
Abstract
Injury prevention exercise programmes (IPEPs) are efficacious, though there is no IPEP specifically designed to reduce shoulder injuries in rugby. This study aimed to determine the feasibility and acceptability of the Rugby Active Shoulder Injury Prevention (RASIP) programme. Three community rugby union clubs participated in a 12-week pilot study (players, n = 51; coaches, n = 7). Two teams were randomly allocated to the RASIP programme and one to the FIFA 11+ (IPEP) intervention. Feasibility was examined by players’ adherence to the IPEP, and acceptability was described by players’ and coaches’ perceptions of the IPEP. On average, more players were exposed to 11+ training sessions (100%) than the RASIP programme (19 out of 36 players, 53%). Higher percentage of exercises was completed over the season in the 11+ (97%) than the RASIP programme (58%). Across both groups, there were different approaches followed in delivering the allocated intervention. The coach-led, prescriptively followed 11+ IPEP was better at achieving higher adherence with exercises. Coaches were concerned of not having enough time in their sessions to include the IPEP. This pilot study has shown that the intervention is feasible to deliver and is acceptable with improvements recommended by community stakeholders, coaches and players in a community youth rugby setting.
Introduction
Upper limb injuries are amongst the most common (25 per 1000 player hours)1,2 and constitute the greatest injury burden (553 days per 1000 player hours) at the elite schoolboy level of rugby union. 3 Such injuries during a time when major physiological developments are occurring can have considerable consequences4,5 which may increase the risk of musculoskeletal morbidity. 6 Preventive measures must therefore be prioritised to reduce this risk and enable players to remain active within the sport into adulthood. 7
Multicomponent injury prevention exercise programmes (IPEPs) have been shown to be efficacious in preventing musculoskeletal injuries in a number of sport contexts.8–13 For example, the Oslo Sports Trauma Research Centre (OSTRC) Shoulder Injury Prevention Programme was tested in a randomised controlled trial of 660 elite handball players, and the risk of reporting shoulder problems during the competitive season was 28% lower in the intervention group (odds ratio (OR) 0.72, 95% confidence interval (CI) 0.52–0.98, P = 0.038). 14 There was also a 22% lower risk of shoulder problems leading to moderate or severe reductions in training volume or performance or total inability to participate (OR 0.78, 95% CI 0.53–1.16, P = 0.23) when compared to a usual practice control. More recently, the FIFA 11+ Shoulder (FIFA 11+S) IPEP was developed 15 with a focus on exercises to strengthen the upper extremity and core stability training. In 2021, its effectiveness in reducing the incidence of upper extremity injuries in one soccer season was subsequently evaluated in a randomised control trial. 13 Amateur soccer goalkeepers (n = 726) aged 18–35 years participated in the study which found a 68% reduction (injury risk ratio (IRR) = 0.32; 95% CI, 0.27–0.34) in the total number of upper extremity injuries amongst those completing the FIFA 11+S programme compared to a regular warm-up.
Similar controlled trials introduced in schoolboy (in 2017) and adult community rugby (in 2018) to reduce the incidence and burden of rugby-related injuries have shown significant injury reductions.16,17 Notably, schoolboy teams (n = 118) doing an injury prevention warm-up sustained substantially fewer upper limb injuries than teams in the control group (burden RR = 0.66, 95% CI 0.40–1.10), which may be attributed to upper body resistance and plyometric exercises in the routine. 16 Importantly, completing the intervention at least three times per week led to a 72% reduction in overall match injury incidence (RR = 0.28, 90% CI 0.14–0.51) compared with the control programme. 16 Advancing this research into ‘real-world’ contexts will only be achieved by understanding the implementation context as outlined in the Translating Research into Injury Prevention Practice (TRIPP) 18 sport injury prevention model. The TRIPP 18 model emphasises that implementation of preventive strategy in youth sport must involve coaches and parents who can provide necessary information about the feasibility and acceptability of interventions to improve player welfare. 19 Until now, shoulder injury prevention has not been a specific priority in youth rugby, and the dearth of evidence in this area justifies the need to address this topic. The purpose of the study was to evaluate the feasibility and acceptability of a shoulder-specific IPEP for community youth rugby players.
Methods
Development of Rugby Active Shoulder Injury Prevention programme as an IPEP
The RASIP (Rugby Active Shoulder Injury Prevention) programme was developed using research evidence which was agreed to be appropriate and suitable by the multidisciplinary technical project group, community stakeholders (intervention delivery, barriers to uptake and sustainability), and was implemented in a pilot study for community youth rugby players. An invitation with the study details was sent by email to individuals with recognised experience as a sport injury researcher, medical or strength and conditioning practitioners in rugby union to contribute to the multidisciplinary technical project group. The process followed in the development of the RASIP programme is outlined in Table 1. Step 5 of the development process forms the main focus of the present paper, where the shoulder IPEP was used in a pilot study with community youth rugby players and feedback was obtained from players and coaches. This element of the study was conducted in 2016, and ethical approval was obtained from the University of Bath Research Ethics Approval Committee for Health, reference EP 15/16 251. The final version of the shoulder IPEP was named the RASIP programme and is described in Table 2.
Summary of the methods used to develop the shoulder IPEP.
