
Abstract
Competitive cyclists may be vulnerable to disordered eating (DE) and eating disorders (ED) due to perceived body composition optimisation and external influences within cycling culture and from stakeholders. Therefore, this study aimed to assess DE and ED risk in competitive cyclists using the Eating Attitudes Test (EAT-26), explore differences in responses based on sex, discipline and level of competition, and to gain insights into contributing factors towards DE via open-ended survey questions. In total, 203 participants completed a mixed-method questionnaire. Eating disorders were reported by 5.7% (n = 11) of participants, with three being historic cases. The median (inter-quartile range) EAT-26 score was 8 (12) of a total possible score of 78. Disordered eating risk was observed in 16.7% of participants due to an EAT-26 score ≥20. Female participants had significantly higher scores than male participants (12.5 ± 17.5 vs. 6.5 ± 10.0; p = .004). There was no significant difference between road cyclists and off-road cyclists (7.0 ± 13.25 vs. 8.0 ± 10.5; p = .683). There was a significant difference in scores between novice/club/regional and national/elite/professional cyclists (6.0 ± 11.25 vs. 10.5 ± 12.0; p = .007). Thematic analysis of open-text responses found that the social environment of competitive cycling contributed towards DE behaviours and body image issues. These findings indicate competitive cyclists do appear to be an ‘at risk’ population for DE/ED. Therefore, there is need for stakeholders to enhance nutritional services, nutrition education and create supportive athlete environments.
Introduction
Eating disorders (ED), such as anorexia nervosa, bulimia nervosa, binge eating and EDs not otherwise specified, are characterised as severe psychiatric disturbances that cause persistent disruption to eating behaviours and body image perception resulting in significant impairment to physiological health and psychosocial functioning.1,2 Disordered eating (DE) behaviours such as purposively skipping meals, restricting overall energy or macronutrient-specific food intake, purging and use of medications can range in severity and may predict the onset of clinical ED development, contributing to their early prevention and/or treatment. Eating disorders are a global public health issue, with 8.4% and 2.2% lifetime prevalence across 33 general population studies in males and females, respectively. 3 Common risk factors such as cultural exposures and expectations, low self-esteem, depression and anxiety and genetic vulnerability can also contribute to their development. 4 Moreover, rates of ED are increasing in the general population internationally, 3 particularly amongst younger people. 5 This is concerning given the health issues associated with EDs 6 and that EDs are associated with some of the highest rates of mortality when compared across mental health disorders. 7
Athletic populations have been identified as cohorts that may be particularly ‘at risk’ for ED and DE. 8 Training and competition demand result in increased energy expenditure meaning athletes have elevated energy, macronutrient and micronutrient requirements to ensure optimal health and well-being and substrate availability for fuel and structural adaptations. 9 Whilst manipulation of dietary intake to enhance training or body composition adaptations are often standard practice in sporting contexts, reducing energy intake without consideration for exercise energy expenditure can result in detrimental low-energy availability (LEA)10,11 and may result in DE behaviours being adopted and the development of a clinical ED. 12 Competing in weight-sensitive sports, engaging in sport-specific training prior to body maturity, performance pressures, injury and team culture may present specific DE risk factors within athletic environments. 4 Given the likelihood of EDs and DE being present to a greater extent in athletic populations,8,13 the risk of LEA and the associated detriments to health, well-being, performance and injury risk are enhanced14,15 and warrant continued focus from researchers and practitioners in sport.
‘Competitive cycling’ as an umbrella term encompasses a range of disciplines including road, track, BMX, cyclo-cross and mountain biking with heterogenous training and competition demands. 16 Large training and competition volumes in cycling, particularly road-based disciplines,17,18 are likely to result in energy expenditures that are difficult to compensate for via dietary intake. 14 Additionally, the desire to maintain a high power to weight ratio may contribute to inadequate dietary intake. Given this, LEA may occur 19 and potentially develop into Relative Energy Deficiency in Sport, characterised by impaired metabolic rate, menstrual function, bone health, immunity, protein synthesis and cardiovascular health in response to LEA.11,20 Whilst LEA may be an unintentional consequence of high energy expenditure relative to intake, it may also occur because of DE behaviours or EDs. 19 The specific demands of cycling disciplines may increase the likelihood of an athlete developing DE behaviours and/or clinical EDs 21 with concerns being raised for ED and DE in competitive cycling, particularly in road cycling. 22
Available research highlights some factors which may influence ED and DE in cycling. Cyclists have self-reported that reductions in nutrient intake are pursued to improve performance, whilst also describing fatigue, illness and injury. 23 Moreover, external influences from practitioners can influence eating behaviours. For example, coaches may not engage with registered nutrition professionals, display a lack of knowledge and appreciation for the importance of nutrition for health and performance and promote sub-optimal eating behaviours. 24 Furthermore, the social environment and culture of competitive cycling may contribute to DE behaviours, 25 with inappropriate comments from support staff and team-mates and a strong focus on body weight for performance purposes influencing an individuals’ eating behaviours and relationships with food.4,19,26,27
Studies have previously described the prevalence of DE behaviours in competitive cycling samples using a variety of self-reported tools such as the Eating Attitudes Test (EAT-26), Eating Disorder Examination Questionnaire and Brief Eating Disorder in Athletes Questionnaire.14,28,29 When using the EAT-26, a score of 20 or greater is indicative of concerning eating behaviours, and potentially a clinical ED.30,31 Previous research has distributed the EAT-26 amongst male32–34 and female competitive cyclists, 35 with studies being distributed in French32,33 or undocumented international populations.34,35 Findings are varied, however, a considerable number of respondents demonstrated susceptibility to DE, with an EAT-26 score of >20 reported by 57%, 32 32% 35 and 20% 34 of cyclists.
