
Abstract
Provincial academies represent an important bridge between amateur and professional level rugby union in New Zealand. Athletes are provided with professional-level coaching; however, limited direct nutrition support is available. Congested training schedules and the requirement to work or study due to a lack of financial support may present a challenge towards athletes meeting nutrition requirements. The aim of the study was to facilitate improvement in nutrient intake, body composition and subjective well-being in provincial academy athletes via the implementation of a nutrition-support protocol based around behaviour change techniques. Significant increases in total energy (pre: 2492 ± 762 kcal; post: 2614 ± 625 kcal), relative energy (pre: 24.4 ± 7.5 kcal·kg; 25.5 ± 6.0 kcal·kg), total protein (pre: 131.1 ± 41.8 g; 153.8 ± 37.1 g) and relative protein (pre: 1.3 ± 0.4 g·kg; post: 1.5 ± 0.3 g·kg) were observed. Furthermore, changes in subjective sleep quality, stress, mood and upper body soreness were observed following the intervention. No changes were observed in body composition, carbohydrate or fat intake. Significant variability in nutrition and body composition changes highlights the importance of applying an individualised approach to nutrition support provision in developmental athletes. Practitioners working within these environments should be aware of the challenges and influences contributing to athletes’ nutrition choices and habits.
Introduction
Rugby union (‘rugby’) is a popular intermittent team sport in which players engage in high-intensity activity bouts interspersed with low-intensity periods. Additionally, players engage in contacts and collisions in the form of tackles, scrums, rucks and mauls. 1 Major differences in both body composition and on-pitch roles lead to heterogeneous training and match demands in rugby players. Forwards are taller and possess greater total, lean and fat mass than backs. 2 Backs cover greater distances during matches (6127 ± 724 vs. 5812 ± 666 m) and spend more time performing high intensity running (1.6 ± 0.5 vs. 1.1 ± 0.4%) however forwards engage in more high intensity activity (11.5 ± 1.8 vs. 3.8 ± 1.3% total match time) due to involvement in static exertion events such as scrums. 1 Furthermore, forwards engage in a greater number of high force collisions during matches than backs. 3 Due to the unique and variable demands and characteristics, rugby players would benefit from an individual approach to their nutrition recommendations and requirements.
Energy intake must be adequate to maintain normal physiological functioning 4 and meet the unique demands of the sport. Across a two week in-season period, elite rugby union players expended 4365 ± 1122 kcal daily, representing 61 ± 10 kcal·kg·FFM. 5 Furthermore, a single bout of training containing 20 collisions resulted in a likely greater energy expenditure over the five-day monitoring period including the collision-based activity session. 6 Whilst differences between forwards and backs are apparent both groups can expect to engage in ˃20 collisions per match7,8 resulting in alterations to energy metabolism. Indeed, energy expenditure following game days (GD)(GD + 1 and GD + 3) appears greater than before (GD-1). As external GPS training and match-play and internal subjective perceived exertion loads were similar on all days of monitoring, the greater energy expenditure observed can likely be attributed to the collisions experienced during match-play. 9
Rugby players utilise both aerobic and anaerobic metabolic pathways to replenish ATP during match-play. Sub-optimal carbohydrate (CHO) availability can interfere with both pathways, resulting in fatigue. 10 Furthermore, low CHO availability for the brain can impair cognitive function and result in sub-optimal decision making and concentration. Muscle glycogen can be depleted rapidly in response to high-intensity intermittent activity such as that observed in rugby match 11 ; previous research has demonstrated a 40% muscle glycogen depletion following a rugby match, 12 supporting the reliance on CHO as a fuel source for rugby players. Additionally, those engaging in multiple daily training sessions should prioritise carbohydrate intake throughout the day to optimise glycogen re-synthesis and ensure effective re-fuelling. 13
Dietary protein is essential for health, repair and re-modelling of damaged tissue following exercise and promoting adaptations. 14 Total protein intake is an important consideration for enhancing the muscle protein synthetic response and eventual fat free mass development 15,16 which can positively influence speed, power, endurance and agility. 17 Requirements for protein intake in athletes are broad (1.2–2.0 g·kg·d)18,19 with no difficulty in meeting these requirements found in professional20–23 and/or developmental rugby players.24,25
In New Zealand, there are unique opportunities for developmental rugby players to be selected to participate in academies. Academies are designed to provide young players with coaching support, professional level programming and access to facilities and skills to prepare the individual for either professional level play and/or a future outside rugby. Academy rugby players in New Zealand are a unique population in that they engage in academy sessions with the aim to develop and potentially play as professional athletes whilst still training and playing at the local amateur club level. Due to the lack of financial assistance associated with receiving a professional contact, academy players need to consider additional obligations such as work and study. This represents a unique challenge for the athlete meeting appropriate nutrition requirements, particularly when multiple daily training sessions are required, 13 and may require specific guidance due to the high training volumes, with convenience, food availability and family likely to influence choices athletes make.26,27 Furthermore, many young and developing athletes are unlikely to possess appropriate nutrition awareness or an ability to purchase and prepare meals resulting in a risk of under-fuelling.28,29 These barriers may be influenced by poor nutrition knowledge, a potential major factor in the athlete making appropriate food choices to support sporting performance and health. 30
A lack of data exists regarding nutrition in developmental players in New Zealand despite representing an important bridge between club and provincial level rugby and engaging in high training volumes. The present team-based case study aimed to explore the impact of a structured nutrition support programme on energy and macronutrient intake in academy rugby union players, with body composition changes and subjective well-being presenting secondary objectives. We hypothesised that provision of nutrition support would facilitate improvements in the aforementioned variables.
Methods
Participants
Seventeen players from a provincial rugby union academy volunteered to participate in the study. At the time of data collection, all participants trained with both the provincial academy and their local club whilst engaging full-time in outside obligations, such as work and study. Training demands of the participants during data collection are described in Table 1. At the time of data collection, nutrition support for the team totalled 6 h per week, spread across all players associated with the club (contracted male players, contracted female players and academy players). Participants provided written informed consent and ethical approval was obtained by the University of Waikato Human Research Ethics Committee (HREC(Health)2020#46).
Participants’ weekly training schedule.
Research design
The current study utilised a non-randomised cross-over design, with participants completing both a monitoring and intervention period simultaneously; randomisation was unfeasible due to the nature of the intervention. During the monitoring period, participants logged their full dietary intake including all meals, snacks and beverages; a high-training volume, low-training volume and rest day were monitored each week. Following a four-week monitoring period, basic nutrition education was provided during a one-week period during which no dietary intake monitoring occurred. Dietary intake was then monitored for another four weeks, with active input provided to assist with optimising nutrition intake in-line with best practice sports nutrition recommendations.18,19 Body composition was measured using a three-dimensional optical scanning device (FIT3D®, San Mateo, CA, USA) 31 prior to the monitoring period and both prior to and following the intervention period. Finally, subjective fatigue, sleep quality, muscle soreness, stress and mood were measured weekly following the Monday morning training session.