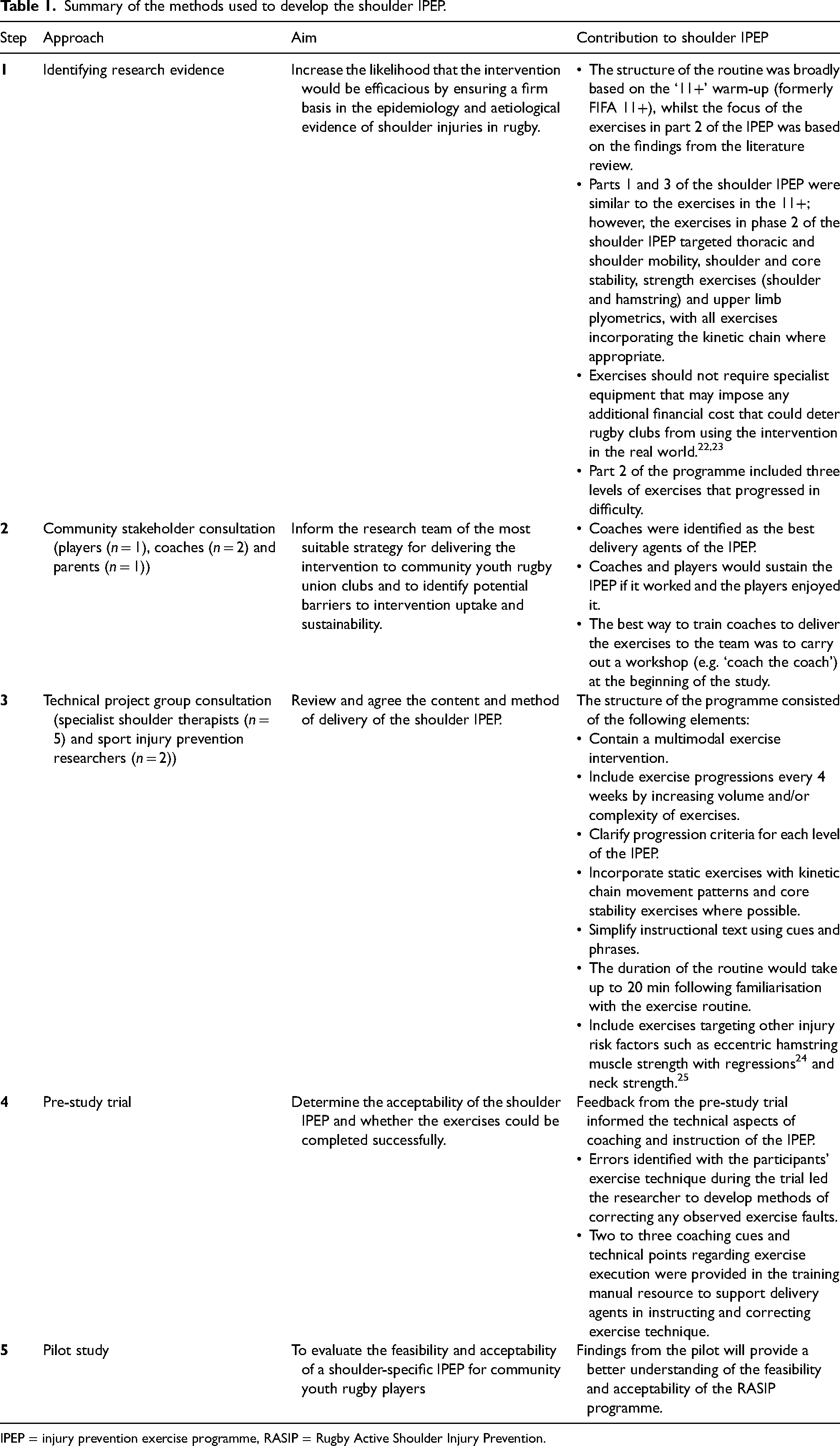
IPEP = injury prevention exercise programme, RASIP = Rugby Active Shoulder Injury Prevention.
The rugby activate shoulder injury prevention programme.
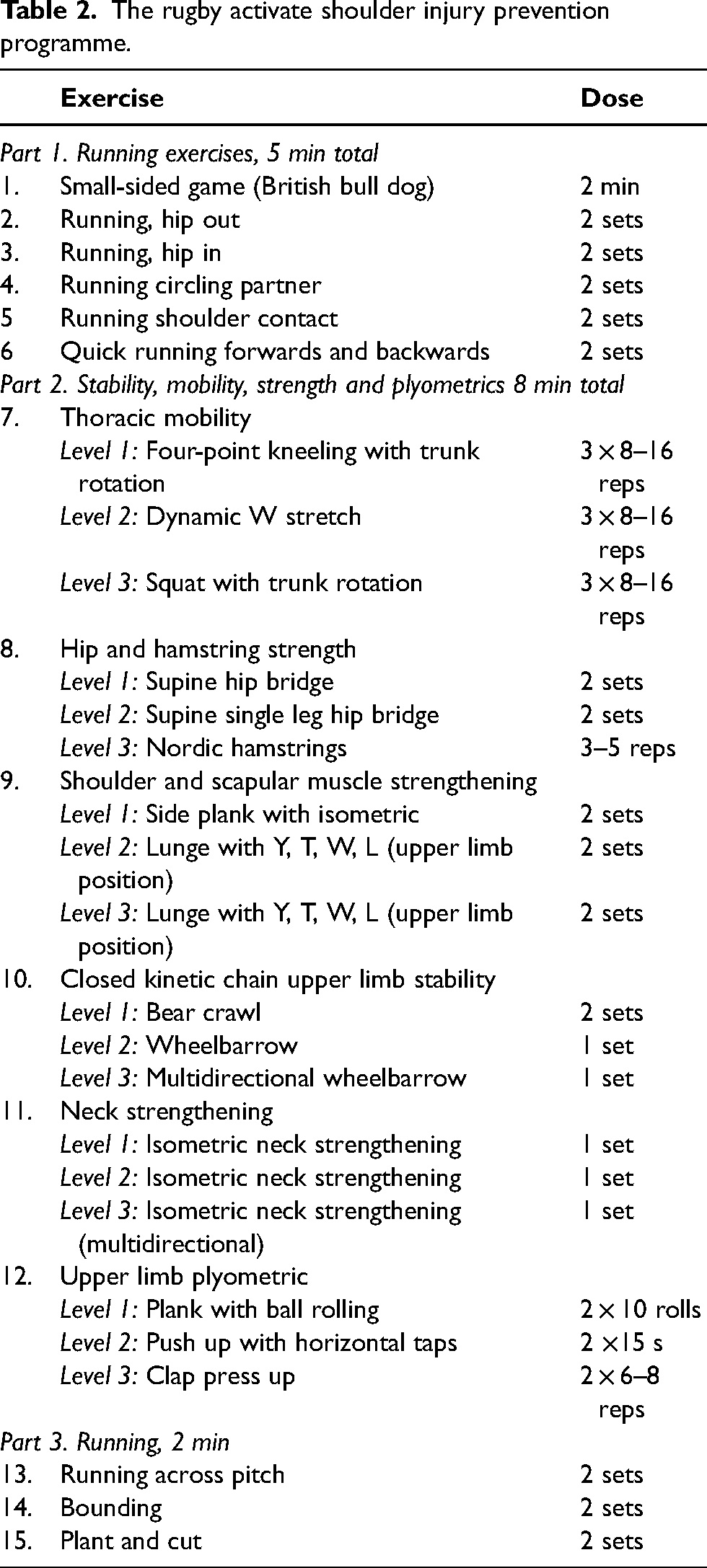
The ‘11+’ was selected as the control because it has been shown to be an efficacious general injury preventive intervention in other youth sports.20,21 The ‘11+’ protocol consists of three parts: part 1 comprising six running drills, followed by six exercises, focused on lower extremity strength, balance, neuromuscular control and stability in part 2. Three levels of exercise progressions are included in part 2 of the programme. The final part consists of three high-speed running drills. The RASIP programme was designed to mirror this, such that the two programmes were structurally indistinct but with different exercise content. This allowed for the content of both interventions to be evaluated in order to determine which IPEP may have been more acceptable to the teams.