Despite this small body of work, much of the research in the area is heterogeneous in terms of level of cyclists studied, cycling disciplines engaged with and inconsistencies existed in the level of reporting of demographic and training information.14,29 This may limit the ability to understand how information such as the competitive level, cycling discipline and training volume may influence DE behaviours. Furthermore, there has been very limited qualitative research, and previous survey-based studies have infrequently obtained qualitative data alongside quantitative measures such as the EAT-26. Without this information, a richer understanding of the context behind potential DE behaviours is not possible. The primary aim of this study was to quantify DE and ED risk in a global sample of competitive cyclists using the EAT-26 and compare responses between sex, discipline and level of competition. A secondary aim of the study was to obtain self-reported information related to cycling and nutrition provision from organisations the participants may be affiliated with, as well as to gain greater contextual understanding of what may contribute to the risk of DE behaviours in competitive cyclists.
Methods
Study design
A cross-sectional questionnaire was used to assess and explore DE behaviours in a cycling population using a mixed-methods approach. The questionnaire was self-reported, anonymous and distributed online allowing participants to complete it in their own time and in private. This approach was deemed most appropriate to achieve the research aims due to the nature of the research area. Ethical approval was provided by the University of Northampton Faculty of Arts, Science and Technology Research Ethics Committee (FAST-REC 222321).
A participant information sheet was provided on the first page of the questionnaire. If participants did not select that they provide informed consent following consideration of the participant information sheet, they were unable to proceed to the questionnaire. Due to the sensitive nature of the research area, support resources were provided for participants at the end of the questionnaire should they feel they are affected by this topic.
Participants
Participants were recruited using convenience sampling via the distribution of the questionnaire through social media (Facebook, Twitter, LinkedIn and Instagram) and through personal networks of the research team. The study invited cyclists that were 18 years or older and self-described as competitive based on total training volume per week (≥6 h per week), as defined by McKinney et al. 36 Whilst the definition from McKinney et al. 36 includes ‘official competitions’ in the criteria, the questionnaire was open to cyclists based on the volume of activity only given that pseudo-competitive cycling groups may operate outside of conventional sporting structures. 37 There were no further inclusion criteria to our participant recruitment strategy. The questionnaire was simply advertised as exploring ‘Eating Behaviours of Competitive Cyclists’, with no reference to ED or DE in advertising to reduce risk of bias in those completing the questionnaire.
Materials
The full questionnaire can be viewed in Supplementary Materials 1. The questionnaire was designed amongst the research team and consisted of three sections. The questionnaire was inputted and completed on an online questionnaire-hosting website (Microsoft Forms, Microsoft, Redmond, WA, USA). Section 1 obtained demographic information along with primary racing disciplines, years of racing, experience level and primary country of racing. Section 2 contained the EAT-26 to assess eating attitudes, behaviours and beliefs and outlined our primary outcome measure for the study. The EAT-26 comprises of 26 eating attitude questions and five behavioural questions. The instrument is not able to clinically diagnose an ED but provides a screening tool to identify behaviours that may suggest an increased risk. The EAT-26 has been used in previous studies in athletic and non-athletic populations,38–40 allowing comparison and outlining the rationale for its selection in this study.
When completing the EAT-26, participants were required to select a response from five options (always, usually, often, sometimes, rarely and never). Participant responses to each of the 26 items were scored to yield the individual's EAT-26 score, with possible scores ranging from 0 to 78. A score of ≥20 has been demonstrated to correctly classify 83.6% of individuals with anorexia nervosa and is used to provide basis for referral to a medical specialist. 31 Previous studies have suggested scores ranging from 10 to 19 indicate trending towards potential DE behaviours. 35 Section 3 of the questionnaire included additional cycling-specific open-text questions to supplement the EAT-26 and provide greater context to any findings. These questions were constructed based on the research team's expertise and experience in cycling, as well as findings from a recent scoping review on ED and DE in competitive cycling. 29 Following completion of the questionnaire, participants were encouraged to seek further specialist support if they felt they were affected by the topics covered in the questionnaire and were provided with a link to further information and support services on EDs or DE.
Data analysis
Quantitative data were analysed using SPSS (Version 29, IBM Corp., Armonk, NY, USA). Descriptive statistics were generated to present differences in EAT-26 scores between sex, discipline and level of competition. To compare between disciplines, participants who competing in road-based disciplines were grouped and compared against ‘off-road’ disciplines due to a low response rate from other disciplines. For comparison between level of engagement in competition, participant responses that included the highest level of competition were grouped (novice/regional/club and national/elite/professional). Data were deemed to be non-parametric via Kolmogorov–Smirnov testing and thus, an independent-samples Mann–Whitney U test was applied to compare EAT-26 scores between sex, discipline and level of competition. Statistical significance for all tests was accepted at p < .05. Demographic data are presented as mean ± standard deviation, and EAT-26 response data are presented as median ± inter-quartile range.
Qualitative data obtained from the open-text questions were analysed using thematic analysis. The six-stage process outlined by Braun and Clarke 41 was followed, with analysis led by JH. All open-text responses were extracted and collated into a Microsoft Excel spreadsheet and JH then read through all responses to familiarise himself with the dataset as a first analytical step. Data were then coded in line with one of our research aims of seeking to understand factors that may contribute to the risk of DE behaviours in competitive cyclists. JH then grouped coded data into sub-themes and shared this process with CJR for insight and alternative perspectives on the data. Next, JH and CJR developed over arching themes which captured recurrent patterns in the data. These themes were then further refined through a cyclical process of moving between existing literature and our data to build a synthesis from the data which was connected to key concepts in previous research related to ED/DE within sporting settings. The proposed themes were then shared with all authors, alongside the supporting data, to check agreement and authors acted as ‘critical’ friends 42 in encouraging JH to consider his positionality and interpretations of the data. The final stage involved re-assessing the themes against the dataset to ensure internal coherence had been maintained. 41 Each theme is presented alongside contextual key concepts and literature which informed the analysis as well as extracts of supporting data.
