
Abstract
A cultural initiative, ‘Becoming Trauma-Informed’, was introduced into prisons in England and Wales from 2015 based on the work of American clinical psychologist, Dr Stephanie Covington, and as part of a more general trend towards the recognition and treatment of trauma-related conditions in the community and in mental health settings. Becoming trauma-informed training for Prison Officers in England and Wales was carried out in all 12 women’s prisons during 2015–2017 and began in the long-term high-secure male estate from May 2018. The becoming trauma-informed work is based on considerable expertise, and a deep commitment by experts and practitioners to the development of trauma-informed practice. The authors welcome this ‘trauma-turn’ in thinking and practice and describe an extended pilot attempt to operationalise and measure its impact on the prison experience. The results were disappointing. By highlighting challenges, and exploring meaning-in-practice, we hope to contribute to the improvement of these initiatives.
A cultural initiative, ‘Becoming Trauma-Informed’ (BTI), was introduced into prisons in England and Wales (and elsewhere) from 2015 based on the work of American clinical psychologist, Dr Stephanie Covington (2016) and as part of a more general trend towards the recognition and treatment of trauma-related conditions in the community and in mental health settings. Research on the impact of trauma has not only increased significantly in the fields of psychology, psychiatry and neuroscience but also in the practice-based fields of social care, education and criminal justice (Becker- Blease, 2017). King (2017) describes trauma as an individual’s experience of an event that considerably negatively affects their ability to cope with or recover from it, evoking emotions such as fear, hopelessness and a sense of violation. Randall and Haskell (2013) differentiate between acute (time-limited), chronic (multiple or ongoing) or complex (a mixture) trauma, all of which can have long-lasting effects, particularly when experienced during developmental years. Trauma can affect people from all backgrounds, but there is a strong correlation between levels of marginalisation and risk of exposure. Prison populations are especially likely to include disproportionate numbers of individuals exposed to trauma from a young age (Crisanti and Frueh, 2011).
Covington (2003) defines trauma-informed services as ‘services that have been created to provide assistance for problems other than trauma, but in which all practitioners have a shared knowledge base and/or core understanding about trauma resulting from violence’ (p. 95). Trauma-informed training interventions promote awareness of the significance of trauma in an individual’s everyday life in order to support recovery (King, 2017; Miller and Najavits, 2012). This is important in criminal justice settings where inadvertent re-traumatisation through seemingly unthinking staff or poor cultural practices may be more likely than support for recovery (Covington, 2003), particularly among female prisoners (e.g. Eastel, 2001).
BTI training for Prison Officers in England and Wales was carried out in all 12 women’s prisons during 2015–2017 and began in the long-term high-secure male estate from May 2018. The BTI work is based on considerable expertise (see Covington, 2008) and is supported financially by a charitable organisation, One Small Thing, led and funded by prison philanthropist, Lady Edwina Grosvenor.
1
The aim of this organisation is, cultural change in the criminal justice system: to shift the question away from ‘what’s wrong with them?’, towards ‘what happened to them?’ . . . We aim to humanise the process for individuals caught up in a cycle of crime by training front line staff and those who are caught up in the Justice Saystem to understand trauma and its impact on both a systemic and an individual level. We support staff to ensure the systems within which they work run concurrently and complement the process of self–discovery. Our ultimate aim is . . . to transform cultures and systems and – crucially – to change people’s lives for the better, one small thing at a time. (Website)
The training modules delivered in prisons in England and Wales are based on Covington’s model and include courses on, ‘Becoming Trauma Informed: A Training for Correctional Professionals’ (an initiative that aims to bring about organisational change towards trauma-informed practice), and ‘Healing Trauma – a Brief Intervention for Women’ (a specific trauma-informed intervention that is delivered in prison and other settings (Covington, 2019). The materials include an ‘Implementation Plan and Goal Attainment Scale’ to facilitate change including training packages for the ongoing assessment and training of staff (Covington and Fallot, 2015). Across the women’s custodial estate at least 4000 members of staff (and some prisoners) have been trained in trauma-informed practice. This involves staff being aware of the backgrounds and vulnerabilities of those in their care, being sensitive, protective, offering help, affirmation and safety, and looking after their own health and well-being at work in order to provide the right kind of environment for prisoners. The BTI training attempts to embed trauma-informed practice through all levels of the prison and includes regular consultations (and bi-annual ‘top-up’ training where appropriate) with Governors, Prison Officer BTI Leads, Guide Teams and prisoner resident peer monitors. The training is very well-received by staff, who find it informative, relevant and useful. Two women’s prisons have declared themselves to be wholly ‘trauma-informed’.
This welcome ‘trauma turn’ – a movement in language and practice – is linked to broader changes in the community and in professional circles as the significance of trauma or adverse childhood events in later life struggles including offending, violence and suicide, is increasingly recognised (e.g. Wolff and Baglivio, 2016). The trend has been for much of the work to begin in settings for women and young adults, and then for it to be extended to adult men. This is related to the extremely high prevalence of traumatic forms of adversity, such as sexual abuse and neglect, among young women who find their way into mental health and criminal justice settings (Randall and Haskell, 2013: 508). The work, in general, is characterised as ‘gender-sensitive’. According to Kubiak et al. (2017: 96), ‘a trauma-informed correctional organisation is one in which administration have committed to creating a trauma-informed setting and will facilitate an infrastructure to initiate, support and guide changes’ which requires long-term commitment and guiding ‘champions’. This description, like much of the available literature, is about ‘inputs’ or provision. It does not set out what a trauma-informed setting might feel like for those who live in it. What does it mean for a prison to be ‘trauma-informed’?
The authors’ research in prisons has been largely driven by a preoccupation with the meaning-in-practice to prisoners of important words, or ‘concepts that matter’, such as humanity, respect, safety and trust (Liebling and Arnold, 2004; Liebling et al., 2011) and good uses of authority (Crewe et al., 2014). As might be expected, insufficient attention is paid to the challenging translation into practice of these key concepts in prison settings, and all too often official claims about ‘treating prisoners with humanity’ are not matched by prisoners’ experiences. Perhaps surprisingly, but important for our developing understanding of the complex inner life of prisons, there are significant differences in the extent to which individual establishments operationalised or ‘deliver’ what prisoners understand by humanity, respect, safety or authority (see Liebling, 2015) despite the best intentions of officials who launch such well-meant initiatives with increasing frequency (other examples include Rehabilitative Culture, Enabling Environments and Every Contact Matters). It was difficult not to approach the newly emerging ‘trauma-informed’ terminology in prisons with these interests and concerns in mind. The development of trauma-informed work is important and promising, and reflects enormous effort, undertaken in good faith and organised around several individuals’ expertise and engagement, as well as deep practitioner relevance and need. We fully support the intention and values underlying this development. We wondered what is meant by the concept, as well as what difference trauma-informed training, or claims, made to the treatment and experience of prisoners.
