
Abstract
Children who are care-experienced are criminalised at disproportionately high rates. The long-term vulnerability associated with care-experience has been established in male prisoners, who have higher rates of neurodisability, substance use, and homelessness. However, it is not known whether this enduring vulnerability impacts justice-involved women in the same way. This study addressed this gap using data collected from 66 women in contact with the criminal justice system in Wales, UK. In this sample, 29% of women were care-experienced. Care-experienced women were significantly more likely than those who were not care-experienced to have a diagnosed acquired brain injury, to have another neurodisability, to have attempted suicide, and to have experienced homelessness. This study contributes a new understanding of the unique, life-course vulnerabilities associated with care-experience in justice-involved women. This group would benefit from targeted mental health support, as well as support with housing on re-integration into the community.
Keywords
Introduction
Care-experienced children (i.e. those children with experience of out-of-home care, including residential or group care homes, foster care, and kinship care) are significantly more likely to be criminalised than their peers (Department for Education, 2024). The impacts of being care-experienced are pervasive and wide-reaching, affecting outcomes well into adulthood including employment, health, education, and risk of criminalisation (Sacker et al., 2021; Testa et al., 2022). These outcomes are not inevitable but rather reflect a systemic failure to support these children. Understanding these long-term vulnerabilities associated with care-experience is critical in improving the design and implementation of rehabilitation and support services in criminal justice contexts, where care-experienced people are consistently over-represented. In a previous study, we found that adult male prisoners who were care-experienced were more likely to have experienced homelessness, have substance-use difficulties, to have been excluded from school, to have challenges with employment, and we found that they had higher rates of neurodisability (Kent et al., 2023b). To our knowledge, no study has examined the long-term implications of care-experience on women in the criminal justice system. As discussed by Gooch et al. (2022), adults in prison who are care-experienced remain invisible in the data, and without quantitative estimates of intersectional disadvantage in this group, appropriate funds and multi-agency support cannot be ring-fenced to support them. We aimed here to examine whether care-experienced women in contact with the criminal justice system had higher rates of Acquired Brain Injury (ABI), neurodisability, substance dependencies, homelessness, domestic abuse victimisation, and mental health problems.
The care-criminalisation link
Children who have been in care for at least 12 months are five times more likely to be criminalised than children in the general population in the United Kingdom (Department for Education, 2018). This pattern of disproportionate criminalisation has also been documented in other jurisdictions, including Australia (McFarlane, 2018). The reasons for this are complex, but include exposure to Adverse Childhood Experiences (ACEs), which is strongly associated with later justice system contact (Graf et al., 2021). Criminalisation increases cumulatively over the life course as the number of ACEs experienced increases (Testa et al., 2022). Many care-experienced children have been exposed to ACEs, as the most common reasons for children being taken into care include abuse, neglect, or family dysfunction (Department for Education, 2024). These vulnerabilities are further compounded by intersecting experiences of marginalisation, particularly for children from minoritised ethnic backgrounds (Baidawi, 2020; Hunter et al., 2023a).
In addition to these developmental exposures, there are situational factors relating to the care environment which increase criminalisation – for example, often police are called to residential care homes in response to behavioural incidents that would not require police intervention in the domestic home (Shaw, 2017). Care-experienced children are also more vulnerable to exploitation and manipulation by adult gangs, who coerce vulnerable children to commit crimes on their behalf in order to shield themselves from prosecution (Baidawi, 2019).
Neurodisability
Neurodisability is a key, yet significantly under-recognised factor shaping to vulnerability to criminalisation (Borschmann et al., 2020). Neurodisability is an umbrella term, encapsulating a range of congenital and acquired conditions which affect the brain and nervous system. These conditions include, but are not limited to, ABI, autism, ADHD, and learning disabilities (Morris et al., 2013). While the resultant presentations of these conditions are heterogeneous, neurodisabilities frequently impact functional problems in key developmental domains: cognition, memory, social and communication skills, attention and concentration, emotion regulation, impulse control, and physical motor skills (Patel et al., 2011). These developmental challenges can increase vulnerability to victimisation (Allely, 2015), exclusion from school (Kent et al., 2023a), and contact with the justice system (Hughes et al., 2020). Under-identification of neurodisability within the justice system, and lack of rehabilitative service provision, then leads to an increased risk of reoffending and ‘revolving door’ justice system contact, as well as harsher sentencing and more severe disciplinary sanctions in custodial settings (Baldry et al., 2018).