Results
Descriptive overview
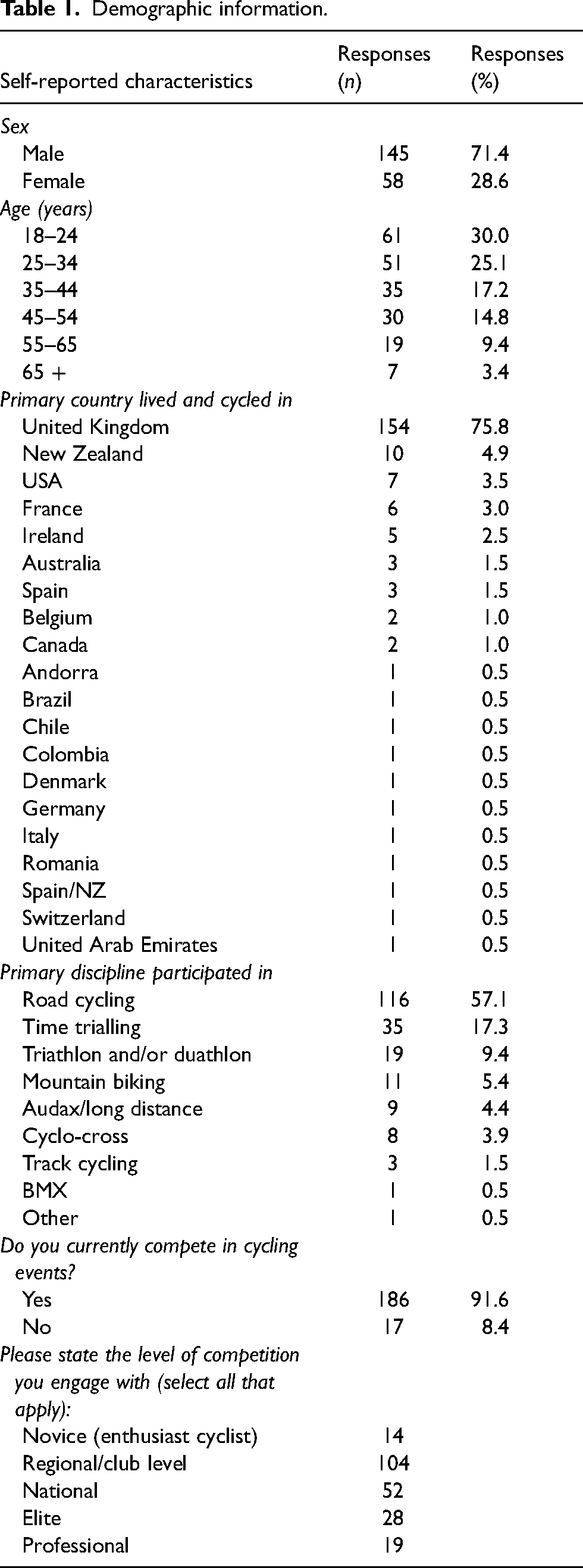
A total of 203 cyclists completed the questionnaire. Participant demographic information is presented in Table 1. Stature (176.4 ± 9.1 cm; n = 201) and body mass (70.7 ± 11.3 kg; n = 202) were self-reported by participants. Most participants (n = 144; 71.4%) reported being a member of a cycling organisation. Of these, 17 (11.7%) report having weekly contact with a nutritionist or dietician and 69 (47.6%) report receiving nutrition support from their organisation.
Demographic information.
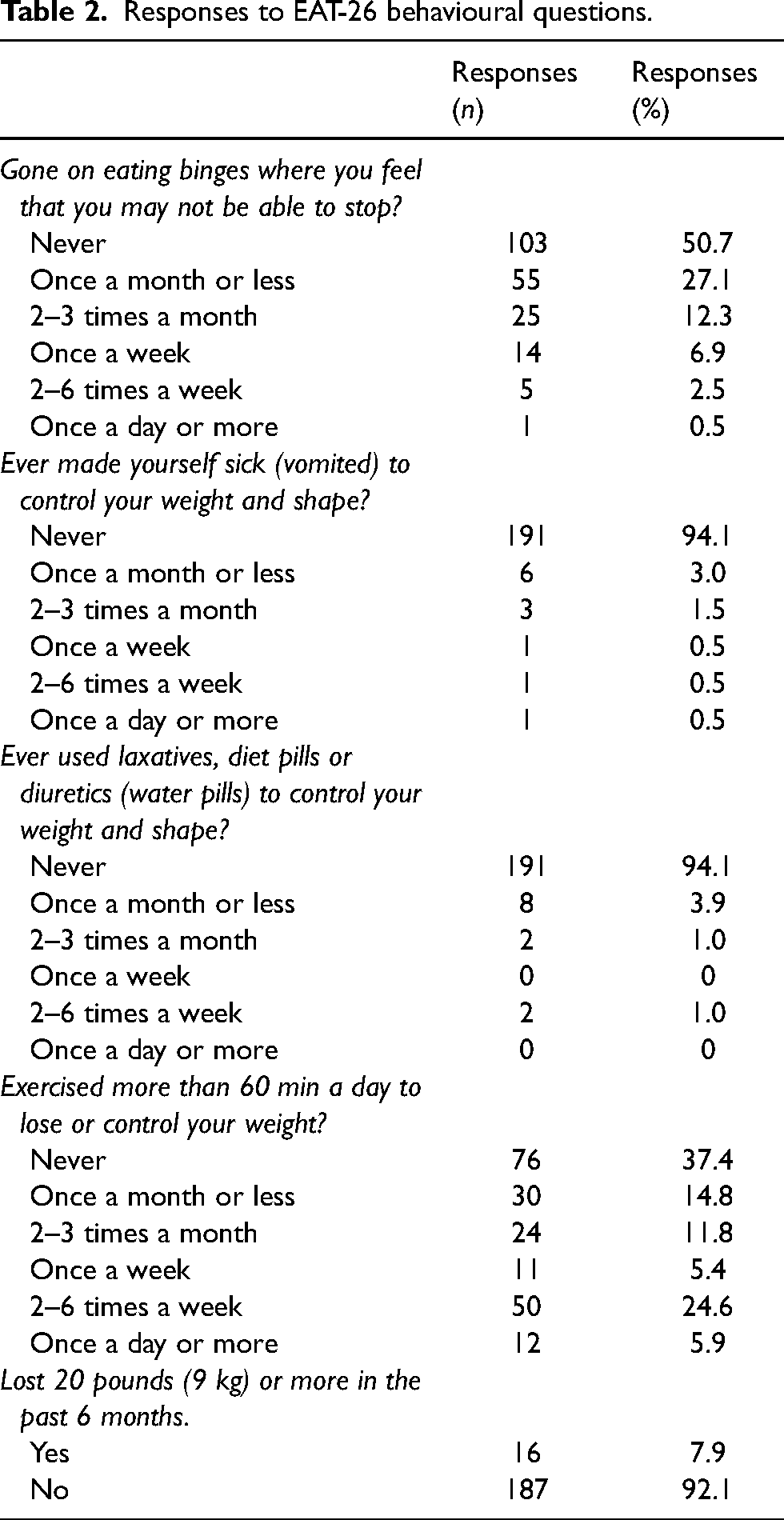
Overall median EAT-26 scores for the sample were 8.0 ± 12.0, with 34 (16.7%) participants scoring equal to, or greater than, the cut-off of 20 that is reported as reflective of DE. 31 An ED diagnosis was reported by 11 (5.4%) participants. These were reported as anorexia nervosa (n = 6, 3.0%), anorexia nervosa and exercise addiction (n = 1, 0.5%), bulimia nervosa with anorexia nervosa tendencies (n = 1, 0.5%) and three (1.5%) reported as being historic (anorexia nervosa, n = 2, 1.0%; bulimia nervosa, n = 1, 0.5%). Responses to the EAT-26 behavioural questions are displayed in Table 2.
