
Abstract
Players who lack the knowledge to recognise the signs and symptoms of concussions may be less likely to disclose their injury. New Zealand Rugby's Community Concussion Initiative includes an interactive education session highlighting peer-recognition of concussions. This mixed-method study examined the effect of an education session on high school players’ concussion knowledge and attitudes as well as the impact of player demographics on these variables. Focus groups were used to explore player experiences. The RoCKAS-ST was used to measure concussion knowledge/attitudes before and after the education session. Multiple linear regression examined associations between demographic variables, including school decile (relative wealth of the geographic region the school serves), and pre-education concussion knowledge/attitudes scores. Wilcoxon signed-rank tests compared pre-concussion and post-concussion knowledge/attitudes scores. Qualitative data were analysed via thematic analysis. Overall, 532 players completed questionnaires; 75 players participated in focus groups. Pasifika players had lower concussion knowledge than NZ Europeans (p < .001). Mid-decile schools had higher concussion attitudes scores than low decile schools (p < .001). Pre-education and post-education session concussion attitudes and knowledge scores did not differ significantly, suggesting the one-off education session was not successful in improving these outcomes. Players identified: (i) the education session to be valuable, but some uncertainties remained; (ii) the importance of player comfort, interaction and comprehension; (iii) the need for role models, real stories and regular content refreshers. Requests for presenter diversity, support and easily understood information were more prominent in Māori/Pasifika and low-decile groups. Greater consideration of these factors is necessary in the development of education interventions.
Introduction
Rugby union (henceforth referred to as rugby) is a popular contact team sport played internationally by players of different ages and genders. Due to its inherent collision-based nature, rugby has a high prevalence of concussion. 1 The immediate implications, as well as the uncertainty surrounding the long-term consequences of concussions, continue to be a concern for international and national sporting organisations, healthcare professionals, and the wider community. 2 Recognition and reporting of concussion symptoms are critical components of safe and appropriate concussion management. However, concussions are complex injuries that may be difficult to recognise as this partly relies on patient-disclosed non-specific symptoms. 2
In New Zealand (NZ), rugby is played by approximately 40,000 male and female high school athletes (NZ Rugby National Database, 2020). In this setting, reporting of concussions are especially challenging due to the high level of non-disclosure and lack of medical support staff.3,4 Since 2001, NZ Rugby (NZR) has delivered a compulsory annual education programme (RugbySmart) for coaches and referees. The purpose of RugbySmart is to provide injury prevention information through education, technical skill development and coaching theory. Conversely, in NZ player concussion education at the community level has primarily been indirect/passive, relying on coaches and/or managers to translate and communicate information. Findings from a 2017 survey of NZ high school players found coaches were the main source of concussion information. 5 While providing the RugbySmart course has been linked to higher levels of concussion knowledge and attitudes in coaches, 6 research also suggests a coach's communication and translation of concussion knowledge to players is strongly predicted by their own personal concussion attitudes and beliefs. 7
Coach communication paired with an athlete's perception of coach communication both play a role in an athlete's intention to report a concussion. 8 Also, younger and/or less experienced coaches had poorer attitudes towards concussion knowledge and reporting, which is likely to impact these factors for their players. 6 In contrast to the passive ‘trickle-down’ strategy employed by NZR, direct concussion education interventions for players, employed by other countries, have resulted in a higher level of concussion knowledge.6,9 Providing direct education to players may be one strategy to overcome current system barriers in concussion knowledge translation to facilitate improved concussion recognition.
While some concussion education sessions have had significant positive effects immediately following the intervention,10,11 the sustained effects 2 to 6 months post-intervention are mixed.10,12 Additionally, although players may have the knowledge to recognise the symptoms of concussion, factors such as players’ attitudes towards concussion symptom disclosure and reluctance to be removed from play are critical considerations in concussion reporting. 13 Chrisman et al. 14 found that although most rugby players were able to identify the dangers of a concussion, when presented with scenarios involving concussive symptoms, they reported that players would continue to play. Similarly, a survey of collegiate athletes found that 43% of respondents with a concussion history reported that they knowingly hid symptoms to avoid being removed from play. 15 Even though the link between concussion knowledge and reporting behaviours appears to be tenuous, 16 players who lack foundational concussion knowledge may not recognise their symptoms as a suspected concussion.3,17
In 2018, NZR began piloting a Community Concussion Initiative (CCI) which adopted a system approach to identify key stakeholders involved in the management of concussions, their level of influence and the impact these factors have on player welfare. 18 The CCI's purpose was to facilitate a positive change in concussion attitudes and reporting behaviours in both players and the wider community by considering potential systemic influences. The Theory of Planned Behaviour (TPB) offers a framework to explore the barriers to concussion reporting in community sport; it purports that reporting behaviour is determined by intention, which is, in turn, predicted by attitudes (beliefs around the consequences of reporting concussion), subjective norms (beliefs around the views of other stakeholders) and perceived behavioural control (beliefs about ability to identify or confidence to report a concussion). 19 Understanding reporting behaviour thus extends beyond the reporting pathway alone and instead should be understood in terms of the informational, social and cultural factors that may inhibit the behaviour. 19
To target this change in behaviour and attitudes, an interactive concussion education intervention was developed for players as part of the NZR CCI. The initiative was based on recent research (as of 2018) which focused on shifting subjective norms and empowering players to look out for one another, 20 highlighting peer-recognition of concussion signs and symptoms, following NZR ‘4 R's’ (Recognise – Remove – Recover – Return) (www.rugbysmart.co.nz/injuries/concussion/), and emphasised the reduced performance effects of playing through a concussion.21,22
The approach best suited for a specific context requires an understanding of the community priorities and resources available within the specific sports setting. In the context of high school rugby in NZ, this includes an understanding of the differences in attitudes, behaviours and cultural beliefs held by players from different demographic groups (e.g. Māori/Pasifika, female players, players from disadvantaged backgrounds). Without these contextual considerations, the resulting ‘one-size-fits-all’ approach is unlikely to shift concussion reporting or management as information may not be considered relevant or meaningful by all stakeholders. This may indeed have been the case in previous research wherein Māori and Pasifika players, and players from lower socioeconomic areas were less likely to be aware of concussion guidelines compared to NZ Europeans. 5 Therefore, the primary aim of this study was to examine the effect of an education session on high school players’ concussion knowledge and attitudes, and to explore the impact player demographics had on these outcome variables. The secondary aim was to explore player perceptions and experiences of the education session using focus groups.
Methods
Study design
The current study is part of a wider project investigating NZR CCI. 18 This specific study was conducted during the 2018 high school rugby season (February to August) and utilised a mixed-method design. Mixed-method research combines qualitative and quantitative research approaches to enhance breadth and depth of understanding. 23 Quantitative (survey) and qualitative (focus group) data were collected and analysed separately. Integration of the two data sources was conducted at the level of interpretation/reporting. 24
Education session
As part of the CCI, an interactive educational presentation focused on shifting subjective norms and promoting peer-supported action was delivered at each school by a researcher with expertise in concussion (DMS). The education sessions (lasting ∼20 min) were delivered during the pre-season at a convenient and quiet location during lunch break or before a training session.