Participants
Three community youth rugby union clubs (15 player-a-side) with players in the under 14–18 age groups in the south of England were block randomised into the RASIP intervention (n = 2 clubs, 36 players and five coaches) or control group (n = 1 club, 15 players and two coaches) (Figure 1). Teams from the same competitive levels were involved in the study. The guardians/coaches were provided ample opportunity to review study materials. Consent from parents and assent from players were obtained prior to data collection. No one was financially compensated in this study, and governing bodies were not involved in recruitment.
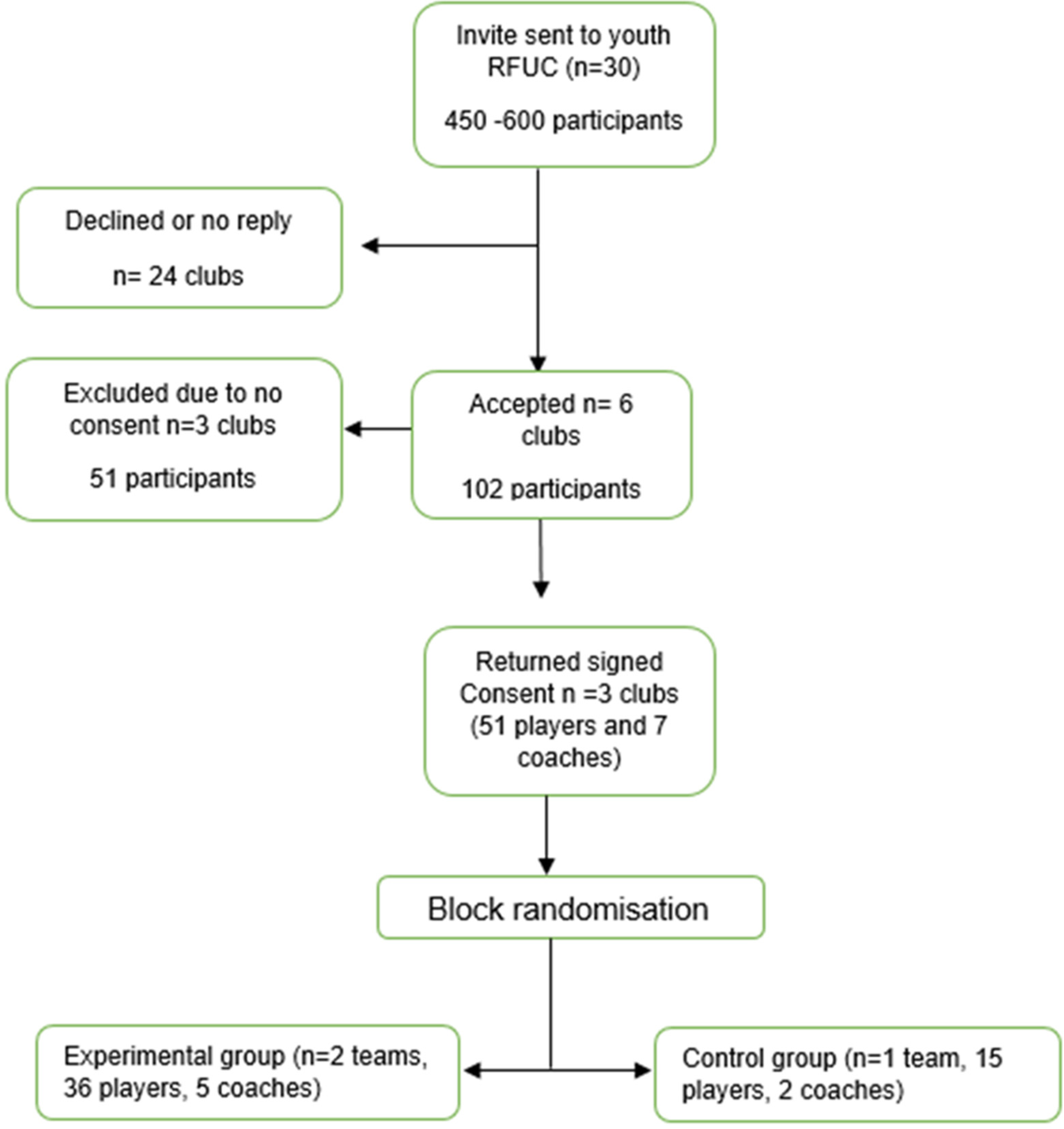
Flowchart of participation through study.