Responses to EAT-26 behavioural questions.
A significant difference in EAT-26 score was observed based on sex, with female participants reporting a significantly greater score than male participants (12.5 ± 17.5 vs. 6.5 ± 10.0; p = .004; Figure 1). There was no significant difference between road cyclists and off-road cyclists (7.0 ± 13.25 vs. 8.0 ± 10.5; p = .683; Figure 2). There was a significant difference between novice, club and regional cyclists (n = 96) and national, elite and professional cyclists (n = 90) in EAT-26 scores (6.0 ± 11.25 vs. 10.5 ± 12.0; p = .007; Figure 3).
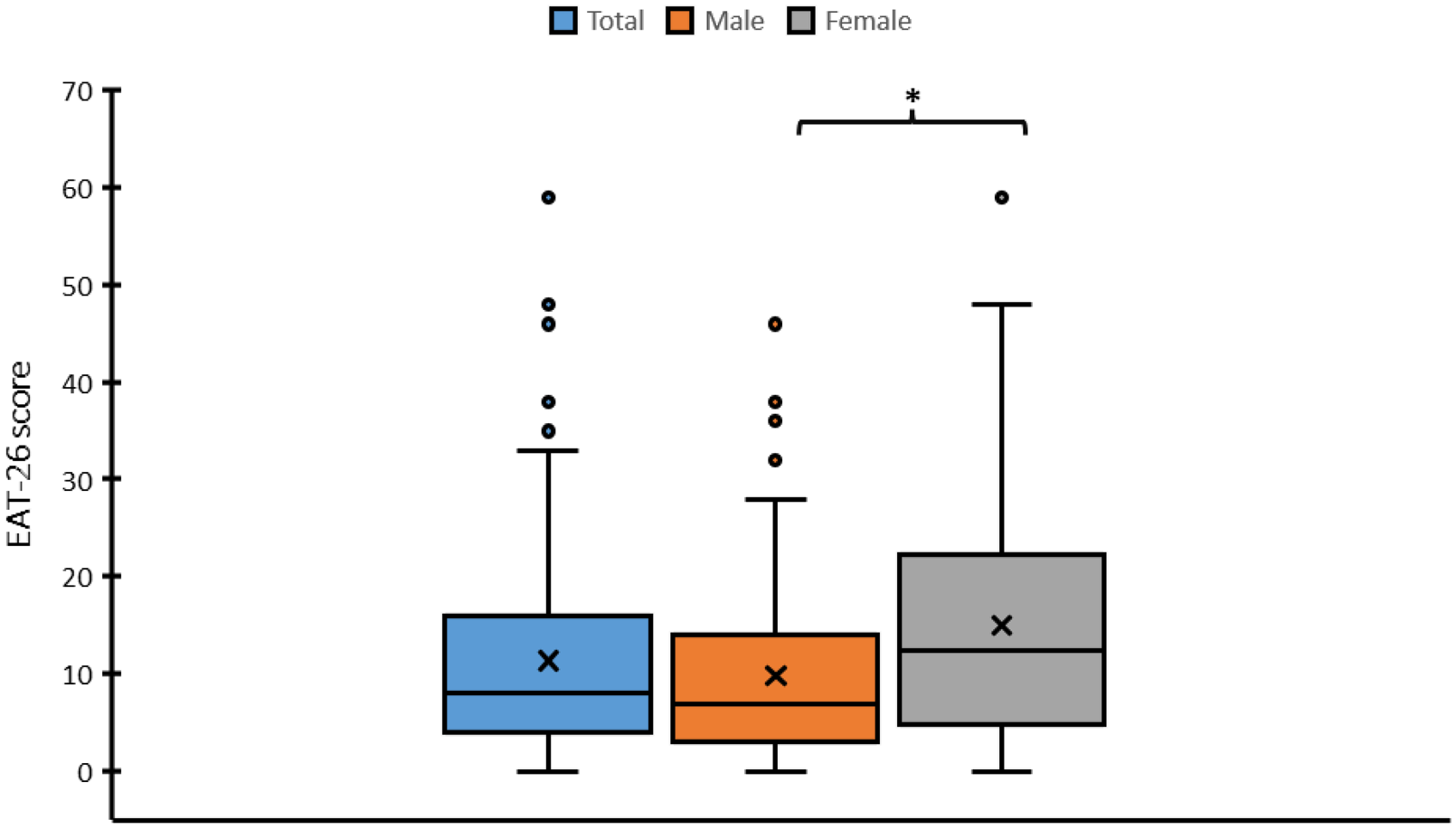
Differences in Eating Attitudes Test (EAT-26) scores between total, male and female respondents. * denotes significant difference.
