
Abstract
Hip fractures are common injuries in the elderly and are associated with significant morbidity and mortality. There are multiple perioperative factors that must be considered when managing these patients. These include analgesia, timing of surgery, choice of operation, type of anaesthesia, postoperative complications and comorbidities. Guidelines from The National Institute for Health and Care Excellence and the National Hip Fracture Database have been updated to reflect many of the above, but the importance of psychosocial factors is still emerging. This article focuses on the evidence for the key perioperative factors in hip fracture management and the tools available to predict hip fracture outcome.
Introduction
Approximately 76,000 patients with a hip fracture were admitted to a hospital in England in the past year (Hospital Admitted Patient Care Activity 2018–19). Of these patients, 84% were aged 70 years or older. Hip fracture is therefore the most common serious injury in the elderly and its incidence is set to double over the next 25 years in parallel with our ageing population (White & Griffiths 2011). These patients require surgery but are often poor surgical candidates due to frailty and comorbidity.
Hip fractures are associated with significant morbidity and mortality, especially amongst the elderly. According to the National Hip Fracture Database (NHFD), approximately 7% of hip fracture patients die within one month (NHFD 2018). In Europe, 23% die within one year of fracture (Downey et al 2019). Of those that survive, only half return to mobilisation, even with the aid of walking devices (Dyer et al 2016). It has been reported that 40% of patients are discharged directly to long term care facilities or nursing homes rather than their prefracture place of residence (Dyer et al 2016). Hip fractures can have psychosocial effects on the patient and their family.
Hip fractures also represent a large financial cost to our resource-strained healthcare system (Leal et al 2016). This is especially true during the perioperative period in which patients receive expensive analgesia, investigations and timely surgery. The NHFD reports that the average hip fracture patient may remain in hospital for up to 20 days (NHFD 2018). This equates to over 1.5 million bed days per annum in the UK (NHFD 2018). Taking social care and follow-up costs into account, this one injury uses 1% of the entire NHS budget – over £1 billion per year (Leal et al 2016).
As a result, The National Institute for Health and Care Excellence (NICE) has produced detailed guidelines on hip fracture management (NICE 2011). These emphasise the importance of early surgery and coordinating a multidisciplinary team to maximise recovery in these patients. Best practise tariffs are based on these recommendations and several other metrics as outlined by the NHFD. Healthcare providers must abide to these guidelines in order to be reimbursed financially for the care hip fracture patients receive (Metcalfe et al 2019).
The aim of this review is to use an evidence-based approach to raise awareness of the important perioperative factors that healthcare professionals need to consider in cases of hip fracture. Whilst this review may not be exhaustive, it helps to rationalise the latest hip fracture guidelines and optimise the perioperative care of these patients.
Preoperative considerations
Assessment
Hip fractures classically present with hip and/or groin pain worse on movement, and an inability to weight bear (LeBlanc et al 2014). If the fracture is displaced, the affected limb may appear shortened and externally rotated (LeBlanc et al 2014).
History taking in these patients should include mechanism of trauma, such as a fall, and the presence of any comorbidities. One should also perform an Abbreviated Mental Test Score (AMTS) and nutritional assessment in accordance with current best practise tariffs (NHFD 2018). The hip joint should be examined, and a distal neurovascular assessment should be performed and documented (LeBlanc et al 2014). Investigations include routine blood tests such as a full blood count, urea and electrolytes, glucose, a clotting screen and a group and save (Costa et al 2016, Bhatti & Ertl 2019).
Electrolytes are particularly important in elderly patients who have had prolonged periods of immobility secondary to their fracture (eg: a long delay to arrival at hospital). This will identify hyperkalaemia secondary to rhabdomyolysis (Griffiths et al 2012). Plain X-rays should be taken, including an antero-posterior radiograph of the pelvis and a lateral view of the affected hip (LeBlanc et al 2014). If these are negative but a fracture is suspected, NICE guidelines recommend a magnetic resonance imaging scan (NICE 2011). A preoperative assessment should identify any correctable comorbidities to avoid a delay to surgery (NICE 2011).
