
Abstract
This study interviewed stakeholders involved with women's Rugby in Ireland consisting of male and female coaches (n = 5), physiotherapists (n = 3), strength and conditioning coaches (n = 3) and female players (n = 3) on their knowledge and awareness of breast health issues. The findings indicate overall limited breast health knowledge and awareness amongst interviewees. Breast health issues can have potential future health complications such as fat necrosis or tissue scaring. The primary barrier to reporting breast health issues ascertained was due to the sensitive nature of the topic. The results further highlighted a lack of reporting pathways and treatment options for breast health problems among support staff overall. Additionally, this study indicates that current breast protective measures were not evidence-based, requiring further research. The findings underscored the need for targeted education, preferably by a female educator, on breast health issues for female players, coaches, and support staff, and tailored to stakeholder preferences to improve efficacy.
Introduction
Female participation in sports is increasing globally 1 and is supported by the International Olympic Committee (IOC) encouraging females to participate at all levels of play. This encouragement is further supported via initiatives aiming to create equality in key areas such as resource allocation or access to facilities and coaches. 2 A notable example of this progress can be observed in Rugby Union, (hereafter Rugby), where World Rugby has reported a 28% rise in female player registrations since 2017. As a result, females now constitute over a quarter of the total playing population in the sport worldwide. 3
Increased female participation in sport brings with it a concomitant increase in injury frequency, as well as a rise in issues that are particular and unique to the female athlete. These include issues pertaining to peri and post pregnancy and the pelvic floor.4,5 Breast health in female rugby athletes is a further issue that is poorly addressed and lacks awareness in female athletes, despite a marked prevalence of breast pain and injury in this cohort.6–8 The foci of this study were two breast health issues: exercise-induced breast pain (EIBP) and contact breast injury (CBI). CBI results from a blunt force impacting the breast,9,10 while EIBP stems from excessive or frictional movement during sport.11,12 Existing literature has displayed the under or non-reporting of both CBI6,13 and EIBP 14 but explanations for these reporting inadequacies are inchoate.
Further considerations surround the flexibility of current injury surveillance systems to appropriately record breast pain and injury, 15 as well as the willingness of players to report these events. Breast health may be perceived as a delicate subject that might be a source of embarrassment for some players, and potentially support staff. However, it is key that any stigma is addressed and that players are empowered to report and receive treatment for their pain and injury. Existing research indicates that female players may be less comfortable discussing sensitive issues with male support staff.16,17 Given that the majority of support staff in rugby are indeed male,18,19 targeted measures to overcome any reticence to report are urgently required.
Breast pain and injury may have significant short- and longer-term consequences for the player. These include performance deficits while playing,6,8 and more worrisome future health complications such as tissue scarring, haematomas, and fat necrosis which can complicate breast screening as it might be falsely identified as cancerous tissue. 20 Raising awareness of breast health in players is thus of high importance, and must involve all stakeholders including players, support staff and management charged with their care.
Previous research in Rugby environments, which surveyed coaches and medical staff on their awareness and perception of breast injuries, 21 was limited by a quantitative approach that lacks the nuance of data produced by alternative methodologies, for example the reduction of topic complexity, overgeneralisation, and context limitations. Hence, the current study aimed to qualitatively investigate the awareness, experience, and knowledge of EIBP and CBI among multiple stakeholders involved in women's Rugby.
Methods
This study included interviews with coaches, strength and conditioning coaches (S&C), physiotherapists and female Rugby players. These perspectives were explored in an Irish setting. Irish Rugby is amongst the most developed in the game internationally, both at the elite and grass root levels in both genders as current world rankings indicate. 22 Interviewees provided insights into reporting situations of pain or injury and perceived barriers, the availability of treatment, prevention, and access to female staff, as well as the influence breast pain and injury might have on team selection or training participation.
Study participants
Coaches (n = 5), physiotherapists (n = 3) and S&C (n = 3) of male and female sex as well as female players (n = 3) representing different levels of play (amateur, provincial, and national) were included (Table 2). Participants were identified using the researchers’ network. Coaches, physiotherapists and S&C had an average of 6.7 years’ experience (SD = 5.1, Range = 1–15), while players had an average of 6 years’ experience playing at their respective level (Table 1). Interviews lasted between fourteen and twenty-eight minutes in duration.
Participant characteristics.
Strength and conditioning coach (S&C).