Nutrition support intervention
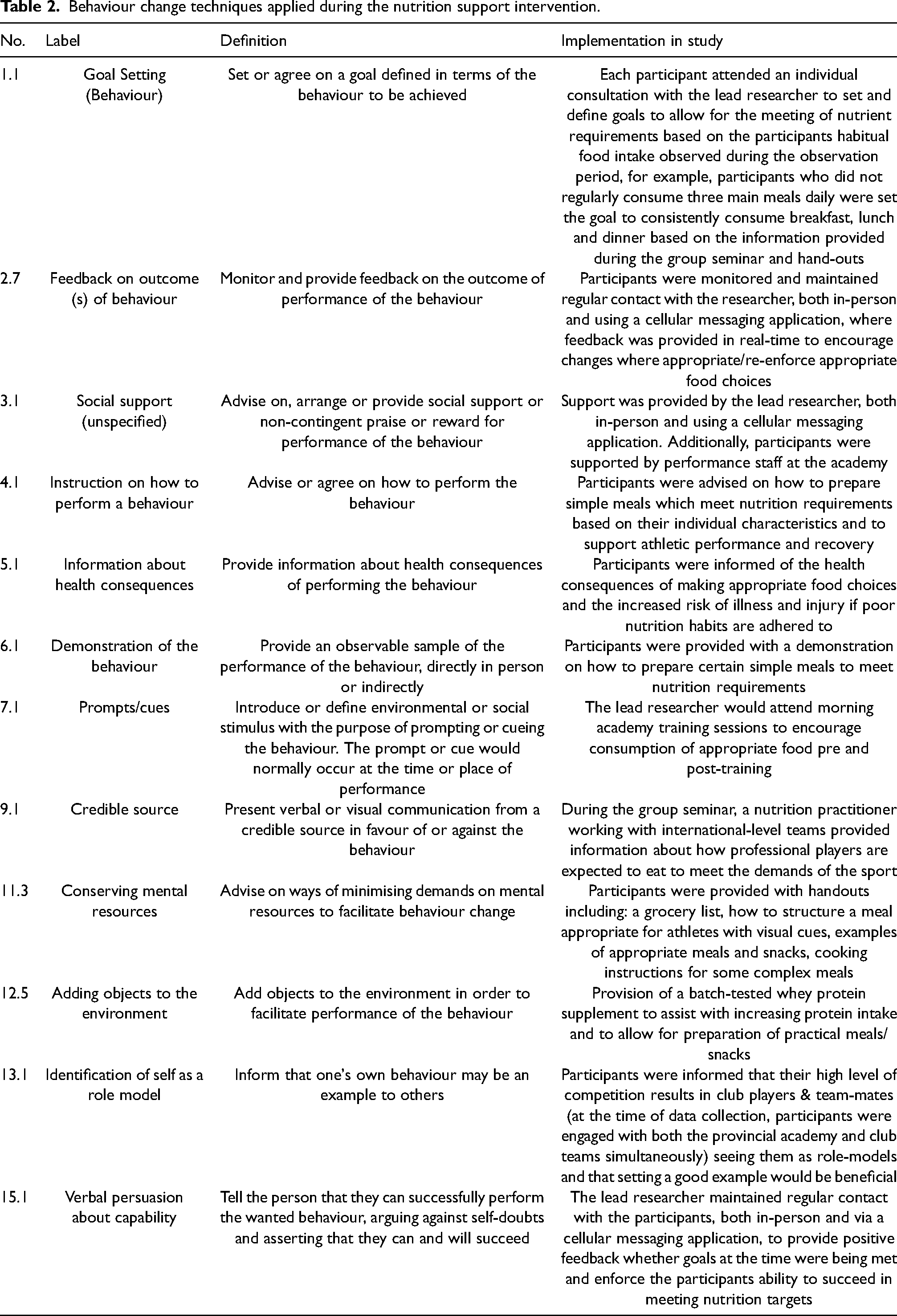
The delivery of nutrition support was provided by the lead investigator, a certified nutritionist, in conjunction with high performance support staff at the club and was provided on both an individual and group level. The nutrition support implemented behaviour change techniques (BCTs) as described by Michie et al. 32 The BCTs implemented in the present study are detailed in Table 2.
Behaviour change techniques applied during the nutrition support intervention.
As a group, participants attended a 60-min seminar detailing their collective macronutrient intake during the monitoring period. Information regarding meeting macronutrient requirements and improving diet quality, from both a health and athletic standpoint, was provided along with strategies to facilitate this. Participants were provided with hand-outs containing information detailing how to appropriately structure a core meal to meet nutrition requirements for an athlete. Ranges of nutrients were provided to account for the heterogeneity in body composition and on-field demands of the participants, which were then customised during individual consultations. Hand-outs were also provided to address example meals and snacks, recipes for example complex meals and a grocery list.
During the week following delivery of the group seminar, each participant was provided with a third party-tested whey protein supplement (Combat 100% Whey, MusclePharm, Calabasas, CA, USA batch #A163830620A) and had an individual 10-min consultation to discuss personal goals for the intervention period. During these consultations, the lead researcher and participant identified strategies to assist them in reaching their overall and per-meal nutrition targets. Such strategies included choosing meals which could be prepared with minimal time available and/or in bulk, identifying meals which align with family and/or friends’ preferences and goals and choosing convenience and takeaway options that provide appropriate nutrient composition and density.
Throughout the intervention period, regular contact was maintained with participants both in-person during the academy gym training sessions and using a free cellular messaging application (WhasApp, Inc., Santa Clara, CA, USA). This contact allowed the lead researcher to monitor food intake, suggesting changes and re-enforcing good practices where appropriate.
Body composition
Body composition was measured using a three-dimensional optical scanning device (FIT3D®, San Mateo, CA, USA). 31 Such scanners produce a three-dimensional avatar of the body allowing for anthropometric assessment. Prior to baseline body composition analysis, participants body mass and height were recorded. The device was installed in a room with no natural light interference and shiny surfaces covered. Participants were required to create an account with FIT3D®, allowing for repeated use and their own access to body composition results. Following account creation, users are presented with instructions via the attached monitor for accurate body composition analysis. The participants were asked to remove all clothing to underwear and tie their hair up above their head if necessary. Prior to commencement of the scan, participants were required to hold two handles allowing for an anatomical position to be maintained. Participants were asked to stand still and look forward for the 40-s scan duration.
Body composition analysis was conducted at baseline, immediately prior to delivery of the nutrition support intervention and the final week of the intervention period. Baseline and pre-intervention scans were completed in the morning (05.00 – 06.00) in a fasted state prior to training. Due to a change in the athletes’ schedules, post-intervention scans were completed at lunchtime, whereby the participants had engaged in a training session and were likely not fasted (12.00 – 14.00). Coefficient of variation ranged for between-day reliability of the device used for lean mass and fat mass is 0.0–1.8% and 0.3–6.4%. FIT3D® scanners have previously demonstrated equivalence to a four-compartment model for lean mass and fat mass measurements. 31
Dietary intake
Dietary intake was monitored using the remote food photography method (RFPM). Two consecutive days during the week were monitored; a high-volume day, during which participants completed two training sessions and a low-volume day, whereby participants completed a single training session were observed. Additionally, a weekend day whereby no structured training sessions set by either the academy or amateur club was monitored.
Photographs were uploaded using a mobile phone application (MealLogger, Wellness Foundry, Ashburn, VA). MealLogger was chosen as it allows for users to upload photographs with descriptions to assist with the identification and analysis of foods or items and the use of the RFPM has been demonstrated as a valid dietary analysis tool in rugby athletes. 33 Additionally, the application is preferred to traditional dietary analysis methods in athletes. 34
Participants were instructed to take a clear photo of all meals, food item or beverage consumed and including a hand, pen or cutlery in the picture to act as a size reference. Multiple pictures were encouraged if participants were preparing complex meals. Participants were encouraged to provide as much detail in the description box as possible to assist with the analysis, including using weighing scales if available, detailing other common house-hold measures, including brand names and portion sizes and detailing cooking methods, condiments or beverages.
Participants were contacted for any clarifications regarding logged items or meals if the quality of either photographs or descriptions was inadequate using WhatsApp. Additionally, each participant was contacted the morning following each monitoring day to both provide clarification on uploads if required and to recall the previous days intake and tease out unlogged items if appropriate. If a participant did not provide information, adequate photographs and/or descriptions or could not describe food eaten out (e.g. a meal at an establishment from which nutrition data could be found) the day was excluded from analysis.
Dietary intake was analysed using FoodWorks 10 (Version 10.0.4266, Xyris Software, Australia) as it contains a comprehensive database of food items in both Australia and New Zealand. If a food item was not present in FoodWorks, energy and macronutrient information was collected from food labels or the company website. Analysis was conducted by a registered nutritionist with the Nutrition Society of New Zealand for consistency.