Analgesia
Pain management should be initiated at presentation in all patients, irrespective of age or cognitive impairment (NICE 2011). This also helps to facilitate examination. Provided there are no contra-indications, paracetamol should be given every six hours (NICE 2011). Opioids can be added in refractory cases. In the preoperative period specifically, nerve blocks (eg: femoral) may also be used as a third-line measure or to limit the opioid dosage (NICE 2011). Notably, the use of non-steroidal anti-inflammatory drugs is discouraged due to its association with bleeding and nephrotoxicity in the elderly (Wongrakpanich et al 2018). Using extensive pain management as a substitute for early surgery should also be avoided. Analgesia use in the postoperative period follows the same general principles and is paramount to enabling patients to mobilise as part of their rehabilitation (Hida et al 2018).
Timing of surgery
In the past, hip fracture surgery was often delayed (Novack et al 2007). This led to repeated periods of starvation in physiologically compromised patients. Guidelines on hip fracture management have since been updated and now advise that patients undergo surgery as soon as possible (NHFD 2018, NICE 2011). This should ideally be on the same day as presentation or within 36h (NHFD 2018, NICE 2011). This guidance has arisen as a result of numerous studies which have shown that a short window to surgery reduces costs, morbidity and mortality. Focusing on the latter, in a study of 129,522 hip fracture patients across 151 NHS Trusts, Bottle and Aylin (2006) found that the odds ratio for death rate for patients with more than one day’s delay, compared to one day or less, was 1.27.
Achieving this target has a number of challenges. Hip fracture surgery is a significant operation and elderly patients often have multiple comorbidities that need to be managed preoperatively (Smith et al 2014). It may also be difficult to arrange the coordination of various teams: emergency departments, orthopaedic trauma services, orthogeriatricians, anaesthetic teams and operating teams to say the least. Moreover, hospitals must have appropriate theatre space available and the flexibility to adapt to variations in admission. One caveat is that this can lead to free theatre capacity in quieter periods. More recently, mainstream media has picked up on the idea of a ‘weekend effect’ in which surgeries that occur on the weekend result in poorer outcomes than those on weekdays. Currently, the literature around this topic is conflicting (Thomas et al 2014, Sheikh et al 2018).
Intra-operative considerations
Anaesthesia
At the time of writing, NICE recommends that patients be offered a choice of spinal or general anaesthetic after discussing the risks and benefits of each (NICE 2011). A number of groups have compared these two techniques. A recent study by Fields et al (2015) found that the latter is associated with a higher risk of 30-day complications (45.8% versus 50%). In addition, Van Waesberghe et al (2017) concluded that neuraxial anaesthesia is associated with a reduced in-hospital mortality and length of hospitalisation. However, the type of anaesthesia did not influence the 30-day mortality in this study. These mixed results have led many authors to conclude that there is no clear overall advantage of one type of anaesthesia over the other and large randomised studies are required (Guay et al 2016, Van Waesberghe et al 2017). The choice should therefore be made on a case-by-case basis jointly by the patient, surgeon, geriatrician and anaesthetist. It is important that this multidisciplinary discussion considers the wider clinical context as certain factors may contraindicate specific types of anaesthesia, such as the use of warfarin and spinal anaesthetic (Clinical Excellence Commission 2018).
Choice of operation
Surgery is the gold-standard treatment for hip fractures and there are a number of different operations available. This depends on the type of fracture as determined by imaging (Figure 1). According to NICE, extracapsular fractures (occurring outside the hip joint capsule) should be treated with surgical fixation due to a low likelihood of non-union (Figure 2; NICE 2011). More specifically, intertrochanteric fractures can be managed using a sliding (dynamic) hip screw, whilst subtrochanteric and reverse oblique fractures are better managed with intramedullary nailing (Figure 2).