Approximately half of adult prisoners have an ABI (Hunter et al., 2023b), compared to approximately 12% of adults in the general population (Frost et al., 2013). Similarly, approximately 5% of adults in prison have a learning disability (Ali et al., 2016), compared to 1% of adults in the general population (McKenzie et al., 2016). Yet despite this, people with neurodisability are often under-identified and not properly supported in criminal justice contexts, and they consistently have higher rates of mental health difficulties and substance-use problems in prisons (McCarthy et al., 2016; O’Rourke et al., 2016). Acquired Brain Injury, in particular, is linked to suicidality (Ineson et al., 2023). It is known that among crossover children (who come into contact with both child welfare and justice systems), rates of neurodisability are particularly high (Baidawi and Piquero, 2021). In our previous work, we also found that care-experienced men in prison had significantly higher rates of neurodisability compared to their non-care-experienced peers (Kent et al., 2023b). However, it remains unclear whether similar patterns are observed among women.
Gendered vulnerability
The relationship between care-experience, neurodisability, and criminal justice contact is shaped by gender. Feminist criminological theories have long emphasised that women’s pathways into the justice system differ from men’s, often rooted in histories of trauma, coercive control, and structural marginalisation (Gelsthorpe, 2020; Phillips et al., 2022). This disadvantage is often also intergenerational, as having an incarcerated parent has pervasive impacts on the child’s psychosocial outcomes, which are amplified if the incarcerated parent is the mother (Murray and Farrington, 2008). Maternal imprisonment significantly disrupts family life and increases the likelihood that children will have to move out of the home, often being placed into kinship or state care (Booth, 2017), leading to further instability and compounding cycles of disadvantage.
Girls in care face particularly heightened vulnerabilities, including sexual exploitation, gang involvement, and grooming (Shaw et al., 2024). This context can be stigmatising, contributing towards discriminatory and distorted perceptions of victimhood of girls in care, meaning that critical moments for intervention are missed (Shaw et al., 2024). Once inside prisons, women are particularly vulnerable to suicidality and self-harm. In a study of 24 European countries, prisoner suicide rates were estimated to be ten times higher than in the general population for women (rates were between three and eight times higher than the general population for males) (Fazel et al., 2017). The annual prevalence of self-harm in prisons is estimated at 5%–6% of adult male prisoners and 20%–24% of adult women in prison (Hawton et al., 2014). The most recent available statistics from the Ministry of Justice indicate that the incidence of self-harm in women’s prisons is currently extremely high, at 5906 incidents of self-harm per 1000 prisoners, and that rates are continuing to increase, rising by 6% in the 12 months to March 2025 compared with the previous year (Ministry of Justice, 2025). Upon release, women also often face additional psychosocial disadvantage – nearly half are released into homelessness (Prison Reform Trust, 2022).
Women in contact with the criminal justice system frequently also have extensive histories of domestic abuse victimisation, which are intertwined with brain injury. A study of women in Scottish prisons found that 78% of women had experienced a significant head injury (McMillan et al., 2021), and most brain injuries in this study were sustained through domestic abuse. In domestic abuse victimisation, a high proportion of physical assaults are targeted at the head and neck (including through non-fatal strangulation, which can lead to anoxic or hypoxic injuries) (Valera and Kucyi, 2017). Acquired Brain Injury therefore appears to disproportionately affect women in the justice system and may follow a distinct pathway, linked to gender-based violence. For this reason, in the present study we examined ABI separately from other forms of neurodisability. These patterns demand a gender-informed approach to understanding the intersection of care-experience, neurodisability, and justice system contact.
Theoretical framework
This study is grounded in theories of cumulative disadvantage and the stress proliferation model, which explain how early adversity and marginalisation compound over time to produce entrenched disadvantage across the life course. Cumulative disadvantage theory (Dannefer, 2003; Dannefer and Han, 2021) posits that inequalities accumulate across the life course, with early structural disadvantage, such as entry into the care system, increasing the likelihood of subsequent disadvantage. For care-experienced children, exposure to trauma and instability early in life heighten vulnerability to later difficulties, including poor mental health, substance use, homelessness, and contact with the criminal justice system. These adversities rarely occur in isolation: rather, they cluster, accumulate, and interact over time, leading to increasingly limited life chances and entrenched psychosocial need in adulthood. Crucially, these adversities are not simply individual in origin, but are moulded and reinforced by systemic factors, including under-resourced care environments and inadequate access to support services (Dannefer and Han, 2021). The stress proliferation model (Pearlin et al., 2005) adds to this by showing how an initial stressor (such as childhood trauma or removal from the family home into care) can generate secondary stressors across domains, including poor mental health, unstable housing, and relationship breakdown. Essentially, we can understand that stress begets stress: children who have experienced adversity in early life are more vulnerable to cascades of further adversity. Among women in the justice system, these stressors are frequently gendered, shaped by experiences of domestic abuse, coercive control, and social stigma (Bartlett and Hollins, 2018; McGinley and McMillan, 2019).