Implementation of RASIP intervention
Delivery
Community stakeholders’ feedback in step 2 (Table 1) of the development process identified that coaches were the best delivery agents of the IPEP. Coaches had the option of nominating a player champion to be responsible for the warm-up routine. The lead researcher therefore visited participating teams at the start of the 12-week study to deliver an induction (i.e. ‘coach the coach’ session) to the IPEP. Teams were provided with educational resources that included hard copy laminated sheets with pictures and instructions for each exercise and a training manual covering correct technique and coaching points, available on a bespoke website. Material was the same as on the website as provided in the hard copy version to the study participants. To evaluate team adherence to the IPEP, the coach at each club was tasked with completing a weekly reporting form that included details about completion of the IPEP (Appendix A). Regular periodic contact was maintained between coaches and the researcher during the study period to prompt form completion.
Adherence
Intervention fidelity was defined as the overall proportion of exercises completed at the team level across all exposures, based on coach reporting. During the intervention, all teams involved in the study had two scheduled visits (during week 4 and week 12 of the study) which were coordinated with the coaches of each team to observe whether they completed the IPEP and to specifically record the number of exercises done at that session. These observational visits were not carried out to identify or correct technique. The intervention's feasibility was also qualitatively captured by the coaches weekly completed reported forms which required them to tick which exercises were done during that session and observing the method of delivery demonstrated by the delivery agents in their approach to engaging with and delivering their allocated programme. 26 The reporting forms were completed weekly and submitted at the end of the study then imported to Microsoft excel by the lead author.
‘Fastsms’ (Commify UK Limited) was the SMS internet service provider used to collect programme exposure data from players in this study. As the players were under 18 years old, a SMS had to be sent to their parents/guardians in accordance with the Rugby Football Union (RFU) Safeguarding Policy. 27 The SMS was sent to the players’ parents/guardians following the observational visits, asking them to reply ‘yes or no’ to indicate whether their child did the warm-up programme that day. If they replied ‘yes’, they were sent another SMS to find out how many exercises were completed at that session, which was compared to the number recorded by the observer and with the coach's reporting form to assess the congruence between reporting methods. The flowcharts in Appendix B illustrate the structure of the text messages sequence and triggers that were sent.
Data collection
Questionnaires
Attitudes pre- and post-intervention
Coaches’ and players’ attitudes were assessed through a pre- and post-intervention online questionnaire, using the Online Survey system (Jisc, Bristol, UK). A hyperlink to the surveys was sent via email to guardians/coaches. This was adapted from a questionnaire developed for use with youth soccer coaches. 28 The questions were re-phrased to reflect the rugby setting and underwent face validation by the research team prior to the start of the study. The questionnaire captured information about the coaching and player experience in section A, perceptions and attitudes towards injury risk in rugby in section B, knowledge of injury prevention and risk in section C and feedback about the RASIP intervention in section D (Appendix C). The questionnaire was formatted with separate versions for coaches’ and players’, with polychotomous and seven-point Likert scale responses to all questions. The questionnaire had 33 questions pre-intervention and 39 questions post-intervention and took 10–15 min to complete. The data acquisition and transferring from Online Survey (Bristol) were imported to Microsoft excel for analysis by the lead author.
Injury surveillance method
Injuries were reported using an ‘all complaints’ definition, which included any injury that resulted from the player's body's inability to withstand a transfer of energy during rugby, irrespective of the need for either medical attention or time loss from rugby activities. 29 Fastsms system was used to collect player self-reported injury entered by their parent/guardian via SMS. Injury data was also collected by the coaches on the reporting form and reported descriptively.
Analysis of results
Intervention fidelity was determined by the proportion of exercises completed for each group, which was calculated as the total number of exercises completed during the study divided by the total number of exercises that could be completed. The duration (minutes) taken to complete the programme was also used as an assessment of fidelity, and the method of intervention delivery was reported descriptively based on the coach's weekly reporting forms and observations.
Feasibility was evaluated by describing the coaches’ and players’ perceptions and attitudes towards using their allocated programmes. Feasibility was also indirectly assessed by considering the recruitment and retention of participants to the study, including obstacles to recruitment.
Questionnaire
Questionnaire responses were descriptively analysed and reported as proportions to determine coach and player injury risk awareness and outcome expectations and feedback about the warm-up routine. Deductive coding was then applied by the lead author to identify themes allowing for the coaches’ and players’ responses to be described as perceived barriers and facilitators to the implementation of the warm-up routine.
Match exposure
Players’ parents/guardians were sent weekly SMS asking if the player had participated in a match on the weekend. This information was used to calculate weekly group match exposure which was determined by the number of matches × number of players per team × match duration (hours). 30 This exposure was used for self-reported exposures. The results from this evaluation were used to describe the injury epidemiology.
Results
Participant characteristics
The mean age for all 51 players was 15 years old, their height was 1.72 meters (SD ±9 cm) and weight was 71 kgs (SD ±13 kgs). The characteristics of the participants who completed the questionnaire are presented in Table 3. The average participation in rugby was 2–6 h per week, and one player who was in the RASIP group (9%) had reported using a conditioning programme to reduce the risk of injury during the previous season. One player (by his parent) asked to be withdrawn from the study.
Coaches’ and players’ baseline characteristics.