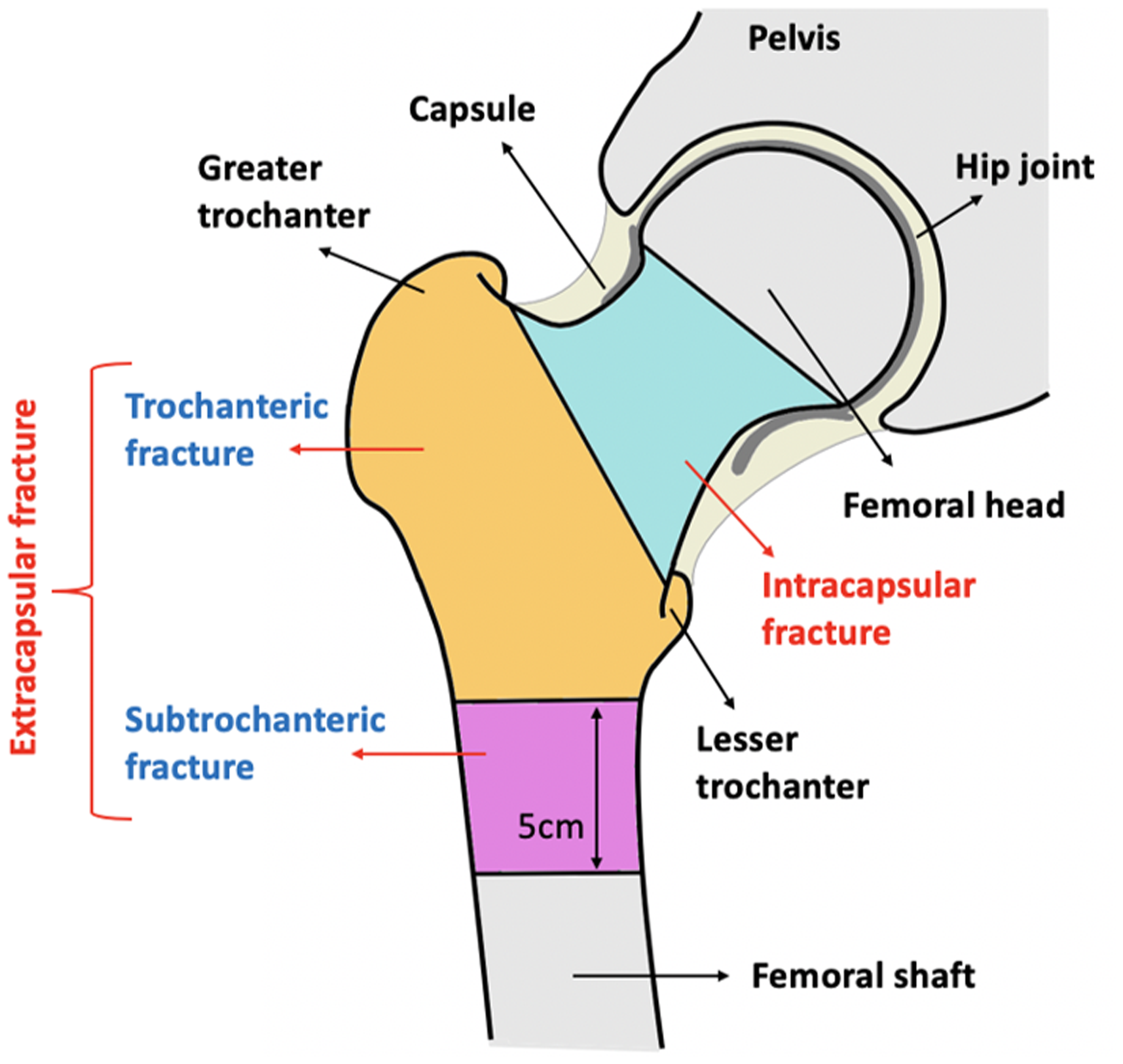
Types of hip fractures
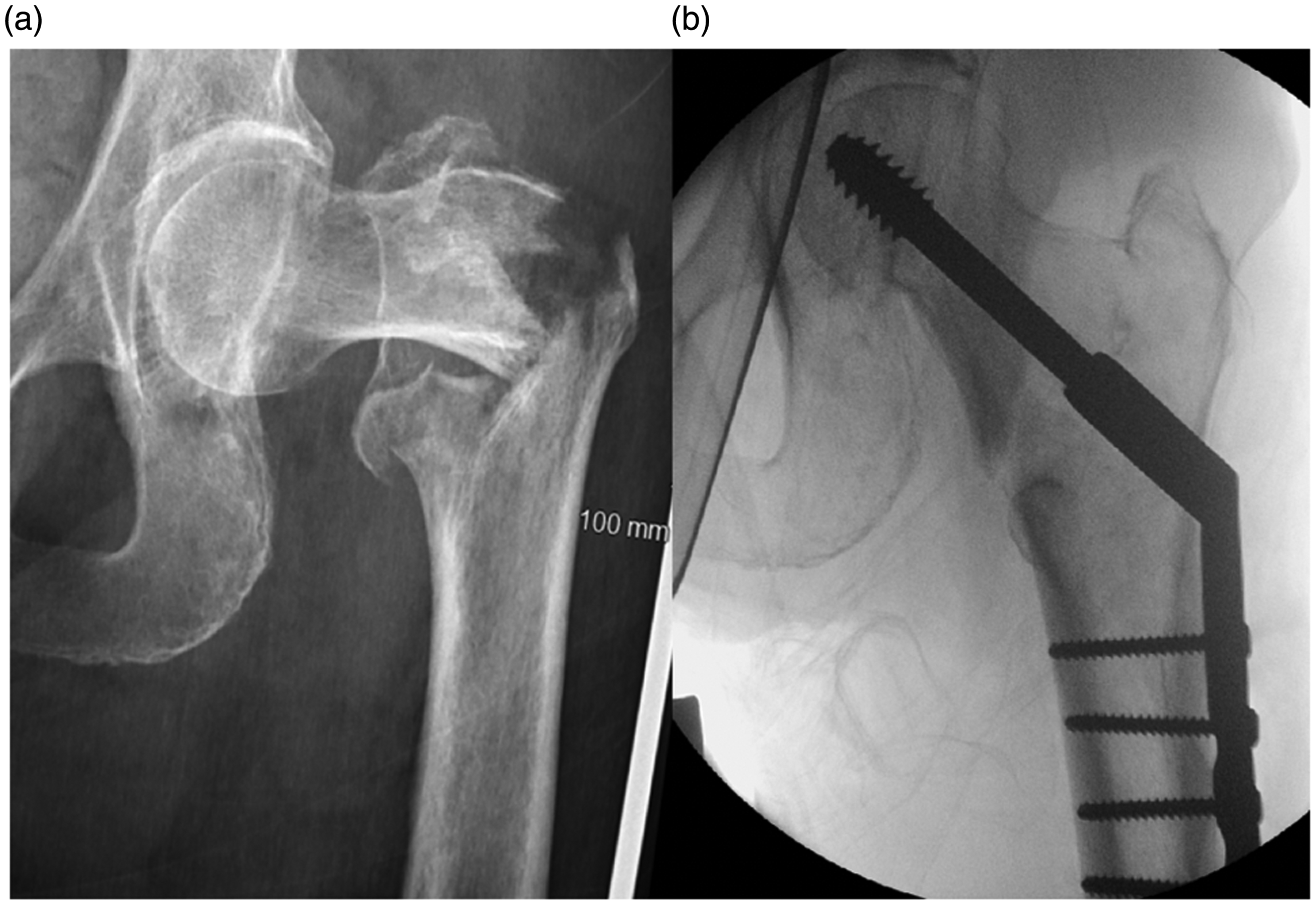
Management of an extracapsular hip fracture. Note: The patient in this figure presented with an extracapsular, intertrochanteric hip fracture. Radiograph (a) was taken preoperatively and radiograph (b) was taken intraoperatively. This patient’s fracture was fixed using dynamic hip screw fixation (shown in (b))
Intracapsular fractures (occurring inside the hip joint capsule) can also be fixed if they are non-displaced. However, displaced intracapsular fractures are generally replaced due to the risk of avascular necrosis of the femoral head (Figure 3; NICE 2017). Hemiarthroplasties used to be the preferred procedure in these cases. This was until 2011, when the NICE guidance was first updated to emphasise the role of total hip arthroplasty (THA) in patients that can mobilise independently, have no cognitive impairment and are medically fit for surgery. This has been met with some criticism and despite being emphasised again in the 2017 revision, was only employed in 31.4% of eligible patients in 2018 (NHFD 2018). In comparison, the NICE recommendation that arthroplasties should now be cemented reached 83.6% compliance in 2015 (NHFD 2016). Once the choice of operation has been made, surgeons must then decide on what surgical approach to use (Figure 4). A detailed comparison of hemiarthroplasty versus THA and the different surgical approaches are beyond the scope of this review.