Participants
Male and female rugby players from 22 high schools across NZ were invited through provincial union representatives (via email) to participate. Purposeful sampling was used to target schools representing a range of ethnic, socioeconomic, gender and geographic backgrounds. 6 Schools and clubs that consented to be involved were then asked to identify and invite suitable teams to take part in the study. For the focus groups, participants who had participated in the NZR CCI and sustained a rugby-related concussion during the current season or previously (as identified by the school contact/coach) were invited.
Ethics
Ethical approval was granted by the University of Otago Human Research Ethics Committee (approval 18/087). All participants provided informed written consent. Parental/guardian consent was obtained for participants aged 15 years or younger.
Data collection
Quantitative data: The Rosenbaum Concussion Knowledge and Attitudes Survey-Student Version (RoCKAS-ST) questionnaire 25 provided a measure of concussion knowledge and attitudes. Concussion knowledge was measured by 25 items, consisting of 17 true/false and 8 symptom recognition questions; scores ranged from 0 to 25. Concussion attitudes were measured by 15 items on a 5-point Likert scale; scores ranged from 15 to 75. Both concussion knowledge and attitudes were presented as percentages – for example, a concussion knowledge score of 20 would be presented as 80%. 25 The methods for collecting and scoring the pre-education surveys are described previously. 6
Participants completed the RoCKAS-ST immediately before, and 2 months after the education intervention. These time points were selected for consistency with other concussion education intervention programmes.12,26 Additionally, a post-education survey was administered with eight questions: five Likert-style questions to gather education session feedback; one rank-order question in which players selected the ‘4 R's’ in the correct order from an eight-word list; one multi-select question to identify things one should/should not do within the first 48 hours following a suspected concussion; and one short-answer question regarding player preferences for future education initiatives.
The follow participant characteristics were collected ethnicity, decile and gender. Players identified their ethnic background (NZ European, Māori, Pasifika, or Other (e.g. Asian or Indian)). Pasifika is a broad and diverse term that encompasses individuals from, or whose ethnic heritage links them to various Island nations and communities (e.g. Samoa, Tonga) in the South Pacific.27,28 Schools in NZ are ranked by deciles, which is a measure of the relative wealth of the area that the school serves. A decile ranking of ‘1’ represents the poorest 10% of the population, while ‘10’ represents the wealthiest 10% (www.education.govt.nz). Deciles were grouped into three categories: low (1–4), middle (5–7) and high (8–10) decile.
Qualitative data: Focus groups were conducted in the post-season period, approximately 4 months after the education intervention. Focus groups allowed players to describe their experience with the intervention, and to inform future concussion education sessions. Details of the focus group data collection are described previously. 29 Briefly, an interview guide was developed which included questions about roles and responsibilities, concussion education, concussion baseline assessments, and concussion management. Focus groups were facilitated by four trained interviewers experienced in qualitative methods. For the current study, only the questions surrounding concussion education in the player focus groups were included.
Data analysis
Quantitative data: Data were analysed using SPSS (v.23, Armonk, NY: IBM Corp.). Surveys were scored following Rosenbaum and Arnett guidelines 25 and described previously. 6 Multiple linear regression analyses examined the association of age, ethnicity, decile and gender on the pre-education concussion knowledge and attitudes scores. Both models were assessed for regression diagnostics (normality of residuals) and collinearity (variance inflation factor (VIF)). Overall, regression models were well fitted (p < .05). Collinearity of the independent variables was low for both models (VIF < 10), but residuals of both models indicated some deviation from normal distribution at extreme values. Overall composite Cronbach's alpha for concussion attitudes scores for sections 3 and 4 of the RoCKAS-ST was 0.76.
To assess the effect of the interactive educational intervention, concussion knowledge and attitudes percentage scores were compared before and after the intervention. As concussion knowledge and attitudes percentage scores were not normally distributed, median and inter-quartile ranges were presented. Wilcoxon signed-rank tests were used to compare pre-percentage and post-percentage overall and within each category of ethnicity, decile and gender. The alpha was set a priori at 0.05.
Qualitative data: Focus group recordings were transcribed verbatim and organised in NVivo 11 (QSR International). Thematic analysis was used to analyse the data. 30 Following familiarisation with transcripts, a process of inductive coding was followed. Throughout this step, the research team convened regularly to discuss the coding process. Codes were grouped into categories, which were reviewed and discussed until final themes were generated. The analysis process was iterative and the team's focus was on the development of themes that were well-explored and supported by the data. 31
Results
Participant demographics
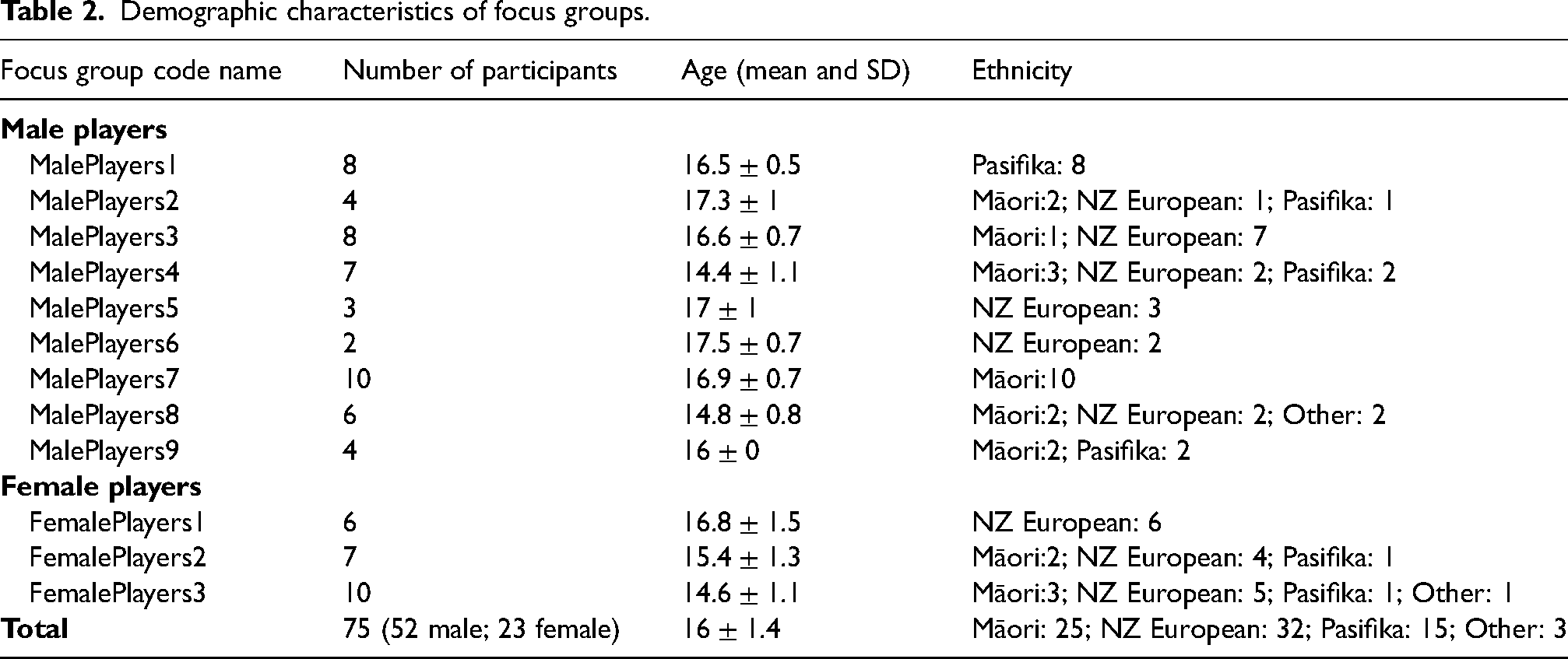
Overall, 596 players were approached to participate, 532 (89%) players provided consent and completed a pre-survey and attended the concussion education session. Of these players, 224 (43.8%) completed a valid post-concussion knowledge and 229 completed a post-concussion attitude (44.2%) questionnaire, for an average attrition rate of 56%. A total of 75 players (52 male; 23 female) participated in the focus groups. Demographic characteristics of participants are summarised in Tables 1 and 2.
