
Abstract
Objectives
The primary objective of this scoping review was to examine existing evidence regarding the dietary intake and nutrition habits of elite and highly trained junior and young adult tennis players.
Methods
Systematic searches of MEDLINE, EBSCOHost and Scopus were undertaken from the earliest record to December 2021. Reference lists of articles selected were manually searched. A five-stage protocol informed by Arkey and O’Malley's framework with consideration for the Joanna Briggs Institute (JBI) methodology from scoping reviews was followed.
Results
The initial searches yielded an initial 145 records following the removal of duplicates. Following the screening process 14 articles were accepted for analyses. Three major themes were identified: (1) dietary intake and negative energy balance, (2) sub-optimal nutrient intake/habits, and (3) the use and impact of dietary supplements/ergogenic aids.
Conclusion
Research indicates sub-optimal nutritional practices amongst elite and highly trained junior and young adult tennis players. Particular concerns have emerged regarding insufficient calorie consumption to support performance, growth, and wellbeing.
Introduction
Tennis is an intermittent sport characterised by explosive high intensity efforts interspersed with short rest intervals over sustained periods. An average point in tennis typically lasts <10 s, with matches commonly between 1.5–3 h in duration, known on occasion to exceed 4 h.1,2 The intermittent bouts of high intensity predominantly utilise anaerobic metabolism, whilst the lower intensity efforts and set rest periods allow the aerobic system to aid in recovery. 3 Promising young tennis players are exposed to high training and competition loads, commonly training in excess of 15 h a week, 4 competing in more than 15 tournaments a year, 5 spanning approximately 8 months in duration. 6 It is important that players are physically robust enough to sustain such demands to optimise adaptation and minimise injury risk. 7
The importance of nutrition and its direct influence on optimising energy stores, 8 reducing fatigue, 9 recovery from injury, 10 and health status 11 is widely acknowledged. Nutrition is considered a key factor in overall athlete development, 8 essential for success in sport at any age. 4 Amongst young athletes, nutrition is particularly critical, not only to provide the increased needs for training, but also the needs generated by the growth spurt associated with puberty. 12 Supporting elite and highly trained young tennis players with appropriate nutrition is vital, in order to avoid the deleterious effects associated with insufficient nutrient and energy intake (EI). These include, but are not limited to impairments in metabolic rate, menstrual function, bone health, protein synthesis and immunity. 13 Furthermore, adolescence is an important time in establishing a lifelong relationship with food; to develop a positive connection between diet, exercise, and body image, 14 whilst minimising the risk of developing disordered eating (DE) tendencies and susceptibility to eating disorders. 15
Whilst literature exists assessing dietary intake in highly trained young athletes in other sports, 16 research is in its infancy, and very little has been conducted exploring nutrition and junior and young adult tennis players. To date, no attempt has been made to systematically review nutrition in elite and highly trained junior and young adult tennis players. Scoping reviews address published evidence over a broad topic by summarising, mapping and categorising key concepts that underpin the research area using a systematic protocol.17,18 They are appropriate for understudied areas, making a scoping study relevant for this review. The identification and investigation of nutritional habits and practices in this population, including nutritional periodisation and supplementation use, will offer important insights to inform practice and future research.
Objective
The primary objective of this scoping review is to examine existing evidence regarding the dietary intake and nutrition habits in elite and highly trained junior and young adult tennis players. Additional objectives include: (1) conducting a systematic search of published literature, (2) mapping the characteristics of the research, (3) providing a brief summary of the research themes, and (4) identifying research opportunities and gaps in current research.
Methods
Protocol design
The protocol of this scoping review followed five stages informed by Arkey and O’Malley's framework, 17 with consideration for the Joanna Briggs Institute (JBI) population, concept, context methodology for scoping reviews. 19 These stages consisted of (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, (5) collating, summarising, and reporting the results.
Stage 1: identifying the research question
Through consultation with the research team, the key objective of this systematic scoping review was to identify what is known from existing literature about nutritional intake in elite and highly trained junior and young adult tennis players. The scope of sports nutrition in junior and young adult tennis is broad, an area that has not been reviewed to date. The key objective was guided by the following research questions:
How are players fuelling to support performance, growth, and maturation? What nutritional habits are evident amongst junior and young adult tennis players? What is known regarding the impact of supplementation/ergogenic aids on tennis performance in this population?
Stage 2: identifying relevant studies
Information sources
The following databases were searched in December 2021 to identify relevant literature: MEDLINE (Ovid; 1950 – present), EBSCOHost (1892 – present) and Scopus (1960 – present). The reference lists of articles selected for full text review were hand-searched to identify any additional literature. Studies published in a foreign language were translated and included in the review.
Search strategy
The search strategy was developed and piloted in MEDLINE (Ovid) and agreed by the research team (see Supplementary Material). The following keywords were used: ‘Tennis’ OR ‘Racket Sport’ OR ‘Racquet Sport’ AND ‘Nutrition’ OR ‘Nutritional Status’ OR ‘Nutritional Intake’ OR ‘Intake’ OR ‘Ingestion’ OR ‘Nutrition Habits’ OR ‘Diet’ OR ‘Dietary Intake’ OR ‘Dietary Status’ OR ‘Dietary Supplements’ OR ‘Ergogenic Aids’. Filters were applied to retrieve articles in a junior, young adult and elite/highly trained population (see eligibility criteria for definitions). No date restrictions were applied.