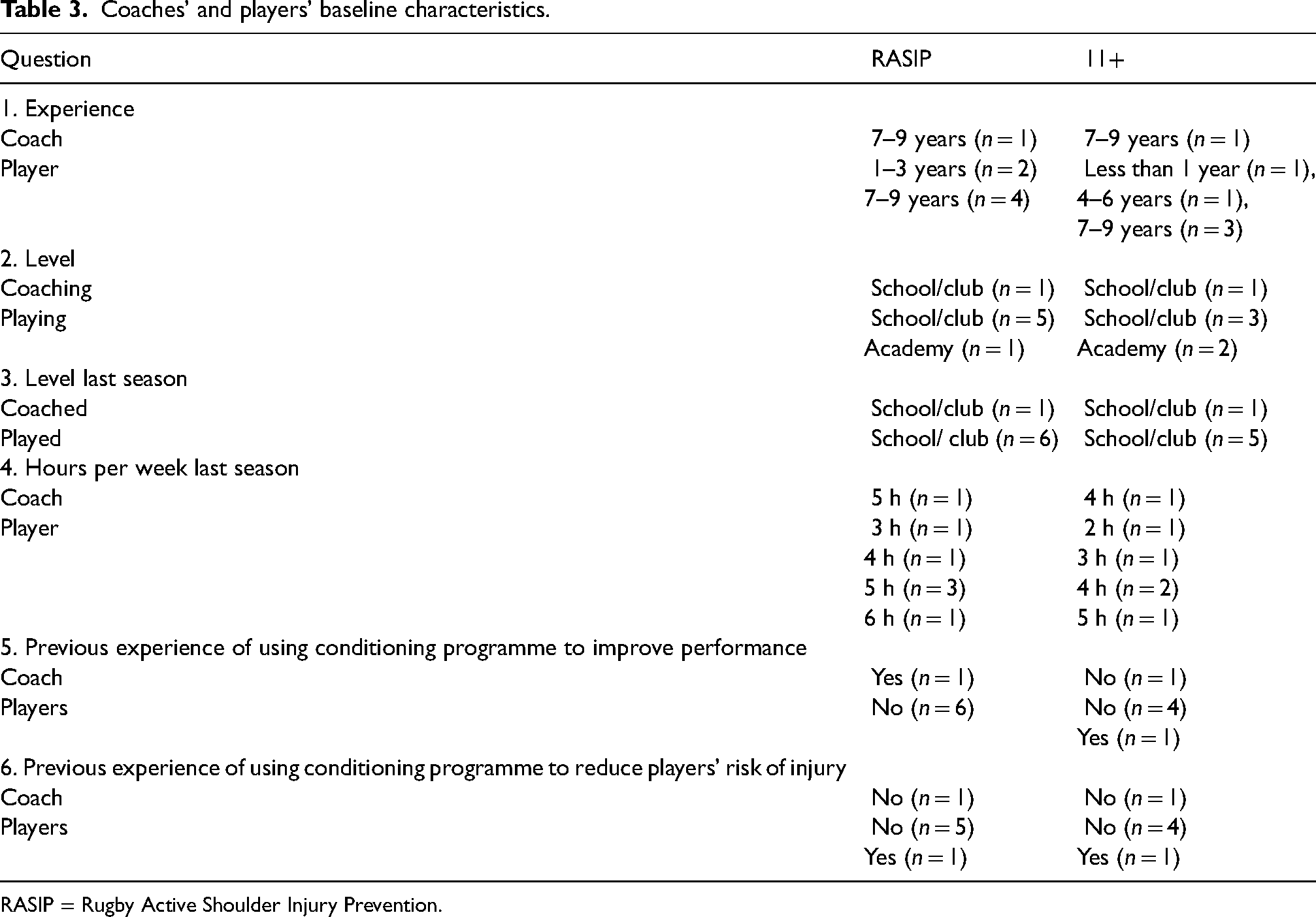
RASIP = Rugby Active Shoulder Injury Prevention.
Intervention delivery
One team doing the RASIP warm-up and the team doing the 11+ warm-up had the intervention delivered by their coach, whilst one team in the RASIP group allocated a player ‘champion’ to deliver the warm-up. When observed, the coach in the 11+ group delivered the warm-up specifically as prescribed in the IPEP. The delivery agents of the RASIP warm-up varied which exercises they did and the number of exercises completed on the day.
Adherence
The average weekly attendance at training sessions during the 12-week study was 19 of 36 players (53%) in the RASIP group, whilst on average, all 15 players (100%) were in attendance in the 11+ group. Participation in the warm-up for the 11+ group ranged from 88% to 100%, whilst the RASIP group ranged from 95% to 100% over the 12 weeks of the intervention.
Based on coach reported data, teams completed their assigned IPEP two to three times per week, on average. The 11+ group completed a higher proportion of exercises (291 of 300 possible exercises, 97% adherence) compared to the RASIP group (261 of 450 possible exercises, 58% adherence) (Table 4). The mean duration of the 11+ was 24 min (range 20–30; 95% CI: 23–26), which was higher than the mean duration (15 min, range 10–25; 95% CI: 14–17) of the RASIP group. There was more variation in the selection of exercises completed weekly in the RASIP group compared to the 11+ group, as indicated by the exercises marked off on the weekly reporting forms. In addition, feedback from the coaches revealed that, due to time constraints, they chose the exercises which they believed to be best for the type of session they were running that day such as attacking, defence or passing and handling.
Adherence to warm-up routine.