High school rugby player survey demographics of those that completed the pre-survey and post-survey (n(%)).
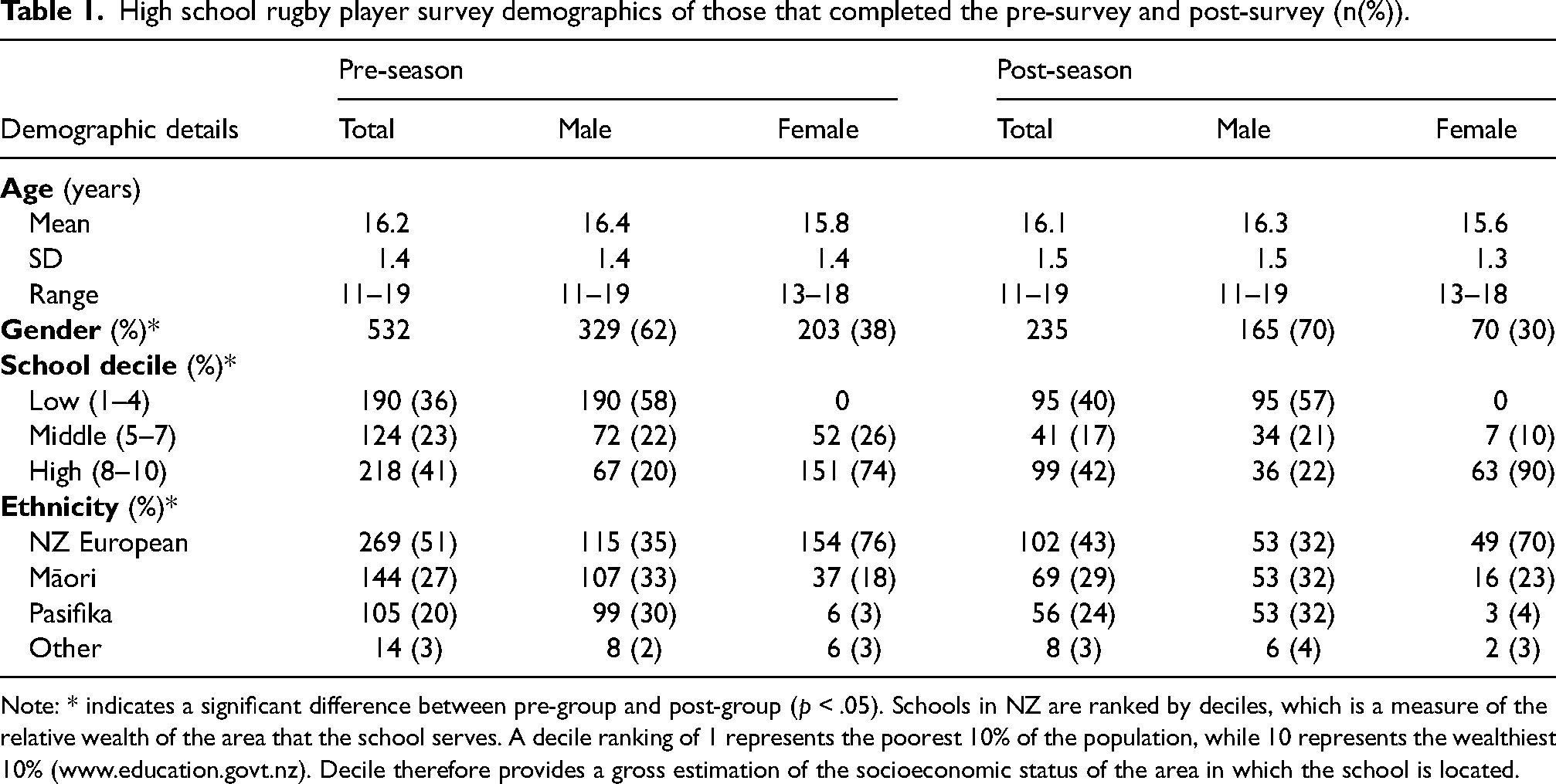
Note: * indicates a significant difference between pre-group and post-group (p < .05). Schools in NZ are ranked by deciles, which is a measure of the relative wealth of the area that the school serves. A decile ranking of 1 represents the poorest 10% of the population, while 10 represents the wealthiest 10% (www.education.govt.nz). Decile therefore provides a gross estimation of the socioeconomic status of the area in which the school is located.
Demographic characteristics of focus groups.
Quantitative
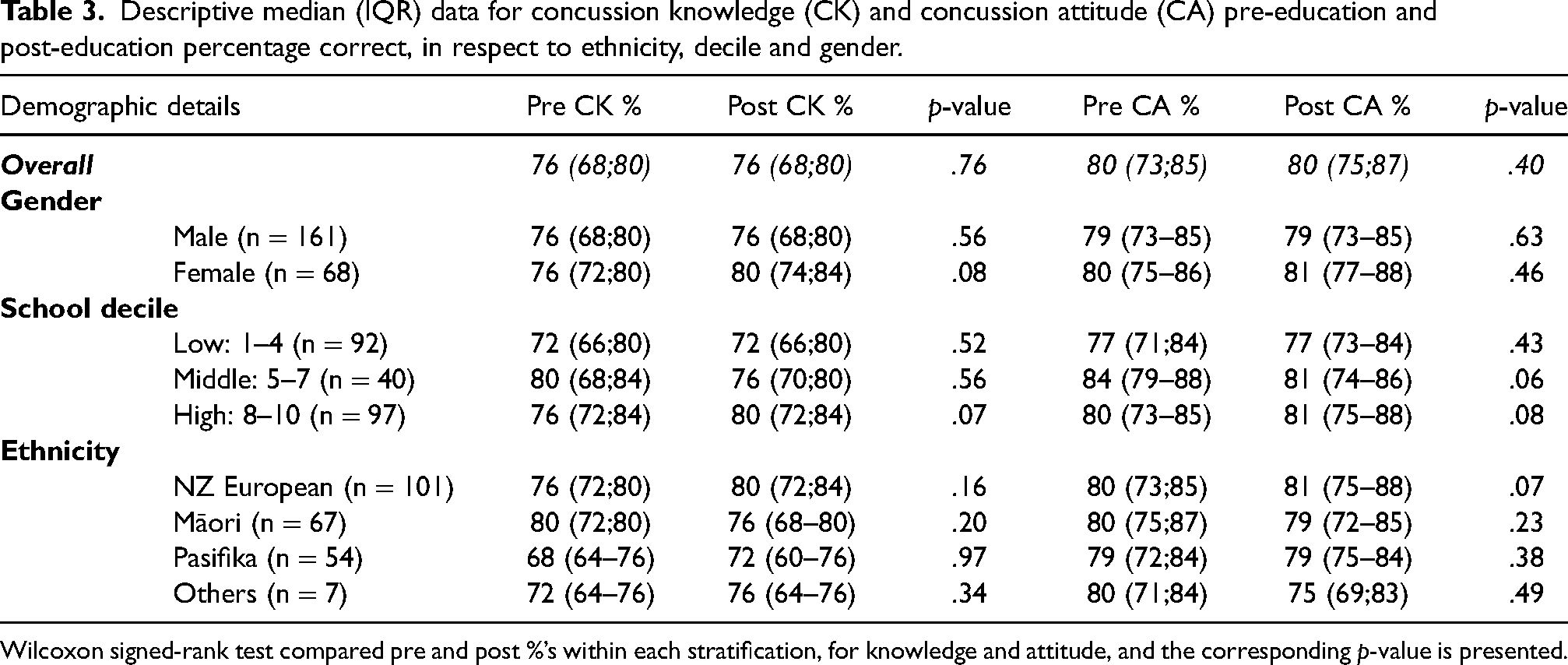
Pre-intervention and post-intervention median and inter-quartile range data are presented in Table 3 overall, and by ethnicity, decile and gender, for concussion knowledge and attitudes. There were no differences in the pre-concussion and post-concussion knowledge or attitudes scores, overall or by ethnicity, decile or gender.