Daily dietary intake was analysed for energy intake, energy intake relative to lean body mass, total and relative to bodyweight macronutrient intake (protein, carbohydrate and fat).
Subjective wellbeing
Participants completed a short 5-point wellbeing questionnaire previously used in rugby athletes 35 to measure subjective fatigue, sleep quality, upper and lower body muscle soreness, stress levels and mood. The questionnaires were completed on a weekly basis following a Monday morning gym session (07.00 – 07.30). Weekly questionnaires were distributed using an online form (Google Forms, Google, CA, USA) and completed on a personal mobile phone at the end of the gym session.
Analysis
Statistical analysis was conducted using SPSS (Version 27, IBM Corp., Armonk, NY, USA) with significance set at p ˂ 0.05. Shapiro-Wilk testing was applied to determine normality, with energy and macronutrient intake deemed nonparametric. Descriptive statistics are displayed as means ± SD.
To account for data on days where nutrient intake could not be determined due to missing or incomplete information, data were cleaned using ‘replace missing values’, whereby new values were added to reach the same mean and SD and allow for analysis. Wilcoxon-signed rank-sums test was applied to analyse changes in total nutrient intake. Changes in body composition variables and change in total wellbeing scores across the four-week blocks were analysed using a repeated-measures ANOVA.
Results
Participants
Of the original participants, two were excluded due to injury and illness, three were excluded due to inadequate adherence to the dietary analysis study procedures and one was excluded due to leaving the academy. Dietary and subjective well-being analysis was conducted on ten participants due to providing limited data for analysis, whilst body composition analysis was conducted on twelve participants (body mass: 102.4 ± 18.2 kg; height: 185.7 ± 9.5 cm; age: 20.5 ± 1.6 years). Of a potential 90 days dietary analysis, 57% and 46% of days were sufficiently logged for analysis during the monitoring and intervention periods, respectively. All participants completed each subjective well-being questionnaire during the monitoring period, whereas one participant did not complete a full week and two participants did not complete one day of upper body muscle soreness and mood, respectively. All eligible participants completed all three body scans.
The 12 total participants represented a variety of positions: prop (n = 2), lock (n = 3), flanker (n = 2), half-back (n = 2), centre (n = 1), wing (n = 1) and full-back (n = 1). Of the 10 participants included in dietary analysis, living situations were reported as living in house-shares (40%), with family or other caregivers (40%), alone (10%) and with a partner (10%). One participant followed a pescatarian dietary pattern whilst the remaining participants followed an omnivorous dietary pattern.
Total nutrient intake
Changes in total nutrient intake between pre- and post-intervention are displayed in Table 3 with individual changes displayed in Figure 1. Total (p = 0.02) and relative (p = 0.04) energy intake were greater post-intervention. Additionally, total and relative protein intake significantly increased post-intervention (p < 0.001). No significant difference was observed between all other nutrients.
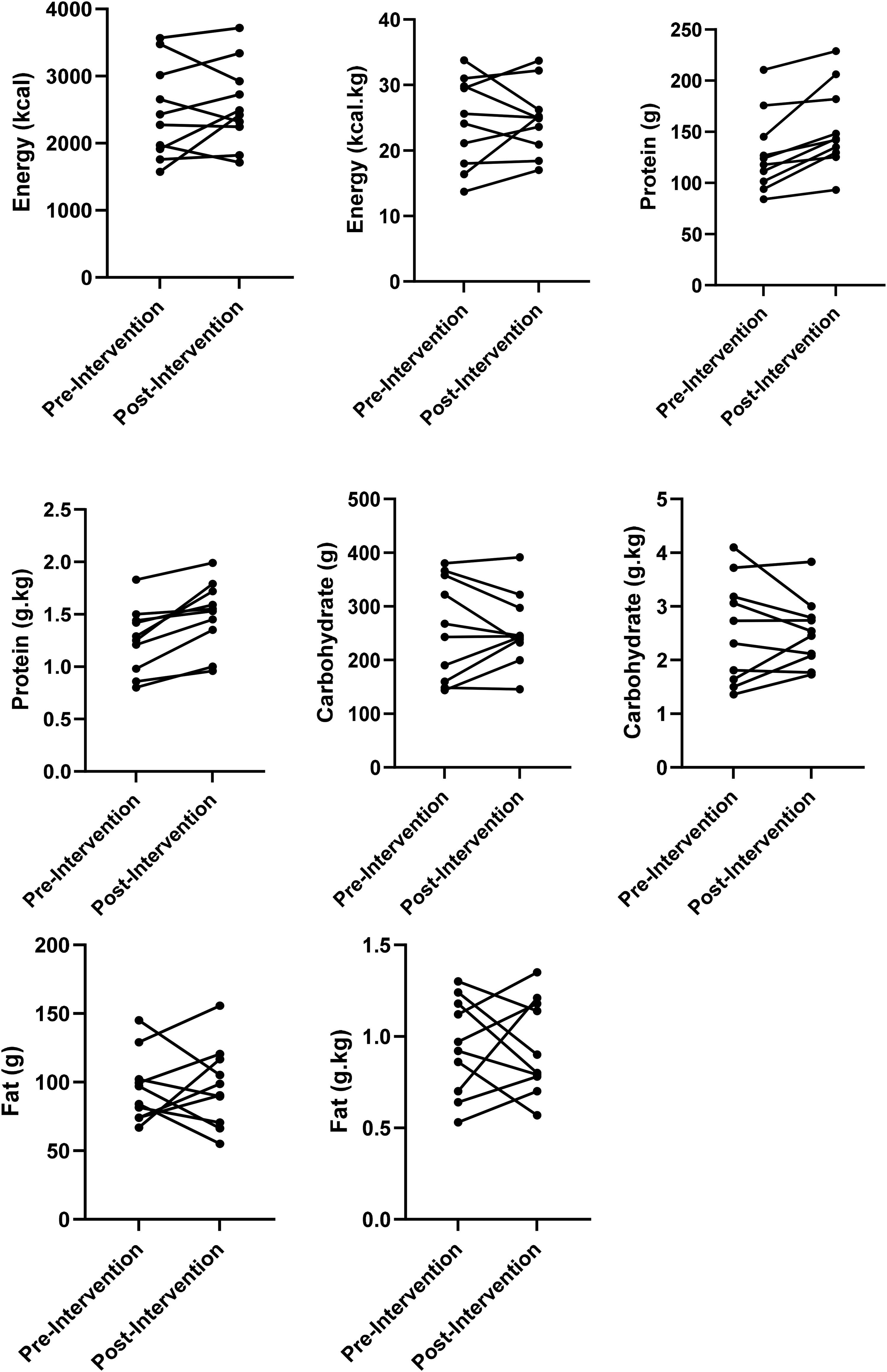
Change in individual total nutrient intake.
Total and relative energy and macronutrient intake.

*Denotes significance ≤ 0.05.
Body composition
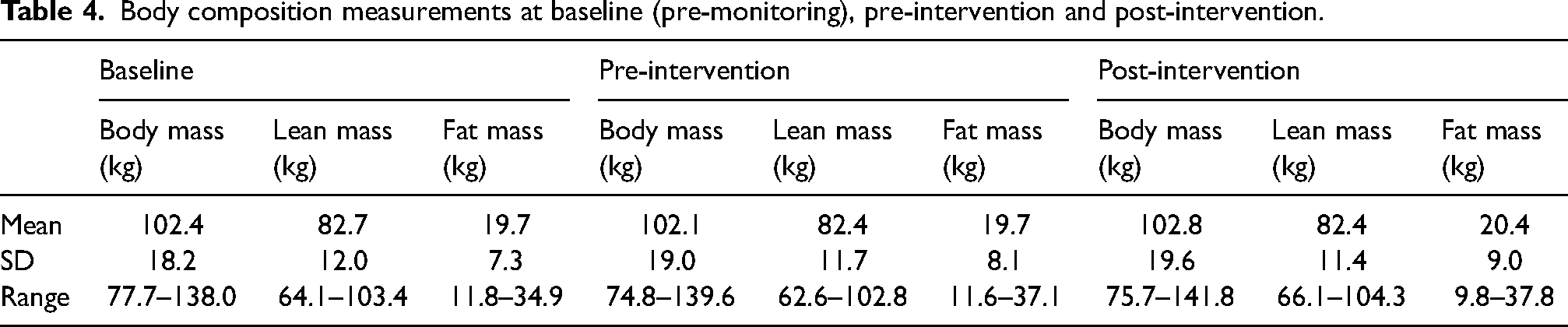
Body composition values are displayed in Table 4. There was no difference between measurements for body mass (p = 0.29), lean mass (p = 0.83) or fat mass (p = 0.38) between baseline, pre-intervention or post-intervention.
