution of drugs and their clearance and elimination is altered in elderly patients (Guay et al 2003). Psychoactive drugs that are fat soluble, such as diazepam or fentanyl, have an increased volume of distribution, whereas water-soluble drugs, such as morphine, have a decreased volume of distribution. Because of the decrease in serum albumin that binds to acidic drugs such as naproxen, they have increased free or unbound drug and decreased protein bound drug in the plasma (Eddington 1996). On the contrary, basic drugs such as lidocaine have a decreased drug-free action because the binding alpha-1 acid glycoprotein remains the same or rises.
For epidural analgesia, the intervertebral foramina are progressively occluded with connective tissue preventing the spread out of the epidural space. Furthermore, the use of epidural analgesia has decreased clinically in older adults, not because of any bias versus the technique, but rather because many elderly patients are on anti-platelet medication and anti-coagulnts. In such cases, epidural analgesia would be contraindicated however, ultrasound-guided peripheral nerve blocks (PNBs) can still be used for postoperative analgesia with a lower risk of adverse effects. Anticoagulants are stopped prior to surgery dependent on the type of anticoagulation and national guidelines.
Systemic versus epidural analgesic therapy of acute postoperative pain
At any age group, adequate analgesia in postoperative pain management is a primary aim of treatment and opioids are the cornerstone of the analgesic plan. On the some older studies showed that epidural opioids provide better postoperative analgesia compared to IV route (Eisenach et al 1988, Harrison et al 1988), other older studies have shown these two routes to be equally effective (Camann et al 1992, Camu & Debucquoy 1991, Ellis et al 1990, Glass et al 1992, Loper et al 1990).
To get a higher level of evidence regarding that debate, a recent Cochrane meta-analysis evaluated the use of postoperative epidural analgesia, where analgesic efficacy of parental and epidural opioids for postoperative analgesia was examined (Weibel et al 2017). Epidural analgesia was compared to IV patient-controlled analgesia (PCA) in ten trials for pain management in labour. Overall, epidural analgesia was better; the standardised mean pain score after one hour in the PCA group was 0.57 higher (0.31 higher to 0.84 higher), and nearly all epidurally administered regimens resulted in overall better satisfaction with pain relief compared with intravenous opioids for both pain at rest and incident pain. However, the quality of this evidence using GRADE was very low in this article. In addition, only 10 per 1000 required additional analgesia in the epidural group compared to 93 per 1000 in the PCA group, and the quality of evidence was moderate using GRADE.
We also examined another meta-analysis of 100 controlled trials, where the analgesic efficacy of postoperative parentral and epidural opioids was evaluated (Block et al 2003). Epidural analgesia was compared to IV PCA in 48% of these trials, and to IV shots of opioids on patient demand in 43% of them. Surgeries performed were thoracic, abdominal, pelvic (including caesarean section delivery) and lower extremity. Overall, epidural analgesia was also better: parenteral analgesia had visual analog scale (VAS) pain scores from 16.2 to 42.5mm, compared with 12.0mm for epidural analgesia (p value < 0.001) at all time points measured (Viscusi 2005). Also, nearly all epidurally administered regimens resulted in better analgesia compared with intravenous opioids for both pain at rest and incident pain. Patients who received intravenous analgesia had mean VAS scores ranging from 12.1 to 31.3mm for pain at rest and from 36.2 to 60.2mm for incident pain. In patients who had epidural analgesia, mean VAS scores were from 6.9 to 26.5mm for pain at rest and from 24.7mm for incident pain (p value < 0.001 for all measures) (Viscusi 2005). VAS scores were decreased by 30%–33% for patients who had epidural analgesia compared with intravenous analgesia, a magnitude of effect that can be considered clinically relevant (Viscusi 2005). Results for epidural analgesia extended as favourable across patient populations, including the elderly. Regarding abdominal surgery, all types of epidural-administered regimens (local anaesthetic with or without opioid added, opioid alone) provided better analgesia than intravenous opioids. Mean VAS scores ranged from 16.0 to 31.4mm for epidural analgesia compared with 33.9–38.1mm for intravenous analgesia (p value < 0.001). Similar results were observed in analyses for pelvic and lower extremity surgeries. Patients who underwent thoracic surgery, thoracic epidural analgesia (TEA) using a local anaesthetic, with or without an opioid added, showed the greatest improvement in analgesia. Mean VAS scores were 16.5–21.8mm for epidural analgesia, compared with 24.7–27.6mm for intravenous analgesia (p value < 0.002).