Descriptive median (IQR) data for concussion knowledge (CK) and concussion attitude (CA) pre-education and post-education percentage correct, in respect to ethnicity, decile and gender.
Wilcoxon signed-rank test compared pre and post %’s within each stratification, for knowledge and attitude, and the corresponding p-value is presented.
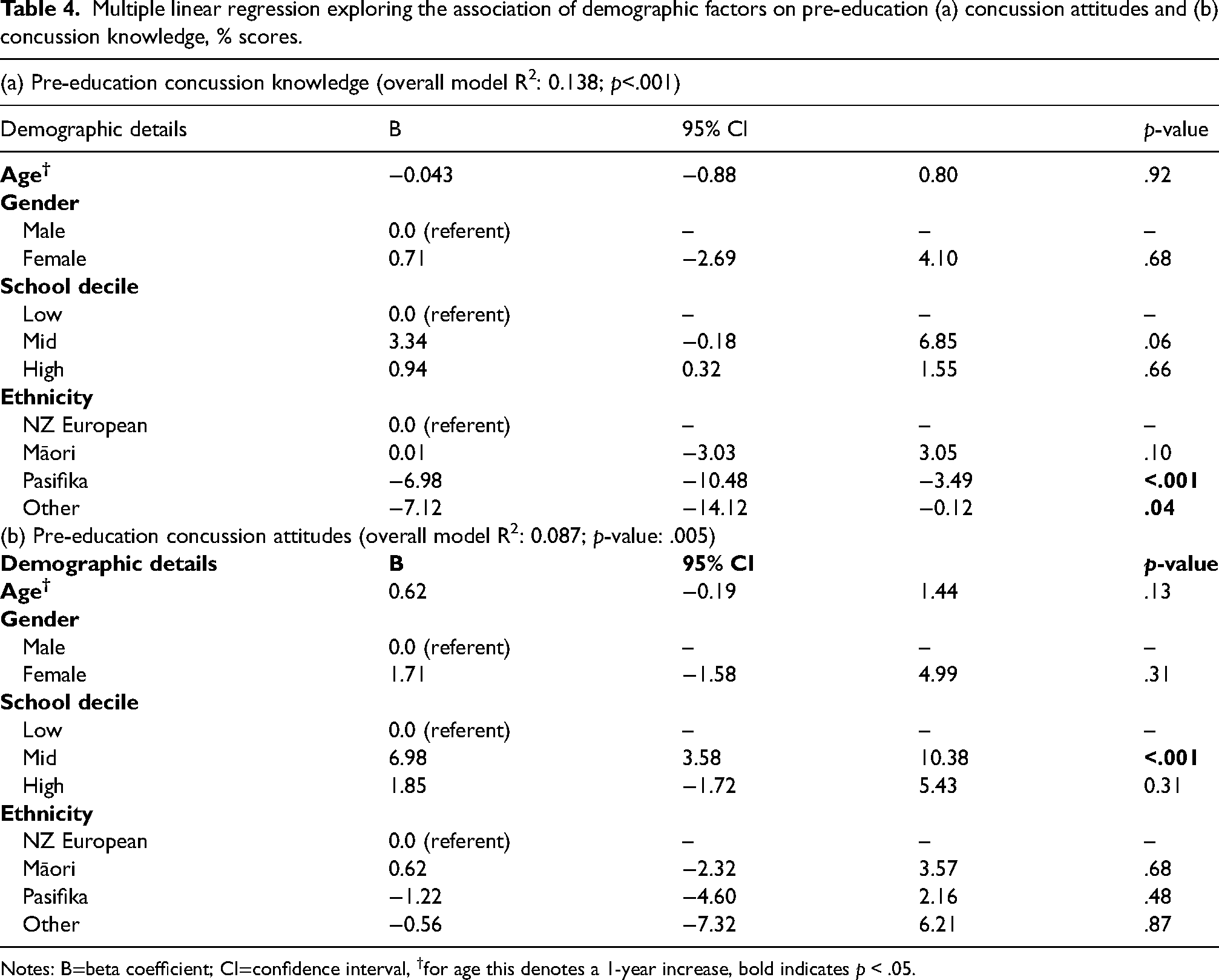
Multiple regression models explored the association of age, ethnicity, decile and gender with pre-education concussion knowledge and attitudes scores and are shown in Table 4. For concussion knowledge, the overall model R2 was 0.14 (p < .001). Only ethnicity was significantly associated with pre-education concussion knowledge scores. Compared to NZ Europeans, Pasifika (beta coefficient: −6.98; 95% confidence interval (CI): −10.48 to −3.49; p < .001) and ‘other’ sub-groups (beta coefficient: −7.12; 95% CI: −14.12 to −0.13; p = .046) were associated with lower pre-education concussion knowledge scores. For concussion attitudes, the overall model R2 was 0.09 (p = .005). Only decile was significantly associated with pre-education concussion attitudes scores. Compared to low-decile, the mid-decile sub-groups were on average, associated with higher pre-education concussion attitudes scores (beta coefficient: 6.98; 95% CI: 3.58 to 10.38; p < .001).
Multiple linear regression exploring the association of demographic factors on pre-education (a) concussion attitudes and (b) concussion knowledge, % scores.
Notes: B=beta coefficient; CI=confidence interval, †for age this denotes a 1-year increase, bold indicates p < .05.