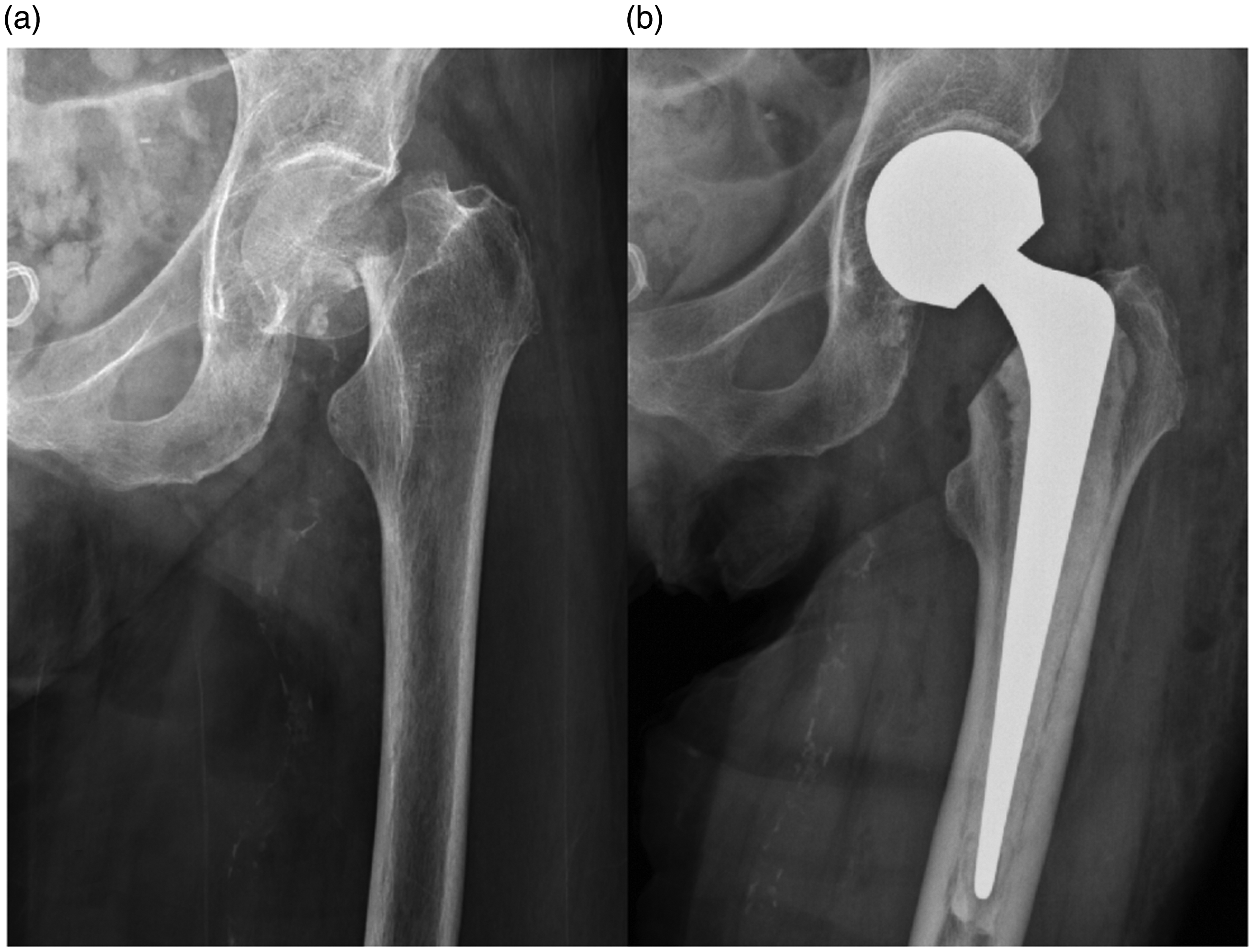
Management of an intracapsular hip fracture. Note: The patient in this figure presented with an intracapsular hip fracture. Radiograph (a) was taken preoperatively and radiograph (b) was taken postoperatively. This patient underwent a cemented hemiarthroplasty (shown in (b))
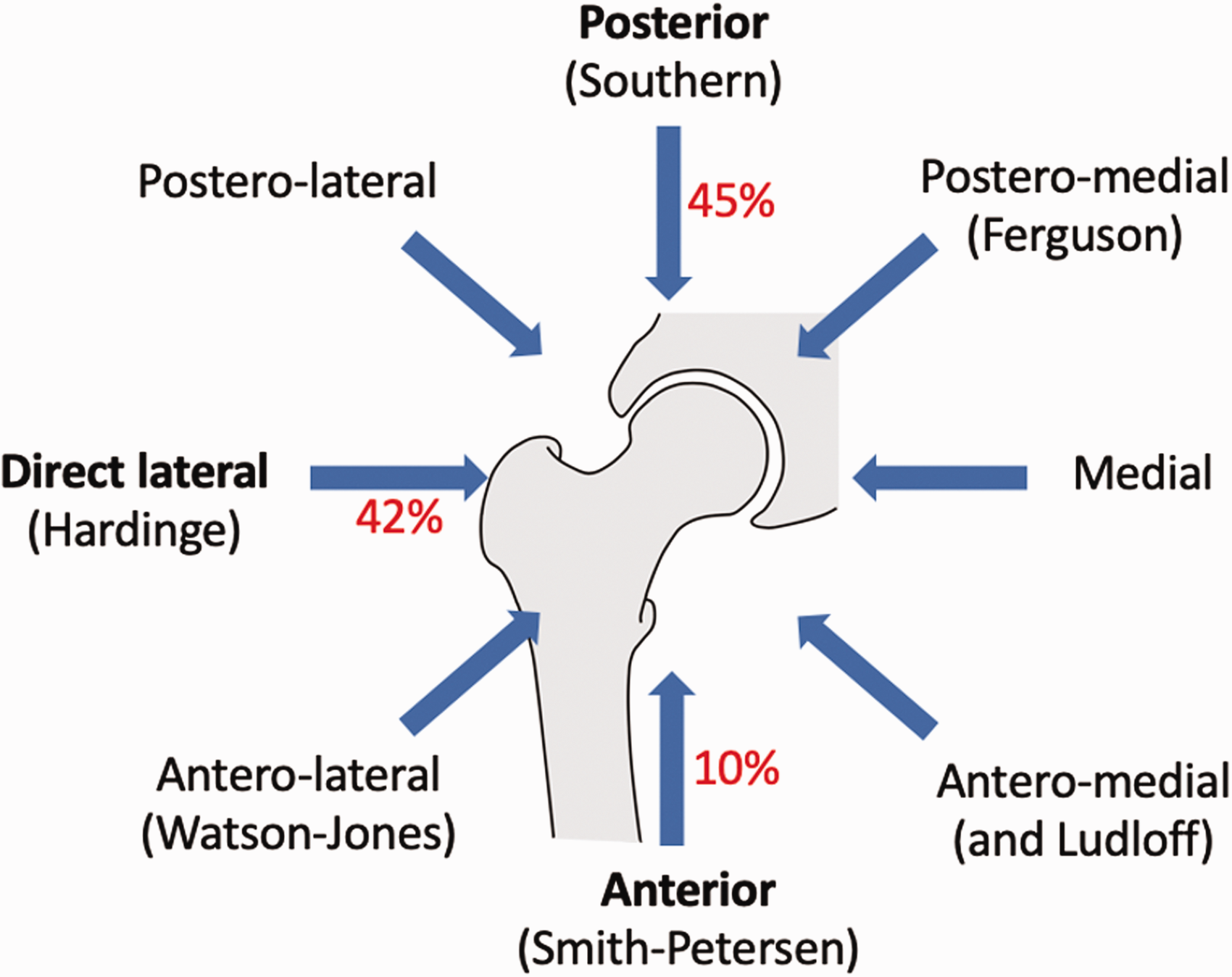
Approaches for total hip replacement.
Postoperative considerations
Physical complications
The complication rate after hip fracture surgery has been reported to be as high as 85% in some centres (Flikweert et al 2018). It is therefore important to be aware of these so that we can better prevent and treat them. Surgical complications include hip dislocations, failure of fixation, periprosthetic fractures, neurovascular injuries, deep joint infection and leg length discrepancies. Medical complications include superficial infection, deep vein thrombosis and venous thromboembolism, heart failure, postoperative confusion and/or delirium, and the development of pressure sores (White et al 2011). Medical complications are encountered more frequently than surgical complications (Flikweert et al 2018).
In the past, it was thought that hip fracture patients needed extensive bedrest and time to heal. However, studies have shown that prompt mobilisation can reduce the rate of physical complications in these cases. For instance, Oldmeadow et al (2006) found that early ambulating hip fracture patients were less likely to need high-level postoperative care (36.8 compared with 56%). This has been incorporated into recent guidelines. It is also important to realise that to achieve mobilisation one must have good postoperative pain control. This is because pain is one of the leading causes of immobility. Moreover, patients should be discharged as soon as possible. In favour of this, Nordström et al (2015) showed that in a study of 116,111 patients, an increased length of hospital stay resulted in a significant risk of death within 30 days of discharge. The NHFD recommends a return to residence within 120 days (NHFD 2018).