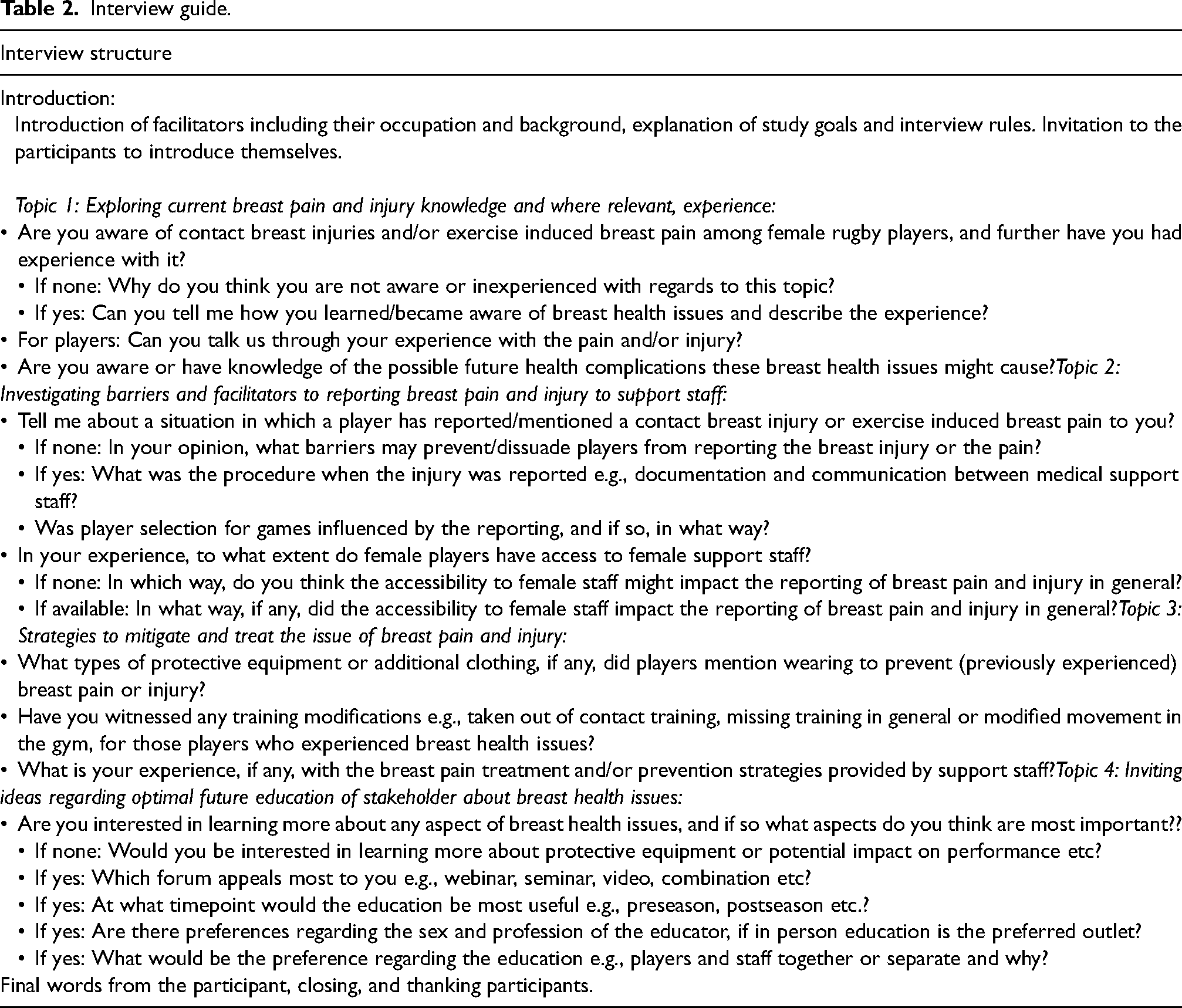
Interview guide.
Materials
The study was guided by the consolidated criteria for reporting qualitative studies checklist (COREQ). 23 In preparation for the interviews, an interview guide was developed by three of the researchers (KB, IK, and RC) (Table 2). The interview guide was informed by pre-existing research refined iteratively by these members of the research team. 24
Procedure
Initially males and females aged 18 or over based in Ireland were identified, from a profession of relevance (coach, S&C, physiotherapist, and players) and different levels of play (amateur, provincial, and national). Provincial women's Rugby in Ireland provides a competitive platform for players across the four provinces of Munster, Ulster, Leinster and Connacht. Each province selects players from amateur clubs within its region, usually involving some of the most skilled available, including those who may be on the radar for national selection. For recruitment of participants the authors’ network was utilised. Study information and consent form were circulated to potential participants via existing contact details or social media (X or LinkedIn). All interviewees provided written informed consent prior to participation with ethical approval for the study obtained via the institution's ethical review board. Participants undertook a semi-structured, in-depth interview which was led by a female and a male moderator (LG and KB) online via Microsoft Teams, and was video recorded. A backup audio recording was additionally obtained. The moderators LG and KB are experienced working within Rugby in Ireland as a physiotherapist and S&C respectively. Interviews consisted of open-ended questions (Table 2). Follow-up questions focused on eliciting a deeper understanding of the support staff and players’ knowledge on the management, reporting, and prevention of breast pain and injury. The interview guide was further piloted with members of the target study cohort, who suggested minor additions which were embedded in the interview guide. Sampling stopped when data saturation was reached, meaning no new conceptually significant information was emerging from additional interviews. 25 A randomly chosen member from each cohort received their transcript to check for correctness, and no changes were made to any transcript.