The current study
Emerging evidence indicates that care-experience is associated with lifelong cumulative disadvantage, higher rates of neurodisability, and poorer outcomes across substance use, homelessness, disability, and poor educational outcomes in male prisoners (Kent et al., 2023b). However, it is not known whether care-experience is associated with these enduring vulnerabilities in justice-involved women. This study aims to address this gap, using data collected from women in contact with the criminal justice system in Wales, UK.
Our research question is: Are there significant differences in psychosocial needs and outcomes (including but not limited to homelessness, substance use, and neurodisability) between care-experienced and non-care-experienced women in contact with the criminal justice system?
It is important to note at this stage that our data are limited by their cross-sectional nature, and, like much research in this field, may also be impacted by unobserved confounding through variables not captured here (such as socioeconomic status). We therefore do not aim to infer causality in these findings. Instead, we aim to examine comorbidities in the population of justice-involved women who are care-experienced, compared to those who are not care-experienced.
Method
Ethics
Ethical approval for this study was granted by HMPPS NRC (His Majesty’s Prison and Probation Service National Research Committee) [application no. 2023-147]. The research was supported by Brainkind’s research group, the institutional review board overseeing research governance and ethics within the organisation.
Participants and procedure
This study involved secondary analysis of data originally collected for the Brainkind Complex Lives Report (Brainkind, 2024). In brief, the procedure was as follows: 70 women in contact with the criminal justice system in Wales (UK) were recruited from a range of settings, including prison, probation, and early-intervention community settings. Data from four women (5.7% of the sample) were removed from the study due to incomplete responses and potentially re-identifiable answers. In line with ethical requirements, these responses were removed from the analysis. Given the small proportion of missingness, no further imputation or adjustment procedures were undertaken (Kang, 2013). The final sample therefore comprised 66 women, of whom 41 (62.1%) were in prison, 21 (31.8%) were on probation, and 4 (6.1%) were engaged in early-intervention community settings.
Data collection was carried out through semi-structured interviews, supplemented by a series of validated self-report measures. The interviews explored a broad range of topics, including demographic characteristics, experiences of the care system, current and past mental health difficulties (such as suicidality, self-harm, and substance use), and histories of brain injury. Brain injury discussions were prompted using the Brain Injury Screening Index (BISI), described below. Educational background and other life experiences were also discussed, although several areas fell outside the scope of the current analysis. Interviews lasted approximately 60 minutes and were conducted in private settings.
Variables
Demographics
Age and ethnicity were treated as demographic variables and compared between care-experienced and non-care-experienced groups to assess whether any group differences in psychosocial outcomes could be attributed to underlying demographic variation. Age was reported as a continuous variable. Ethnicity was dichotomised into those who were White Welsh or British, and Other. This was due to the high proportion of White British/Welsh women in the sample. Disaggregation into more detailed categories was not appropriate given the very small numbers in other groups, which limited statistical power and raised concerns about potential re-identification.
Care experience
Women were asked during the interviews about their interactions with social care systems. This included asking whether they had ever experienced being in care as a child, whether they had any children themselves, and if so, whether their children had ever been taken into care (including kinship care). All of these variables were dichotomised (e.g. for care-experience, Yes = 1, No = 0).
Homelessness
Women were asked ‘have you experienced homelessness or stayed in hostels?’ Their responses were dichotomised, where 1 = Yes, 0 = No.
Education level
Self-reported highest level of educational qualification was categorised into three mutually exclusive groups:
(1) No formal qualifications
(2) Foundational qualifications, including GCSEs (typically taken at age 15–16 in the United Kingdom) and National Vocational Qualifications (NVQs)
(3) Higher-level qualifications, including AS- or A-Levels (typically taken at age 17–18) and higher education degrees.
Brain injury
Participants were asked whether they had ever received a formal diagnosis of a brain injury (e.g. by a doctor or in hospital). If they reported a brain injury, they were asked to expand on the injury and how the diagnosis was made. Women were also asked whether they had ever experienced non-fatal strangulation or been held in a way where they felt like they could not breathe, as this is an often under-recognised cause of hypoxic and anoxic brain injury in women who have experienced domestic abuse (Monahan et al., 2022). In addition, all participants were screened for possible brain injury using the BISI, an 11-item screening tool developed by Brainkind to identify lifetime exposure to events that may be indicative of ABI. The BISI is freely available online 1 and has been validated for use with women in criminal justice settings (O’Sullivan et al., 2019). The 11 items were scored in accordance with the BISI guidance, with negative screens indicated by scores between 0 and 4, and positive screens indicated by scores of 5 or more. Three binary variables were created:
(1) Diagnosed brain injury, based on self-reported formal diagnosis;
(2) Suspected brain injury, based on a positive BISI screen;
(3) Experienced non-fatal strangulation, based on self-report.