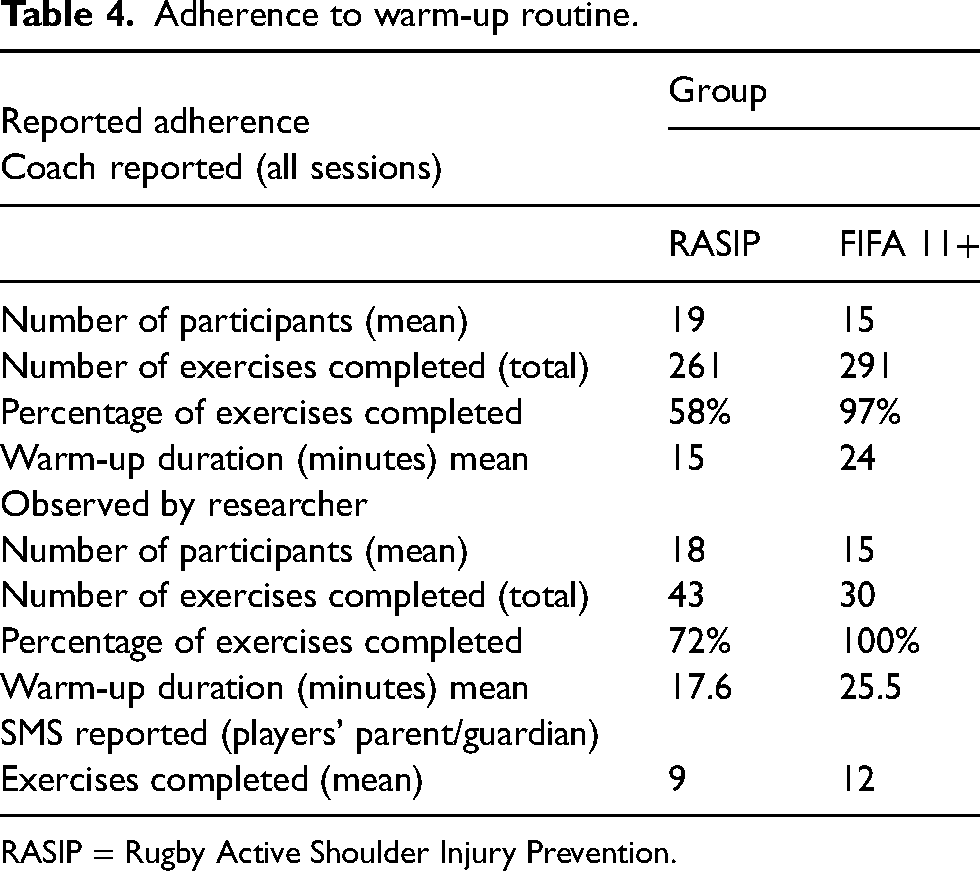
RASIP = Rugby Active Shoulder Injury Prevention.
Coaches’ injury risk awareness and outcome expectancies
Two of the coaches (one from each group) completed the questionnaire. The coaches’ intent to complete both IPEP was rated as ‘extremely good’ (rated 7 out of 7 by one coach from each group) prior to starting the study and at the end of the intervention. They expected that players would be ‘quite and extremely likely’ to improve (6–7 out of 7) their skill by doing the IPEP. Coaches responded that the IPEP would be ‘extremely good’ at reducing the players’ risk of injury. They anticipated that the IPEP would be fun.
Both coaches said that it was ‘extremely likely’ that players would sustain an injury during the season and that it was a shared responsibility between the coaching staff, players and referee to prevent injuries from occurring. At the outset of the study, the coaches perceived their role in injury prevention to be ensuring player fitness, recovery and preparation for the match. Poor muscle strength, a lack of skill and poor technique were considered to be contributing factors to injuries.
The coaches thought that injuries to the face and head would be most common at the start of the study; however, on completion of the study, they believed that injuries to the shoulder and arms or knees and ankles were the most common injuries in the RASIP and 11+ groups, respectively.
Feedback about the warm-up routine
The coach felt that doing the IPEP left them with little time to do other rugby skills training in the 11+ group. The RASIP exercises were not perceived to be specific enough to rugby, and the coach thought routines could include exercises that involved a contact element such as grappling. The coach in the RASIP group liked the idea that by doing the routine, they learnt exercises that may reduce injuries to their players, whilst the coach of the 11+ group liked that their players got better at doing the exercises.
Players’ injury risk awareness and outcome expectancies
Of the 51 players, 21% (n = 11, 6 in RASIP and 5 in 11+) completed the pre-intervention questionnaire. There were slightly fewer players (17%, n = 5 in RASIP, n = 4 in 11+) completing the post-intervention questionnaire. At baseline, 11 players felt that completing the IPEP would be ‘good’, which did not change by the end of the study for the 11+ group, though one player in the RASIP group said it was ‘unpleasant’. Initially all players agreed that ‘having fun with their team would enable them to complete a rugby specific routine’, which was the same at the end of the study for the 11+ group. A high percentage of players (66%, four out of six players) in the RASIP group believed that an IPEP would improve their physical conditioning, whilst 33% (two out of six players) felt that it would be ‘slightly unlikely’ to have this effect. At the end of the study, 80% of players (four out of five players) in the RASIP group believed that the routine would improve their conditioning. All players in the 11+ group felt that an IPEP would improve their conditioning at baseline, whilst 25% (one out of four) felt that this was ‘slightly unlikely’ by the end of the study.
At baseline, all players who completed the questionnaire expected that they would sustain an injury during the season. This did not change by the end of the study. The players in the RASIP group (50%, three out of six players) initially thought that injuries to the head and face and shoulders and arms were the most common injuries in rugby. Injuries to the knees and ankles were thought to be most common at the end of the study. The 11+ group said that injuries to the head and face, chest and abdomen and lower body (hamstring and thigh, pelvis and hips) were most common. All players apart from one in each group at baseline believed that injuries are preventable. This was the same at the end of the study, apart from the 11+ group where all players thought that injuries were preventable.
It was a common view that coaching staff, players, parents/guardians, referees and medical staff were responsible for preventing injuries. A lack of skill, poor technique, and inadequate warm-up were identified by both groups as factors that contribute to injuries in rugby. In addition, 60% (three out of five players) in the 11+ group said that body contact was a contributing factor to sustaining an injury. These factors were also reported by the groups at the end of the study, as was a lack of fitness or training, poor strength and flexibility and player aggression and tackling risk. Furthermore, the players said that ensuring they completed a proper warm-up routine, were adequately recovered and ate healthily was the thing that they could do to reduce their risk of injury.