Body composition measurements at baseline (pre-monitoring), pre-intervention and post-intervention.
Wellbeing
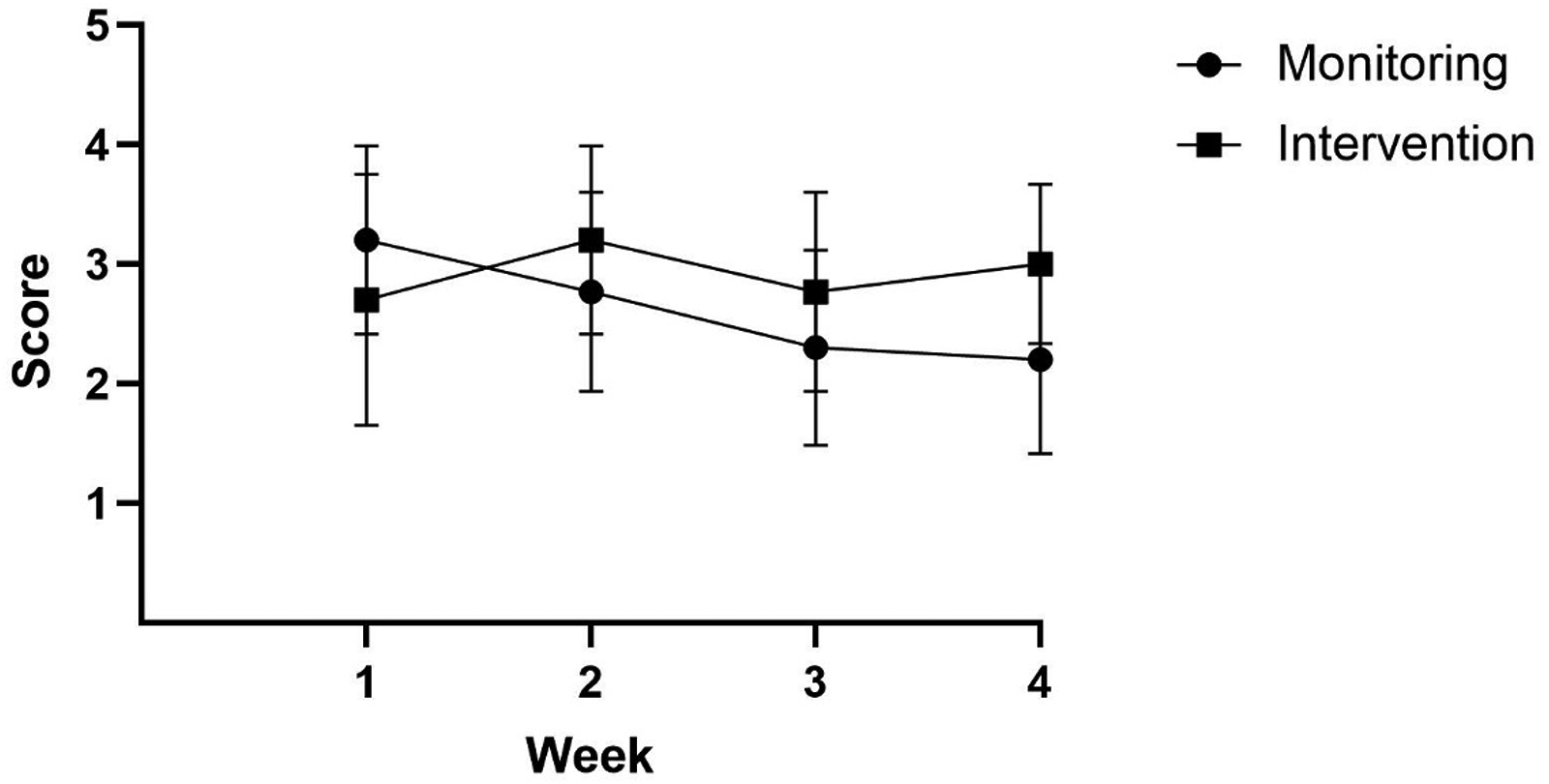
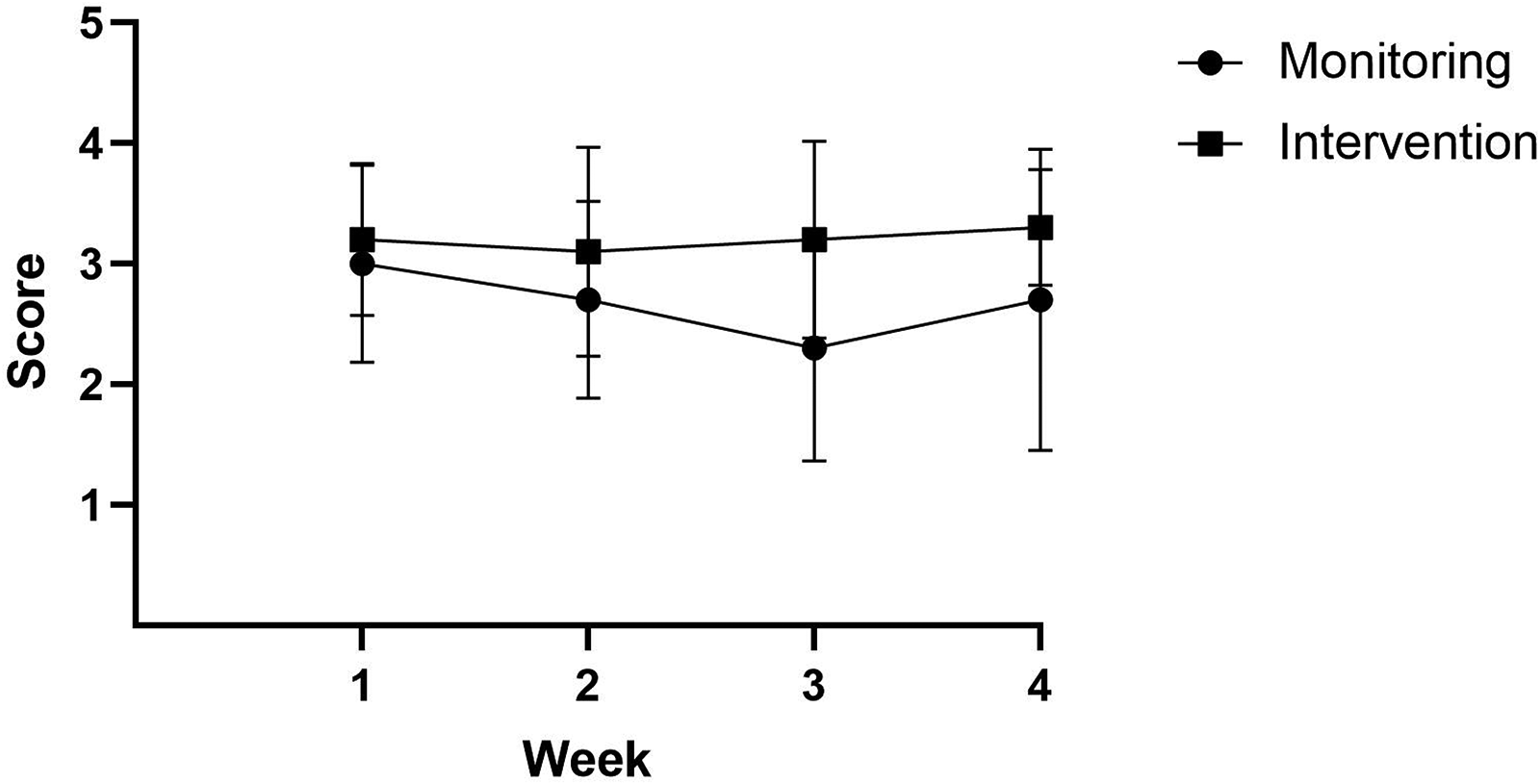
Changes in wellbeing scores across monitoring and intervention weeks are displayed in Figures 2–7. Significant improvements between pre- and post-intervention were observed for sleep quality, stress and mood. A significant increase between pre- and post-intervention was observed for upper body muscle soreness. No differences between time-points were observed for fatigue or lower body muscle soreness.