These groups were not mutually exclusive. All participants with a diagnosis also screened positive on the BISI, therefore, the suspected brain injury group includes both diagnosed and undiagnosed cases.
Participants also completed the Rivermead Post-Concussion Symptoms Questionnaire. This is a validated 16-item tool which captures the impact of post-concussion symptoms (Maruta et al., 2018). Each symptom is scored on an ordinal scale from 0 to 4, where 0 = never experienced at all, and 4 = a severe problem. Total scores were treated continuously. Example symptoms include dizziness and headaches.
Substance dependency
Responses relating to current or previous drug or alcohol dependency and prescription of methadone for opioid use disorders were dichotomised where 1 = Yes, 0 = No.
Physical health conditions
Self-report of any long-term disabilities or medical conditions were dichotomised, 1 = Yes, 0 = No.
Other neurodisability
Self-report of any other neurodisabilities or neurodivergent conditions, including ADHD, Autism, and Learning Disabilities, were dichotomised (1 = Yes, 0 = No).
Domestic abuse
Women were asked whether they had ever been a victim of domestic abuse. Responses were dichotomised (1 = Yes, 0 = No).
Suicidality and self-harm
Women were asked whether they had ever thought about ending their lives (suicidal ideation, 1 = Yes, 0 = No), whether they had ever attempted suicide (suicide attempt 1 = Yes, 0 = No), and then were asked to expand on this as appropriate. Where more than one attempt was disclosed (multiple attempts), this was also dichotomised. They were also asked whether they had self-harmed, either currently or in the past (1 = Yes, 0 = No). Where suicidality or self-harm was disclosed, researchers initiated further conversations about safety with the woman’s support worker, to ensure support could be put into place where appropriate.
Anger
The Dimensions of Anger Reactions (DAR-5) questionnaire was used to capture feelings of anger (Phoenix Australia, 2022). This is a five-item questionnaire, and respondents rate the frequency of each item over the past 4 weeks, using a Likert-type scale from 1 (none or almost none of the time) to 5 (all or almost all of the time). Items are summed to provide a total severity score (range 5–25) and were treated continuously. Higher scores indicate higher levels of anger. Example items include ‘My anger prevented me from getting along with people as well as I’d have liked to’. The DAR-5 has been validated in samples who have experienced trauma (Forbes et al., 2014).
Anxiety and depression
The Patient Health Questionnaire-4 (PHQ-4) was selected as a brief, validated measure of anxiety and depression (Löwe et al., 2010). This is a four-item measure, where respondents rate the frequency of each item over the past 2 weeks on a Likert-type scale from 0 (not at all) to 3 (nearly every day). Scores were treated continuously. Example items include ‘Feeling down, depressed, or hopeless’.
Post-traumatic stress
All women completed the Trauma Screening Questionnaire (TSQ), a validated 10-item measure of the impact of traumatic events (Walters et al., 2007). Each question is scored as 1 or 0, and total scores for this measure were treated continuously. Example items include ‘upsetting thoughts or memories about the event have come into your mind against your will’.
Analysis
All data were analysed quantitatively, including variables derived from semi-structured interviews. Although interviews were used to facilitate a trauma-informed and relational approach to data collection, the primary aim was to obtain structured information on key life experiences. This approach allowed for sensitive engagement with participants while creating data suitable for group-level comparisons and quantifying patterns across the sample. Analyses were conducted using R statistical software (version 4.5.0) (R Core Team, 2021). Statistical significance was set at p < .05.
Chi-square tests of independence were used to compare care-experienced women with non-care-experienced women on categorical or binary variables, with Cramér’s V effect sizes. Conventionally, Cramér’s V effect sizes are interpreted as follows: V > 0.1 indicates a small effect size, V > 0.3 indicates a medium effect size, and V > 0.5 indicates a large effect size (Cramér, 1946). To examine whether the children of care-experienced mothers in the criminal justice system were more likely to also be in care, we conducted a separate chi-square test of independence in a smaller subset of the sample (those with children). For continuous variables, group differences were assessed using Welch’s t-tests, with Cohen’s d used to estimate effect sizes. Welch’s t-test was used due to unequal sample sizes and to account for potential differences in variance between groups. According to Cohen (1992), d > 0.2 is considered a small effect, d > 0.4 medium, and d > 0.6 large.
Notably however, emerging evidence indicates that these thresholds for effect sizes may be too conservative, and may underestimate meaningful effects particularly in the context of social science research (Correll et al., 2020). Given the homogeneity of the women’s prison population and the structural disadvantages faced by both groups, even small differences may hold practical significance. Accordingly, we discuss the implications of our findings with context in mind.