Eligibility criteria
Population
The scoping review included junior and young adult tennis players. Players had to be considered ‘highly trained’ or ‘elite’. Highly trained was defined by players training at least 5 h per week, competing regularly in official match play and tournaments, and/or representing their county, region, or province. Elite refers to players competing at national or international level, with Association of Tennis Professionals (ATP), Women's Tennis Association (WTA), International Tennis Federation (ITF) or national rankings. The population was not limited by sex. Age categories were considered with junior players ≤18 years of age, in line with eligibility to enter junior competitions from national and international governing bodies, 20 and young adults between 18 and 21 years of age. 21
Content and context
The scoping review explored studies that considered the nutritional intake and dietary habits of elite and highly trained junior and young adult tennis players. Studies that report habitual dietary intake and intake during training, competition and rest were considered. Studies investigating the manipulation of dietary intake and its effect on tennis performance were also considered. Selection of studies was not limited by geographical location, with the aim of exploring trends in this population.
Stage 3: study selection
The study selection was undertaken in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews) extension for scoping reviews guidelines. 22 The review process consisted of three stages. Firstly, titles and abstracts were screened by the lead author to determine potential eligibility against a broad inclusion criteria. Secondly, the full text of records deemed relevant were retrieved and assessed in detail against the inclusion criteria. Finally, reference lists/bibliographies of the remaining articles were read to identify any eligible studies. If papers were deemed appropriate and published in a foreign language, a translated version was sought.
Stage 4: charting of the data
The key data extracted from the selected articles were authorship (inc. year of publication), participant information, aims/objectives, methods/protocol, and key findings.
Stage 5: collating, summarising, and reporting the results
Results were summarised to present an overview of the evidence. A summary of study characteristics including total number of studies involved, year of publication, study design, and study population is provided. The analysis carried out to describe study characteristics enabled major themes and gaps in the literature to be identified.
Results
Search results
The initial searches yielded 145 records following the removal of duplicates (n = 30). Following the omission of studies that did not comply with the eligibility criteria, ten articles remained. The bibliography/reference lists of the remaining articles were read, leading to the identification of four further studies. Fourteen articles were accepted for the scoping review following the full screening process. The PRISMA flow chart detailing the study identification procedures is included in Figure 1. The lead author (JF) extracted the following information from each article: authors and year of publication, participant information, aims/objectives, methods/protocol, and key findings. These are presented in Tables 1 and 2.
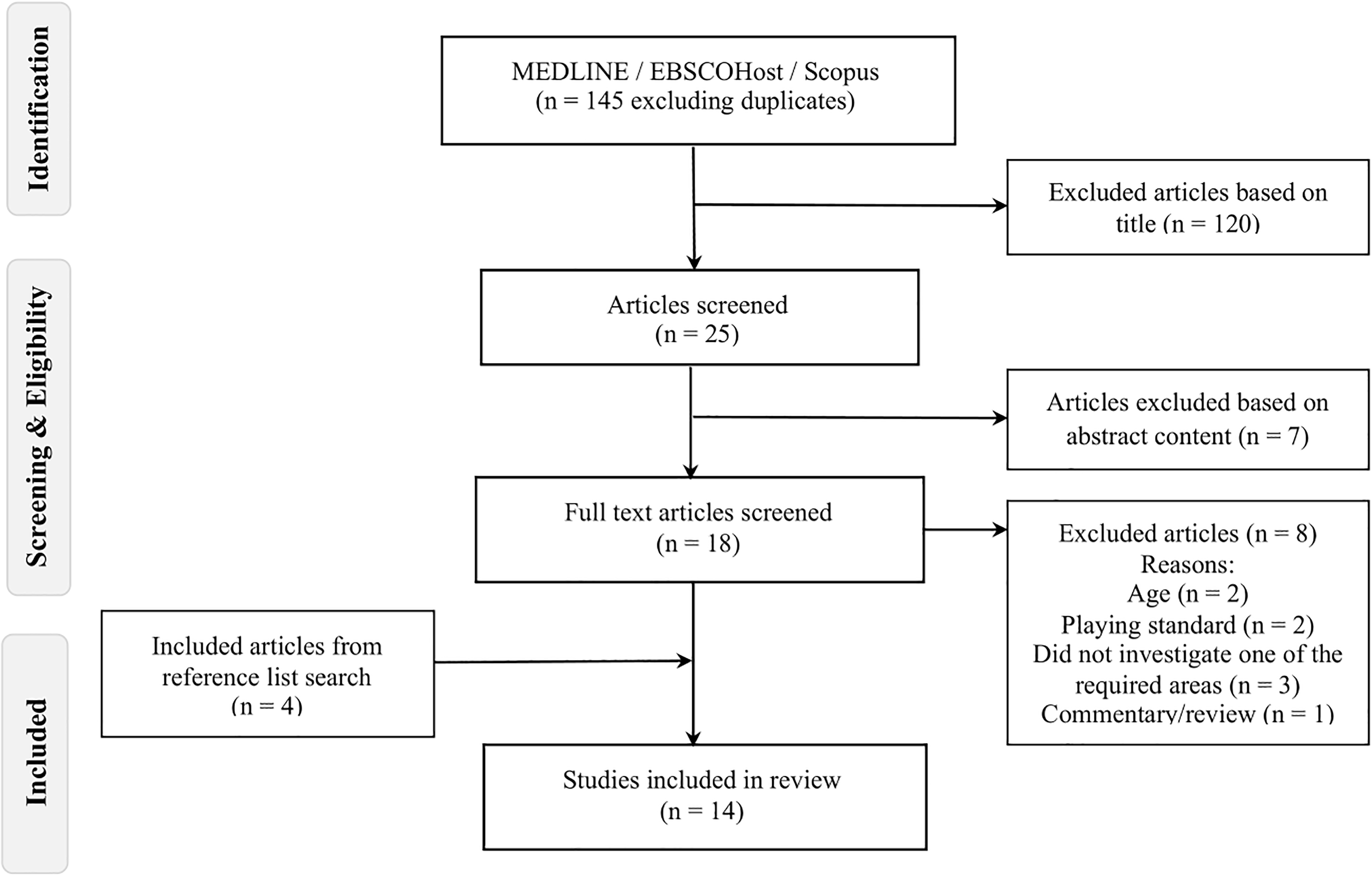
Flowchart of the review process.