Subjective change in fatigue during monitoring and intervention periods.
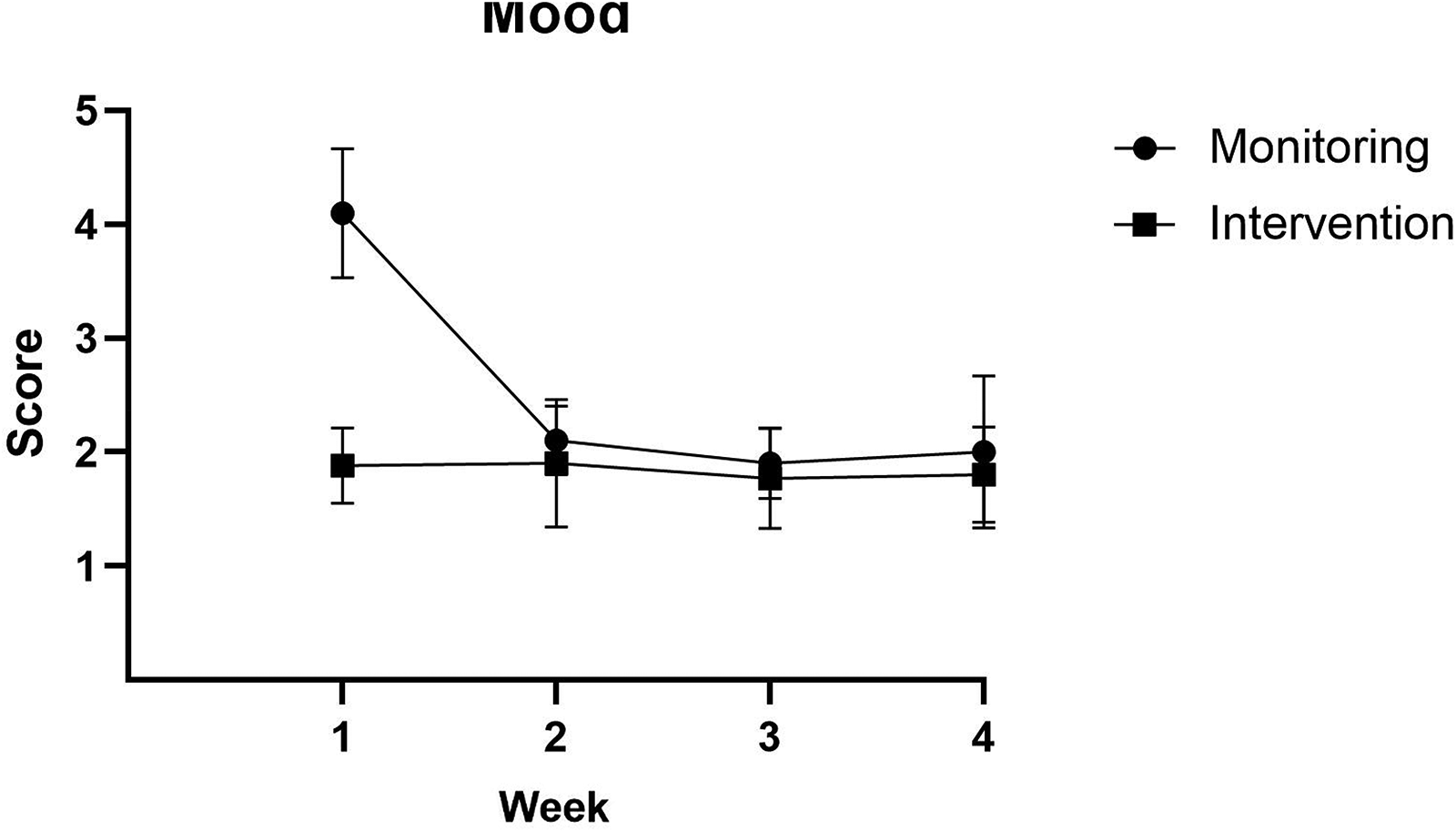
Subjective change in mood during monitoring and intervention periods.
Subjective change in lower body muscle soreness during monitoring and intervention periods.
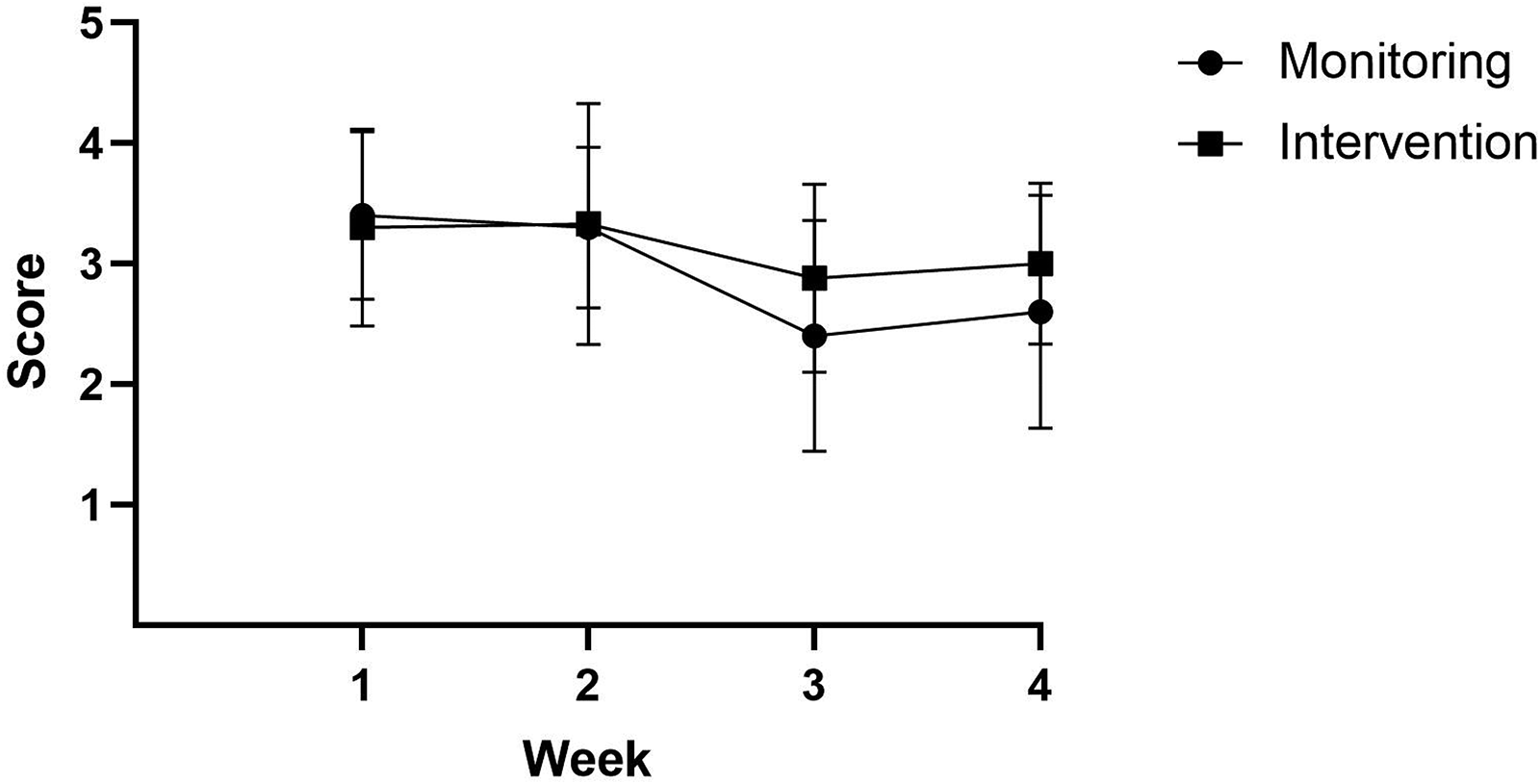
Subjective change in upper body during monitoring and intervention periods.