All players in the 11+ group felt that decreasing their risk of sustaining an injury would be ‘good’, whilst 50% (three out of six players) in the RASIP group felt that it would be ‘extremely good’ at baseline. At the end of the study, this remained the same for both groups. A similar trend was seen with players’ expectations of an IPEP reducing the risk of injuries with 17% (one out of six players) in the RASIP group thinking that it would be ‘quite unlikely’ to reduce injury at baseline. All players in the 11+ at baseline believed IPEP would reduce their risk of sustaining an injury; however, at the end of the study, 25% (one out of four players) of the 11+ group believed that it would be ‘quite unlikely’ to reduce injury.
Injury data
The self-reported injuries using SMS for all injuries was 24 (95% CI: 37–89) for both groups. The number of self-reported injuries using SMS in the 11+ group was 6 (95% CI: 12–108) compared to 18 in the RASIP group (95% CI: 37–100).
Discussion
Minimising the risk of shoulder injuries in rugby union is an important direction for injury prevention, yet, until now, there has been no attempt to outline and develop a shoulder injury prevention programme in community youth rugby union. This study outlines the development process of a new shoulder IPEP in community youth rugby union that encapsulates research evidence integrated with expert views and perceptions of end users. Youth rugby union teams adhered better to a lower limb focused routine than to a shoulder IPEP. Coaches’ and players’ attitudes towards injury prevention were also explored to bridge the gap between research and practice in determining successful injury prevention implementation.
The RASIP intervention was developed in 2016 utilising the available evidence at the time from efficacious IPEPs and also input from the technical project group. Using the structure of efficacious IPEPs such as the 11+ 31 provided a useful framework to develop a new shoulder-specific IPEP. At the time that the RASIP intervention was developed, the development process of the FIFA 11+S intervention had just been published in response to shoulder injuries in goalkeepers in soccer. 15 Though the efficacy of the FIFA 11+S 15 had not been evaluated at the time of the RASIP development, its development process provides a practical and generalisable process that can be applied to developing a similar intervention in other sports. The steps taken in designing the RASIP intervention are supported by evidence-based shoulder-specific preventive exercises that are functional and integrates kinetic chain movements without the need for any specialised equipment and are deemed to be time efficient and less likely to deter engagement with the intervention.22,32 Adhering to this design specification proved to be useful in addressing feedback from the technical project group to ‘avoid static standing exercises’.
Engaging with end users (coaches and players) in the development process of an intervention is vital to gain their support as co-creators of the strategy that they are intended to adopt and sustain in practice. 33 A coach-driven preventive intervention was identified by the community stakeholders as the best method to deliver the IPEP, and this is corroborated in the literature.34–36 This was also the case amongst junior players in a cross-sectional study done with South African rugby players. 37 From 2008 to 2012, Brown et al. 37 used a questionnaire to assess whether injury prevention behaviours were associated with coach-directed education amongst rugby players (n = 2279 junior and n = 1642 senior players). They found that coaches were the preferred source of injury prevention content, acknowledging them as influencers of player behaviour in rugby. The preferred source of warm-up education differed amongst the age groups: junior players preferred to receive this from coaches, whilst the senior players preferred physiotherapists to provide this information. This may reflect that fewer resources are available to community youth teams. Furthermore, when the benefit of including physiotherapists was evaluated in a cluster randomised trial in female youth soccer players, it was found that there was no additional benefit on adherence for team adherence to the intervention from their involvement. 38 These findings also suggest that investing time in ‘coaching the coach’ on the IPEP can effectively support subsequent team adherence. 38 Community stakeholder feedback in our study to train the coach to deliver the shoulder IPEP is in line with these findings and other existing research implementation strategies. 31
Assessing IPEP feasibility and fidelity highlighted that the percentage of weekly attendance and average number of exercises completed weekly was higher for the 11+ than for RASIP (89% vs 53% and 97% vs 58%, respectively). The reason for higher attendance in the 11+ than in RASIP was not evident, and it cannot be concluded that this was due to lack of engagement with either of the IPEPs. Low player attendance at training sessions has also been seen in youth female soccer players though it was not possible to determine if this impacted low IPEP fidelity. 39 Yet, the lower average number of exercises completed in the RASIP group does suggest that the programme or the delivery agents for this routine did not encourage the players to adhere fully to that programme. Players said that ensuring they completed a proper warm-up routine was something they could do to reduce their risk of injury. Despite believing this, it did not persuade the RASIP group to complete the exercises in full. This is not an uncommon finding, as low exercise fidelity (58% exercises completed correctly) and utilisation fidelity (full completion of IPEP in four out of 31 sessions) to the Knee Control IPEP has been seen in a youth floorball teams (mean age 13.6 years, SD 1.1). 40 A recent cross-sectional survey exploring the awareness of the 11+ in Australian amateur footballers (n = 328 players, 55 coaches, 37 non-coaching staff and 16 medical staff) also highlights this challenge in compliance and adoption of IPEPs. 41 Almost 90% of coaches reported modifying the 11+ in their sessions with 48.3% coaches and medical staff reported not completing the full 11+. Interestingly, though players in the 11+ group in the present study found the routine to be boring and said that it detracted them from practicing other rugby skills, they still completed all the exercises in the routine delivered by a coach that prescriptively followed the programme. In community youth rugby teams where there is a lack of medical support, a coach-led and prescriptively followed IPEP was better at achieving higher adherence with exercises compared to a player-led warm-up routine.