Studies investigating the dietary intake of elite and highly trained junior and young adult tennis players.
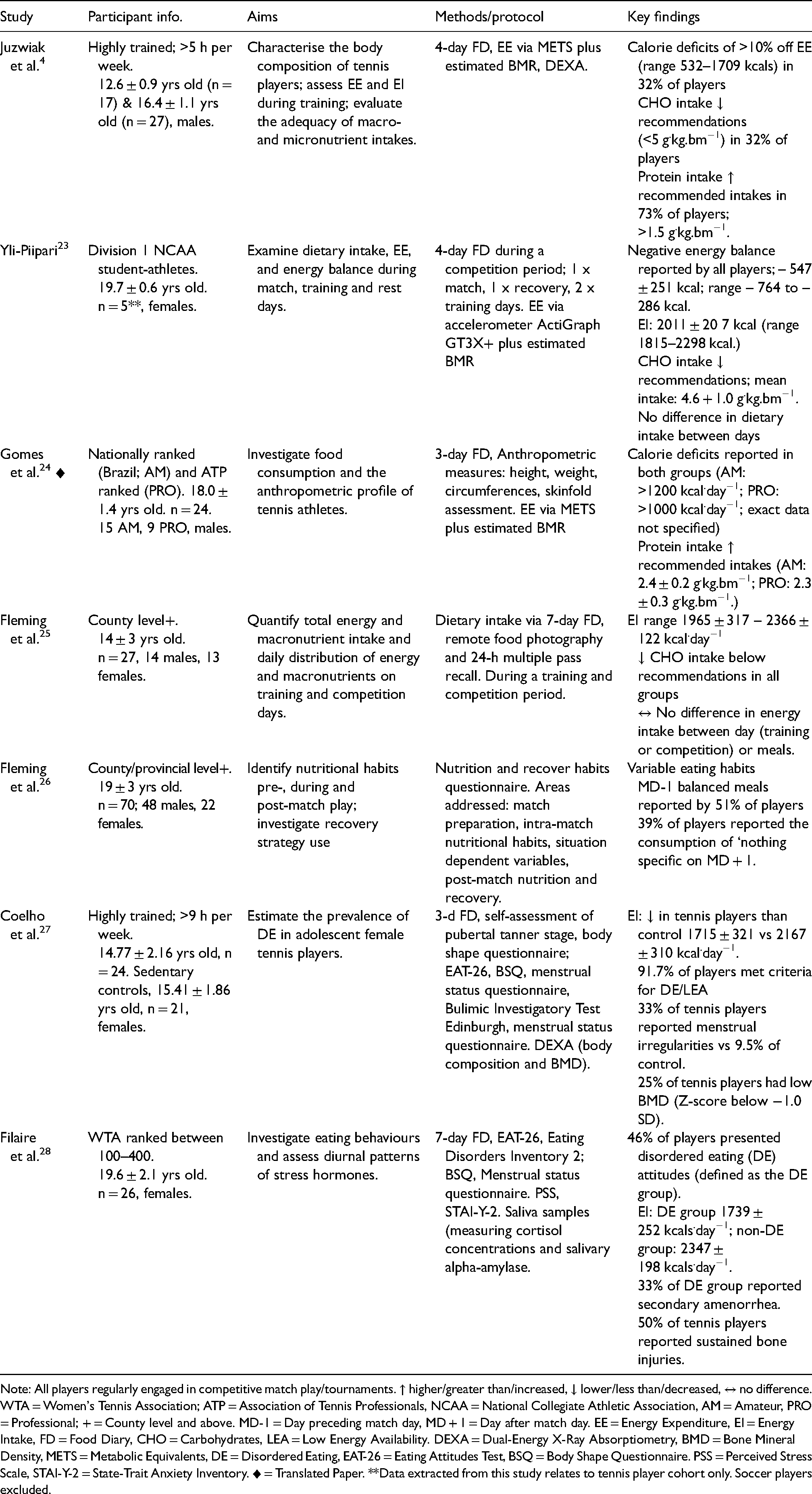
Note: All players regularly engaged in competitive match play/tournaments. ↑ higher/greater than/increased, ↓ lower/less than/decreased, ↔ no difference. WTA = Women's Tennis Association; ATP = Association of Tennis Professionals, NCAA = National Collegiate Athletic Association, AM = Amateur, PRO = Professional; + = County level and above. MD-1 = Day preceding match day, MD + 1 = Day after match day. EE = Energy Expenditure, EI = Energy Intake, FD = Food Diary, CHO = Carbohydrates, LEA = Low Energy Availability. DEXA = Dual-Energy X-Ray Absorptiometry, BMD = Bone Mineral Density, METS = Metabolic Equivalents, DE = Disordered Eating, EAT-26 = Eating Attitudes Test, BSQ = Body Shape Questionnaire. PSS = Perceived Stress Scale, STAI-Y-2 = State-Trait Anxiety Inventory. ♦ = Translated Paper. **Data extracted from this study relates to tennis player cohort only. Soccer players excluded.