As we routinely carry out investigations of the ‘moral quality of life’ of individual prisons using a well-developed survey, and other methods, we were invited to carry out such an exercise in a prison that declared itself ‘wholly trauma-informed’, and to use our usual methodology to ‘pilot’ relevant items. 2 This possibility was welcomed by prison service managers, who were both excited by, and curious about, the impact of this work in the female estate in particular. At the request of the organisation, we developed an additional set of items intended to operationalised the concept of trauma-informed practice, which we were also able to test in a second prison for women. We used Factor Analysis to develop and evaluate survey items that we though captured the experience of trauma-informed practice. In this article, we describe this process and report on the findings. The results were, in many ways, disappointing. Only two of 22 relevant items were scored by prisoners at or above neutral; most were scored negatively. These results, discussed in more detail below, suggest that ‘trauma-informed practice’ might be both desirable and achievable – and our findings should not be interpreted as a criticism of its goals – but there is much work to be done in understanding what it is, how best to put it into effect or how staff know when they are ‘getting it right’. Its delivery does not necessarily coincide with adoption of the label (which raises the question of whether other terms might be more appropriate), as we have discovered in subsequent research. In this article, we describe the development of the 22 new items and present the results from the two women’s prisons: our first, and most systematic, attempt to explore this term and develop a measure. We argue, based on our experiences in the field, that a different language – of care and engagement – may help to make ‘trauma-informed’ practice real. We do this without professional expertise in trauma work, but with considerable experience in exploring the lived experience of imprisonment. Our aim is not to undermine the often outstanding initiatives that are going on, but to create a dialogue, based on empirical evidence, that might enhance it, supporting more sensitive or appropriate work with vulnerable populations and a better fit between aspirations and reality.
The underlying principles of TI practice
One of the key features of trauma-informed services is that they do not treat symptoms related to traumatic histories of abuse, but the services they offer are provided in a way that is sympathetic to the needs of service users with histories of abuse. Harris and Fallot (2001) were the first to call for such a ‘paradigm shift within service delivery systems’ (p. 21). They identified two distinct aspects of an organisation becoming ‘informed about trauma’; first, having knowledge of the abuse histories of their service users, and second, understanding the role that such histories play in their lives. They should then use this knowledge to reconfigure their service systems, taking these vulnerabilities into account in a way that would encourage the service user to engage with them.
Recent research has shown that there is relative consensus around the core domains of trauma-informed care (TIC). Branson et al. (2017) identified 10 core domains of trauma-informed practice in their systematic review, and organised them into the following three areas:
Clinical services. (1) Screening and assessment, (2) services and interventions, (3) cultural competence.
Agency context. (4) Youth and family engagement/involvement, (5) workforce development and support, (6) promoting a safe environment, (7) Agency policies, procedures and leadership.
System level. (8) Cross-system collaboration, (9) system-level policies and procedures, (10) quality assurance and evaluation.
The Substance Abuse and Mental Health Services Administration (SAMHSA, 2014) have produced a framework for the behavioural health speciality sectors that can be adapted to other settings that have the potential to ease or exacerbate individuals’ capacity to cope with traumatic experiences, such as prisons. They identify the following six key principles which are fundamental to their approach:
Physical and Psychological Safety.
Trustworthiness and Transparency.
Peer Support: ‘Peers’ refers to anyone who has experienced trauma; their stories are used to aid recovery and healing.
Collaboration and Mutuality: Emphasis is placed on forming partnerships between staff and clients, and reducing power differentials. The organisation recognises that ‘healing happens in relationships’ (SAMHSA, 2014, p. 11) and that all individuals can have a role to play in this.
Empowerment, Voice and Choice: Those served by the organisation are acknowledged and valued; clients have the autonomy and choice to make their own decisions. Staff are trained in self-advocacy skills: they are not controllers of recovery.
Cultural, Historical and Gender Issues: The organisation actively addresses cultural biases and stereotypes; and acknowledges and addresses historical trauma.
Can prisons be ‘trauma-informed’?
Trauma-informed environments seek to enhance feelings of safety and security (King, 2017). This presents significant challenges in penal environments where lockdowns, lack of personal space, risk of violence and confinement to a cell are commonplace. Practices like strip searches, the use of authority and difficult inter-personal relationships in a social environment that is not chosen create additional difficulties, and may echo or resonate with traumatic experiences. Staff may be influenced by vicarious trauma, which can affect workplace decision-making. Prison environments are often highly reactive and ‘reliant on “management by crisis”’ resulting in hyper-vigilance or numb detachment within work practice (Miller and Najavits, 2012: 3).
Scholars have noted some of the difficulties of achieving trauma-informed practice in institutional settings. Becker-Blease (2017) has stressed that ‘cultural awareness of trauma and its effects waxes and wanes’ (p. 131) and that vigilance is needed with regard to its current popularity. Several researchers have highlighted that trauma-informed training has been highly marketised, producing expensive training programmes whose efficacy is unproven (Becker-Blease, 2017; DePrince and Newman, 2011; Hanson and Lang, 2016; Jewkes et al., 2019) have problematised trauma-informed initiatives, observing that ‘it is not enough for prison staff to speak a trauma-sensitive language, or even engage in trauma-informed practice, if it is not fully embedded in the prison’s culture, fabric and design philosophy’ (p. 13). Carlen and Worrall (2004), Comfort (2009), Genders and Player (1995) and others have explored the troubled relationship between the fundamentally opposed concepts of therapy and punishment, which can undermine efforts to introduce trauma-informed practice in a prison context.
A systematic review of 23 studies which evaluated the effects of organisational interventions including a ‘trauma-informed’ staff training component (Purtle, 2018) concluded that training staff members about trauma-informed practice seemed to improve their knowledge about and attitudes towards others. However, it was not clear if these effects were long or short-term. The use of more sophisticated evaluation techniques and procedures would help improve the evidence base for these interventions and ensure that their effects are maximised.
Becker-Blease (2017) calls for critical engagement, without which there may be a risk of perpetuating damaging practices ‘by another name’ (Tseris, 2013 in Ibid: 132) by neglecting to address underlying causes of trauma including inequalities in power and societal forms of oppression (Reeves, 2015). Vaswani and Paul (2019) explored the views of over 200 prison staff members on the implementation of a trauma-informed approach in young people in custody in a Scottish female prison. They argued that prison staff support and endorse the role of a trauma-informed approach in prisons, but this is constrained by factors related to organisational purpose, which is fundamentally to punish. Bloom (2011) explains why this may be so: our systems often repeat the toxic experiences of the people they are supposed to help. Just as the lives of people affected by abuse and neglect become organised around the trauma they have experienced, so too can the experiences of those working within our helping systems. Smith et al. (1989) define these as ‘parallel processes’.