Results
Nineteen women (28.8% of the sample) reported being care-experienced. Table 1 illustrates a comparison of those women who were care-experienced, compared to those who were not. We found that adult justice-involved women who were care-experienced were significantly more likely to have experienced homelessness (89.5% of care-experienced women compared to 63.8% of those who were not care-experienced), more likely to have a diagnosed ABI (26.3% compared with 4.3%), more likely to have another neurodisability, including autism, ADHD, and learning disabilities, (78.9% compared with 42.6%), and more likely to have attempted suicide (100% compared with 55.3%). Care-experienced women were also significantly less likely to have achieved a higher-level education qualification (5.3% compared with 27.7%). Cramér’s V effect sizes for these comparisons ranged from 0.25 to 0.43 – small to medium effects. Women who were care-experienced also scored more highly on a measure of anger (mean score of 17.7 compared with 12.7). Cohen’s d effect size for this comparison was -0.82 (a large effect size). There were no significant differences between the groups by age or ethnicity, or on any other measured variables.
Sample description, including comparison of care-experienced versus non-care-experienced women, including chi-square and Welch’s t-test statistics with effect sizes.
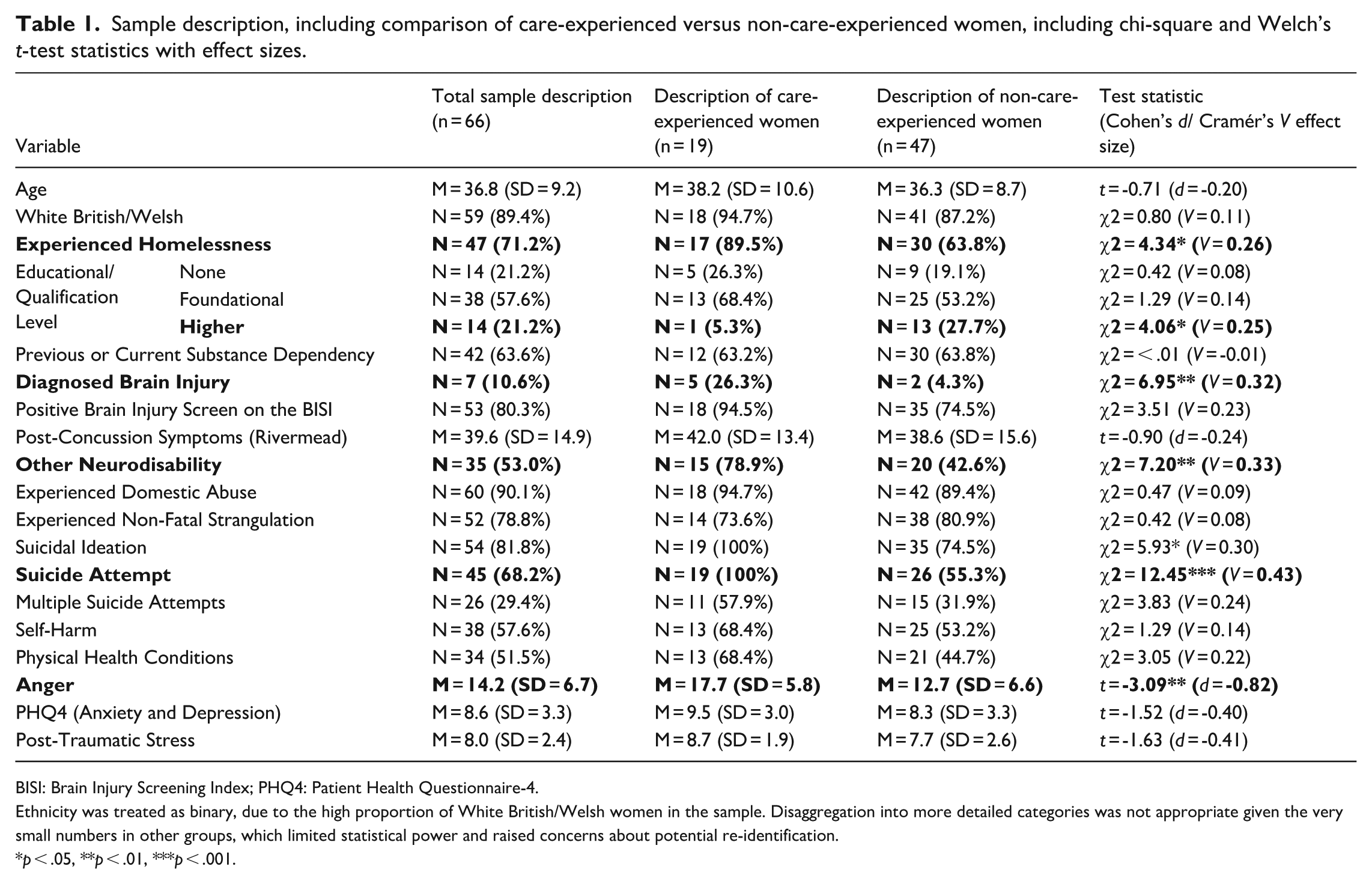
BISI: Brain Injury Screening Index; PHQ4: Patient Health Questionnaire-4.