Studies investigating the effect of dietary supplements/ergogenic aids on tennis performance.
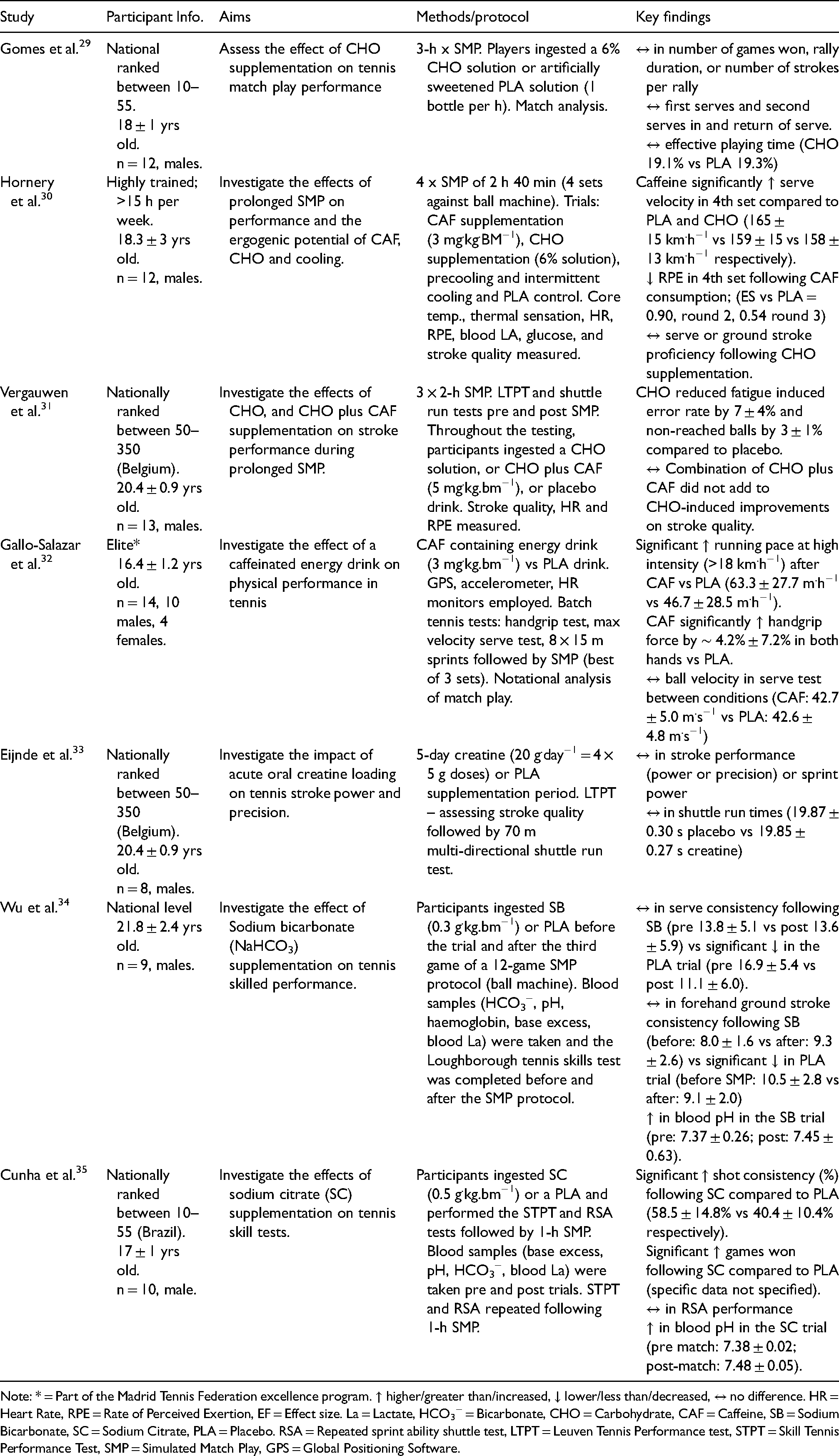
Note: * = Part of the Madrid Tennis Federation excellence program. ↑ higher/greater than/increased, ↓ lower/less than/decreased, ↔ no difference. HR = Heart Rate, RPE = Rate of Perceived Exertion, EF = Effect size. La = Lactate, HCO3− = Bicarbonate, CHO = Carbohydrate, CAF = Caffeine, SB = Sodium Bicarbonate, SC = Sodium Citrate, PLA = Placebo. RSA = Repeated sprint ability shuttle test, LTPT = Leuven Tennis Performance test, STPT = Skill Tennis Performance Test, SMP = Simulated Match Play, GPS = Global Positioning Software.