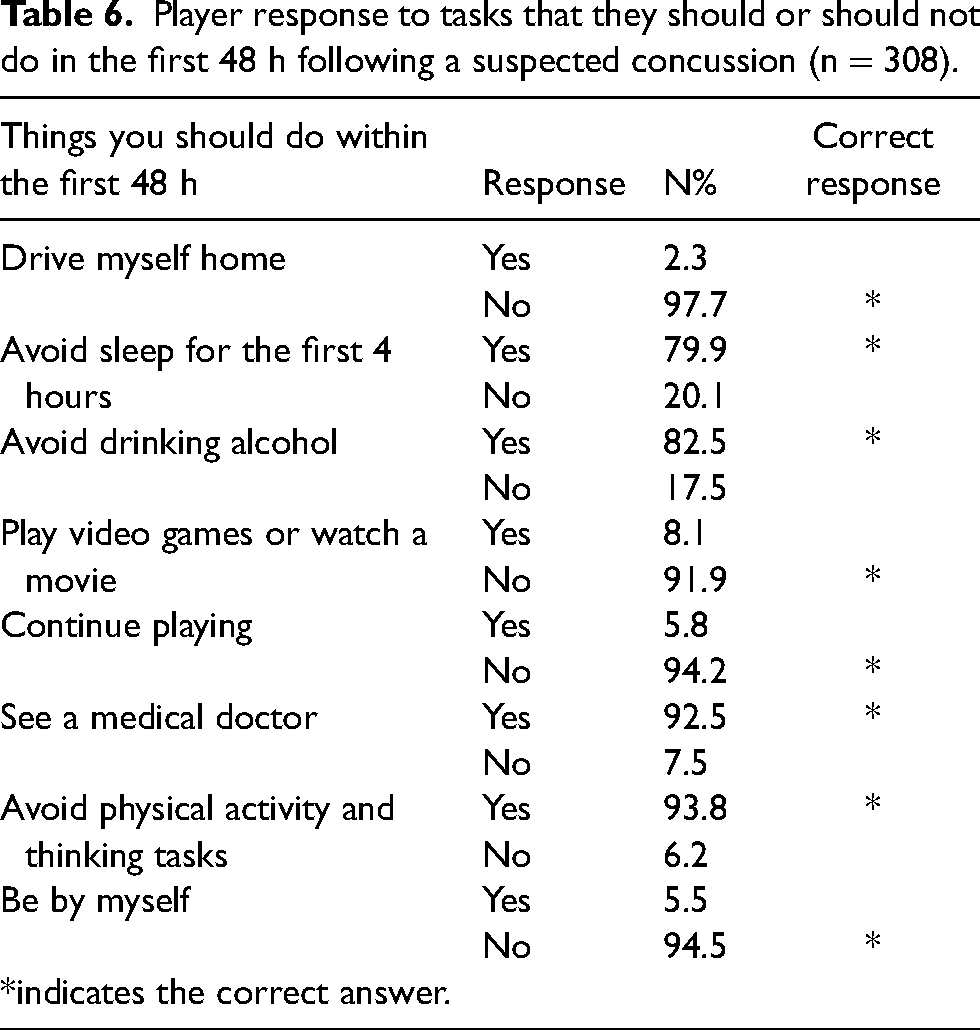
The feedback questions indicated positive evaluations regarding the education intervention with the median response for the five questions being ‘agree’(n = 308), for further details see Table 5. Also, 60% (n = 304) of participants correctly identified the ‘4 R's’ of concussion management in the correct order. Most participants, 91% (n = 280) selected the correct actions to take in the first 48 hours following a concussion (Table 6). Participant preference for future concussion education interventions was in-person (60%), within a mobile app (20%), or online (16%).
Likert scale end-of-season feedback regarding the pre-season education session (n = 308).
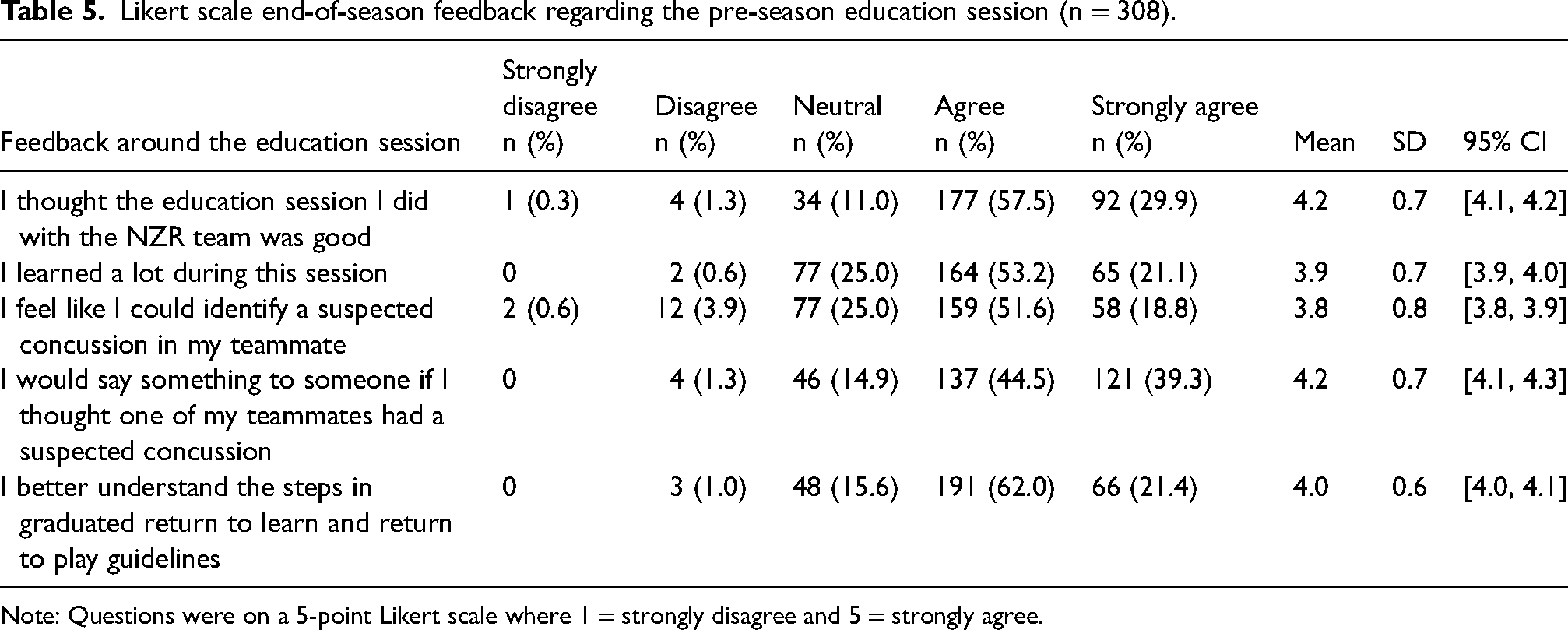
Note: Questions were on a 5-point Likert scale where 1 = strongly disagree and 5 = strongly agree.
Player response to tasks that they should or should not do in the first 48 h following a suspected concussion (n = 308).
Qualitative findings
Three themes with associated sub-themes were derived from the data and are presented in Table 7.
Players’ perceptions of the education session.