Pollack (2005) describes a women-centred programming course in Canadian women’s prisons, aimed at addressing trauma inflicted by high rates of abuse, violence and sexual assault among the female prisoners which, in practice, meant a different way of labelling and managing problematic individuals. The long-term effect of such interventions, especially in the post-release period when women remain at high risk, are unknown (Harner and Burgess, 2011). Levenson and Willis (2019) use SAMSHA’s core principles to make suggestions for the improvement of implementation of TIC in prisons, emphasising the importance of relationships. Safe relationships are stable, predictable and non-shaming. They model shared power and respect. This is the core of TIC. They also suggest that the acronym SHARE (safety, hope, autonomy, respect, empathy) will be helpful for staff trying to translate trauma-informed concepts into practice.
Studies of women’s experiences of ‘Healing Trauma’ (HT), a trauma-informed intervention delivered in prisons in England and Wales found that, in focus groups, the women said that the programme had the potential to give them opportunities to heal from trauma, and this was crucial given their generally negative experience of imprisonment. The women also highlighted areas of the programme that could be developed, such as follow-up sessions and holistic support outside the group (Petrillo, 2021). 3 Studies in the United States have shown similar promise: Rousseau et al. (2019) report on an evaluation of a trauma-informed programme that integrates psycho-education and mindfulness developed by the organisation YogaHOPE. Based on survey measures and qualitative feedback from 12 participants, the authors reported that the programme was beneficial overall, citing a wide range of effects such as decreases in the experience of negative symptomatology for depression, anxiety and post-traumatic stress disorder (PTSD), greater awareness of self and renegotiation of self-belief.
Our main argument in this article is that before any ‘effects’ of trauma-informed practice can be properly investigated, we need to be clearer about what this is and whether it exists in practice, beyond the delivery of some highly promising awareness training. Our aim, then, is to add to the knowledge-base and thinking in this important area.
Methodology: Conceptualising and measuring trauma-informed practice in a prison for women
Our attempt to capture the experience of trauma-informed practice for females in two prisons began with a review of the relevant literature, with a particular focus on research syntheses (e.g. Reeves, 2015) and papers that explored the concept of TIC (e.g. Hales et al., 2017; Harner and Burgess, 2011). Themes that emerged in the literature were used as ‘orienting’ concepts (see Layder, 1998: 101–103) in order to start the process of using theory to develop a measurement instrument. We also drew, throughout, on our varied experiences of doing research in women’s prisons, all of which involved extensive immersion in the field (Crewe et al., 2017; Digard and Liebling, 2012; Liebling, 1992, 1994; Liebling et al., 2005; Schliehe, 2016).
After digesting the literature, and drawing on fieldwork notes from several projects, each member of the research team was asked to draft five survey items that might reflect the concept of trauma-informed practice, expressed in terms of participants’ treatment and experience. We chose to avoid using the word ‘trauma’ in our descriptions, and to translate the underlying principles and values of TIC into a language that would reflect subjective experience, rather than referring to procedures and policies such as ‘Screening & assessment’ or ‘Promoting a safe environment’ (i.e. Branson et al.’s 2017 core elements). The statements were to ask as closely as possible about tangible events or experiences rather than hypothetical situations. We wanted to ask questions about a broad range of possible experiences, given that prisons differ, while keeping the number of questions as small as possible.
The literature suggests that TIC can be understood from several different perspectives including, but not limited to, the concept or experience of trauma, the individual seeking care, the care received and the relationship participants have to those responsible for their care. We attempted to explore all of these areas descriptively.
In our attempt to quantify complex experiences and processes, we faced the tricky issue of assigning a positive or negative value to each item. Some items, for example, ‘this prison allows me to express difficult feelings’ could be seen as an uncomfortable yet positive experience, and fairly typical of the experience of good TIC. Yet prisoners negotiate the expression of feelings and experiences in complex situations in prison in which their ‘risk’ is continually evaluated. They often find themselves under pressure to engage in ‘narrative labour’ or adopt an inauthentic self (Warr, 2019) in order to appear to others in a positive light. Contemporary prisons may be especially unlikely places for ‘expressing difficult feelings’ to lead to positive outcomes.
The statements that were drafted by the team were combined, and then reviewed one by one in a team meeting. The Chair (AL) proposed each item in turn, and each was discussed in detail by the team. Items were dropped or merged to avoid repetition and aid clarity until a final agreed list of 22 items was produced (see Table 1). This group of items formed a subscale in a larger research instrument called Measuring the Quality of Prison Life (MQPL), which had been developed using a more intensive, and largely qualitative methodology. 4
Structure matrix giving correlations between trauma-informed items and the two factors.