Study characteristics
A total of 319 tennis players were included in the studies reviewed. Seven of the studies (50%) recruited participants with either an ITF, junior, national, or senior ATP or WTA ranking. One study recruited Division 1 National Collegiate Athletic Association (NCAA) players: the highest level of intercollegiate sporting competition in the United States. 36 The remaining studies recruited participants classified as elite (n = 1; Madrid Tennis Federation excellence programme); competing regularly at county/provincial level or higher (n = 2), and/or training a minimum of 5 h (n = 1), 9 h (n = 1) and 15 h per week (n = 1). Most studies recruited exclusively male players (n = 9); three exclusively female players, and two recruited both male and female players. Mean age for participants was 17.6 ± 1.7 years old. Seven of the studies (50%) investigated dietary intake/dietary habits,4,23–28 and seven (50%) investigated dietary supplements/ergogenic aids.29–35 Most studies assessed dietary intake via self-reported food diaries (n = 6). Either 3-day,24,27 4-day4,23 or 7-day25,28 food diaries were used. One study assessed dietary intake and habits via a questionnaire. 26 One study used multiple methods to assess dietary intake, consisting of a 7-day food diary (FD), 24-h multiple pass recall and food photography. 25 Energy expenditure (EE) was quantified by three studies via accelerometery, predictive equations and metabolic equivalents (METS).4,23,24
Two dietary intake studies also analysed attitudes towards eating and body shape via completion of the Eating Attitudes Test-26 (EAT-26) and body shape questionnaire (BSQ).27,28 Menstrual status and eating disorder/disordered eating prevalence was also assessed in these two studies. Body composition was investigated in three studies, with the use of dual-energy x-ray absorptiometry (DEXA),4,27 and anthropometric measures including body mass, height, skinfold analysis and body circumferences. 24 Bone mineral density (BMD) was also assessed in one study. 27 Of the seven studies that investigated dietary supplement/ergogenic aids and tennis performance, carbohydrates and caffeine were investigated most frequently. Three studies investigated the effect of isotonic carbohydrate solutions (n = 3).29–31 Two of which also included the investigation of caffeine,30,31 and one study investigated the effect of caffeine in isolation. 32 Two studies investigated the effect of extracellular buffers (often referred to as alkalising agents); sodium bicarbonate (NaHO3) 34 and sodium citrate (Na3C3H5O7) 35 respectively. One study also investigated the impact of creatine loading on tennis stroke performance. 33 Four of the studies analysed in this scoping review were published since 201823,25,26,35; four between 2013–201527–29,32; four between 2006–2009,4,24,30,34 one in 2001 33 and one in 1998. 31
Organisation of data
The studies within this review included relevant information relating to nutrition and dietary intake in elite and highly trained junior and young adult tennis players. Three main themes emerged, with some articles containing data related to several themes. First, dietary intake and negative energy balance. Second, sub-optimal nutrient intake/habits to support training and performance, and finally, the use and impact of dietary supplements/ergogenic aids. Themes were classified by the lead researcher, and where ambiguity occurred, constructive debate ensued until a consensus was achieved.
Dietary intake and negative energy balance
Dietary intakes ranged between 1715 ± 321 kcal.day−1 in highly trained competitive junior females 27 to 3212 ± 782 kcal.day−1 in professional ATP ranked young male players. 24 Juzwiak et al. 4 reported intakes of 2635 ± 727 kcal.day−1 and 2967 ± 775 kcal.day−1 in 10–13 and 14–18 year old highly trained male players respectively. Yli-Piipari 23 established five female NCAA Division 1 players to consume 2011 ± 207 kcal.day−1, and Fleming et al. 25 reported intakes consistently below 2250 kcal.day−1 irrespective of age group (ranging from 12–20 year olds). No differences in total daily EI were established between type of day (match vs. training vs. rest).23,25 Fleming et al. 25 also reported no differences between energy or macronutrient distribution at breakfast lunch, dinner or snacks irrespective of type of day (with the exception of increased protein intake at lunch on training days vs. match days).
All three studies that quantified EI and EE reported negative energy balance/energy deficits. Yli-Piipari 23 identified energy deficits of – 546 ± 251 kcal (range – 756 to – 286 kcal) amongst five female NCAA Division 1 tennis players. Similarly, Gomes et al. 24 reported energy deficits >1000 kcal.day−1 (exact data not specified), albeit in a male population. Furthermore, Juzwiak et al. 4 reported energy deficits of >10% in 32% of the participants (male, n = 8), ranging from – 532 to – 1709 kcal. Approximately half of the participants in Coelho et al. 27 and Filaire et al. 28 research reported the consumption of <1800 kcal.day−1, considered the minimum energy necessary to maintain positive energy balance and prevent the disruption of endocrine function. 37 Specifically, 54% (n = 13) of players consumed 1715 ± 321 kcal.day−1, 27 and 46% (n = 12) consumed 1739 ± 252 kcal.day−1. 28 Coelho et al. 27 also reported tennis players to consume significantly fewer calories than the sedentary control group (1739 ± 252 kcal.day−1 vs. 2347 ± 198 kcal.day−1). Low energy availability (LEA) was identified in 87.5% (n = 21) of tennis players in the Coelho et al. 27 paper, defined as energy availability below 45 kcal.kg−1 of fat-free mass per day (kcal.kg− FFM.day−1). Eight players (33.3%) reported intakes <30 kcal.kg− FFM.day−1, considered the threshold at which severe health implications can be observed. 38
Other variables including eating behaviour and attitudes were investigated by two studies amongst highly trained 27 and professional female tennis players. 28 Filaire et al. 28 reported DE attitudes in 46% (n = 12) players. Coelho et al. 27 reported 91.7% (22 of 24) of players met criteria for DE and or/LEA. BMD was analysed by Coelho et al., 27 with 25% of players (n = 6) reporting low BMD (Z-score below −1.0 SD). Similarly, 50% of participants (n = 13) from the Filaire et al. 28 study reported having sustained bone injuries during their tennis career to date. Menstrual dysfunction was also reported in both studies, referring to the development of oligomenorrhea (≤9 menstrual periods in 12 months), primary amenorrhea (first menstrual period >15 years of age), or secondary amenorrhea (cessation of menses for >3 months). 39 Primary and secondary amenorrhea or oligomenorrhea was reported in 33% (n = 8) of players versus 9.5% (n = 2) of the sedentary control group. 27 Secondary amenorrhea was reported by 33% (n = 4) players by Filaire et al. 28 One player also reported menstrual dysfunction (unspecified categorisation).