Data analysis
Due to the exploratory nature of this research in a new setting, a directed content analysis was chosen.26,27 This deductive approach added further description to the existing limited research, while also aiming to report common issues identified in the data, and to validate or extend currently existing theories.26,28 The ten step guideline for content analysis developed by White and Marsh (2006) was used, and supported by the deductive analysis approach presented by Elo and Kyngäs (2008). Where applicable, results were presented using visual techniques to aid interpretation. 29 Supportive, non-quantifiable data were descriptively reported via detailed examples and quotations. Deductive content analysis, using NVivo 14, was conducted after it was agreed by the facilitating researchers that data saturation had been reached.
Results
Awareness of, and experience with, breast pain and injury and future health complications
Awareness of and experience with breast pain and injury
Of all fourteen interviewees, just half were aware of CBI or EIBP; this included two coaches, two S&Cs and three physiotherapists (Figure 1).
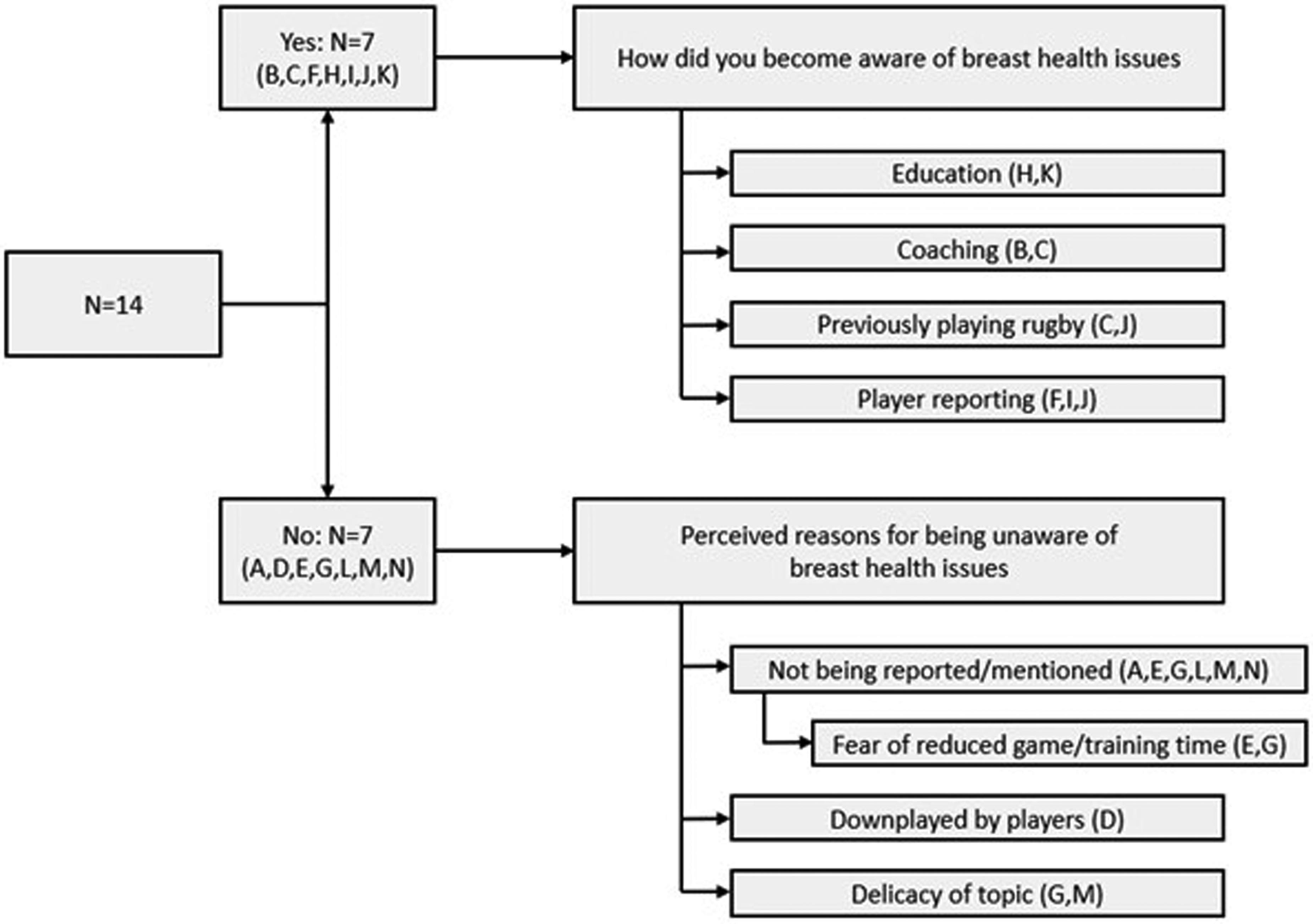
Awareness and proposed explanation regarding awareness or unawareness of breast pain and injury among coaches, strength and conditioning coaches, physiotherapists, and players.