Ethnicity was treated as binary, due to the high proportion of White British/Welsh women in the sample. Disaggregation into more detailed categories was not appropriate given the very small numbers in other groups, which limited statistical power and raised concerns about potential re-identification.
p < .05, **p < .01, ***p < .001.
In addition, most women in the sample (56 out of 66; 84.8%) reported having children. Of these, 38 women (67.8%) had experienced their child being taken into care. This high rate of children in care was observed across the sample and did not differ significantly by the mother’s care-experience status (χ² = 0.52, p = .47, V = 0.10).
Discussion
In this study, 29% of women in contact with the criminal justice system were care-experienced. It is difficult to find comparable general-population statistics for adult women in the United Kingdom, however approximately 70 children per 10,000 (0.7%) are in care, indicating significant over-representation among women in the criminal justice system. The vast majority of women in our sample (90%) had experienced domestic abuse victimisation, which is consistent with other studies indicating that justice-involved women have frequently experienced victimisation across the life course (McMillan et al., 2021; Villacampa and Torres, 2015). We also found evidence of the intergenerational impact of maternal incarceration as discussed by Booth (2017), as 68% of women who had children reported that their children were in care, either through kinship care or more formal social care. Justice-involved populations, particularly women, are relatively homogeneous in terms of poor life outcomes. Despite this, we found meaningful differences between care-experienced and non-care-experienced women.
For example, a significantly higher proportion of care-experienced women had a formally diagnosed brain injury, and had other neurodisabilities (including autism, ADHD, and learning disabilities). The contextual interview data indicated that these diagnosed brain injuries were quite severe, necessitating hospital treatment, and several women reported having been in a coma. Care-experienced women in the justice system are therefore likely to have more complex needs and ongoing disability associated with moderate/severe brain injury (Tate et al., 2020).
This finding must be situated within a context of very high levels of self-reported brain injury across the sample as a whole, with 86% of women screening positive for a history indicative of brain injury on the BISI. Previous studies have found similarly high rates of brain injury among women in prison, which frequently result from domestic abuse (McMillan et al., 2021). This pattern is reflected in this sample given the high rates of domestic abuse victimisation (90%) and non-fatal strangulation (78%). Non-fatal strangulation is a well-established cause of anoxic or hypoxic brain injury which is often overlooked and underdiagnosed (Monahan et al., 2022). Although recent media and public health campaigns have increasingly (and importantly) drawn attention to the impact of non-fatal strangulation in the context of unsafe sexual practices, contextual interview data in the present study indicated that non-fatal strangulation was used as a form of violence within extremely coercive relationships. This aligns with a substantial body of literature framing non-fatal strangulation as an extreme and potentially lethal form of interpersonal violence, closely linked to coercive control and death threats (see Stansfield and Williams, 2018 for further discussion). Improved awareness of the severity and impact of non-fatal strangulation in this context, particularly among health and justice professionals, could help to improve support for justice-involved women.
It is therefore essential that screening for neurodisability is in place in justice system contexts, to understand how the functional impact of neurodisability (including difficulties with attention, memory, and emotional regulation) might impact engagement with education and rehabilitation programmes. Training for criminal justice staff is also critically important, as misconceptions about brain injury and neurodisability can result in poorer rehabilitative outcomes and harsher sentencing (Baldry et al., 2018; O’Rourke et al., 2018), and create barriers to accessing justice (Brookbanks et al., 2022). The systemic under-recognition of, and lack of support for, brain injury in the justice system contributes to entrenched disadvantage for vulnerable women, compounding adversity and limiting access to meaningful rehabilitation. This reflects a pattern of cumulative disadvantage, whereby unaddressed needs associated with neurodisability intersect with trauma, poverty, and systemic exclusion across the life course, progressively narrowing life chances and entrenching contact with the criminal justice system.
The high rates of suicide attempts reported by this sample warrant particular emphasis. All the care-experienced women had attempted suicide at some point in their lives, compared with just over half of the women who were not care-experienced. This represents an exceptionally high level of suicidality, even within a population already known to be at elevated risk. This is therefore a group clearly exhibiting high levels of emotional distress, shaped by a history of early adversity, unmet need, and systemic neglect across the life course (Hughes et al., 2017). The elevated rates of suicidality among care-experienced women can be understood within a life course framework, where the accumulation of trauma, neurodisability, and institutional exclusion compounds over time, heightening vulnerability and undermining opportunities for recovery and resilience. The elevated rates of brain injury among care-experienced women likely contribute to this increased suicidality, given the well-established association between brain injury and suicidal behaviour (Fazel et al., 2014).