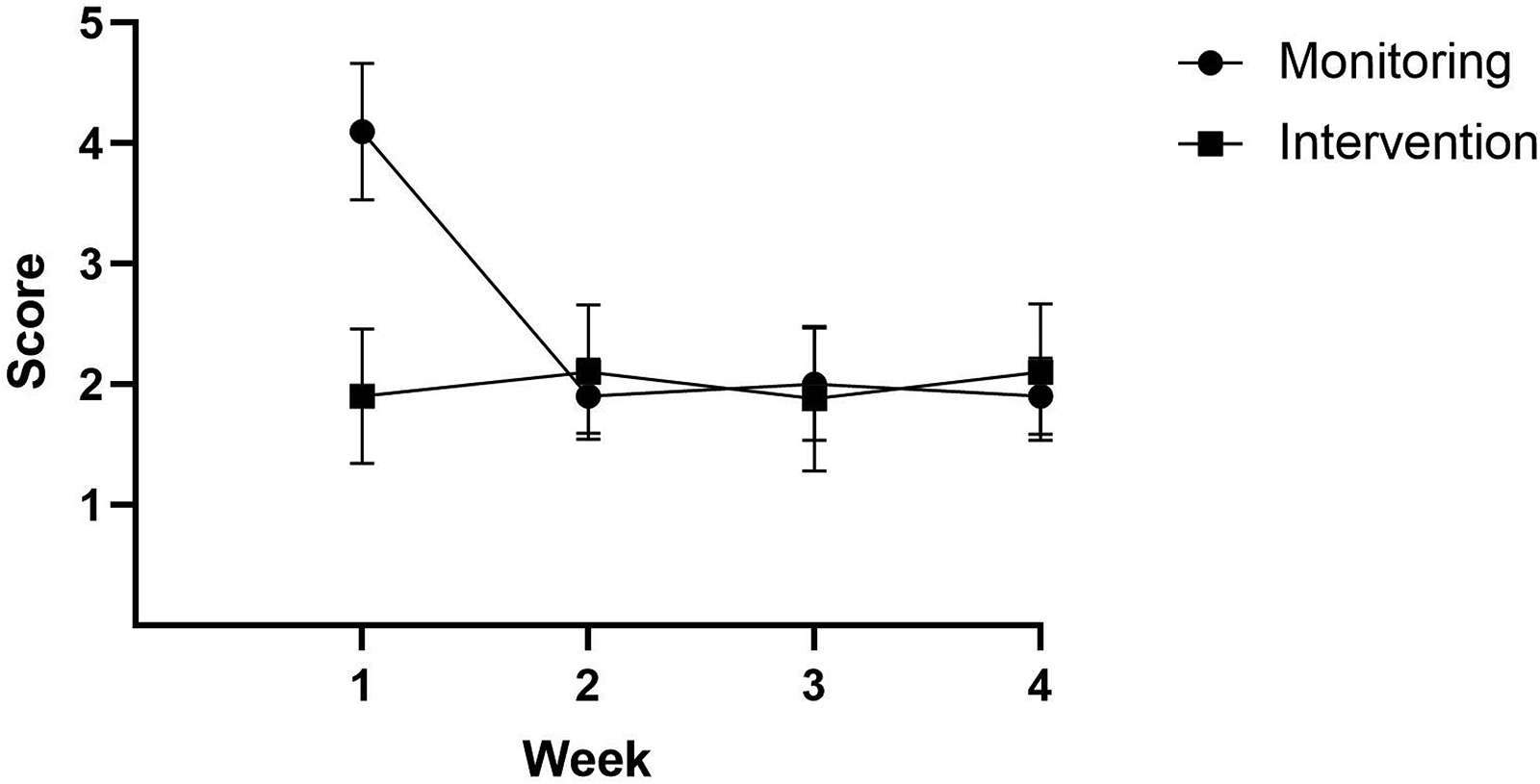
Subjective change in sleep quality during monitoring and intervention periods.
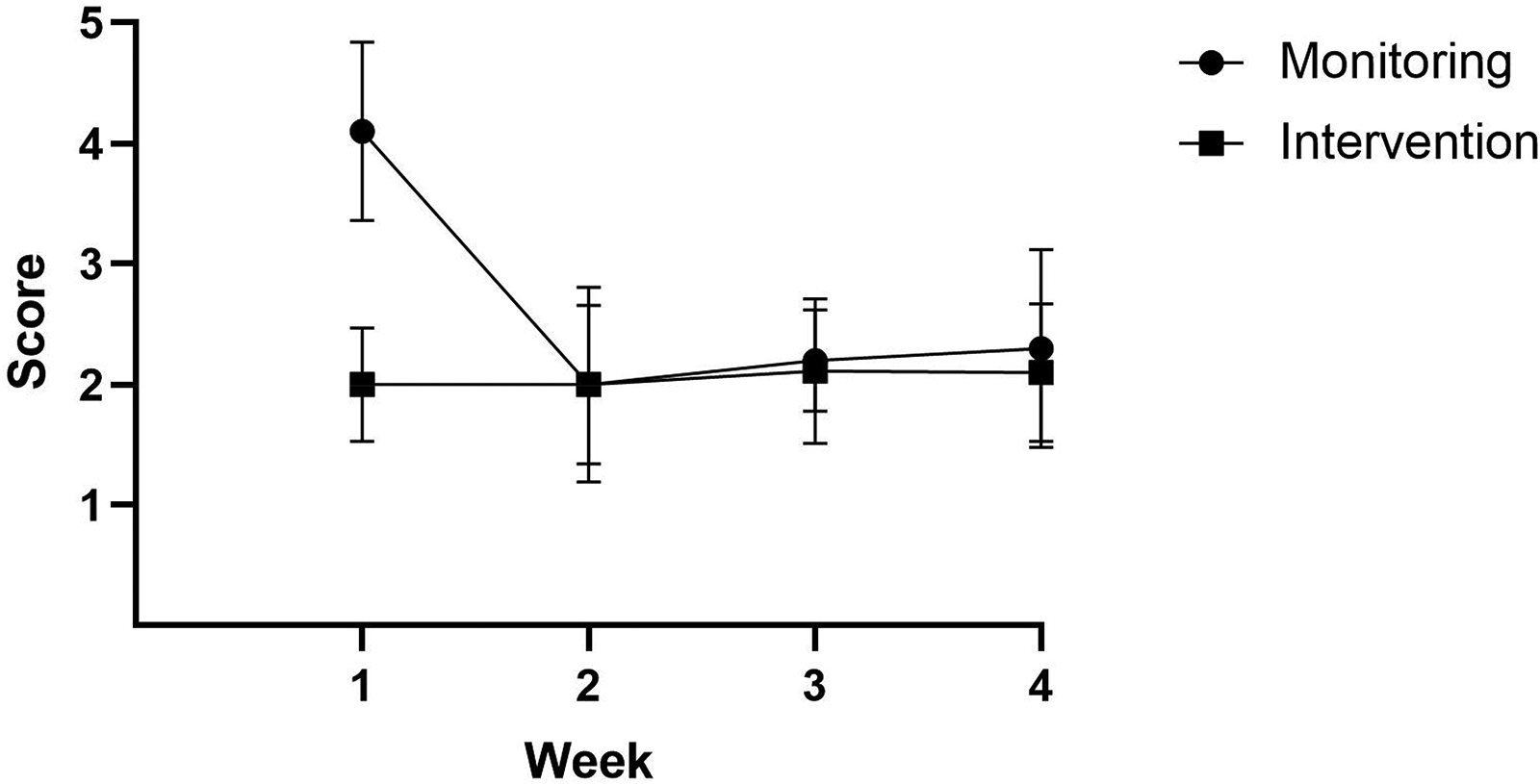
Subjective change in stress during monitoring and intervention periods.