Considering this work, epidural analgesia, regardless of analgesic agent, location of catheter placement, and type and time of pain assessment provided better postoperative analgesia compared with parenteral opioids. The limitation to this conclusion is that most of the studies are in the field of orthopaedic and obstetric surgery, therefore focusing on a young population (Viscusi 2005).
Epidural analgesia versus PNBs as a postoperative analgesia
PNBs are becoming a popular choice for management of acute postoperative pain, especially in the frail elderly. On searching the literature for a high-quality evidence, four most recent meta-analyses were found that compare epidural analgesia with other regional modalities after hip, knee, thoracic and abdominal surgeries.
Regarding hip surgery, a network meta-analysis of 1111 patients from 13 studies on 24- 48 hours pain management was examined. This meta-analysis compared epidural analgesia with facia Iliana compartment block (FIB), femoral nerve block (FNB), local infiltration analgesia (LIA), lumbar plexus block (LPB), periarticular injection (PAI) and posterior nerve block (PNB) (Liu et al 2019). The effect of the six studied intervention was not statistically different to each other and epidural analgesia. It was also found that LPB is a slightly better choice to reduce pain 12–4 hours after total hip arthroplasty (THA). However, limited sample size and moderate pain scores reported by the patients might be related to these findings. Therefore, further studies are needed to assess the efficacy of these modalities at a longer time.
After total knee replacement surgeries, another recent meta-analysis of 670 patients from 12 randomised controlled trials (RCTs) on 0–12, 12–24 and 24–48 hours postoperative pain comparing PNB and epidural analgesia was considered (Gerrard et al 2017). There was no significant difference in VAS scores at the three endpoints between the two groups; 0–12 hours (Mean Difference (MD) –0.48; 95% confidence interval (CI) –1.0 to 0.11, p = 0.11), 12–24 hours (MD 0.04; 95% CI –0.81 to 0.88, p = 0.93) and 24–48 hours (MD 0.16; 95% CI –0.08 to 0.40, p = 0.19). However, epidural analgesia was found to have significantly higher risk of postoperative nausea and vomiting (PONV) (RR 1.65; 95% CI, 1.20–2.28, p = 0.002), hypotension (RR 1.76; 95% CI, 1.26–2.45, p = 0.0009) and urinary retention (Risk Ratio (RR) 4.51; 95% CI, 2.27–8.96, p < 0.0001) in comparison to PNB.
Regarding thoracic surgery, a recent Cochrane systematic review and meta-analysis of 195 patients undergoing cardiac surgery from two studies compared TEA with PNBs (Guay & Kopp 2019). There was no, or little, difference in pain at rest at 48 hours after surgery between the two modalities. However, there was one trial of 50 patients that reported that pain score, on movement or on coughing at 48 hours is lower with bilateral erector spinae block than with epidural analgesia (MD 1.36, 95% CI 0.76–1.96). Results were inconclusive for secondary outcomes such as risk of myocardial infarction, risk of atrial fibrillation and flutter, risk of pulmonary complications and risk of neurological complications because of lack of data and high risk of bias.
Continuous peripheral nerve blocks (CPNBs) are also becoming more popular after abdominal surgeries such as wound catheter, intraperitoneal catheters, peritoneal catheters, transversus abdominus plane (TAP) catheters, rectus sheath catheters and paravertebral catheters (Baily et al 2021). In overall comparison of the latter six modalities with epidural analgesia, a recent systematic review and meta-analysis of 1646 patients from 26 trials found no statistically significant difference in pain management. Furthermore, no statistically significant difference was found in PONV between the two groups. Opioid consumption at 48 hours was lower with epidural analgesia than with CPNBs (MD –16.13; 95% CI –32.36 to –0.10). Moreover, the length of hospital stay was lower with epidural analgesia (MD –0.78 days; 95% CI; –1.29 to –0.27) compared to CPNBs. However, the quality of all evidence in this analysis is low using Cochrane and Grade recommendations.