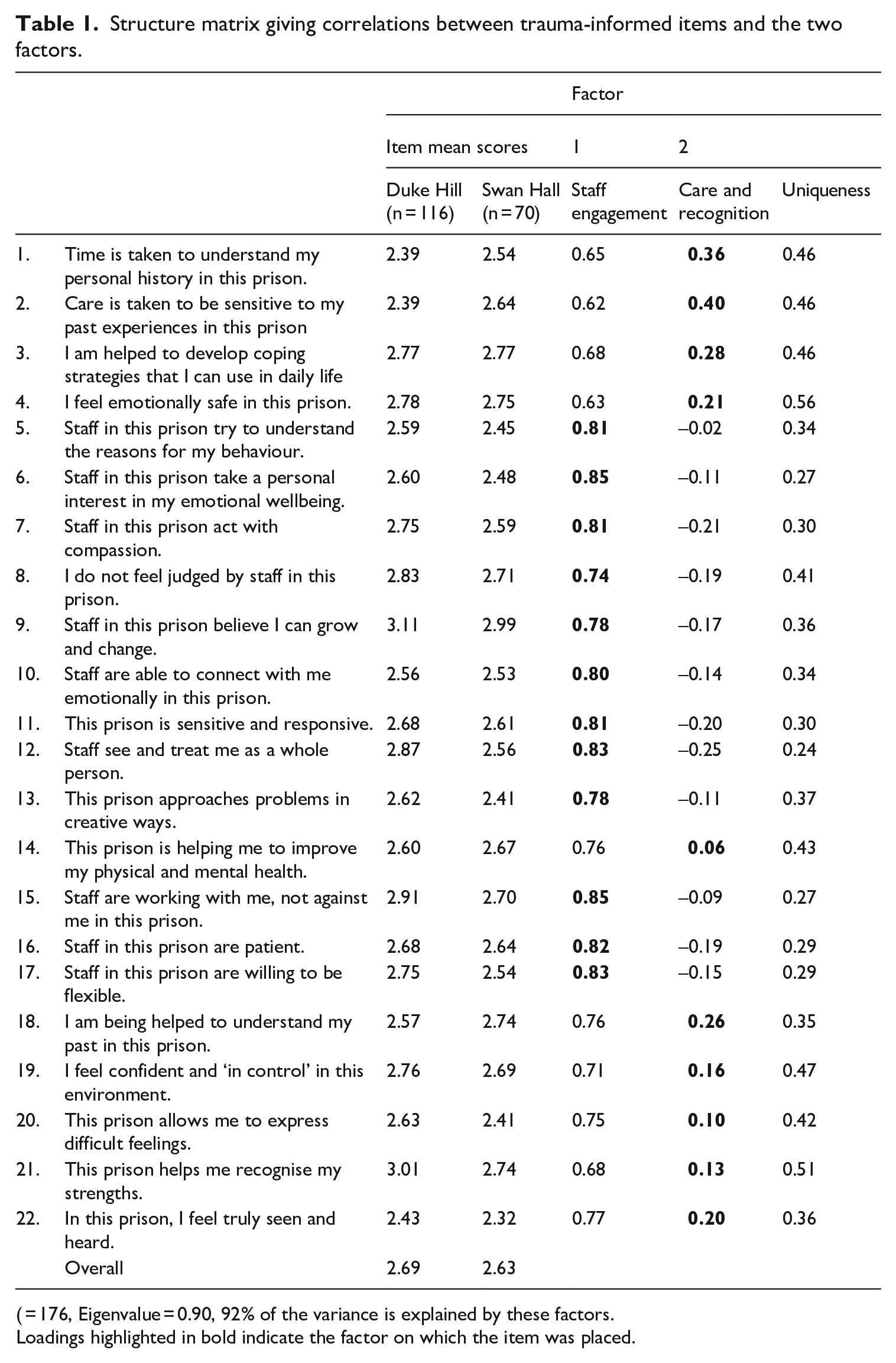
( = 176, Eigenvalue = 0.90, 92% of the variance is explained by these factors.
Loadings highlighted in bold indicate the factor on which the item was placed.
An existing ‘moral quality’ staff survey (the SQL) was adapted in the same way, with a list of additional items reflecting staff attitudes towards trauma-informed work, prisoners and their work experience, developed for this purpose.
In the first stage of the research (in June 2018), a random sample of approximately 100 prisoners in HMP Duke Hill – a women’s prison in the West Midlands, holding around 340 women aged 18 or above – were invited to complete the MQPL survey, as part of a wider research exercise aimed at understanding the quality of life for prisoners and staff at the establishment (in total, 116 women completed the survey). Informed consent for the surveys was obtained from each participant. The whole survey contained 116 items and asked about many aspects of the experience of life in Duke Hill. All participants were asked to indicate the extent to which they agreed or disagreed with each item on a 5-point Likert-type scale (strongly agree, agree, neither agree not disagree, disagree, strongly disagree). The prisoner surveys were completed mainly in focus groups with 8 to 10 participants at a time. The groups were overseen by members of the research team, who were present to explain the research, double check consent and address participants’ queries. Two research members in each group then hosted a discussion elaborating on participants’ views, including asking for feedback on the new items (this was positive). The staff survey was administered to all staff present at a full staff meeting (n = 113 surveys), following a presentation by the research team about the study. These methods were supplemented by observations, individual interviews with staff, senior managers and prisoners, and informal engagement in aspects of life in the prison. A team of nine from the Cambridge University Prisons Research Centre (PRC) were engaged in the fieldwork each day for a week. We stayed locally and held extensive debriefs each evening, swapping fieldwork notes and impressions of the prison throughout, and subsequently.
Analysis of the results
Mean scores were produced for each item, including the new ‘trauma-informed’ items. Those with a score of 3.00 or higher indicate an overall positive view for that item. Scores below 3.00 are negative. Based on cumulative experience carrying out MQPL+ exercises in more than 30 prisons, we treat scores approaching 2.50 or below as ‘alarming’ or crossing a dangerous threshold. Some dimensions in the survey (such as ‘bureaucratic legitimacy’) prove difficult to score well on generally (but importantly, we find occasional prisons that do score well). The interpretation of the quantitative survey data was undertaken in conjunction with the coding and synthesis of a large amount of qualitative data, collected as part of the intensive MQPL+ research. This included written comments from open-ended questions in the MQPL survey, and the formal and informal interviews and observations described earlier.
Results: HMP Duke Hill – Is trauma-informed practice going on?
Duke Hill is a semi-open prison, set in a rural location. The prison received an Enabling Environment award from the Royal College of Psychiatrists in March 2016 and began to develop ‘trauma-informed practice’ training for staff in the same year. Its Enabling Environment status had been recertified shortly before our visit. HMIP Inspectors had praised the prison at its last inspection (in 2016) for its stability, and the progress made on safety. ‘Non-invasive’ alternatives to physical searches had been introduced, a peer-led trauma-informed group operated in the prison, posters and other relevant information were on display in the reception and in the gate area, and training courses for staff were well-advertised.
Prisoners in Duke Hill, however, reported moderately positively for only two of the 22 relevant items – ‘staff in this prison believe I can grow and change’ (3.11) and ‘this prison helps me recognise my strengths’ (3.01, more ‘neutral’ than positive: 36% agreed and 33% disagreed). They reported negatively for the other 20 (see Table 1). Prisoners could see that some staff in the prison took a future-oriented approach to their lives, but staff did not always situate their behaviour in the context of their biographical experiences. In total, 58% prisoners disagreed or strongly disagreed that ‘time is taken to understand my personal history in this prison’. Some prisoners complained that prison staff had little meaningful understanding of their histories, or exacerbated their problems: Trauma-orientation is bullshit – they do not look into the deeper reasons for your behaviour. (Prisoner) They don’t know your story here. They all knew my story in [another prison]. (Prisoner comment) It’s [this prison] caused me trauma. (Prisoner comment) They take the lid off the can of worms and leave you in prison, with officers that are not mental health trained. (Prisoner comment)
Only 16% of women agreed with the item, ‘in this prison I feel truly seen and heard’. Many prisoners expressed scepticism about the prison’s proclamations about being trauma-informed in practice. That the language of ‘trauma-informed’ was being used around the prison, but censoriously or critically, made the contrast between ‘the aspiration’ and ‘the reality’ stark: The staff need training in how to understand trauma. (MQPL comment) Trauma ethos not trickling through to operational staff. (MQPL comment)
The overall score for the ‘trauma-informed’ dimension was a low 2.69 (a score of 2.50 or below is our ‘alarm’ threshold for MQPL dimensions in general).