Psychosocial complications
In a survey of 194 women ≥75 years, 80% said that they would rather die than suffer a bad hip fracture (Salkeld et al 2000). This is largely related to the fear of losing their independence, dignity and moving into a nursing home. Hip fractures therefore represent a large source of psychosocial stress for patients, especially during the postoperative and lengthy rehabilitation periods. This may lead to depression and the literature in this area is rapidly expanding (Cristancho et al 2016). It may also result in variants of post-traumatic stress disorder, albeit infrequently (Kornfield et al 2017, Salkeld et al 2000).
It is important to be aware of these psychosocial factors for two reasons. Firstly, conditions such as depression are associated with increased morbidity and mortality in hip fracture patients (Cristancho et al 2016). This may be a direct effect, and/or due to the idea that psychosocial and physical complications can perpetuate each other. Secondly, if healthcare professionals are aware of the psychosocial complications, they are better able to identify them at an early stage, provide support and start management if necessary.
Predicting outcomes
Comorbidities
According to Barnett et al (2012), comorbidities increase with age. In this group’s sample of 1.7 million patients, 30.4% between 45 and 64 years had at least two chronic conditions, 64.9% between 65 and 84 years and more than 80% over 85 years. Similarly, elderly patients are at the greatest risk of hip fractures. Studies have shown that in these hip fracture patients, the number of comorbidities is the strongest predictor of mortality (González-Zabaleta et al 2015, Roche et al 2005). Interestingly, González-Zabaleta et al (2015) also found that after controlling for age, sex, type of fracture, surgical delay and previous fracture, comorbidity was the only indicator capable of predicting incapacity to walk. In a sample of 2448 patients, Roche et al (2005) found that the most common preoperative comorbidities were cardiovascular disease (24%), chronic obstructive airway disease (14%) and cerebrovascular disease (13%). A number of studies have corroborated these findings and identified additional factors. For example, in a systematic review of 53 studies including 544,733 participants, Smith et al (2014) found that cognitive impairment was another key factor. Other large-scale studies have argued that comorbidity indices only marginally predict long-term mortality better than chance after THA (Bülow et al 2017). It may therefore be useful to combine comorbidity with additional factors.
Tools available
There are a number of multifactor tools used to predict hip fracture outcome. The most popular of these is the American Society of Anesthesiologist (ASA) classification system (ASA 2014; Table 1). This was created as a means of estimating operative morbidity, but has since been found to strongly correlate with postoperative complications, length of hospitalisation and even total hospital costs (Kastanis et al 2016). However, it does not attempt to define the nature of the limiting disease(s). Some authors therefore prefer other measures such as the Nottingham hip fracture score (Maxwell et al 2008). This considers the following parameters: age, sex, AMTS, haemoglobin on admission, residence, comorbidities and active malignancy in the last 20 years. Alternatives such as measures of frailty and the Almelo Hip Fracture Score have been proposed but have not been as widely adopted (Nijmeijer et al 2016).
ASA gradings
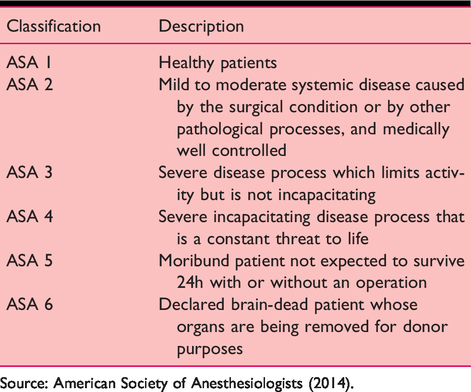
Source: American Society of Anesthesiologists (2014).
However, these tools do not yet consider social factors. Not only are these important postoperatively as described above but they may also play a role pre-fracture and in predicting outcome. In support of this, Mortimore et al (2008) found that patients who had no contact with family members pre-fracture were more than twice as likely to die within two years as those who communicated daily during the two weeks before fracture. Clearly this area is still evolving and would benefit from future review.
Conclusion
Hip fractures are associated with significant morbidity and mortality in elderly patients. This is especially concerning given the rate that our population is ageing. To better manage these patients and reduce the strain that hip fractures impose upon our healthcare system, it is important to be aware of the key perioperative factors in these patients’ care.
Key phrases
Hip fractures are associated with significant morbidity and mortality Hip fracture patients should be operated on as soon as possible and mobilise early after surgery There are physical and psychosocial complications of hip fractures There are a number of tools we can use to predict hip fracture outcome.
No competing interests declared