Based on the above analyses, a benefit–risk assessment of epidural analgesia should be in mind, especially in the elderly patients. In orthopaedic surgery, the risk of epidural analgesia outweighs its benefit. Therefore, PNBs are more practically and clinically useful. On the contrary, the benefit of epidural analgesia is higher in thoracic and abdominal surgeries because its non-analgesic effects outweigh its risk.
Non-analgesic effects of epidural analgesia
Beside analgesia, there are further non-analgesic effects of the epidural analgesia. It is assumed that the resorption of the local anaesthetic injected produces a selective sympathetic trunk blockade (Weiss & Pöpping 2018). The extent of this blockade corresponds to the range of the sensory blockade, even partially beyond in clinical practice. Fibres supplying the cardiopulmonary system (T1–T4) and gastrointestinal nerves (thoracic and lumbar splanchnic nerves, T5–L2) can be largely influenced by TEA (Weiss & Pöpping 2018). In lumbar epidural analgesia (LEA), these effects are limited so that non-analgesic effects are less pronounced due to physiological and anatomical reasons (Sagiroglu et al 2014, Scott et al 1996). In addition, there are central nervous system–related side effects that can be spared via alternatives of LEA in peripheral regional anaesthesia with equipotent analgesia effect (Sakai et al 2013).
From a pathophysiological point of view, emerged possible effects on various organ systems are discussed.
Gastrointestinal effects
The selective sympathetic blockade of TEA results in an increased intestinal perfusion and gastrointestinal recovery is therefore promoted (Freise et al 2008, Freise & Fischer 2009). It has been shown that pain and perioperative stress can seriously disturb gastrointestinal homeostasis. This can lead to intestinal motility disorders or even ileus. Compared to systemic opioids, TEA has been shown to reduce the time needed for intestinal function to return to normal by 37 hours (95% CI 19–55 hours) with epidural local anaesthetics alone and by 24 hours when on epidural opioids (95% CI 10–38 hours) (Guay et al 2016, Jørgensen et al 2001, Zingg et al 2009). Peristalsis is resumed significantly slower under LEA than under TEA (Freise et al 2008). The incidence of postoperative ileus is significantly decreased under TEA if injected above T12 (Scott et al 1996, Steinbrook 1998, Zingg et al 2009). In addition, opioid consumption of patients with epidural analgesia was significantly reduced. A study demonstrated that patients under TEA used as nearly half the amount of morphine (59 mg) as the control group (123 mg), 48 hours postoperatively. Consequently, there is also a significant decrease of side effects related to opioids, such as nausea and vomiting, sedation, respiratory depression and ileus (Block et al 2003, Guay et al 2016, Pöpping et al 2008b, 2014). A meta-analysis concluded that reduction of epidural analgesia is superior to systemic opioids in terms of reduction of ileus. The incidence of postoperative ileus reached 3.6% in the group that received a combination of general anaesthesia (GA) and epidural analgesia, while it was 8.5% (odds ratio [OR] 0.43, 95% CI 0.21–0.88]) in the opioid-based group (Liu et al 2004). In addition, a recent review showed that a TEA does not only reduce the duration of ileus but also prevents reductions in gastric conduit perfusion and enhances intestinal blood flow and as well after oesophageal surgery (Feltracco et al 2018, Guay et al 2016). The suspicion that anastomotic leakage occurs due to early postoperative peristalsis or perioperative hypotensive episodes after abdominal surgery could not be proven. Such effects could not be proved by recent studies (Gendall et al 2007, Jestin et al 2008). On the contrary, a positive effect of epidural analgesia on the stability of anastomoses was found (Michelet et al 2005).