Staff attitudes were raised as a general problem in the prison by both prisoners and staff. Although some officers were very motivated, passionate and caring, many prisoners identified problems with the prison’s underlying (traditional, divided and heavily unionised) culture. Staff and prisoners told the research team about incidents in which some staff intentionally antagonised, provoked or shamed women in their care. Aspects of the staff culture were, then, punitive and uncaring, as some staff themselves acknowledged: Just because they’re women doesn’t make them nice and sweet – they’re just as dangerous as men, sometimes even more so . . . can’t trust ‘em. (Staff quote from fieldwork notes) Some staff love to catch the women in the wrong and punish them. It’s like what they live for. (Staff member) I know a young girl who’s had a trauma and hasn’t spoken to anyone. She told an officer she couldn’t cope and he just sort of told her she’d have to get on with it. (Prisoner) Staff go out of their way to not see prisoners as people. (Staff member)
These were ‘condemnation narratives’ (Maruna, 2001). The team witnessed several incidents of verbal abuse of women by staff (e.g. ‘you don’t deserve a family visit’), and some observed practices, like the forceful removal of clothing from women suspected of hiding contraband, or hospital escorts accompanied solely by male staff, were likely to compound rather than neutralise past traumas. This was dispiriting to those senior managers and other staff who were invested in making trauma-informed practice and enabling environments a reality.
A lack of access to regular, formal counselling was considered problematic by many prisoners and some staff. Many of the women were attempting to regulate extremely complex experiences, or manage grief, on their own – or sometimes, with the help of the chaplaincy – rather than with any significant therapeutic provision: There was nothing therapeutic here – no counselling, no mental health or other support groups (outside the peer-led trauma group), few (if any) informal therapeutic outlets, staff were not therapeutically inclined or supportive, nor were there any behaviour intervention courses which may have helped some women, and at the very least looked good for parole boards. (Comment from fieldwork notes) There is not enough on a day-to-day basis for counselling. (Prisoner comment)
Healthcare was described as ‘awful’. ‘There is no compassion and they do the bare minimum. Just no decency and completely inflexible’ (Staff member). Attitudes towards self-harm were often unsympathetic. Anxiety about being patronised or humiliated prevented some women from seeking help from unit staff: ‘there’s no care, it’s frightening’ (Prisoner). The distance between the promise and delivery of support services made some women more vulnerable to the use of illicit substances: ‘you leave your addiction at the gate, but it’s always waiting to wrap itself back ‘round you’ (Prisoner comment).
These responses indicate that vulnerable women, especially, felt insecure or invisible and considered the overall climate to lack sufficient care. In our general report to the prison, we characterised its form of order as ‘light, absent, insecure’ (see Crewe et al., 2014; Kant et al., 2018). Only 11 of the 21 usual MQPL dimensions scored 3 or above. 5 That 11 did so suggests that the new dimension is a ‘stronger test’ of ‘trauma-informed prison quality’ than many of our existing dimensions, and that it is hard to achieve.
Staff, however, generally reported very positively on their trauma-informed practice and saw themselves as very willing to engage with women with complex histories on an emotional level (see Table 2).
6
Such orientations were reflected in high scores on the items, ‘I recognise the impact of past experiences on the prisoners in my care’ (4.15), ‘I am confident in helping women work through difficult feelings’ (4.04) and ‘I consider the life histories of prisoners in most of my interactions with them’ (3.95). Nevertheless, the practice of TIC was not ‘embedded’. A minority of staff were actively resisting its implementation. Others expressed disappointment or were disheartened by the distance between the advertised status of a trauma-sensitive prison and the day-to-day experience of life for the women: Trauma-informed care is there in name and logo, but not in practice. (Staff member) We see the words written on signs [about trauma informed] but that’s where it stops. (Staff member)
HMP Duke Hill descriptives for trauma-informed practice staff items (n = 113).
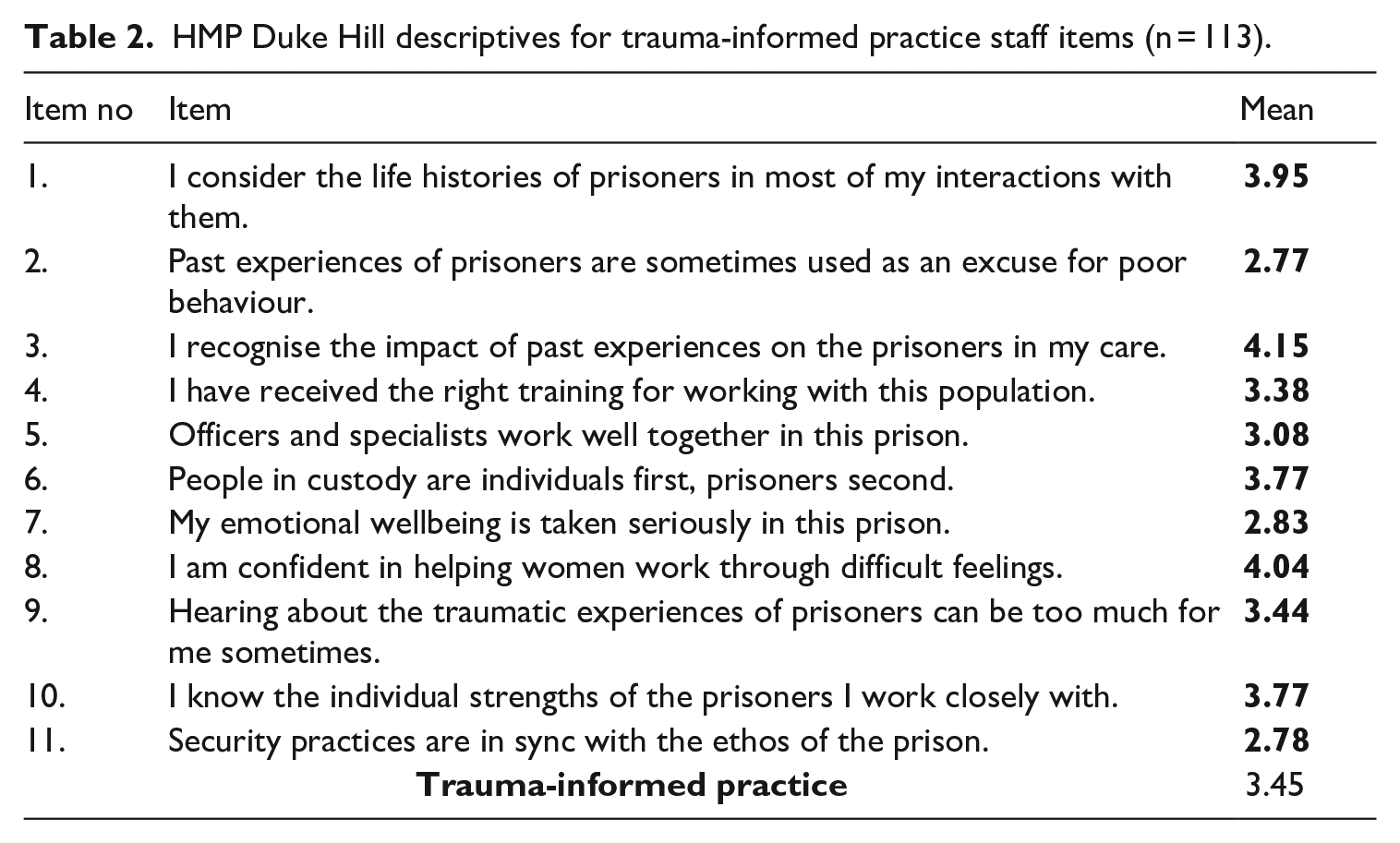
While many staff used trauma-informed language, trauma-informed practice was limited. Many staff felt that they lacked the training and support to engage fully with the concepts they had been taught. Often, staff expressed a view that the prison was addressing trauma only superficially, or was producing additional problems: We teach them how to build a bike [in a cycle workshop], but we don’t help them deal with their underlying issues. There is nothing therapeutic here. (Staff member) The general environment in here is not trauma informed at all. Trauma is not recognised. There’s absolutely zero help with self-harm. (Staff member) People get lost in the system here, and the chaos and misery that it creates is dehumanizing. (Staff member)