Participants with prior awareness or experience of the topic mentioned that this stemmed from players reporting either pain or injury to them. One coach stated that he had experienced players mentioning breast pain and injury, almost “as an aside”. He further mentioned that he was lacking the awareness to classify these reports as potential breast health issues: […] it was kind of raised in a not a serious way, in a jokey kind of way. ‘I can't do this because it's actually really sore’. So, like you know, it's totally fair. But before that didn't really put two and two together, which is probably in hindsight, something that we need to look at. (D)
None of the female players themselves had experienced either a CBI or EIBP. Two players (L, N) witnessed other players mentioning EIBP and/or CBI but reported a general lack of awareness of these events being an issue: I think there's been a few, a few girls that I remember during a contact session and more so than in a game. I definitely have heard girls that have had breast contact during training sessions. And again, ironically, nothing enough that I'd say that's an injury that you'd stop, or you'd do anything about it, but you definitely would hear people in training if they get a big hit on their chest and it tends to be girls with probably a bigger chest than those with a smaller chest that would make the comment. (L) Yeah, not myself. Through other players, yes. And their only awareness around it is the fact that they be looking to buy a more supportive sports bra for protection. But that's literally it, to be quite honest with you […] I've never had pain from impact. I suppose, well depends on the size, breast are made up of fatty tissue. It probably isn't going to hurt as much and long-term stuff would know nothing about it. Short term, if someone does get a bang, I don't think it was them being in a lot of pain. (N)
When participants with no awareness of CBI or EIBP were asked to speculate on why that might be, they posited several reasons, centring on player behaviours in reporting (Figure 1).
Awareness of possible future health complications of breast health issues
Out of all interviewees, twelve were unaware of the possible future health complications arising from CBI and or EIBP. One coach (C) and one physiotherapist (K) reported “some” or “little” awareness but admitted that there were gaps in terms of knowledge.
Perceived barriers of reporting CBI and EIBP towards support staff
Reporting and recording of CBI and EIBP
The majority of participants recounted that the reporting of CBI and EIBP happened infrequently, and when arose was typically a passing comment from players that was not formally recorded. Reporting by the female players towards support staff was mainly done in an informal manner, as highlighted during interviews: You know, it's normally a bit of a laugh and a joke that they will come up to and go, ‘Oh my God, I just got hit and it is so sore’ and it's 5 seconds and it's never going to be a time loss, so we never have it as a time loss injury or anything like that, but it is something that they'll comment on. (F) They would mention it very flippantly so like often it would happen that they would report it, but not that they actually looking for more treatment for it or anything like that. It would be something that they would note to me and then just carry on playing. (J)
Throughout the responses, there was a generalised vagueness about the reporting and recording of breast health issues. One participant commented: I did ask the player, had they seen the physio with the injury? Kind of on the assumption that it would be recorded and in the kind of injury surveillance software, whatever is in place. But yeah, I didn't follow up on that. (C)
In just one instance, there was a clear episode where CBI and EIBP were reported and duly recorded. This was by one of the physiotherapist participants (I). When pressed on possible reasons for non-reporting of CBI and EIBP, half of the participants mentioned delicacy of topic and/or body region as a potential barrier (Figure 2). Other potential barriers to reporting are outlined in Figure 2 and include a range of player and structural factors. One barrier to reporting, classified as maturity, included younger age and shorter playing experience.
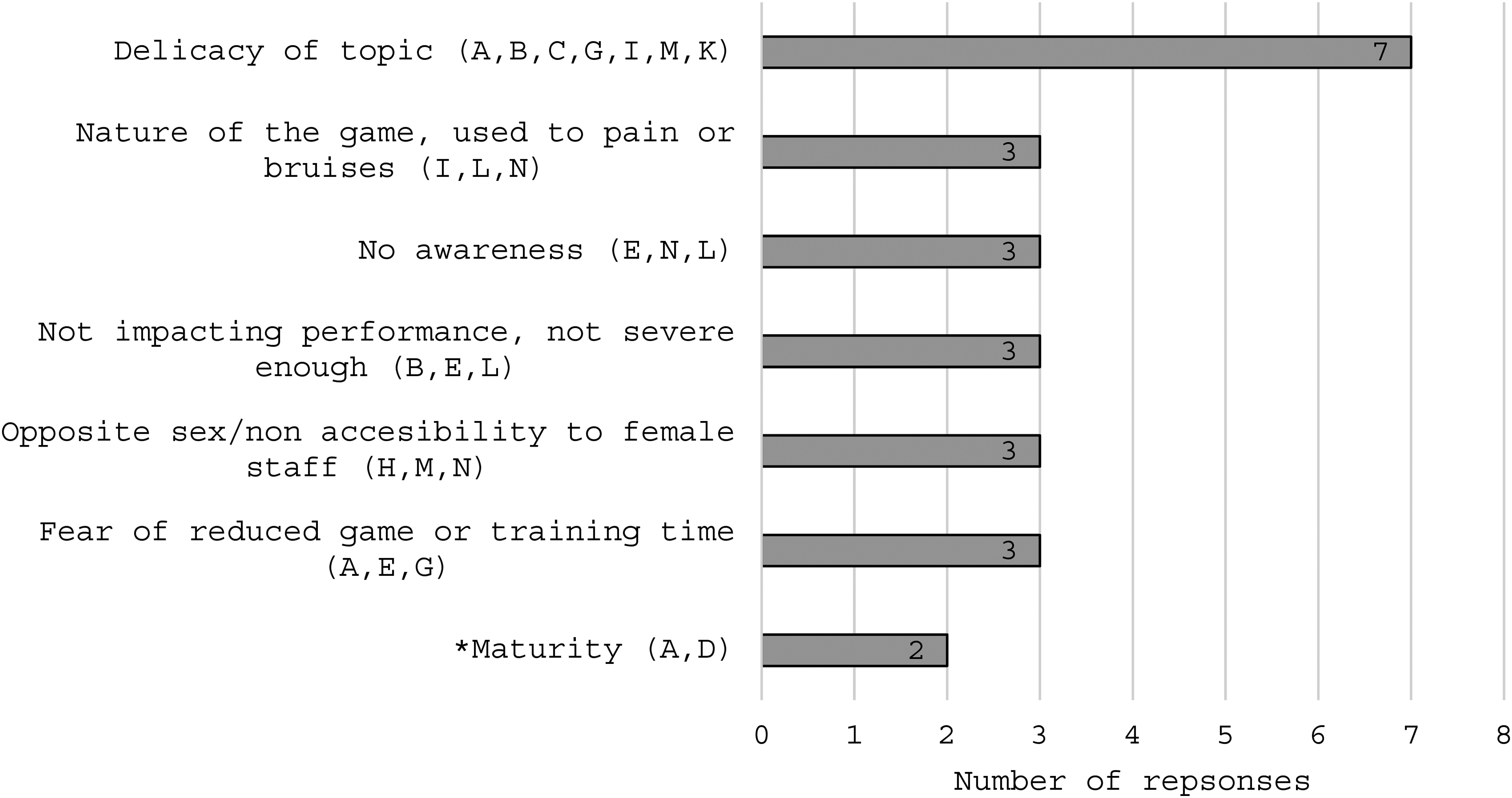