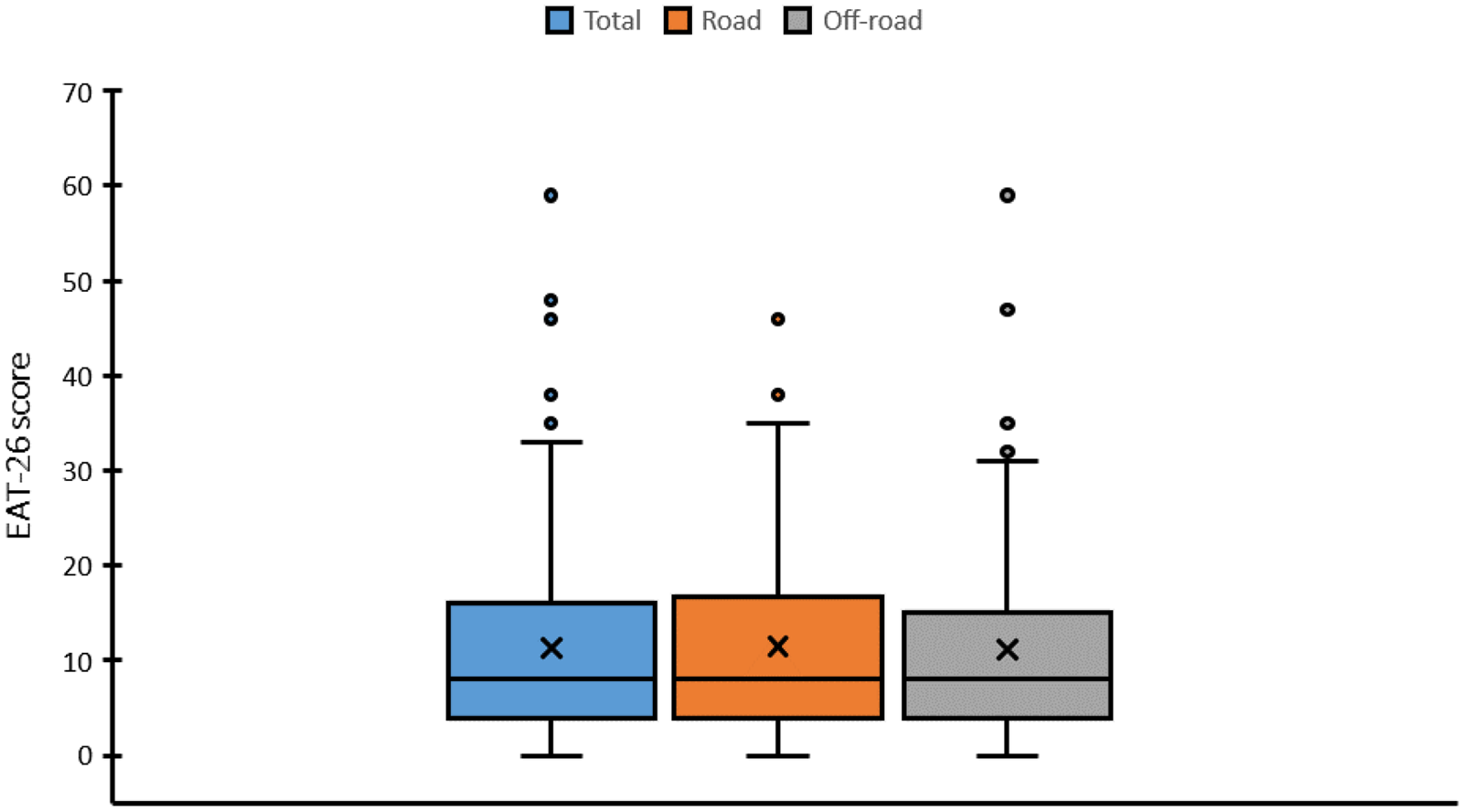
Differences in Eating Attitudes Test (EAT-26) scores between total, road and off-road cyclists.
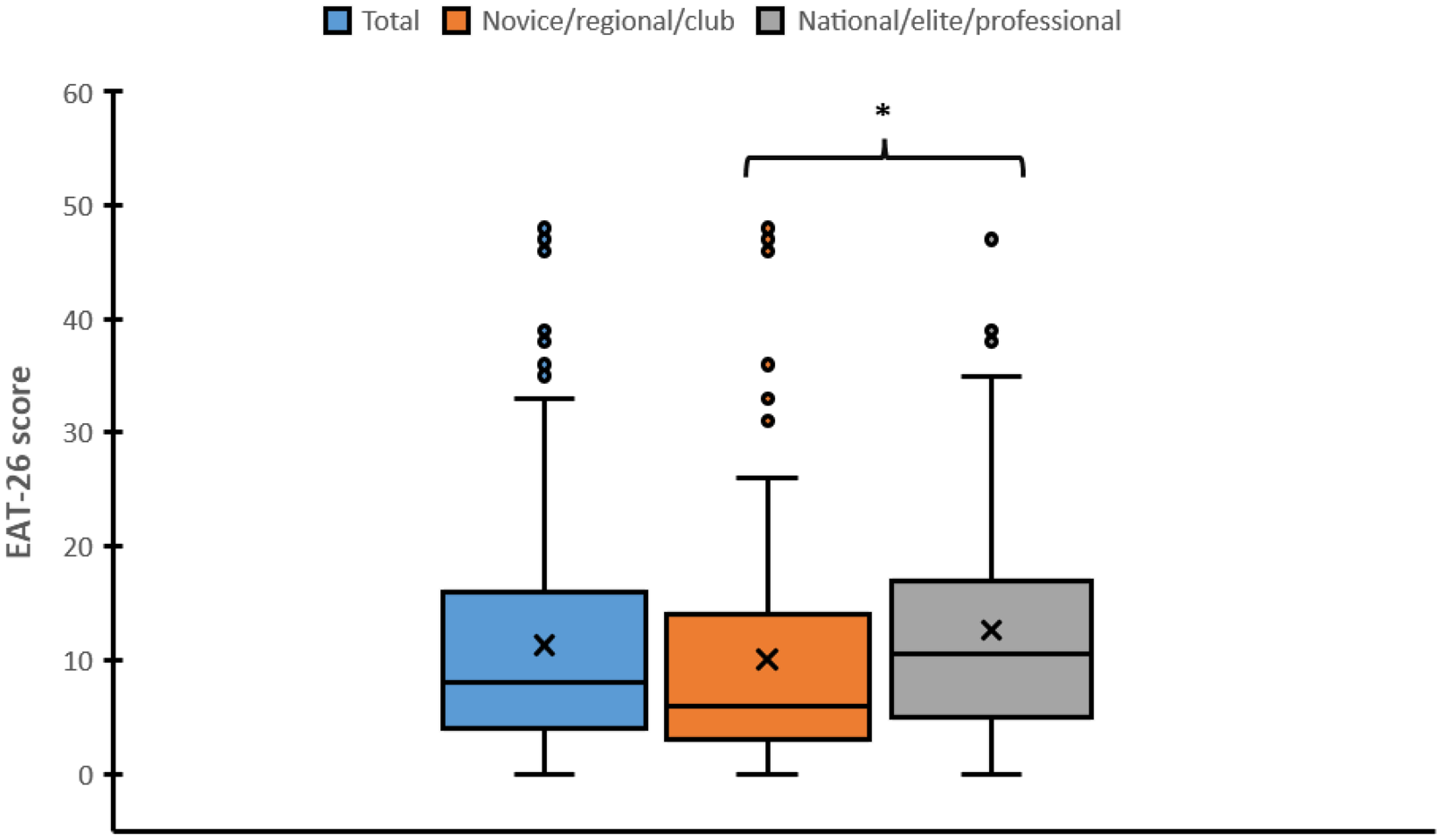
Differences in Eating Attitudes Test (EAT-26) scores between total cyclists currently competing (n = 186), novice/regional/club level and national/elite/professional respondents. * denotes significant difference.
Participants were asked the following, ‘Please select your level of agreement with the following statement: “Competitive cyclists are a weight-conscious population”’. Responses were as follows: ‘Agree’ (n = 94, 46.3%), ‘Strongly Agree’ (n = 81, 39.9%), ‘Neutral’ (n = 18, 8.7%), ‘Disagree’ (n = 5, 2.5%) and ‘Strongly Disagree’ (n = 5, 2.5%).
One hundred and four (51.2%) participants reported experiencing comments in a cycling context (e.g., at races, on rides, amongst peers) regarding their body weight. One hundred and twenty four (61.1%) participants indicated they had felt pressure, personally, to be a certain weight for cycling and 110 (54.2%) reported that they had purposefully manipulated their body weight for reasons associated with cycling in the past 12 months.
For the question ‘Have any of these individuals ever given you advice regarding your diet? Select all that apply:’ coach (n = 83, 40.9%), friends (n = 71. 35.0%) and family (n = 62, 30.5%) were the most frequently reported. When asked to select the top three sources of information relied on, and trusted, for nutrition information, participants responded with ‘academic journal’ (n = 87; 42.9%), ‘nutritionist’ (n = 80; 39.4%) and ‘coach’ (n = 66; 32.5%).
Thematic analysis results
Following a thematic analysis of the open-text responses, three themes were generated to represent the data: (1) Pressure to be a certain weight for cycling, (2) Peer comments on body weight and, (3) The performance focus and culture of competitive cycling. In the following section, we outline each theme which, when taken together, provide an overview of the various influences on eating habits and body image reported by the cyclists.
Pressures to be a certain weight for cycling
Previous research has highlighted that weight-sensitive sports, such as many competitive cycling disciplines, can contribute to an environment whereby athletes feel various pressures to reach certain body weights to optimise performance. 4 With that in mind, it is perhaps unsurprising that 124 (61.1%) of the questionnaire respondents reported feeling pressure to being a certain weight for cycling. Of these participants, 114 (91.9%) provided responses detailing where they felt this pressure came from. Athletes embodiment of attitudes and feelings of pressures to have a certain body is influenced by a range of social processes, 13 including pressures from coaches and associated staff to maintain a low body weight to maximise athletic performance.43,44 The interplay of influences on pressure to be a certain body weight resonated with our data.
Whilst some of the responses framed pressures to be internally driven, and because of their ‘Desire to win’ (M, 45–54, Road Cycling), most identified external factors which were reported to place pressures on being a certain body weight. Comparison to other competitors was particularly prominent, with examples including ‘How my competitors look in relation to how I look’ (F, 45–54, Mountain Biking) and ‘Everyone else being lighter than me’ (M, 18–24, Road Cycling). Reference to team managers, coaches and directeur sportifs was made across participants competing towards the higher ends of the sport as sources of pressure to be a certain weight. Some examples include: ‘Team owner saying I need to drop weight to be more competitive; statement I believe is true for cycling so I agreed with him and felt a reminder to watch what I am eating’ (F, 18–24, Road Cycling) ‘Comments about my leg size and in the past about how small I was so that was why I was good at climbing. Other comments not about me but made to me include ‘look at her and how hollow her cheeks are that means she will go well’ (made by my team manager).’ (F, 18–24, Road Cycling) ‘The pressure to perform for a sponsored team, or to be selected.’ (F, 25–34, Road Cycling) ‘This came from our cycling body Cycling Ireland, during lockdown they were monitoring Zwift racing, power and weight. I had to do a weigh in and email it in. At the time I was very self-conscious of doing this, I don’t think it would bother me now’ (F, 35–44, Road Cycling) ‘Social Media and fellow riders’ (M, 25–34, Road Cycling) ‘Myself primarily, but stems from watching cycling content where w/kg is a badge of honour.’ (M, 35–44, Road Cycling) ‘Media, other people's ftp [functional threshold power] and needing to match their watts per kilo, seeing other competitors at events and not looking like them’ (F, 25–34, Time Trialing) ‘From professionals seen on TV’ (F, 18–24, Road Cycling)
Peer comments on body weight
In the general population, extant research shows an associated between experiencing negative appearance-related comments from peers and an increased risk for body dissatisfaction, DE behaviours and psychosocial issues.47,48–50 These findings extend into athletic populations, with research suggesting that experiencing negative comments on physical appearance from those within an athletes network – such as coaches, teammates, competitors and parents – influenced the development or increased the problem of EDs and DE.51,52
With this context in mind, a total of 104 (51.2%) of our participants reported experiencing comments in a cycling context (e.g., at races, on rides, amongst peers) regarding their body weight. Of these participants, 88 (85%) responses were received providing insight on the context and personal reaction to the comments. The cyclists reported experiencing a wide range of comments on body weight, with reference to comments such as ‘Chonky boy’, ‘Fat bastard’, ‘Big guy’, ‘Carrying winter weight’ and ‘You are too fat’. Many of the participants stated having negative emotional responses to comments they had received regarding their body weight. Examples include: ‘Someone important said to me “I thought you were thinner”. In that moment I said nothing but it felt like the end of the world. That day changed everything because I start dieting and control everything that I eat and do.’ (F, 25–34, Road Cycling) ‘Big legs, thunder thighs, made me sort of proud but also sad and self-conscious’ (F, 25–34, Time Trialing) ‘In France being told I was too heavy to get up the hills. It felt horrible’ (F, 18–24, Road Cycling) ‘When you're lean and you can see veins, muscles and bones there is praise.’ (M, 18–24, Road Cycling) ‘I received a lot of praise from cyclists about weight loss and how this made me “look like a proper cyclist now”’ (F, 25–34, Road Cycling) ‘When at a lower weight had comments praising my weight and encouraging me to not gain weight.’ (F, 18–24, Triathlon) ‘Usually it's when you are thin “you look fit” so thin is good and fit.’ (M, 45–54, Road Cycling) ‘Being ‘lean’ was seen as a huge positive and derogatory comments were made about those who weigh more/ present as overweight’ (F, 25–34, Road Cycling)
This theme has highlighted that, from our data, it appears that the subcultures these participants were apart of were based on ideas and behaviours which negatively stigmatised certain body types and weights, whilst positively reinforcing ‘leanness’ and being ‘skinny’. Our data cannot speak to the direct relationship of such processes and the impact of comments on DE risk but we can infer it may have a negative influence in line with previous research.51,52
The performance focus and culture of competitive cycling
The culture of performance focused sport, across competition levels, is imbued with a ‘discourse of excellence’ which manifests in an environment in which a win at almost all costs attitudes prevails and behaviours and attitudes are predominantly organised around improving performance.
57