The challenges of, and obstacles to, embedding a trauma-informed environment were manifold. One aspect of Duke Hill that was generally regarded as positive was its physical environment, including extensive grounds that were kept very clean and well maintained. The open regime (all day unlock, free flow) meant that many participants expressed a sense of ‘independence’ and ‘freedom’. However, the open environment and low level of supervision meant that it was easy to get into trouble or be at the mercy of other prisoners. For women in the prison who were vulnerable, due to mental health problems, issues with drug use or debt, this created additional stress. On the comments section of the MQPL survey, the presence of drugs, bullying and fear of victimisation were frequently raised as primary concerns and as the most negative aspects of imprisonment. One participant described the prison as ‘run by drugs. The hierarchy know and are not doing anything about it’. Another described staff as ‘lackadaisical about vulnerable prisoners’ (Fieldwork notes). Within the wider MQPL survey results, ‘Drugs and exploitation’ (2.06) was the lowest (most negatively) scoring dimension for prisoners and scored significantly lower than comparable establishments.
One reason for the lack of appropriate care was that many prison officers, whose wellbeing is a key component of good practice in a trauma-informed setting, lacked confidence in how to manage or assist women who were at risk of self-harm and suicide, or who had mental health problems. Many reported feeling unsupported in their efforts to provide professional and emotional support. In total, 60% of uniformed staff agreed that ‘staff need more training and support in dealing with the effects on them of suicide and self-harm’ (2.53). In total, 45% agreed that ‘working in this prison is highly emotionally demanding’ (2.78). In total, 75% stated that ‘dealing with suicide and self-harm by prisoners is extremely stressful’ (2.18). Managing complex cases and histories was demanding and officers repeatedly described the toll that this kind of work took on them: We’re mental health aware, but we’re not trained. We refer someone to healthcare and they just go, ‘oh don’t have the time’. And then I spend half an hour with them and that’s a trigger for me then. (Staff member) Hearing distressing life histories/events of the female prisoners over and over again. (SQL comment) We listen to some horrendous things, and it’s not recognised, the toll that takes on you. (Staff member)
Some officers struggled to come to terms with their feelings of guilt and responsibility about two women who had taken their own lives in the prison within the previous 12-months: ‘I felt like we’d let her down. Why didn’t we see it?’ (Staff member). Some were unsure how to process disclosures of trauma from women in their care and sought more support from managers and greater recognition of the stress produced by this aspect of their work, within a culture that tended to suppress emotional disclosure: We don’t talk about feelings at all in this prison. No one does. Not staff, or prisoners, and certainly not to each other. (Staff member)
In summary, then, trauma-informed practices were both limited and (like other care-related work) difficult to develop, or join up, in a culture that was divided, ambivalent and full of trauma.
HMP Swan Hall
Following the research exercise in HMP Duke Hill, partly driven by our developing interest in the question of what trauma-informed practice might look like, a continuing search for better practice, and in order to increase the sample size so that we could explore the factor structure of the new trauma-informed dimension more carefully, the same trauma-informed items were added into a survey being used in a separate research project, undertaken in a second women’s prison, HMP Swan Hall (in September 2018), located around 20 miles south of London, and holding around 280 women. 7
Unlike Duke Hill, HMP Swan Hall was not officially described as a trauma informed, nor accredited as an ‘enabling’ environment. Nonetheless, aspects of trauma-informed practice existed in its therapeutic community and ‘PIPE’ unit (Psychologically Informed Planned Environment), and a course, ‘Healing Trauma and Becoming Trauma Informed’ was being delivered (from February 2017). Some of Swan Hall’s practice was shaped by trauma-informed thinking (there were many posters around the prison advertising this, and the language was used by some staff). In its most recent inspection report (2018), Swan Hall was rated highly as a safe environment with low levels of violence.
This generally positive review was not reflected in the responses (n = 70) to the 22 survey items relating to trauma, all of which were, like at Duke Hill, rated below the neutral threshold. The highest mean score was for the item, ‘Staff in this prison believe I can grow and change’, at 2.99, while the lowest was for the item, ‘In this prison I feel truly seen and heard’, with almost 60% prisoners disagreeing with the statement. Fewer than 20% of prisoners agreed with the items, ‘Time is taken to understand my personal history in this prison’ and ‘Care is taken to be sensitive to my past experiences in this prison’. Fewer than a quarter of prisoners agreed with the statements, ‘This prison is sensitive and responsive’ and ‘Staff see me and treat me as a whole person’. These findings were strikingly close to those at Duke Hill (see Table 1).
Staff–prisoner relationships in Swan Hall were not highly rated (3.11).