It was intended for coaches to deliver the sessions, but variation existed in the method of delivery of the intervention across all teams. One of the teams in the RASIP group had the IPEP delivered by a team champion, whilst the other had a coach as delivery agent, with both individuals displaying different approaches to delivering the IPEP. One of the coaches in the 11+ group stuck to a prescriptive delivery of the programme, whilst the delivery agents (coach and team champion) in the RASIP group were more selective of the exercises their teams completed. Unsupervised delivery of an IPEP has been shown to lead to reduced 11+ adherence in youth football. 38 It is apparent that doing the IPEP as prescribed can promote better adherence; however, this does not work for everyone, and further research is needed to better understand how to improve implementation in each team's specific context. The different delivery agents used by the teams in this study and their compliance with the IPEPs are acknowledged to have impacted on the internal validity. Whilst tightly controlled conditions may be applied to limit this, such as in efficacy trials, 16 it fails to address the complexity of implementation research. 42 When moving controlled evidence to a practical context, there is less control over how the intervention is followed in real life. This is a necessary adaption that is made to accommodate the realities in different practice settings which dilutes the efficacious effect.43,44 Reporting the delivery methods provides a better understanding about what influences the translation of research into real-world settings under less-controlled and more pragmatic conditions.45,46 Researchers need to consider and accept this reduction in effect when moving evidence into practice. 43
Success of preventive interventions depends on programmes being incorporated into regular training, which requires positive attitudes and beliefs from coaches towards injury prevention. 35 A systematic review has outlined the core implementation components of team ball sports using IPEPs. 47 In the reviewed studies, high adherence was attributed to the IPEP being incorporated into team training. In contrast, low adherence was reported in teams that performed the IPEP in addition to team training. The coaches in the present study had strong positive attitudes towards injury prevention, suggesting that they may be receptive to integrating the shoulder IPEP in their training sessions in future. In sub-elite soccer teams, rescheduling part of the preventive programme at the end of the soccer training session increased adherence without negatively impacting on effectiveness in semi-professional soccer players. 48 This however may not be applicable to the youth rugby setting as, in contrast, focusing on structure and routine was considered a facilitator to adoption and implementing IPEPs in Australian community youth rugby (aged 14–18 years old). 49 Furthermore, the lack of time to implement the IPEPs into training sessions is a common barrier that was reported in their study 49 and also amongst English schoolboy rugby union players. 50 Importantly, Barden et al. 50 recommend that the mechanistic effects of the IPEP should be further researched to understand the acute-chronic effects of the preventive exercises before rescheduling parts of the IPEP in rugby. In addition, the coaches found that the RASIP exercises were not specific enough and they would have liked a contact element such as grappling included. This form of training did not appear in the literature during the review process and was not proposed by the technical project group to justify its inclusion, and it is unclear if this would have contributed to better adherence to the intervention.
Trialling the intervention provided a gauge on the logistics of how long the exercises would take to complete, potentially informing refinement of the technical aspects of the programme delivery and the appropriateness of the sequence of exercises. 51 Technical aspects regarding any unclear or incomprehensible exercise instruction, level of difficulty and faulty exercise technique could be exposed and corrected. This is not only useful to enhance the translation of evidence into practice, but also the steps taken can be followed as a suitable approach in promoting the development of preventive strategies amongst target groups in future research. It is by doing this that a better understanding of how the adopters of IPEP perceive and interpret preventive strategies within the real world. The implications from this study are thereby directly relevant to shoulder injury prevention in community youth rugby players and provide a deeper understanding about developing a shoulder-specific IPEP in real-world settings.
Generalisability of the findings in this study is limited due to the small sample size, though that was not its aim. It was also not possible to visit the teams unannounced, which could have modified the teams’ behaviour in response to their awareness of being observed. However, the mean number of exercises completed for the RASIP group when observed was the same as reported by the coach when they were not being observed, increasing confidence that the observed values are corroborated. Players were required to have their parents return a signed consent form to allow their child to participate in the study, but many forms were lost by the players. A potential option to address this issue is to provide parents the option to electronically consent to their child's participation in the study. The information and consent letter sent to parents could include a unique individual code which the parent could include in a SMS to the research team to acknowledge agreement to participate in the study. Prepaid envelopes could be provided to allow parents to post their consent back to the research team. A wider youth age range and inclusion of other recruitment sites such as schools and a wider geographical region could increase the scope for recruiting more teams into a larger study. Another possible strategy to increase recruitment in this population could allow for additional recruitment time. Alongside this, a directed marketing strategy would be advantageous in promoting the study and attracting more clubs to participate. It is acknowledged that not all parents/guardians will have or know how to use a text messaging service which could have contributed to the lack of recruitment. Training on the use of the text messaging service or alternatives should be considered for future studies. In addition, it is recommended that a training plan on how to use the SMS reporting method is included in the handbook and website for all involved with SMS use to support validity of the data. Challenges to data collection and injury surveillance in this under-resourced environment are a limitation of this study. The SMS text bias may influence fidelity and validity of responses which could be entered incorrectly or falsely by participants and or their parents or guardian. Feasible methods that are reliable, valid and representative of the target audience may be considered to limit this in future research. It is also acknowledged that there is a risk of recall bias when using retrospective approaches. The findings from this pilot study during a development process provide new knowledge about the acceptance of the preventive intervention and need for it to be adaptable for acceptance in this setting. 43
Conclusions
The transparent approach reported here offers guidance to other researchers around the important steps used to develop an intervention that balances research evidence with practitioner expertise and end users’ experience within a specific implementation context. Most importantly, this study provides new knowledge about the feasibility of the shoulder-specific IPEP amongst community youth rugby coaches and players, allowing it to be tailored to encourage maximum participation and effectiveness. Even after following these steps, it still may take some iteration before being implementable in context. These findings provide a better understanding of how the adopters of IPEPs perceive and interpret preventive strategies within the real world and highlight the importance of developing an IPEP specifically suited to the implementation context.
Supplemental Material
sj-docx-1-spo-10.1177_17479541231192170 - Supplemental material for Feasibility and acceptability of a new shoulder-specific warm-up programme to prevent injuries in community youth rugby union as compared to the FIFA 11+
Supplemental material, sj-docx-1-spo-10.1177_17479541231192170 for Feasibility and acceptability of a new shoulder-specific warm-up programme to prevent injuries in community youth rugby union as compared to the FIFA 11+ by Vincent R. Singh, Keith Stokes and Carly D. Mckay in International Journal of Sports Science & Coaching
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
University of Bath Ethics Committee: Research Ethics Approval Committee for Health Ethics number: EP 15/16 251.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Private Physiotherapy Educational Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.