In our data, the culture around competitive cycling and how much of it is driven by a performance focus was highlighted as a source of pressure for being a certain body weight: ‘Culture at local level all the way up to professional’ (M, 25–34, Mountain Biking) ‘Lower weight = faster is a common phrase, from the media and also from coaches’ (M, 18–24, Triathlon) ‘The entire cycling culture. Fellow athletes competing with each other to eat less/be leaner. Coaches/directors/national federations (selecting teams) ignoring the problem. All those individuals and fans who comment on how “fit” you look when underweight.’ (F, 45–54, Cyclo-Cross) ‘To fit an image displayed by others’ (F, 18–24, Triathlon) ‘I know it won’t help performance, but the back of my mind says it's not worth the risk to not try to weigh less. I am fairly new to competitive cycling so I want to fit the image of a cyclist to avoid further exclusion from the community beyond my inexperience.’ (F, 18–24, Road Cycling) ‘Cycling is, fundamentally, a power to weight sport, but I think sometimes this has become a bit of a preoccupation. When I was much younger I was involved in some British cycling talent programmes, and there was always underlying talk of weight/food, even among my peers (I was in my mid teens). There is a culture of talking about food, weight, size etc and conversations around being ‘lean’ (ie skinny) and ‘broad’ (ie not) are commonplace in and out of competition and especially among older experienced cyclists. From my experience now, I think people my age largely have a healthier relationship with these issues, but nonetheless having come through the system myself, I have found myself engaging in sometimes unhealthy eating practices – even when this is detrimental to my performance.’ (M, 18–24, Road Cycling)
Discussion
The aims of this study were to quantify DE and ED risk in a global sample of competitive cyclists using the EAT-26 and compare responses between sex and cycling discipline. Furthermore, we aimed to obtain self-reported information related to cycling and nutrition provision from organisations participants and gain greater contextual understanding of what may contribute to the risk of DE behaviours in competitive cyclists. The results of our study demonstrate that median EAT-26 scores were below the cut-off of 20 proposed as indicative of DE 31 ; however, 16.7% of participants reported scores that equaled or exceeded this cut-off value. Furthermore, analysis of the qualitative data highlighted the complex context in which competitive cyclists developed relationships to food and their bodies, as well as dietary practices being directed by performance possibly to the detriment of health.
A median EAT-26 score of 8.0 ± 12.0 was calculated from the respondents in the present study. Previous research has demonstrated higher scores in cyclists than the general population. 34 Riebl et al. reported that 62 male cyclists reported EAT-26 scores that were significantly higher than those of 63 non-cyclist controls (12.6 ± 9.6 vs. 5.7 ± 5.9), which supports the notion that ED prevalence may be greater in athletes than the general population. 8 High EAT-26 scores have previously been reported in other cohorts engaging in weight-sensitive sports, with baseline scores of 22.3 ± 8.4, 14.8 ± 9.6 and 14.8 ± 12.6 in elite ballet dancers, 59 experienced jockeys 60 and collegiate wrestlers, 61 respectively. A cut-off score of ≥20 on the EAT-26 is used to provide a basis for referral for DE behaviours and for potential ED diagnosis. 31 Of the 203 participants in our study, 16.7% scored ≥20. Amongst 122 female competitive cyclists, 32% scored ≥20 on the EAT-26 35 whilst Ferrand and Brunet 32 reported 57% of male cyclists in their sample scoring above the cut-off. Despite the lower proportion of participants in our study scoring above the cut-off value, there is consistent demonstration in the literature that competitive cyclists are at risk of DE behaviours and possible ED development.