Proposed reasons for non-reporting of breast pain or injury. *Comments made regarding maturity included biological age and time being exposed to higher level of play (e.g., national level).
Accessibility to female staff
Access to female staff differed between levels of play, as those involved in the amateur level generally had less access (C, H) than those involved on a national level (I, L). When asking the sole interviewee involved in all three levels of play on his experience in this regard, he stated: From club to national is a big difference. You're looking at volunteers at club level and a lot more [females] are getting involved in the game [Rugby]. Like I said it is getting better over the last four or five years. Most recently say being involved with the Irish under eighteens, there were only two males out of a staff of about eight. (E)
One coach involved on the national level mentioned that the person chosen for a given position is the best fit for that role regardless of their sex. When asked if this is a privilege of the higher level of play, she responded: Yeah, absolutely. If you go into the club level it is generally parents or volunteers and generally it seems to be the male who volunteers into coaching roles anyway and that is starting to change. But it's going to be a long time before that fully transitions. I suppose a lot of the female roles are like managerial or a system with other things within the club, rather than actually coaching roles. So yes, I do think absolutely we're lucky in that. (A)
A positive trend of more female coaches, female S&C, and female doctors getting involved in women's Rugby in recent years was additionally mentioned by others (A, E, M). Apart from two participants, (F, G) the remaining twelve interviewees stated that existing or potential access to female staff would or did help players to report breast health issues and other female specific health concerns. Four of those twelve (A, D, E, I) further mentioned that this would especially be of relevance for younger and underage female players. Two players (M, N) stated that due to a high level of trust they would be comfortable to talk to their male physiotherapist about any issue.
Mitigation and treatment strategies for breast pain and injury
Protective equipment
Six (F, H, I, J, M, N) participants were aware of the wearing of sports bras for supportive purposes, while others (A, B, C, L) alluded to wearing multiple sports bras for this reason. The wearing of multiple sports bras was predominantly a method to stop excessive movement, but also to provide extra padding for contact protection: I have known of players who have worn multiple sports bras, but as far as I was aware it was more for sizing and to hold them in more than anything. (A) I would say both, I definitely heard it for reducing kind of exercise induced breast pain, but in terms of the contact injuries, yeah, they also use it for extra padding. (C)
One participant (C) further expressed scepticism that wearing one or multiple sports bras would provide any protection against direct contact or trauma to the breast. One physiotherapist (I) talked about considering protective padding which can be slipped into sports bras for the players. The wearing of shoulder pads which offered some sternal protection but not breast protection was also noted (A, H, M, N). It was further mentioned that these shoulder pads were developed for male players: Yeah, they would wear the sports bras and the shoulder pads as well. Especially they had to have protection up there on the chest [sternum], but then I have not asked why they are wearing this [sternum protection]. […] They probably look like they were developed for men's because they are way longer. I actually do not think I've ever seen a shoulder pad developed for women. (M) I know for my shoulder I would wear shoulder pads and the shoulder pads that I have happen to have, have a bit of padding on the chest, but it's definitely not for your breasts cause these ones are actually designed for men they're not designed for women, so it's more so for the sternum I would say than anything. And I haven't come across anything like specifically for breast protection, no. (N)
Four interviewees (D, E, G, K), all of them male, were unaware of any protective equipment such as additional clothing or padding.