Sub-optimal nutrient intake/habits
Six studies involving dietary intake directly assessed macronutrient intake.4,23–25,27,28 One study assessed dietary habits pre, during and post-match play. 26 Yli-Piipari 23 reported carbohydrate intakes of 4.6 ± 1.0 g.kg.bm−1 in female NCAA Division 1 players. Similar intakes were also reported by Coelho et al. 27 and Filaire et al. 28 in a young female tennis population. Specifically, Coelho et al. 27 reported intakes of 4.23 ± 1.42 g.kg.bm−1 (tennis player group) and Filaire et al. 28 3.18 ± 0.43 g.kg.bm−1 DE group versus 4.33 ± 0.9 g.kg.bm−1 non-DE group, respectively. Also, carbohydrate intakes of 4.6 ± 1.4 g.kg.bm−1 were reported by Fleming et al., 25 amongst highly trained male and female junior tennis players, and carbohydrate intakes <5 g.kg.bm−1 were established in 32% of junior male players (n = 14) by Juzwiak et al. 4 In contrast, Gomes et al. 24 reported intakes of 6.3 ± 0.5 g.kg.bm−1 and 6.5 ± 0.7 g.kg.bm−1 between Brazilian nationally ranked and professional ATP ranked players. Although relative intakes were not assessed by Fleming et al., 26 51% of players (n = 36) opted for balanced meals (consisting of carbohydrates, fats and protein and some micronutrient considerations) rather than prioritising carbohydrates as the predominant macronutrient on the day prior to match day (MD-1).
Protein intakes >1.4 g.kg.bm−1 were reported in four studies23–25,27 ranging from 1.43 ± 0.43 g.kg.bm−1 27 – 2.4 ± 0.2 g.kg.bm−1. 24 Protein intakes >1.5 g.kg.bm−1 were reported in 73% (n = 32) of players by Juzwiak et al. 4 Conversely, Filaire et al. 28 reported intakes of 1.15 ± 0.23 g.kg.bm−1 and 1.35 ± 0.36 g.kg.bm−1 between the DE and non-DE groups of professional (WTA ranked) female tennis players. Fat intake contributed towards >30% of total daily EI (TDEI) in two studies (35 ± 4% 25 and 33 ± 3% 27 ). Similarly, Juzwiak et al. 4 reported fat intakes between 32–42% TDEI in 80% of players (n = 35). In contrast, Gomes et al. 24 reported fat intakes of 16 ± 5% and 24 ± 4% TDEI amongst nationally ranked and ATP ranked male tennis players respectively. Two studies reported fat intake in grams relative to body mass (rather than as a % of TDEI), with both reporting intakes between 1.09 ± 0.40 g.kg.bm−1 28 and 1.13 ± 0.33 g.kg.bm−1. 23
Micronutrient intake was investigated by two of the six studies.4,24 Fibre, calcium, potassium, magnesium, and folic acid intakes were below dietary reference intakes (DRI) for 98%, 80%, 100%, 100%, and 98% of the tennis players respectively. 4 Gomes et al. 24 also reported calcium intakes significantly lower than DRIs in both nationally ranked and professional tennis players (778.7 ± 535 mg and 782.6 ± 491.9 mg respectively).