Discussion
The aim of the study was to explore the impact of complete nutrition support on nutrient intake, body composition and subjective well-being in provincial academy rugby union players in New Zealand. Both absolute and relative to body weight energy and protein intake increased following the intervention. Furthermore, significant improvements between pre- and post-intervention were observed for sleep quality, stress and mood. A significant increase between pre- and post-intervention was observed for upper body muscle soreness.
Energy intake
A significant difference was observed in total energy intake and energy intake relative to body mass in response to the nutrition support intervention. Whilst expressed against total body weight as opposed to FFM, energy intakes likely do not meet the threshold required to suggest energy sufficiency in exercising males (40 kcal·kg·FFM·day). 36 Furthermore, the energy intakes observed in the present study overall (pre: 2492 ± 762 kcal, post: 2614 ± 625 kcal) and a relative level (pre: 24.4 ± 7.5 kcal·kg, post: 25.5 ± 6.0 kcal·kg) lower than values reported in English U19 elite rugby academy players (3412 ± 670 kcal, 38.2 ± 9.8 kcal·kg). 25 Additionally, large variability in individual energy intake was apparent but not unexpected due to the variability in total and lean body mass, of which influences individual energy requirements. 37
Previous research has demonstrated that rugby players expend considerable energy daily. Using doubly-labelled water, 5 observed daily energy expenditures of 4010 ± 744 (U16), 4414 ± 1523 (U20) and 4761 ± 1523 (U24). Due to three different age cohorts being represented considerable variability existed in both the number of heavy and light training days and matches during the period athletes were monitored. Due to the observed energy intake being lower than both intakes and expenditures seen previously5,25 it is possible the current athletes were not meeting energy requirements. Low energy availability can impair athletic performance in the form of a decreased neuromuscular function, impaired cognitive function, endocrine dysregulation and increased irritability38,39; male athletes are particularly susceptible to decreased testosterone levels and sub-optimal bone mineral density, 36 which can negatively influence performance and recovery, injury risk and health. Despite lower energy intakes than those previously reported body mass remained stable indicating athletes maintained energy balance throughout the duration of the study. Numerous reasons may account for this.
First, the collection and interpretation of dietary intake data is questionable; whilst the RFPM has been demonstrated as valid in rugby populations 33 inter-practitioner variability in the interpretation of photographs and descriptions provided may influence the results. 40 Furthermore, athletes may intentionally or unintentionally mis-report dietary intake 41 which may further confound both the assessment of energy intake and subsequently body composition.
Second, the schedule of the present athletes may present multiple differing challenges to meeting energy requirements. Time, convenience, and knowledge are described as components of the food choice process 42 and an athlete with multiple obligations may favour convenience over appropriate food choices for health and performance. 27 Intense exercise may delay feeding, 43 a response which may be of particular importance for the present population as balancing multiple obligations may leave inadequate time to appropriately consume food.
Third, alcohol ingestion may be problematic in rugby players, with a high prevalence of weekly binge-drinking sessions (defined as ≥ 5 drinks per session)44,45 and 22% of a 595 professional cohort reporting adverse alcohol intake. 46 Irrespective of excessive intake, consumption of alcohol is not typically compensated for with a reduction in energy intake and may result in a greater food energy intake than non-consumption. 47 During the study, no players reported consuming alcohol however data collection did not occur on Fridays or Saturdays when drinking is most likely to occur due to a lack of responsibility over the weekend 48 or following matches 49 As such, eating and drinking habits on non-observation days may have resulted in a meeting of weekly energy requirements.
Fourth, athletes are often required to alter their body composition to optimise performance via lean mass gain, adipose tissue reduction or a combination of both. 22 If athletes had been undergoing a weight loss regimen, adaptive thermogenesis may cause a reduction in total energy expenditure such that is lower than would be expected. 50
Fifth, body image concerns and disordered eating may be significant factor in athletes not meeting energy requirements. 27 Disordered eating can present in behaviours such as skipping meals and restricting eating 51 which can negatively influence overall energy and nutrient intake. Disordered eating can develop in response to various sociological factors such as culture, education, family, team-mates and coaching staff and can play a role in the development of LEA and its adverse physiological and psychological outcomes. 36
Current data regarding the prevalence of disordered eating in male athletes is mixed. 52 Nonetheless, 53 reported that 30% of Super Rugby players who completed an Eating Behaviour Questionnaire were classified as ‘medium risk’ for developing an eating disorder. Despite the limited data in rugby union athletes, it is prudent for practitioners and coaching staff to be aware of risk factors of disordered eating and monitor the athletes in their care accordingly.
Macronutrient intake
Total protein intake significantly increased following the nutrition education protocol. Despite the increase, post-intervention (153.8 ± 37.1 g, 1.5 ± 0.3 g·kg) absolute and relative protein intake in the present study was lower than in the previous work in male academy rugby union players (210.7 ± 46.7 g, 2.3 ± 0.5 g·kg). 25 A possible reason for this was the incorporation of BCT's in the intervention, specifically adding objects to the environment in the form of providing supplemental protein to each participant. Ingesting adequate protein has long been recognised as a crucial consideration of dietary intake for athletes, with those engaging in team sports requiring substrates for training-induced protein re-modelling resulting in adaptations and to replace oxidised amino acids during prolonged exercise bouts. 15
Despite the average protein intake meeting requirements, large variability between individuals was apparent. During the monitoring period, two participants did not meet the 1.2 g·kg minimum threshold set by the International Society for Sports Nutrition and American College of Sports Medicine18,19 and only three exceeded 1.6 g·kg·d, with greater protein intakes recommended for individuals when energy availability is low.19,54 These findings highlight the importance of both working with athletes individually to ensure protein requirements are met and the reporting of individual values in future studies.