This finding must be considered within the context of inadequate mental health services in UK prisons, which currently are drastically under-funded, and not meeting the complex needs of prison populations. A report from the House of Commons Justice Committee found that just 10% of UK prisoners are receiving any intervention for mental health, while an estimated 70% are in need of interventions (House of Commons Justice Committee, 2021). An analysis of unannounced prison inspection reports identified that low staffing, delays to service access, a lack of appropriate interventions, and limited access to supervision, training, and opportunities for reflective practice are all systemic challenges in prison mental health services (Patel et al., 2018). Against this backdrop of constrained service provision, the extreme suicidality among all justice-involved women, but particularly those who are care-experienced, represents an urgent unmet need, and indicates that this group should be prioritised for trauma-informed mental health interventions.
Care-experienced women were also significantly more likely to have experienced homelessness and reported markedly higher levels of anger. These findings point to the layered effects of structural and psychological marginalisation. Homelessness represents both a consequence and a driver of cumulative disadvantage, often arising from disrupted early attachments, housing instability post-care, and limited social and financial support networks (Paulsen and Thoresen, 2023). Care-experienced women in this sample were also significantly less likely to hold higher-level educational qualifications, consistent with evidence that school exclusion and disrupted learning are common among children in care (Jay and Mc Grath-Lone, 2019). This educational marginalisation likely contributes to limited employment opportunities and economic precarity in adulthood, further compounding their disadvantage. Elevated anger scores may reflect chronic exposure to trauma, disrupted attachments, and persistent invalidation across childhood and adolescence. For care-experienced individuals, anger can emerge as a response to the institutional environment of residential care, and a lack of trust in professionals who have control over that individual’s life (Day, 2017). These findings highlight the importance of justice interventions that recognise and respond to the intersecting forms of disadvantage and complexity that shape women’s lived experiences.
We did not observe significant group differences in the prevalence of domestic abuse, which is likely due to the very high rates across the entire sample (90.1%). Similarly, rates of suspected brain injury, as screened by the BISI, were comparable between groups, with 86.4% of the overall sample screening positive for a history indicative of brain injury, reflecting the homogeneity and high level of need within this population. Of note, lifetime substance dependency was also similar among care-experienced and non-care-experienced women. This contrasts with our previous findings in male prisoners, where care-experienced men were significantly more likely to report substance-use problems (Kent et al., 2023b).
One possible explanation exists for this through gendered patterns of trauma responses and coping mechanisms. While both men and women who are exposed to traumatic experiences are at an elevated risk of substance-use dependencies (Rogers et al., 2021), for men, physical abuse and exposure to violence (common among care-experienced populations) are particularly predictive of later substance misuse (Danielson et al., 2009). In contrast, for women, sexual assault appears to be a more salient risk factor, and substance dependencies may be more strongly linked to specific experiences of interpersonal trauma (Danielson et al., 2009). These gendered trajectories may explain why substance use is disproportionately elevated among care-experienced men, but more evenly distributed among justice-involved women – where sexual abuse is highly prevalent, impacting an estimated 56%–82% of women (Karlsson and Zielinski, 2020). Indeed, 90.1% of women in this study had experienced domestic abuse, which often co-occurs with sexual violence (Blasdell, 2021). In addition, as with domestic abuse and suspected brain injury, high rates of substance dependency in the female prison population overall may mask between-group differences, creating a ceiling effect.
Implications
Our findings indicate that a high proportion of justice-involved women are care-experienced, and that care-experienced women in the criminal justice system are a particularly vulnerable group who have experienced intersectional, cumulative disadvantage throughout the life course. The fact that all care-experienced women in our sample had attempted suicide highlights an urgent need for accessible mental health support, which should be sensitive to the needs of those who may have had previous negative experiences of seeking support, and flexible to meet the needs of those who require adjustments to interventions to make them more accessible (e.g. due to cognitive difficulties following brain injury). Neurodisability was also more prevalent in this group, suggesting a need for screening, specialist input, and accessible rehabilitation, with a particular emphasis on gendered pathways for support for women who have experienced ABI because of domestic abuse. Neurodisability must also be recognised as an accessibility issue, with implications for the design of education, restorative justice, and community-based programmes. Care-experienced women may require additional support with housing and education, given their lower qualification levels and often limited family support. While recent policy has focused on preventing the criminalisation of care-experienced children (Department for Education Home Office and Ministry of Justice, 2018), greater attention is needed for those who have aged out of care and are now in the adult justice system. Targeted investment in this group could help break cycles of systemic exclusion and reduce long-term justice system contact.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the data were based on self-report measures, which are reliant on participants’ autobiographical memory and willingness to disclose sensitive information. While Schofield et al. (2011) found people in prison to be reliable at self-reporting brain injury when compared with medical records, there is a possibility that other biographical information may not have been reported accurately. We were unable to corroborate diagnoses or experiences through medical or administrative records, but future research should look to include this.