There were no recorded reports of player selection being influenced by issues related to either CBI or EIBP.
Training modification
Nine of the fourteen interviewees were unaware of any training modifications by themselves or others due to CBI or EIBP. However, training modifications to several exercises causing discomfort to player's breasts were noted by the other respondents. These included adaptations to weight (G, F) and contact (C) exercises identified as problematic by players. Three interviewees (B, D, G) mentioned modifications to an exercise called body ball, to minimise the impact of landing on one's chest. Body ball can be described as a movement in which the player propels him- or herself forward, from standing or running, onto the ground with the ball being held close with both arms to the chest to then, when landed, recoil and present the ball towards teammates.
Provided treatment for breast pain and injury
According to five participants (J, K, L, D, F) who witnessed limited reporting of CBI or EIBP, they could not recall the specifics of any treatments. One coach (C) mentioned “(verbal) education” and “referral” when asked about treatment provided. One physiotherapist (I) noted that although players were sometimes assessed by the team doctor, typically no active medical intervention was deemed necessary. This participant noted that the lack of any active medical intervention was potentially problematic when player behaviours around future reporting was considered: […] if we have had a few people that present to us and the intervention is no intervention and they're females, they talk a lot, maybe that's influenced the other athletes will to come forward if they're like, well, actually there's nothing that can be done here or, you know, the assessment is let's see how it goes in a few days and maybe that's their strategy […] So, I think if there is no intervention, even though that could be appropriate, and you know it might actually stop them coming because they don't see the point in it. (I)
Future education on CBI and EIBP
All participants stated their interest regarding the future education on breast health issues in female Rugby players. Collected responses regarding preferences for various aspects of future education on breast health issues among coaches, S&C, physiotherapists and players can be seen in Figure 3. The three most frequent response themes for each question are shown in the diagram (Figure 3).
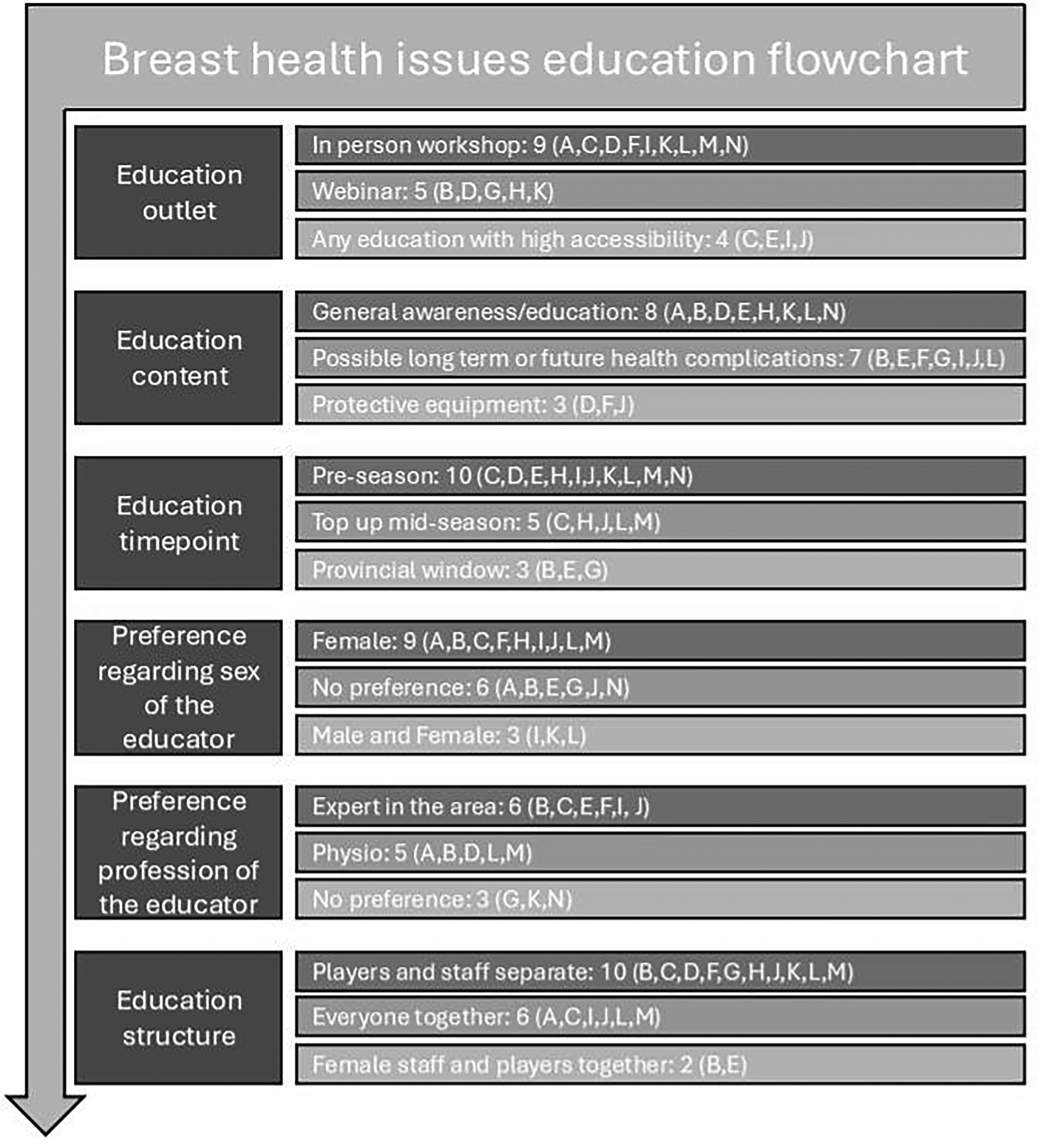
Breast health education flowchart informed by interview participant responses.