Certain behavioural characteristics may be predictive of competitive cyclists demonstrating DE or developing clinical EDs. Competitive cyclists being a weight-conscious population was agreed or strongly agreed by 86% of participants. Additionally, 54% of participants indicated that they had manipulated their body weight in the previous 12 months for cycling-related purposes. Similar findings were reported by Hoon et al. 62 with 86% of cyclists also agreeing or strongly agreeing that cyclists are a weight-conscious population. Additionally, 79% of participants had purposefully manipulated their body weight in the previous 12 months, and 69% believed being at their lowest body weight was beneficial for cycling. 62 Moreover, Haakonssen et al. 63 report 70% of cyclists attempted to reduce their body weight in the past 12 months. Harmful weight reduction practices have been reported in other sports, particularly those who are required to make a weight category 64 such as female physique athletes 65 and combat sport athletes. 66 As such, providing athletes with structured support towards body mass reduction may ensure safe weight making practices are observed that encourage optimal eating patterns and feelings towards dietary practices. 67
Regarding nutrition, 52.4% of cyclists reported receiving no nutritional support from their organisation, and 88.3% stated that they received no contact time from a nutritionist or dietician. It has been previously suggested that availability of qualified nutrition personnel and support can positively influence competitive cyclists’ health, well-being and performance. For example, competitive male cyclists who adopted behaviours that positively impact energy availability demonstrated greater lumbar spine bone mineral density and favourable cycling outcomes, alongside perceived improvements in well-being and cycling performance across a six-month period. 23 Whilst the initial aim of the study was to compare the provision of both nutrition and skeletal loading education in an intervention format, the authors noted that athletes from the control group adopted behaviours consistent with receiving, or seeking, additional information. 23 Nonetheless, it is clear that the provision of education from a qualified practitioner can facilitate improvements to dietary intake that offset both health and sport-specific issues related to reduced food intake. 23 Collectively, cycling organisations should strive to ensure athletes are supported by qualified nutrition practitioners and support staff who are able to identify, monitor and assist with the management of EDs and DE.
In our study, females reporting significantly greater scores on the EAT-26 than males. This finding is perhaps not surprising, given the sex differences in ED and DE prevalence at a general population level, with females being suggested to be at higher risk than males. 68 This trend is largely reflected in athletic populations with rates of between 6–45% and 0–19% reported in female and male athletes, respectively. 13 Body dissatisfaction is significantly more likely to be reported by elite female athletes than male athletes 69 ; however, ED and DE risk is not always different, with similar EAT-26 scores in elite soccer players previously reported. 38 On a physiological level, EDs disproportionately affect females when compared to males, with genetic and endocrine variation likely to contribute to this. 70 On a sociological level, women have long faced gendered body image pressures in sporting settings, largely driven by sexualisation of female bodies within sporting media.38,71 The implications of this are that further directed research to understand the influence of sex and gender on DE and ED risk, as well as body image is warranted. Furthermore, any potential individual or team interventions may need to be tailored to specific populations.
Finally, the qualitative data obtained from this study provides some initial insight into the social context of competitive cycling and how this may contribute to the development of ED and DE. Through the synthesis of the qualitative data presented, we show the complex interplay of factors which influenced the cyclists dietary practices and perceptions of body image. The implication of these results are that greater focus needs to be placed on the social context of competitive cycling, the networks around the athletes, and the sporting ‘culture’ to understand how these influence individual eating behaviours and body image. A better understanding of this would help shape more effective interventions, and these partial insights offer a good starting point for further qualitative research using interview-based methods to gain a greater understanding.
A strength of the current study is the large sample size from a global sample, and the addition of qualitative data to build on gaps in knowledge. Moreover, the reporting of complete demographic and training information is important due to a lack of consistency in this information in previous studies. 29 However, there are limitations of the study to be considered when interpreting the findings. The self-reported nature of the study, and convenience sampling approach applied, means the results may be subject to sampling bias and social desirability bias in open-text responses. There was no definition provided for participants when selecting the level of competition/s that they engage with, and as such these may have been misinterpreted when the questionnaire was completed. Additionally, whilst we sought to collect data from all competitive cycling disciplines, most responses were from road cyclists. Similarly, whilst the aim was to collect data from a global sample, 76% of responses were from the United Kingdom. As such, despite our efforts to increase the homogeneity of responses, the data must be interpreted with this in mind.
Practical considerations
Based on the results of this study, there are a number of practical considerations for those working in the sport and connected stakeholders:
Re-education of athletes and stakeholders is required around the idea that lightweight and lean always equals improved performance. From the results and comments within this study, there appears to be the assumption that weight loss equates to fat loss, yet such loss may also include muscle mass, which may be detrimental to performance. Additionally, a cultural shift within the sport is needed in order to create positive sporting environments and the potential impact that comments can have on self-esteem and body image. A more detailed evaluation of the media's role in promoting body image within cycling is justified, and whether cyclists view this positively or negatively.
Conclusion
In conclusion, the findings from the present study indicate competitive cyclists do appear to be an ‘at risk’ population for DE/ED, and this risk may be increased for female cyclists. Furthermore, there is a complex interplay of socio-cultural factors which influence competitive cyclists relationships to eating and their bodies, as well as dietary practices being directed by performance possibly to the detriment of health. This warrants further research using qualitative methods such as interviews to gain a richer and more in-depth understanding of these processes and experiences. In light of these findings, different stakeholders involved in competitive cycling should look to develop further nutritional services, access to nutrition education and consider their role in creating positive environments for athletes.
Supplemental Material
sj-docx-1-spo-10.1177_17479541241251688 - Supplemental material for An appetite to win: Disordered eating behaviours amongst competitive cyclists
Supplemental material, sj-docx-1-spo-10.1177_17479541241251688 for An appetite to win: Disordered eating behaviours amongst competitive cyclists by Charlie Jon Roberts, Howard Thomas Hurst, Nicola Keay, Jennifer Hamer, Stacy Sims, Katherine L Schofield and Jack Hardwicke in International Journal of Sports Science & Coaching
Footnotes
Data availability statement
All data underpinning this publication are openly available from the University of Northampton Research Explorer at 10.24339/d9dfc5c2-e36a-4ea4-a458-aa694487fd05
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.