8
Many interviewees, especially those on the prison’s more open units, reported that officers were rather absent, and while there were many calm and supportive staff who executed their duties in ways that were consistent with trauma-informed practice (e.g. taking time to talk one-to-one with prisoners about their mental health problems, and how to manage them), prisoners often described a culture that could be somewhat oppressive and antagonistic: I avoid officers like the plague [. . .] they antagonise you and abuse their authority [. . .] some are preying on vulnerable women. (Prisoner, interview) When you’re not a good prisoner, officers target you. When you are on their radar, you’re fucked. (Prisoner, interview)
Participants often felt that prison staff were somewhat indifferent to their emotional needs. Over 50% disagreed with the statements, ‘Staff in this prison try to understand the reasons for my behaviour’ and ‘Staff in this prison take a personal interest in my emotional wellbeing’, while over 60% disagreed with the item, ‘Staff are able to connect with me emotionally in this prison’. Such views were corroborated by comments made in interviews: This jail in general doesn’t have many officers who understand emotional needs of trauma certain women have been through. 20-30% are homophobic and I feel targeted by at least three officers. (Prisoner comment survey) Staff telling me to ‘grow up’ – they make you out to be immature. (Prisoner, interview)
Many women talked about the negative effects on them of not being fully ‘seen’, including feelings of loneliness: ‘all you are here is a number. In here you are very alone – extremely lonely’ (Notes from interview); ‘I feel like I am dead’ (Prisoner, interview). Likewise, many participants described being unable to fully communicate their problems and concerns: 55% disagreed with the statement that ‘This prison allows me to express difficult feelings’. In interviews, many women who were categorised as ‘trouble’ – often black, younger women from around London, but also those struggling with chronic illnesses and mental health problems and/or learning difficulties – expressed this view.
As in Duke Hill, some qualities of the establishment impeded or undermined trauma-sensitive experiences. The physical environment and well-maintained grounds, including a pond with ducklings, were attractive and the relatively open regime within the prison’s perimeter (free association outside, free flow inside) was appreciated. Much like in Duke Hill, such conditions provided a sense of ‘independence’, but produced an environment that was insecure for women who were vulnerable or anxious around others. A ‘hands-off’ orientation among some staff enabled bullying and threatening behaviour between the women. Many reported staff practices that echoed the forms of abuse they had experienced in their lives before prison, including the forceful removal of clothing from those suspected of hiding contraband.
Other sources of frustration were similar to those in Duke Hill, including the level and quality of healthcare and poor mental health provision. Women who did not qualify to go onto the prison’s PIPE unit or therapeutic community complained about the relative paucity of therapeutic work. Some women felt particularly isolated and neglected: My health deteriorated in here, pain is not managed and there are not enough resources, no help for disabled people [. . .] staff don’t ask and assume everything is fine [. . .] it’s the disabled looking after the disabled. (Prisoner, interview)
Some participants experienced high levels of stress relating to negotiations to see children, receiving authorisation for home visits, or managing the stark difference between emotionally intense visits and the subsequent feelings of separation.
At both prisons, then, the results on the new ‘trauma-informed’ items were surprisingly poor. The self-declared status of being a ‘trauma-informed prison’ did not differentiate it from a prison without this self-image. 9 We received positive feedback on our items (women assured us that we were measuring the right things) but our findings were disappointing.
The underlying dimensional structure
In the last section of this article, we explore the underlying structure of the trauma-informed construct, as captured by our 22 survey items. How did the items ‘work’? Did they form a single dimension, or were there distinct, latent constructs within it? This analytic step also helps highlight why trauma-informed practice in prisons, and in women’s prisons particularly, is so essential and yet so hard to achieve.
These questions were explored using factor analysis (for a concise explanation of this approach, see Bartholomew et al., 2008). 10 A principal factors unrotated factor analysis was performed. The eigenvalues revealed one dominant factor, but also suggested the possibility that two factors might exist. After examining a screen plot, we decided to extract two factors. The estimated factor loadings for the two-factor model are shown in Table 1.
The output revealed that the two-factor solution appeared to be contrasting two sets of items. We offer our interpretation of these two factors below. Figure 1 shows a plot of the factor loadings from the two-factor model. From this plot, we can see that the survey items were roughly separated into two groups (as shown by the two ellipses). The smaller blue ellipse at the bottom left-hand corner of the chart is Factor 1, which we have called (based on the items within it) Staff Engagement. This is the dominant factor, as reflected in the fact that the points lie close to each other. The larger red ellipse is factor 2, which we have called (based on the items in here) Care and Recognition. In this weaker factor, the points are much more dispersed throughout the geometric space.
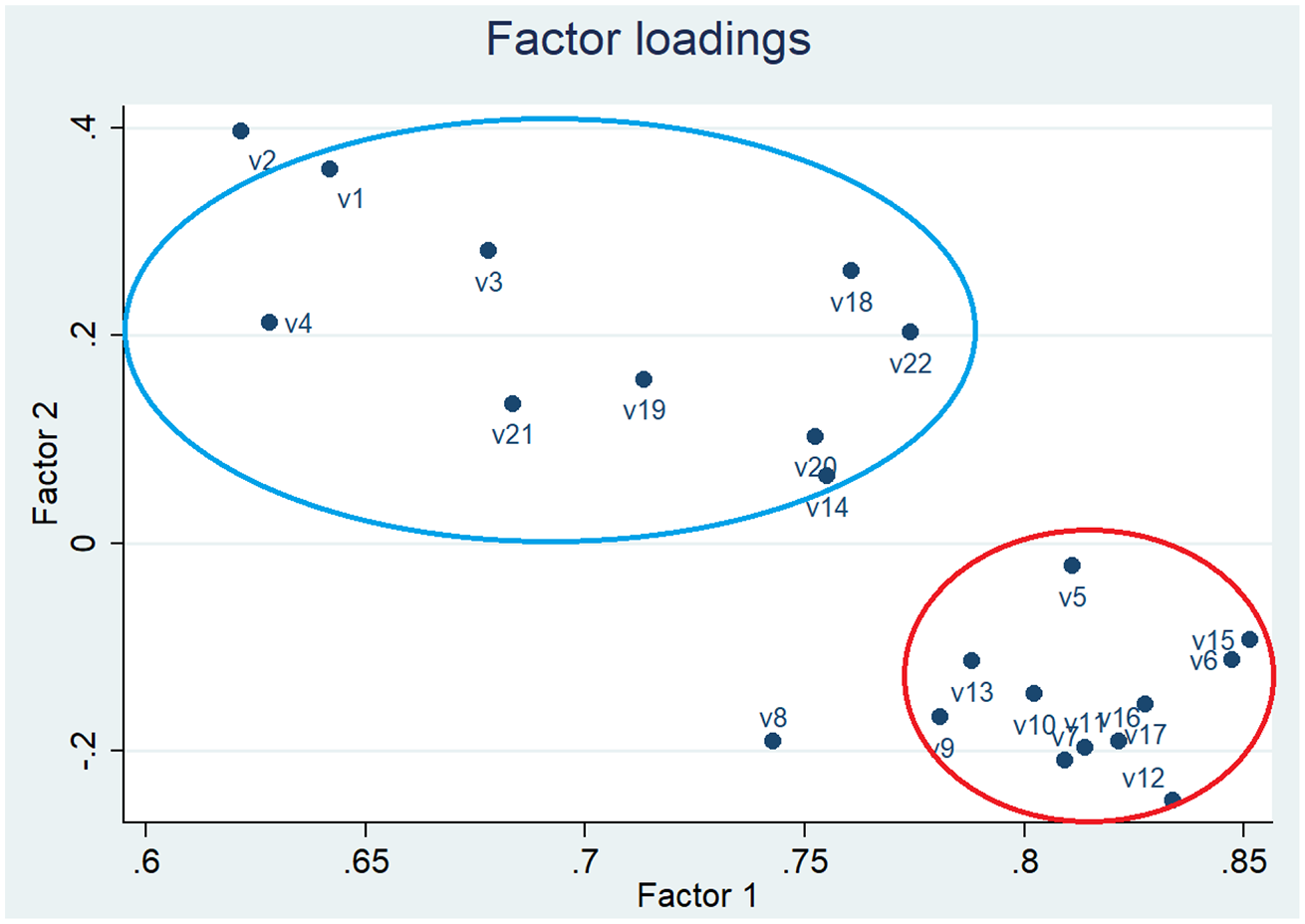
Plot of loadings from a two-factor model of the trauma-informed survey data.