Our decision to dichotomise the care-experience variable was necessary due to the relatively small sample size, which may have limited our ability to detect more subtle group differences. However, future research with larger samples could benefit from incorporating more detailed information about the nature and duration of care-experiences (e.g. kinship care versus residential placements), which may help to elucidate more nuanced patterns of vulnerability.
A further limitation concerns the role of custodial sentences themselves as a potentially confounding exposure. Women’s experiences of imprisonment are known to have independent and detrimental effects on mental and physical health (Douglas et al., 2009), as well as ‘collateral consequences’ affecting housing stability and employment, for example (Bohmert et al., 2018). Imprisonment also severs connections to family and local community support networks, further perpetuating cyclical contact with the justice system (Goulding, 2004). These harms may be particularly acute for women in prison, who often serve short sentences – as discussed by the Prison Reform Trust (2022), 63% of women who started a sentence in 2021 would serve sentences of 12 months or less, which means that they experience all the harm of imprisonment without meaningful time to be offered access to rehabilitation and support services. We did not have data available on previous experiences of imprisonment for women in our sample (for example, whether those recruited from probation services or in community settings had ever been imprisoned), nor any data on length/number of custodial sentences. Therefore, it was not possible to disentangle the effects of care experience from any potentially confounding effects of imprisonment.
The cross-sectional nature of the study also significantly limits the conclusions which can be drawn. Future research should utilise longitudinal datasets to establish temporal order between adverse events in childhood, timing of care experience, trajectories through education, and timing of criminal justice contact. This would strengthen the inferences about the enduring harms of care-experience that can be drawn, over and above the influence of other early adverse experiences. Finally, while the predominantly White British sample reflects the demographics of women in Wales (Office for National Statistics, 2022), the findings may not be generalisable to other regions of the United Kingdom or to more ethnically diverse populations internationally.
Conclusion
This study highlights the significant over-representation and heightened vulnerability of care-experienced women in the criminal justice system. Our findings point to complex, cumulative disadvantage across the life course in domains including neurodisability, mental health, education, and housing. Furthermore, they highlight that current service delivery approaches often fail to address these intersecting challenges, preventing women from accessing the health and social care interventions they need and placing them at greater risk of entering the criminal justice system.
These intersecting challenges illustrate an urgent need for accessible, trauma-informed, and gender responsive approaches to supporting women, particularly those that are care-experienced and/or live in the context of domestic abuse. Key to the development of such services is improved awareness among health and social care professionals of the multiple disadvantages these women face and how normal service delivery can be adapted to meet their needs (e.g. how to adapt talking therapy for someone with a brain injury). These interventions could most effectively be delivered through community-based responses, rather than through custodial sentences, so diversionary approaches are also implicated. Without flexible service delivery, with interventions adjusted to accommodate for the difficulties they face, care-experienced women risk continued marginalisation and cyclical justice system contact. Given the known detrimental effects of custodial sentences on women’s mental health, family life, and the potential to compound cycles of disadvantage, addressing the enduring vulnerability associated with care-experience is not only a matter of justice, but also of social responsibility.
Footnotes
Acknowledgements
We would like to thank Sara de Silva Ramos for her valuable contributions and support during the preparation of this article. We would also like to thank Sarah Turner, Sara de Silva Ramos, and Thea Arch for their contributions to the original Complex Lives study. Finally, we would like to thank the women who participated in this research.
Ethical Considerations
Ethical approval for this study was granted by HMPPS NRC (His Majesty’s Prison and Probation Service National Research Committee) [application no. 2023-147]. The research was supported by Brainkind’s research group, the institutional review board overseeing research governance and ethics within the organisation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Complex Lives study was funded by the Women’s Justice Blueprint and the Criminal Justice Board for Wales. The funders had no role in the study design, data collection, analysis, interpretation, or the decision to submit this article for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study contain sensitive information and a risk of participant re-identification. As such, they are not publicly available for re-use. Access may be considered on a case-by-case basis, subject to appropriate ethical and data governance approvals. Contact
Open Badges Statement
For the purpose of open access, the authors have applied a ‘Creative Commons Attribution (CC BY) license to any Author Accepted Manuscript version arising’.