The use and impact of dietary supplements/ergogenic aids
The majority of studies have investigated the effect of carbohydrate and/or caffeine supplementation on tennis performance.29–32 Isotonic drinks were used in all three investigations considering carbohydrate supplementation.29–31 Simulated match play (SMP) was conducted in all three investigations, with trial durations between 2 and 3 h. Food consumption on the day/s preceding the testing interventions were standardised in all investigations yet details of which were only presented in one study. 29 Participants in the Gomes et al. 29 study consumed an isoenergetic diet consisting of 8.33 ± 0.58 g.kg.bm−1 carbohydrate, 2.10 ± 0.14 g.kg.bm−1 protein and 1.58 ± 0.13 g.kg.bm−1 fat. All studies were placebo controlled. Vergauwen et al. 31 also investigated the co-ingestion of carbohydrate plus caffeine (5 mg.kg.bm−1), whilst Hornery et al. 30 also investigated caffeine (3 mg.kg.bm−1) and cooling interventions (ice baths and cooling jackets). Results assessing carbohydrate supplementation on tennis performance varied. Gomes et al. 29 reported no effect of carbohydrates on performance compared to placebo (including games won, rally duration, strokes per rally, effective playing time, aces, double faults, first and second serve %, and return %). This too was evident in Hornery et al. 30 investigations, where carbohydrate had no effect on performance (serve or ground stroke proficiency) compared to placebo. In contrast, carbohydrate ingestion reduced fatigue induced error rate by 7 ± 4% and non-reached balls by 3 ± 1% compared to placebo in the research by Vergauwen et al. 31
Mixed responses to caffeine ingestion were also established. Ingestion methods varied from caffeinated energy drinks 32 to caffeinated tablets.30,31 Dose varied from 3 mg.kg.bm−1 30,32 to 5 mg.kg.bm−1. 31 Hornery et al. 30 reported significant increases in serve velocity in the final set of the match following caffeine consumption compared to placebo and carbohydrate conditions (165 ± 15 km.h−1 vs. 159 ± 15 km.h−1 vs. 158 ± 13 km.h−1 respectively). A trend towards reduced RPE in the 4th set was also established (effect size – 0.54); specific data was not stated. Similarly, Gallo-Salazar et al. 32 reported significant increases in physical performance, including increases in handgrip force (∼ 4.2 ± 7.2%) and running pace at high intensity (63.3 ± 27.7 m.h−1 vs. 46.7 ± 28.5 m.h−1). Additionally, number of sprints during SMP and a higher percentage of points won on service were reported following caffeine consumption compared to placebo (13.2 ± 1.7 vs. 12.1 ± 1.7; P = 0.05; and 56.4 ± 10.0% vs. 49.7% ± 9.8%, P = 0.07 respectively), albeit not statistically significant. In contrast, research by Vergauwen et al. 31 reported no further beneficial effects on stroke performance when caffeine was ingested alongside a carbohydrate beverage than carbohydrate consumption alone.
Positive effects of alkalising agents (sodium bicarbonate and sodium citrate) on tennis skill performance were established in two papers. Cunha et al. 35 reported significantly greater shot consistency during the skill tennis performance test (STPS) following the ingestion of sodium citrate compared to placebo (58.5 ± 14.8% vs. 40.4 ± 10.4%). Similarly, Wu et al. 34 established sodium bicarbonate ingestion to maintain serve and forehand consistency, compared to significant declines in the placebo condition. Both studies reported significant increases in blood pH following the ingestion of sodium bicarbonate and sodium citrate respectively.
One study to date investigated the effect of acute creatine supplementation (4 × 5 g doses over 5 days) on stroke performance. 33 Creatine supplementation did not affect power or precision of serves, baseline strokes or volleys (specific data not specified). No difference was also reported in shuttle run times between placebo and creatine conditions (19.87 ± 0.30 s vs. 19.85 ± 0.27 s respectively).
Discussion
The primary objective of this scoping review is to examine existing evidence regarding the nutritional/dietary intake and nutritional habits in elite and highly trained junior and young adult tennis players. Emerging evidence indicates that elite and highly trained junior and young adult tennis players, irrespective of sex, are failing to consume sufficient calories, with notable incidence of negative energy balance and LEA reported. Furthermore, nutrient intakes below recommendations seem to be prevalent in this population.
Energy deficits ranging from 500–>1500 kcal.day−14,23,24 and intakes <30 kcal.kg− FFM.day−1 27 indicative of LEA were reported. This raises concerns regarding relative energy deficiency in sport (RED-S), a condition caused by LEA and associated with a myriad of impairments and health implications including but not limited to metabolic rate, thermoregulation, growth, bone health, and menstrual function. 13 Additionally, albeit limited to two studies to date, DE (referring to a group of abnormal eating behaviours such as restricted eating, fasting, frequently skipping meals, the use of diet pills, laxatives, binge eating, and purging 39 ) was established as an area of concern in this population.27,28 Further research is required to add to these initial findings whilst establishing strategies to support young tennis players, to avoid the negative consequences of such conditions.
Additionally, sub-optimal nutrient intake is consistently reported. In particular, carbohydrate intakes below guidelines (<6 g.kg.bm−1) 40 were widely reported. Players tend to be overconsuming protein, with intakes >1.4 g.kg.bm−1 in 80% of studies (4/5), arguably at the expense of sufficient carbohydrate. This may be associated with the satieting properties of protein consumption, reducing overall calorie consumption and carbohydrate intake. 41 Failing to consume sufficeint carbohydrates may impair performance, with the maintenance of adequate energy and glycogen availabilty considered key for tennis performance. 42 Further research is required to sustantiate the impact of such dietary intakes on performance, with research to date failing to directly investigate this relationship. Micronutrient intakes below recommended nutritient intakes (RNIs) were also reported, yet limited to only two studies in this review. Notably, calcium intakes were low in both studies,4,24 with fibre, potassium, magnesium and folic acid also below recommendations amongst highly trained junior male players. 4 Although micronutrient intake was not directly reported by Filaire et al. 28 and Coelho et al., 27 the high incidence of bone injury and low BMD reported in these studies are indicative of prolonged deficiency of calcium and vitamin D. 8 As micronutrient deficiences often occur concurrently where insufficeint calorie intake is reported, supporting players to meet energy needs is vital. Promoting and encouraging the consumption of a well-chosen diet focussed on food variety can help athletes meet their micronutrient needs. 8 Ensuring players have adequate fuelling opportunities around their training, competition and school/educational commitments is also recommended.