The first factor seemed to capture participants’ views of the extent to which the work of staff embraced the values of TIC, or to describe the survey participants’ general attitude towards their care. There were no negatively worded items. The second factor appeared to include two sets of items and to capture individuals’ personal experiences of TIC.
The figures in the ‘Uniqueness’ column reflect the percentage variance for the variable that is not explained by the common factors. As our values were not high (they were all less than 0.6), it seems that all of our variables were reasonably well explained by each of the factors.
To explore these patterns further, we obtained the loadings plot, which is shown in Figure 1.
We consider these two latent factors further below. Factor 2: Care and Recognition is discussed in less detail, as we found more limited empirical support for it, but we think it has future potential.
Factor 1: Staff engagement
This factor reflects the fact that prisons are highly relational environments. The quality of prisoners’ relationships with staff are central to the women’s experiences and are key to many of the principles of trauma-informed custodial care. All the items that have high loadings on this dimension mention staff: the way they relate, understand, take an interest in and connect to, the women in their care. Staff-prisoner relationships are the most important feature of trauma-informed custodial care because (a) staff-prisoner relationships constitute much of the quality of life in a prison and (b) victims of violence or abuse may come to have negative or persecutory thoughts about particular groups of people, for example, those in positions of authority, making their ‘reading’ of, or sensitivity to, these relationships especially acute. According to Covington, ‘in adolescence, girls are more likely than boys to continue to be abused or assaulted, more often in private and by someone close to them, such as a family member’ (cited in Epstein and Gonzalez, 2017: 18). As Jones (2018) argues, ‘all traumatic experiences need to be thought of as being fundamentally relational; they are defined by their impact on the capacity to relate’ (p. 93). ‘This interpersonal aspect of sexual abuse has a unique and complex effect on girls, which can influence the services necessary for healing’ (Epstein and Gonzalez, 2017: 18). In this context, getting staff-prisoner relationships right is paramount. We know from existing research that staff–prisoner relationships and legitimate or illegitimate uses of power are inextricably linked (Crewe, 2011; Liebling, 2000, 2011). Power in prisons is intimate; and since prisoners are dependent on staff for almost all their day-to-day needs, how staff use their authority through relationships, is all the more critical.
Factor 2: Care and recognition
The items in the dimension, Care and Recognition seem to reflect the internal experience of effective trauma-informed custodial care for individual women. These are items relating to the expression of difficult feelings, and feeling safe, confident, heard and accepted. They reflect what it feels like to be treated sensitively and with compassion, where affect dysregulation can be soothed rather than provoked, and feelings of attunement and collaboration can reassure and support. The environment is (i.e. staff are) responsive, and so emotions can be tolerated, and agency can be exercised, safely. This is extremely difficult to accomplish in a prison, but we have found higher scores on these items in other research we hope to report on in due course. These sites had high levels of specialist support. Further testing and development of these dimensions, ideally with others working in the field, is required.
Concluding comments
These two components of trauma-informed practice – staff engagement, and care and recognition – help to give meaning and grounding to what is going on in daily practice, although we do not claim that we have exhausted the possibilities, or achieved full operationalisation of this important area of work. There were strong correlations between items in the ‘trauma-informed’ dimension and those in the existing MQPL dimensions, ‘Respect’, ‘Humanity’ and ‘Staff-Prisoner relationships’. This suggests (as we discovered later, in another prison) that TIC may be, at least in part, an extension and development of ‘good prison practice’ (see, for example, Kubiak et al., 2017) in which clear examples of ‘trauma-informed’ and ‘non-trauma-informed’ behaviours are given). Aspects of the Offender Personality Disorder (OPD) pathway’s relational-developmental strategy, the language of ordinary ‘deep human regard’ (Beedon, 2020), and drawing on all we already know about the importance of respect, fairness and safety, may support the endeavour to bring about ‘trauma-informed practice’ in prisons for women and men. 11 One possibility is that framing this kind of practice in terms that are already meaningful to prison staff might enable them to engage in it more effectively, as part of a general drive towards ‘improved moral quality’, rather than as an ‘add-on’ training package. A second is that providing a trauma-informed environment for female prisoners is a particularly difficult task, because of the exceptional rates of trauma that women bring into the environment, combined with the inherent features of imprisonment. We cannot answer the question of whether better scores on the new items might be found in other women’s prisons, or whether practices have now improved in the two prisons reported on here, following some valiantly received feedback and dialogue about these results. Our hope is that this article goes some way towards highlighting these challenges, improving initiatives that are worthy of support regardless of their current limitations, and finding meaningful ways of evaluating these initiatives.
Footnotes
Acknowledgements
The authors would like to thank Deborah Kant, Bethany Schmidt, Martha Morey, Ben Laws, Aiden Cope and Julie Laursen for their assistance and engagement throughout this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Her Majesty’s Prison and Probation Service and the European Research Council (648691). The views expressed here are those of the authors and not necessarily those of Her Majesty’s Prison or Probation Service or the European Research Council.