Carbohydrate intake during both the monitoring and intervention periods did not meet the best-practice recommendations of 6–10 g·kg·d.13,55 Consumption of carbohydrates in the present study was greater than those reported in professional Australian Football players 56 however lower than professional20,21,23,24 and academy rugby union players. 25
Inadequate carbohydrate intake may impair a rugby athletes’ ability to perform optimally due to the repeated bouts of anaerobic movement patterns, 10 with 12 demonstrating a significant reduction in vastus lateralis muscle glycogen content following a rugby league match. The authors note that pre-match glycogen levels were not different when 3 g·kg·d carbohydrate were consumed in the 36-h lead into the match compared to 6 g·kg·d; despite reliance on endogenous carbohydrates during match-play, this may indicate that requirements may not be as high as those values reported in best-practice sports nutrition recommendations.13,19
Observation of the individual data indicates that some participants experienced a decrease in carbohydrate intake post-intervention. An improvement in food choices may facilitate a reduction in carbohydrate intake; ultra-processed foods may appeal to the rugby academy athlete due to the cost and convenience of such items however they are typically high in calories, sugar and fat. 57 Whilst this may appear sub-optimal, ensuring athletes consume a nutrient sufficient diet along with meeting macronutrient requirements is essential for promoting good health and wellbeing 58 and maintaining function of metabolic pathways in which micronutrients are required. 19
Wellbeing
Participation in competitive rugby union can support and facilitate a range of positive wellbeing outcomes; individuals from an experienced amateur US cohort reported that involvement in rugby created their identity and benefited making friends, improving mental growth and psychological fulfilment. 59 Despite this, young male rugby union athletes reported greater stress on training days. 60 Such stressors relate to diet (e.g. weight and general weakness), sleep (e.g. getting enough sleep) and health (e.g. muscle pain and unexplained aches). 60 This may have particular relevance to the present population, who engaged in six weekly training sessions across four days during the study period however such perceptions were not supported in the present cohort, with significant improvements observed following the intervention for subjective feelings of stress, mood and sleep quality.
Upper body muscle soreness increased from pre to post intervention. Whilst perceptual, this has important implications for rugby players engaging in congested training and play schedules. Muscle soreness may persist for four days following match-play 61 and significant correlations between the number of contacts endured during a match, muscle soreness in forwards (r = 0.62) and fatigue in both forwards and backs (r = 0.44) were observed in rugby league players. 62 Cumulative consecutive day training has previously demonstrated a negative effect on neuromuscular function and perceived muscle soreness in elite rugby players. 63 In contrast to the present study, the authors only observed adverse perceived muscle soreness in the lower body.
Practical challenges and limitations
Practically, data collection during the short period available was difficult for numerous reasons. First, significant changes to nutrient intake are unlikely to occur in such a short timeframe. 64 Modelled the time to automatic performance of a healthy habit in participants by asking for repetition of the habit, logging whether the habit was completed daily over 84 days and completing a self-report habit index 65 to calculate automaticity of said habit. The authors suggest habit formation takes an average of 66 days, with significant variability between participants (18 – 254 days). The eating habits promoted by the researchers were simple tasks (eating a piece of fruit at lunch); complex tasks such as meeting best practice sports nutrition recommendations for multiple nutrients and meals when faced with previously mentioned barriers to resources for optimal food choices may take longer to promote and enforce. Second, two participants were away for a one-week period for recreational purposes. Third, nine participants were not always available due to travel or overseas game commitments.
Baseline and pre-intervention body composition analysis was conducted during early morning training sessions, whereas post-intervention analysis was conducted at mid-day. This was due to a change in the participants training schedules which made early morning data collection unattainable and thus complete standardisation before tests was not practically feasible. Factors such as hydration status 66 and intestinal faecal mass 67 can influence the body composition values obtained both within and between-day 66 which likely influenced the results obtained post-intervention. As such, the values presented from the present study should be interpreted with caution.
The analysis of dietary intake is prone to error and therefore the results must be represented and interpreted with caution. To reduce the likelihood of random error we aimed to measure dietary intake on 12 days during both the monitoring and intervention blocks 68 ; extended periods of dietary analysis can reduce the magnitude of inter-practitioner variance. 40 Furthermore, analysis over an extended period may represent more habitual patterns than observation across a single week. However, all participants failed to fully record dietary intake across all possible eating occasions and days.
Anecdotal observations indicate that better food choices were made by many participants. As diet quality was not a measured variable in the present study, these possible changes are not quantified. Improved diet quality may produce unfavourable effects in that participants are unable to meet energy and carbohydrate requirements due to the additional food volume causing gastric distention 69 and thus inducing satiety before energy requirements can be met; nonetheless, the long-term benefits of athletes making better food choices are likely to facilitate enhanced health, well-being and performance.19,58
The use of BCTs to inform the intervention allowed for a systematic approach to an intervention that would prove difficult to control. As evidenced by the increase in protein intake, the ‘introduction of objects to the environment’ in the form of dietary protein likely influenced the increase in protein intake. Additionally, ‘prompts/cues’ may have assisted as the presence of a full-time practitioner would enforce the importance of nutrition for health, wellbeing, performance and recovery. Collectively, the majority of BCTs implemented in the present study likely influenced the participants positively; however, this cannot be confirmed without qualitative data in response to similar interventions.
Novelty
To the authors’ knowledge, this study was the first to report energy and macronutrient intake, body composition and well-being in provincial academy rugby players in New Zealand. Additionally, we demonstrate the application of a nutrition support intervention informed by behaviour change techniques and how this influenced energy and macronutrient intake. The application of a structured nutrition support protocol over a longer duration in athletes not currently receiving such support may be beneficial to enhance nutrient intake and thus performance, recovery and well-being.
This manuscript highlights the volatile and unpredictable nature of working in performance sporting environments, which may be further exaggerated when individuals play for multiple teams but must be in education, support themselves and/or family members financially and maintain social commitments. Whilst participants were provided with a valid 33 and preferred 34 way of providing dietary intake information, engaging participants over a prolonged period proved challenging. Furthermore, overseas game commitments meant retaining contact and receiving information from participants was not always feasible.
Future research should seek to incorporate a mixed-methods approach to analysing nutrient intake and the role of sports nutrition practitioners working with professional and semi-professional teams. Whilst the analysis of nutrient intake, body composition and subjective well-being has provided insight into how well-received the short-duration nutrition support protocol was, anecdotal conversations with the athletes during this time provided additional information from their perspective. Additionally, research observing changes in both dietary intake and diet quality in response to nutrition education in athletes would be beneficial to identify strategies which may be best applied in a practical setting. Whilst the current data may not demonstrate a large outcome, qualitative data and diet quality analysis would enhance our understanding of the protocols and formulate the ‘bigger picture’.
Considerations for the practitioner
Athletes at the developmental level are typically required to navigate multiple commitments. Attending academy training sessions and games, club training and games and work and/or education may result in the athlete struggling to meet nutritional requirements. Additionally, personal considerations such as maintaining relationships with family, friends and partners should be factored. The practitioner and/or support staff should be aware of this on an individual level and put into place strategies to best support the athlete both physiologically and psychologically.
Rugby codes contain different positions with a variety of on-pitch, training and body composition demands. 70 Ensuring athletes receive tailored nutrition support is paramount to meeting energy and nutrient requirements. At the beginning of the present study, participants’ body mass ranged from 78 to 140 kg thus not only are individual requirements important to highlight but various strategies to implement these may be necessary due to the large variation in absolute food volume required.
Athletes may live with parents, guardians, family members or friends who either contribute to or are solely responsible for the purchasing and/or preparation of food and meals. Strategies should be implemented by support staff and practitioners to include those involved in providing nutrition to athletes to assist with optimising these practices away from facilities. Such strategies may include guiding grocery shopping, cooking classes and tailoring portions to the individual athlete.
Athletes may not possess the required level of nutrition knowledge to execute optimal nutrition practices. Ensuring that athletes, and others in their lives such as family and friends who may influence nutrition habits, receive regular education sessions and materials may allow for the promotion of appropriate food choices.
In New Zealand, rugby athletes engaging with a provincial academy would also concurrently train and play for a local club. This presents challenges in that nutrition advice may not be standardised, with club coaches possibly providing information that contradicts what the athlete needs. 71 Additionally, multiple training obligations may result in difficulties with monitoring training load to promote adaptations and reduce injury risk.
The culmination of factors mentioned may have resulted in the large intra-individual variability in nutrient intake and body composition in the present study. Ensuring that practitioners work with athletes as individuals and provide support and resources to their understanding will likely result in greater engagement.
Practitioners should seek to implement strategies to improve dietary habits and ensure regular monitoring and contact in ways that work for the individual person. Such practices are unfeasible when practitioners are provided little hours and as such, appropriate investment is made into nutrition services to allow for the optimal health, well-being, development and performance of athletes in their care.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.