Cardiovascular effects
For non-cardiac surgery patients, the most common cause of perioperative morbidity and mortality is cardiovascular events that account for about 2%–15% (Mangano 1990). In addition, the number of cardiovascular postoperative complications increases because cardiovascular risk profile increases with older age of patients. Both individual preclinical profile and increased sympathetic activity perioperatively seems to have a key role in pathogenesis of cardiovascular complications. Sufficient analgesia is postulated to influence this pathogenetic process and decrease perioperative cardiovascular complications by a direct and/or indirect reversible sympathetic inhibition.
Several clinical studies and meta-analyses investigated the influence of TEA on cardiovascular morbidity. Rodgers et al (2000) and the MASTER Trial of Rigg et al (2002) are of the most cited papers. Rodgers et al (2000) described one-third decrease incidence of myocardial infarction under TEA. However, both studies did not detect a statistically significant difference on cardiovascular complications and were later accused of methodological weaknesses.
In another meta-analysis by Guay (2006), arrhythmias, among cardiovascular endpoints, decreased significantly in patients under epidural analgesia. Despite lacking statistical significance, evidence showing a protective effect against myocardial infarction was found (Guay 2006). A follow up meta-analysis in 2011 underlines this tendency. A decreased perioperative myocardial infarction rate was found. However, this reduction was not statistically significant with no reduction in perioperative mortality (Gauss et al 2011). A recent meta-analysis from 2014 confirmed both results (Pöpping et al 2014).
It should be noted that in Guay’s meta-analysis, LEA and TEA were not clearly differentiated (Guay 2006). Another study showed a significantly reduced rate of myocardial infarction postoperatively in patients under TEA for at least 24 hours after surgery (Beattie et al 2001), while there was no such an effect in those receiving LEA (Beattie et al 2001, Rodgers et al 2000). Underlining this, adverse cardiac events in patients with coronary heart disease undergoing major abdominal cancer surgery decreased (Mohamad et al 2017) while myocardial perfusion was increased (Nygård et al 2005).
Overall, the data on epidural analgesia showed inconsistency regarding reduction in the incidence of myocardial infarction, whereas it has been proved beneficial in the reduction of arrhythmic complications (Weiss & Pöpping 2018).
Pulmonary effects
Major upper and lower abdominal surgery along with thoracic and vascular operations are a high risk regarding pulmonary complications (Qaseem et al 2006). There is much evidence in literature, reflected by both systematic reviews and RCTs that a TEA has a positive effect on pulmonary complications. This may be due to the epidural analgesia itself, to improved pain relief or arterial oxygenation, a combination of these factors or yet another mechanism. However, the exact mechanism is not fully understood. Ballantyne et al were first to demonstrate systematically such effects as improved lung function, a reduced rate of atelectasis and reduced infectious complications (Ballantyne et al 1998). In addition to confirming these results, a meta-analysis from 2008 demonstrated a reduced rate of postoperative pneumonia for thoracic and abdominal surgeries (Pöpping et al 2008a). Interestingly, another unexpected finding of this analysis was that improvement in standard care analgesia has led to a decrease in the baseline risk of pulmonary complications, which has lessened this beneficial, lung-protective effect over the last 35 years. Nowadays, patients benefit from multimodal analgesia and opioids delivered via PCA devices. This may be the reason why postoperative pulmonary complications have decreased in high-risk patients over time even without epidural analgesia. Furthermore, patients with severe pulmonary lung diseases, such as severe asthma and chronic obstructive pulmonary disease (COPD), seem to benefit the most from epidural analgesia both perioperatively and postoperatively (Van Lier et al 2011).
Conclusion
Pain management in elderly patients is difficult because they are more prone to adverse effects. Physiological and pharmacological changes favour the titration of medications during and after surgery. In comparison with systemic opioids, epidural analgesia provides better control of postoperative pain regardless of location of catheter placement, and type and time of pain assessment. Plexus blocks do not provide superior control of pain when compared to epidural analgesia, but evaluation of the risk–benefit is required. Evidence-based protocols and recommendations should be used to avoid empirical treatment and reduce adverse effects. More studies that compare PNBs and epidural analgesia in the elderly patients are needed with focus of their non-analgesic effects.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.