In person, pre-season workshops were preferred, led by female presenters and focussing on general awareness of breast health issues in rugby. Due to the sensitivity of the topic, one physiotherapist mentioned that preliminary education especially for players should be done in a safe environment without peer pressure: You can have Ice Breakers or different ways of how you can, you know interact with the athlete, but the bit that comes before that is making sure that the athlete is comfortable and what makes us comfortable is knowing a bit about the topic, knowing more about it, and if you can do that in a situation where athletes are in the comfort of their own environment. So it could be that there's an online learning first, you know, this is breast health, this is breast pain. These are the injuries that experience in Rugby, and you got to keep bringing it back to health, important for all of us. (I)
With regards to the preference of a same sex educator, three interviewees (A, B, I) mentioned that player maturity would be of relevance. Maturity included biological age and time being exposed to higher level of play.
Discussion
Current literature regarding breast pain and injury in Rugby environments is limited.15,20 Results of the current work and supported by other pertinent research8,20,30–32 indicate a systemic absence of knowledge and awareness about CBI and EIBP and their potential future health complications. This paucity must be addressed to improve health and performance among female athletes.
Only half of the fourteen interviewees were aware of either CBI or EIBP, despite the cohort including three female players and six female support staff. The lack of awareness of breast health issues amongst interviewees matches the comparable study concerning support staff involved in Rugby codes and Australian Football. 21 Breast pain and injury in our study were explained as being “just the nature of the game”. This attitude may be aligned to socialisation in Rugby environments and associated androcentric subcultural values of being tough and physical. 33 This could potentially also explain the minimisation of breast pain or injury in training or match scenarios, and a reluctance to report same to support staff. The underreporting of breast health issues due to fear of reduced game time, lacking injury awareness, and symptoms of not being deemed severe enough are a documented phenomenon. 34 Other studies on CBI amongst professional basketball players, 32 elite water polo players, 31 college athletes, 30 elite female athletes 35 and contact football players 21 showed similar indications. These records can be seen as similarities to findings in this current study on assumed reasons for the under or non-reporting of breast health issues among female athletes. Topic delicacy was mentioned by 50% of interviewees as the biggest perceived reporting barrier which concurs with other research on female athletes, involving the menstrual cycle, urinary incontinence and breast health issues.34,36,37 Similarly, a reluctance to report an injury that is not impacting performance or perceived to be serious, is known through previous work including urinary incontinence37,38 and breast health issues.32,34 The potential impact of failing to recognise, and appropriately manage breast pain and injury, could have long standing health repercussions as well as impacting short-term performance and player wellbeing. The scale and extent of these repercussions may only be truly apparent as women's Rugby matures as an elite, widely played sport.
The positive development of female athletes involved in Rugby 3 and sport overall 1 does not necessarily transfer to female representation amongst support staff such as coaches, S&C, and physiotherapists within female sport. Males generally outnumber females in roles such as head athletic trainer 39 and sports physician. 40 In Ireland and the United Kingdom (UK) similar patterns are evident, as coaches working in women's Rugby Union are predominantly male. 18 When it comes to injury management, this status quo can be seen as problematic as it conflicts with a documented preference of female athletes to report injuries to someone of the same sex. 16 It is crucial for optimal injury management that supportive and trusting environments where athletes feel comfortable reporting any type of injury, are established. 41 This is even more pointed when considering female specific issues such as menstrual cycle, pregnancy and postpartum return to sport as well as breast health issues, 15 as there might be an additional level of delicacy involved. 17 The study found that access to female staff is better at provincial or national level compared to amateur level primarily due to greater numbers of staff at these levels. Higher levels of play are generally better financed and thus can recruit chosen staff regardless of gender, while amateur sports lack this flexibility. Female volunteer coaches in Western amateur settings face many barriers, including limited access to external resources, role conflicts, gender category sorting, low retention rates, and lack of organisational support. 42 One coach noted potential gender category sorting as women are often placed in managerial roles instead of coaching. Nonetheless, and regardless of the level of play, interviewees mentioned that access to female staff would be helpful overall when it comes to the reporting of breast health issues.