Current recommendations suggest young athletes should aim to eat throughout the day, every 3–4 h, planning intake around their daily commitments. 40 Timing of consumption is also important, to adequately fuel training and match play, 16 promote glycogen resynthesis, 8 and optimise training adaptations including muscle protein synthesis, growth and maturation. 14 Consideration for day to day variation in EE is also advocated, adjusting EI in accordance with the demands and goals of the day. 40 Research to date largely fails to consider the distribution and timing of dietary intake, limited to two studies.23,25 Initial insights suggest a lack of nutritional planning, with no clear differences in nutritional intake (total caloric intake and macronutrient distribution) established between type of day (rest, training, competition) nor meal (breakfast, lunch, dinner, snacks). This raises concerns regarding nutritional knowledge and the amount of time players spend planning and considering their dietary intake. Dietary education may be beneficial with the goal of establishing the nutritional fundamentals, whilst reinforcing eating for performance and long-term health. 14 Including the parent/guardian in this process is encouraged, with many playing a pivotal role in the dietary provision of young athletes. 43
The efficacy of dietary supplementation in elite and highly trained junior and young adult tennis players is unclear. Limited to seven studies investigating several different supplements (carbohydrate, caffeine, creatine, sodium bicarbonate and sodium citrate), current research fails to come to a consensus regarding its use. Although it is widely accepted that carbohydrate-electrolye drinks can improve sporting performance, 44 no ergogenic effects were reported following its consumption in tennis match play performance by Gomes et al. and Hornery et al. 30 These findings may have been due to methodological flaws associated with pre-testing dietary intakes. Specifically, Gomes et al. 29 prescribed the ingestion of high doses of carbohydrate (>8 g.kg.bm−1) on the day prior to testing, notably higher than habitual intakes reported to date (<5 g.kg.bm−1). It is possible that any potential ergogenic effect associated with the ingestion of endogenous carbohydrate during prolonged intermittent exercise may have been blunted, with the high carbohydrate diet and rest periods between matches providing sufficient time to fill glycogen stores. 29 Research from Vergauwen et al. 31 did however report improvements in fatigue induced error rate following carbohydrate ingestion compared to placebo, indicating the need for further research in this area.
Initial findings indicate that caffiene consumption (∼3 mg.kg.bm−1) may attenuate fatigue, with improvements noted in serve velocity, 30 hand grip force, running pace at high intensity and number of sprints. 32 However, research concerning caffeine supplementation is limited to just three studies to date, with no performance benefits reported by Vergauwen et al. 31 Similarly, research indicates that sodium bicarbonate and sodium citrate may attenuate fatigue, and have a positive impact on tennis skilled performance, with particular emphasis on shot and serve consistency34,35; potentially attributable to induced alkalosis (the increase in and/or maintenance of blood pH) and maintenance of prolonged muscle contractile capabilities. 35
In order to determine the ergogenecity of dietary supplementation in this population, further research is warranted. Yet, before addressing the need for dietary ergogenic aids and searching for the ‘silver bullet’ for performance, research should focus on supporting players to meet the nutritional fundamentals (such as meeting energy balance and RNIs), which will have the greatest impact on health, maturation and performance. 14
Limitations
Potential limitations of this scoping review are the heterogeneity and breadth of studies included. Specifically, methods used to quantify dietary intake largely focussed on self-reported food diaries, inherently associated with under-reporting, 45 with only one study utilising multiple methods (food diaries, dietary recall and food photography), 25 deemed a more robust method of accurately assessing dietary intake. 46 This too was evident in the quantification of EE. Only three studies did so,4,23,24 employing a range of methods including METs, accelerometers, and prediction equations. Tennis protocols used, and outcomes assessed also widely varied, making it difficult to draw direct comparisons.
Conclusions
This scoping review serves to provide a clear overview from literature to date regarding the nutritional intake of elite and highly trained junior and young adult tennis players. The following practical implications were summarised from the key findings:
Elite and highly trained junior and young adult tennis players often fail to consume sufficient calories to support performance, growth and wellbeing, posing concerns regarding LEA and RED-S. Subsequent deficiencies in micronutrient status are evident. Indication of a lack of nutritional planning. Concerns regarding unhealthy relationships with food established/being established in this population.
Additionally, this review identified an over-emphasis on the investigation of dietary supplementation in literature to date, with 50% of studies (7 from 14) focussing on their efficacy. Future research should focus on dietary intake and habits in this population, and its impact on performance, with the objective of developing strategies to support players and those working alongside them. Establishing nutritional guidelines and recommendations specific to the junior tennis player offers another exciting opportunity for future research. Supporting this population of talented athletes is imperative, to enable them to meet their sporting potential, whilst developing healthy lifelong eating behaviours to optimise growth, maturation, and wellbeing.
Supplemental Material
sj-docx-1-spo-10.1177_17479541221087687 - Supplemental material for Nutrition and the elite and highly trained junior and young adult tennis player: A scoping review
Supplemental material, sj-docx-1-spo-10.1177_17479541221087687 for Nutrition and the elite and highly trained junior and young adult tennis player: A scoping review by James Andrew Fleming, Robert Joseph Naughton and Liam David Harper in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-2-spo-10.1177_17479541221087687 - Supplemental material for Nutrition and the elite and highly trained junior and young adult tennis player: A scoping review
Supplemental material, sj-docx-2-spo-10.1177_17479541221087687 for Nutrition and the elite and highly trained junior and young adult tennis player: A scoping review by James Andrew Fleming, Robert Joseph Naughton and Liam David Harper in International Journal of Sports Science & Coaching
Footnotes
Author contributions
JF, RJN and LDH planned the study. JF conducted the systematic search of databases and LDH adjudicated. JF wrote the first draft and all authors reviewed the manuscript at various stages throughout the editing process and approved the final draft for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.