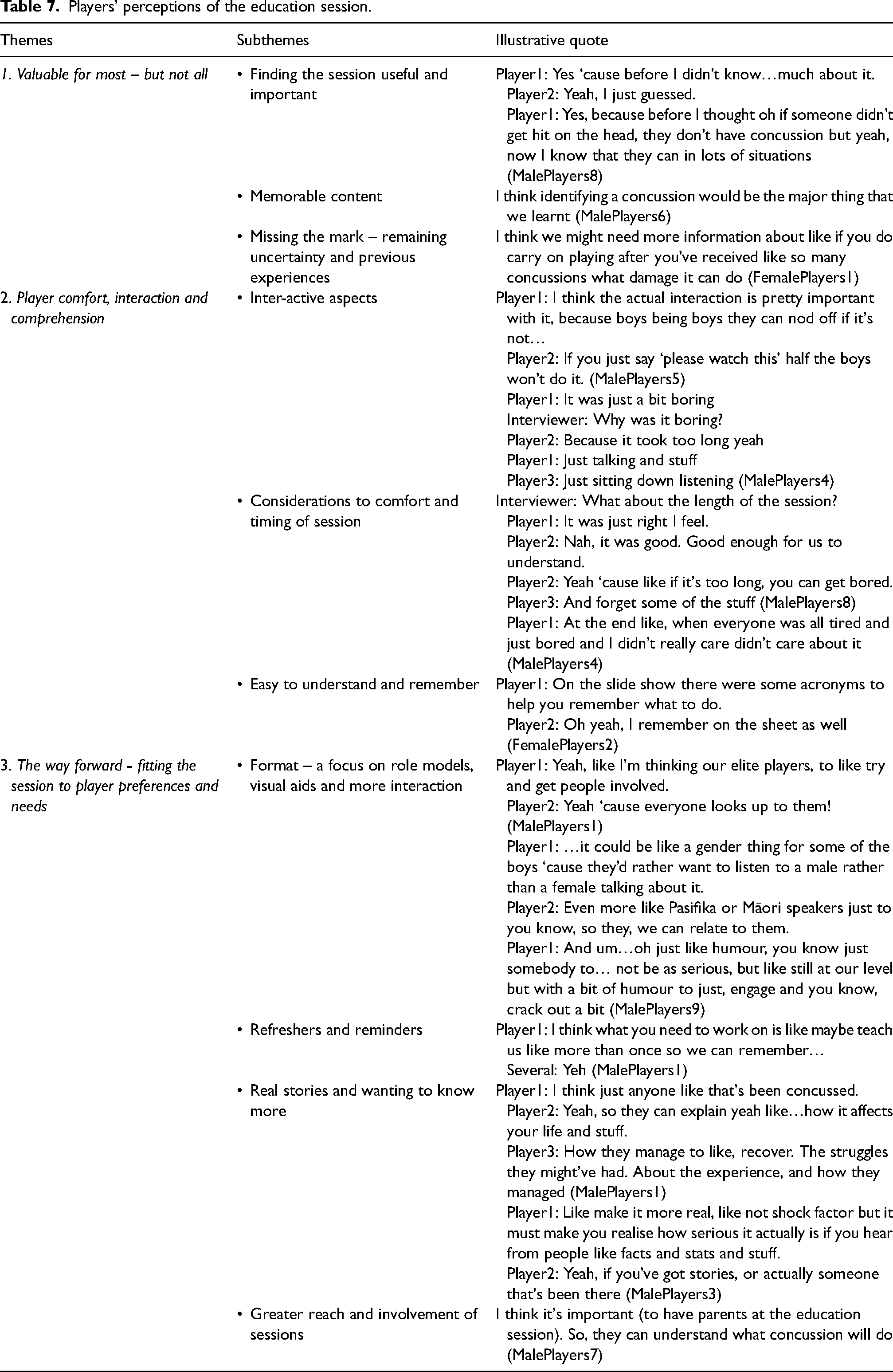
Theme 1: Valuable for most – but not all
Most players found the education session useful and important as it created awareness around the seriousness of concussions, improved players’ confidence in recognising and reporting concussions, and encouraged them to look out for their teammates. Players felt that the session was important enough to be compulsory and that its value extended beyond the context of rugby.
Value was also linked to the content aspects of the session players found most memorable, which were the identification and management of concussion. Specifically, players remembered the ‘4 R's’ (although not always fully), the various signs and symptoms of concussion, as well as some information on what to do in certain scenarios. Players also mentioned that the session highlighted the seriousness or ‘the consequences if you don’t treat it right’.
However, for some players, the session was in some ways, missing the mark. Although these players felt the session made them more aware, they still felt uncertain in some areas. These included being able to confidently recognise a concussion, especially in those instances when concussions were ‘less obvious’. Some uncertainty was also evident around the most likely mechanisms of injury, or ‘how many concussions are too many’. Some players felt they had acquired their knowledge mostly from previous experiences and how that injury was managed, which did not always follow the concussion guidelines.
Overall, this theme (missing the mark) was prominent within focus groups from mid-decile or lower-decile schools or those that consisted of a majority (or all) Māori/Pasifika players. Additionally, female players emphasised the need for more knowledge about the mechanism of injury in different situations, the consequences of a concussion, or the difference between someone who recovers well and those who do not.
Theme 2: Player comfort, interaction and comprehension
Players highlighted the features of the session that worked well such as the interactive aspects and the inclusion of examples or pictures. For most, in-person delivery of the session (‘having someone talk through it’) was important as they felt they were more likely to listen compared to watching a video at home by themselves. Some players commented that the session was easy to understand, the information was new and interesting, and acronyms/mnemonics helped with remembering important content.
Additionally, for some, it worked well because the session was not too long. In this sense, timing and comfort were important and players appeared to prefer education sessions which were ‘fit in during the day, at lunchtime or first thing in the morning’.
Some patterns within this theme were more prominent in focus groups with Māori/Pasifika players or those from low-decile schools. A strong negative perception of the passive aspects of sessions (‘just sitting’ or ‘just being told’) was present. In one focus group, players felt that the session did not succeed in capturing their attention. These players also emphasised the need for delivery of the session in a way that is easy to understand or remember. Similarly, timing and comfort often acted as a barrier in focus groups of either lower decile, Māori/Pasifika, or female teams. Some players in these groups mentioned that the sessions were too long (usually due to additional aspects included before or after the session, such as baseline testing). They would prefer not to have all the content delivered in one session and that the end of the day was not a good time, as players were tired and needed to get home. Additionally, within these groups, players indicated they would like bigger incentives to make the session more enjoyable (e.g., inscribed wristbands, national team merchandise or more food).
Theme 3: The way forward – fitting the session to player preferences and needs
Three main factors were strongly emphasised for future delivery of the session across all focus groups. These factors included (i) format of delivery – a focus on role models, visual aids and interaction, (ii) content – real stories and wanting to know more and (iii) the need for refresher courses and reminders.
Players felt that having role models, such as elite rugby players to deliver the session was important. Players also expressed the need for sessions that were visually stimulating, by having things such as video clips that showed real-life injuries as they happened, which could help to explain more about the mechanism of injury. This included ‘conversation-like’ discussions around different scenarios that may lead to a concussion and activities or ‘mini-games’ to help relay the content. Importantly, players across focus groups stated that they wanted to hear real stories from people who ‘know and understand’ what it feels like to experience a concussion, that could speak about the effect it had on their lives and their experiences returning to play. Refresher courses or more frequent reminders during the season were mentioned often. Players also gave examples of things they would like to see moving forward such as posters in the change rooms or around the school, their coach giving them small refresher sessions, or resources to take home.