To prevent excessive breast movement and accompanying pain, the wearing of multiple sports bras was the most frequently documented prevention strategy. Wearing of multiple sports bras aims to compress the breast tissue, thus reducing breast motion and accompanying discomfort. 43 Education to limit the usage of ill-fitting sports bras with limited support has also been proven to be beneficial in reducing EIBP. 44 There was no consensus amongst participants in this study whether multiple/padded bras provided any protection from contact forces. Current studies acknowledge a lack of research and awareness of protective equipment to prevent or reduce CBI among female Rugby players, 20 and infrequent use among female athletes overall. 6 Limited awareness of existing protective equipment for CBI was recorded. Interviewed players mentioned that shoulder and chest pads which seemingly have been developed for male Rugby players have been utilised by some female players. This finding does not come as a surprise as previous work in this area have found congruent results. 45 This additionally confirms the previously documented necessity of further research on protective breast equipment for female contact athletes. 46 Although the findings of this study did not reflect any impact of CBI or EIBP on player selection, it should be noted that performance decrements due to breast pain and injury have been noted in other studies,8,30,31,35 which may impact directly on player performance and subsequent selection.
Training modifications to several exercises and techniques reflect the impact that CBI and EIBP have on the player. These modifications reflect indirect acknowledgement of breast health issues in female athletes and should form part of the narrative when optimising wellbeing in female athletes across all codes.
The non-provision of an active medical intervention, which was mentioned by one physiotherapist could be seen as challenging. In team environments players communicate with each other and potentially do not see the need of reporting pain or injury when there appears to be no treatment options available. Therefore, more research on this finding is needed to confirm its assumed relevance to increase future reporting and recording of CBI and EIBP.
All interviewees showed interest regarding future education on breast health issues indicating a paucity of knowledge on this topic. Workshops carried out during pre-season on breast health content were the most preferred options among interviewees reflecting timelines and approaches utilised elsewhere for injury prevention programs. 47 Due to topic delicacy and the associated reporting barrier the preference of in-person education by a knowledgeable female was favoured. Educational content focused on the general information about the causes, implications and importance of reporting CBI and EIBP were amongst the topics identified as important in this cohort . A focus on foundational knowledge in this area mirrors comparable approaches to education in the areas of stress urinary incontinence and the return to play after postpartum in female Rugby players.4,5,48 The noted preference of educating players and support staff separately leaves room for discussion. Options to offer player-only educational sessions recognise the potentially sensitive nature of the subject matter. However, decisions on this approach would depend on the age, maturity and preferences of the specific cohort. Opportunities may exist for shared learning in other instances where all parties are comfortable to do so. Results also indicate that bespoke training on breast health issues for support staff and clinicians of both sexes would further empower end encourage open discourse on the topic between players and staff.
Limitations
It may be argued that the representation from an amateur level of play underrepresents the actual number of female amateur players in Ireland as these outnumber their provincial and national counterparts. Even though we had a six to five split favouring female coaches, physiotherapists and S&C, this does not reflect the landscape, and topic knowledge, in women's Rugby in Ireland as it is still predominantly a male-dominated environment. Further limitations were the investigation of a single country which therefore includes culturally specific findings. Albeit the study included a small sample size, the involved researchers were able to agree on data saturation.
Conclusion
Overall limited knowledge and awareness on CBI and EIBP and their potential future health complications among stakeholders in Rugby in Ireland was recorded. There is a reporting barrier of topic delicacy which needs to be addressed in order to create an open and engaging environment in which breast pain and injury can be reported freely by female athletes. This study further reported a lacuna of reporting and treatment options among support staff for breast health issues. This work has conveyed that protective measures are not yet evidence-based and require thorough future investigation. Quintessentially, this work indicates the necessity for elementary education of female Rugby players, coaches, S&C and physiotherapists on breast health issues such as CBI and EIBP. Targeted education is required to address concluded issues and should embody the preferences of potential stakeholders to optimise the impact of such educational interventions. This qualitative study confirmed various aspects of previous quantitative studies while identifying several nuances which are deemed to be of relevance for future research.
Footnotes
Consent to participation and publication:
Interviewees provided written informed consent prior to participation.
Data availability statement
N/A.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical consideration
This study has been approved by the University of Limerick Education and Health Sciences Faculty Ethics Review Board Code: 2016_06_19_EHS.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors of this study are in receipt of funding from the Irish Rugby Football Union (IRFU) for elements of this research. The funders had no input in the review process or writing.