Again, some patterns within this theme were more prominent in focus groups with Māori/Pasifika players or those from low-decile schools. These players indicated that they would respond more to a presenter that was funny, energetic and captivating, and that they would prefer a presenter that is of the same gender and ethnicity.
The sub-theme related to reach and involvement, were only present in focus groups of either lower decile, Māori/Pasifika, or female teams. Players in these groups mentioned that extending the education initiative to other stakeholders (parents and coaches) could create more awareness and support. Some players would have liked more union involvement and support. Reach and involvement also meant more visibility of concussions on social media or at school, as this message would also be valuable for other sports.
Discussion
This study aimed to explore the effect of an interactive education session on high school players’ concussion knowledge and attitudes, and to explore the impact of player demographics on these outcome variables. In addition, focus groups were used to gain a deeper understanding of the players’ perceptions of the education session. The findings showed that a one-off education session in this cohort was not successful in improving concussion knowledge or attitudes 2-month post-intervention. Although players provided positive feedback with regard to what they learned and the value of the sessions, aspects that could be improved were also highlighted, with a particular focus on the use of role models, real-life experiences, and sessions that are culturally responsive.
Results from the RoCKAS questionnaire show that prior to the education session, Pasifika and ‘other’ players’ pre-education concussion knowledge was significantly lower than that of NZ Europeans, similar to previously reported findings. 6 Differences were also observed for concussion attitudes of players from mid-decile schools, who had significantly higher pre-education concussion attitudes scores compared to players from low-decile schools. However, all three school decile groups in this study at both evaluation time points achieved high scores for concussion attitudes in the range of 77% to 84%, which may represent a ceiling effect for this measure, possibly explaining the lack of change. Our results align with those from previous studies, where no significant differences in concussion attitudes after an education intervention were seen. 26 However, the stability of the scores in players from low-decile schools and the improvement in players from high-decile schools is encouraging, as previous research found that players’ attitudes towards reporting concussions decreased as the season progresses. 16 Nonetheless, an area of concern is that Pasifika players and those from low-decile schools’ concussion knowledge and attitudes scores both fell below the median score of the overall group, highlighting the need to explore these results further and the importance of education that is culturally responsive. Consequently, the secondary aim of this study was to improve our understanding of the factors that may influence player engagement with a concussion education session and their experience with the content delivered (e.g. understanding and meaningfulness).
Focus groups discussions indicated that players were mostly positive about the education intervention, and this was also evident in the post-education survey. The survey indicated that 60% of players were able to correctly identify the ‘4 R's’ of concussion management. Most players (91%) identified the correct injury management behaviours to undertake/avoid in the first 48-hour post-injury. Similarly, in the focus groups, most players felt that the education session improved their awareness and ability to identify and manage a suspected concussion. Although knowledge is not directly related to behaviour, it is an essential moderator of behaviour. 19 The first step to increasing injury disclosure is players’ ability to identify the early signs and symptoms of concussions. 32
In contrast, some players felt they had acquired the majority of their knowledge from previous concussion experiences. It is difficult to challenge these existing beliefs, especially if players do not perceive the education session as valuable or important. Therefore, identifying the factors that help facilitate a positive shift in player attitudes towards concussion education is an important starting point. In this study, positive attitudes towards the session were facilitated by inter-active aspects, information that was new and easy to understand, and sessions which were well-timed and considered player comfort. Conversely, players who felt that the session failed to capture their attention, naturally saw less value in the session. These factors highlight the importance of favourable attitudes towards an education session, but also that these attitudes may be greatly dependent on format and delivery.
Players identified specific areas for improvement that would enhance the acceptability and ‘fit’ of the sessions. One such consideration is the need for regular refresher courses and reminders of the education content. Although these factors have been consistently identified in previous research, they can often be difficult to implement in the community context due to resource limitations (e.g. scheduling restrictions, limited funding, lack of access to experts).33,34 This highlights the importance of engaging with the entire rugby system, from the governing bodies through to the immediate environment, to ensure the whole system provides meaningful and engaging educational opportunities. A recent consensus on improving concussion education recommended that education should be provided not only on a regular basis but also in different ways, such as informal conversations and posters. 35 In this study, practical suggestions for the improvement of the education session included more interactive aspects, with discussions, games, visual aids and content that were ‘real’. By incorporating these aspects into future education interventions, players may feel more engaged with the content.
Previous work has highlighted that reporting intention is a strong predictor of behaviour, and thereby concussion disclosure.8,13 Thus it is critical to identify the factors, such as concussion attitudes, that facilitate reporting intention. Findings within the broader NZR concussion project 29 and in previous studies have shown that although players may understand the seriousness of concussions and the role they play in their management, conflicting attitudes (e.g., not wanting to let the team down, pressure to win) or contextual factors can negatively impact safe concussion management behaviours.14,32 Attempting to change these attitudes with a one-off education intervention is challenging. Making the content ‘real’ would work to illustrate that concussion management is supported at a cultural level, which may facilitate a shift in attitudes towards more positive reporting behaviours. Throughout the focus groups, players emphasised the need to hear from role models, and to hear real stories of how concussion has affected players’ lives. Powerful stories can evoke an emotional response that may lead individuals to question deeply held assumptions and beliefs. 36 Additionally, emphasis on role models for content delivery is perhaps a crucial point as subjective norms are known to be an important predictor of behaviour in adolescent populations. 37 Kerr et al. 38 reported that the endorsement of ‘opinion leaders’ are important for favourable concussion attitudes and behaviours. Additionally, the utilisation of a peer-mediated approach to concussion education has shown promise by improving concussion knowledge, concussion attitudes, reporting intention and facilitating attitudinal changes that support peer-recognition among student-athletes.39,40 Regardless of the approach, identifying relevant role models for the target population appears to be an integral step in facilitating players’ perceptions of the session's acceptability.
The qualitative findings from this study documented shared values and experiences across players, some context-specific considerations highlight the dynamic interplay between ethnicity, socioeconomic status, concussion knowledge, and attitudes. Firstly, the need for presenter diversity and role models was voiced strongly by Māori and Pasifika players. These factors may play an integral role in facilitating improved connections with the target audience. For example, the quality of relationships has been identified as a significant factor in Pasifika and Māori education and supportive relationships with peers and mentors in a culturally relevant environment, which may be critical to student success.41–43 Continued efforts are required, particularly those that incorporate Māori and Pasifika ways of negotiating knowledge. This is particularly important for educational efforts that are targeted at Pasifika players who achieved the lowest concussion knowledge scores. While not statistically significant, it may be worth noting that the Māori cohort achieved an above-average score for concussion knowledge before the intervention and were the only players to record a decrease in concussion knowledge post-season.
The qualitative findings suggested that knowledge provision requirements for female players may be different to those of males. In this study, the majority of female players had only played rugby for 1 to 2 years. In comparison, male players had more playing experience, thereby increasing the likelihood of having previously sustained a concussion or exposure to a teammate who had. A previous study had shown that as high school players’ playing experience increased, so did their concussion knowledge. 6 Despite the difference in playing experience in the male and female players in the current study, no differences were observed in concussion knowledge (or attitudes) between these two groups, suggesting females may have a higher level of baseline knowledge. Despite the absence of difference, females still reported feeling uncertain about many aspects of concussion. These uncertainties and frequent lack of medical support many women's teams face in the community game highlights the importance of ensuring coaches and support staff have a good knowledge of concussions and their management. Additionally, gender stereotypes created within a cultural and societal context may affect how females perceive their level of knowledge and competence. 44 In this sense, building trusting relationships and providing opportunities for open discussions around these uncertainties, may be paramount for female players.
Finally, it was clear that when players found the sessions easy to understand, their perceptions of the session were more positive. Similarly, within the lower-decile and Māori/Pasifika groups, the need for acronyms and key messages was voiced. The relatability of the session is thus important in terms of language and communication, specific for the target audience. The need for additional support from other stakeholders, considerations of comfort and timing of sessions and the need for external motivation (incentives) were also especially pertinent in lower-decile and Māori/Pasifika groups. It must also be taken into consideration that discrepancies in the quality of coaching, resources and level of medical support in high compared to low-decile schools may create a context that is not as supportive. Research has highlighted the importance of the role that the coach plays in developing a supportive environment, as well as the level of concussion reporting when there is a healthcare professional involved with the team.8,45 Collectively, these demographic groups may require additional support, facilitation of supportive environments and tailored interventions.
This study is not without limitations. It included high school rugby players in NZ and thus may not be generalisable to other sporting codes. Additionally, the schools and teams that chose to participate in this study may be different from non-participating schools in terms of their support for concussion management and reporting practices. Similarly, it is also possible that the players who opted to complete the post-concussion knowledge and attitudes surveys may be the ones with higher concussion knowledge and attitudes scores. It is possible that these factors may have led to an overestimation of NZ high school rugby players’ concussion knowledge and attitudes. Securing participation of schools in research projects can be challenging and we acknowledge that this is an important limitation. Notwithstanding these challenges, our sample is still substantially larger than most research published in this field, and despite the possible bias of those who completed the survey post-season we did not observe a significant difference in concussion knowledge or attitudes.
Furthermore, there was a limited time for the delivery of the education session, both in terms of the length of the session and scheduling of the session at an appropriate time. Session time and room choice/availability were dependent on the school. While this is a common constraint for community or school-based projects, providers of the education session could track the context of the education session at each school (i.e., tight time frame, students’ engagement, room comfort and timing).
A higher proportion of males completed the post-survey assessment, which may be explained by the difference in the competition schedules. The 2-month period for follow-up was 2 weeks after the female season finished and it was difficult to obtain follow-up from these players, whereas the male players were still in-season. Finally, there appeared to be ceiling effects of the RoCKAS-ST for concussion attitudes. 26 Despite these limitations, this study is an important step in the evaluation of concussion education in NZ as it provides insight into the preferences for education that may lead to improved outcomes in concussion knowledge, concussion attitudes, and behaviours.
Practical application
The perceptions of players and factors that may influence education uptake identified in this study should be incorporated and accounted for in future education sessions.33,34 The findings suggest the need for education to evolve and align with the needs of adolescents, while considering pragmatic and practical factors, as well as challenges of the local context. 46 Importantly, greater consideration of demographic factors is required in the development and implementation of education interventions. Apart from players, it is also important to consider how information is translated throughout the other stakeholder groups. 20 Many current education programmes are still targeted to individual stakeholder groups, rather than the system as a whole (i.e. including coaches, parents, players, etc.). To encourage real systemic change, meaningful education programmes are required to address the underlying components of behaviour change (i.e. TPB) for all key stakeholders in the community rugby system. Coaches are ideally suited as mentors to create a culture of safety that does not support playing through an injury.8,47 Research has shown that athletes who felt supported and could communicate with their coaches were more likely to report a concussion.8,48 Other studies suggested that nurses are also often important contact points for players. 49 Considering the inclusion of such stakeholders may help mitigate the limitations of a one-off education session, by driving a more sustained, multi-pronged approach. 35
Although it is clear that a continuous and full systems approach to concussion management is required, it is also important to ensure that each stakeholder feels meaningfully involved throughout the process. 50 In the present study, players specifically voiced the need for autonomy and some control over the learning process (‘we don’t want to just be told’), which also relates to the preferred content and who delivers that content. Furthermore, although anecdotally, researchers observed that player engagement was often related to whether the school contact or coach endorsed or was present during the session. Such presence highlights the wider systems approach and should be explored in future work.51,52
Conclusion
In high school rugby players, a one-off education session was not successful in improving concussion knowledge or attitudes. Although players mostly perceived the education session to be valuable, areas for improvement were suggested and nuanced needs of different demographic groups were voiced. Players emphasised the need for relatable role models and content that was ‘real’. These findings emphasise the need to move towards a greater consideration of demographic factors, as well as the local context, in the development and implementation of education interventions. Changing knowledge and attitudes with a one-off education intervention is a complex and challenging task, particularly given the high level of baseline concussion knowledge and attitudes scores observed in the current cohort. Strategies that further harness the power of subjective norms should be addressed more explicitly. Additionally, a systems approach that facilitates knowledge translation in a more sustained way, may enhance concussion knowledge and attitudes at a community rugby level.
Supplemental Material
sj-docx-1-spo-10.1177_17479541231156159 - Supplemental material for Concussion education for New Zealand high school rugby players: A mixed-method analysis of the impact on concussion knowledge, attitudes and reporting behaviours
Supplemental material, sj-docx-1-spo-10.1177_17479541231156159 for Concussion education for New Zealand high school rugby players: A mixed-method analysis of the impact on concussion knowledge, attitudes and reporting behaviours by Danielle M. Salmon, Marelise Badenhorst, James Brown, Janelle Romanchuk, Zachary Yukio Kerr, Simon Walters, Amanda Clacy, Sierra Keung, S. John Sullivan and Johna Register-Mihalik, Chris Whatman in International Journal of Sports Science & Coaching
Footnotes
Acknowledgements
Funding for this study was provided by World Rugby, the New Zealand Rugby Foundation and by the NZR and ACC injury prevention partnership. The funders were not involved in the study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the article for publication. The authors would like to acknowledge the support of the high schools and the players, parents and coaches who volunteered to participate in the focus groups. We would also like to thank the Provincial Rugby Unions who agreed to participate in the study and for their assistance with recruitment. For their help conducting and facilitating the focus groups the authors would like to thank Dr Jason Chua, Jody McGowan, Jayden Pinfold, Sarah Kay, Dr Phil Handcock, Sam Miratana, Eleanor Butterworth, Simon Culley and Bella Anastasiou.
Authors’ contributions
DMS, SW, SK, JR and AC designed the study, contributed to data collection, data analysis and interpretation. CW and SJS contributed to the design of the study. MB, ZYK and JR-M contributed to data analysis and interpretation of results. All authors contributed to the manuscript writing.
Author note
James Brown is currently affiliated with Carnegie Applied Rugby Research (CARR) Centre, Carnegie School of Sport, Leeds Beckett University, Leeds, UK.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DS and JR are employed by New Zealand Rugby.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Accident Compensation Corporation, World Rugby, New Zealand Rugby Foundation (grant number RugbySmart, Player Welfare Research Grant).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.