
Abstract
The aim of this study was to examine the relationship between resting morning heart rate variability (HRV) metrics and indirect markers of hydration status in elite male athletes. Twenty-two field hockey players (age 26.8 ± 3.4 yr; height 178.4 ± 6.3 cm; body mass 76.2 ± 7.4 kg) were monitored over 10-d during a pre-Olympic training camp. Measurement of heart rate variability (HRV) during an orthostatic challenge, urine specific gravity (Usg, first morning void) and body mass were captured on seven of the mornings. Individual generalized linear mixed models evaluated the relationships between supine and standing HRV metrics with Usg and day-to-day change in body mass. No meaningful relationships were identified between supine (estimates −0.002 to 0.001) or standing (−0.002 to 0.003) HRV metrics and Usg as well as between supine (−0.003 to 0.016) or standing (−0.004 to 0.006) HRV metrics and changes in body mass. These outcomes indicate that supine and standing HRV metrics are not influenced by indirect indices of hydration status in elite male field hockey players.
Introduction
The use of heart rate variability (HRV) has become increasingly popular in sport and is now a common method to assess autonomic nervous system function of athletes. Fluctuations in resting morning HRV are used to monitor athlete readiness, 1 guide training prescription,2,3 and identify potential over-reaching/training.4,5 However, HRV is influenced by a variety of factors including respiration rate, 6 fitness level, 7 posture 8 and age. 9 Thus, it is important to identify factors that might affect HRV so that efforts can be made to control for them (if necessary and possible) and practitioners can make appropriate interpretations about outcomes. One factor that might influence HRV but has received little attention in athletes is hydration status. 10
Hydration status refers to the balance of total body water (euhydration) or shifts which result in a deficit (hypohydrated) or an excess (hyperhydrated). 11 The most accurate method for measuring fluctuations of body water is deuterated (heavy) water (D2O). However, this method is neither practical or readily available in high-performance sport settings. Therefore field-based approaches that provide an indirect indication of hydration status are favoured. These are often easier to implement and interpret by practitioners working in these environments. Two of the most common indirect markers of hydration status in high-performance sport are changes in body mass and urine specific gravity (Usg). 12 More specifically, the first morning void for Usg and the day-to-day change of morning body mass are valid indices of dynamic hydration monitoring.13–15
A few studies have previously investigated the connection between HRV and field-based indices of hydration status.10,16–19 For example, following an exercise protocol in the heat, participants were permitted (euhydrated – change in body mass –1.6 ± 0.3%) or refrained (hypohydrated – change in body mass –5.1 ± 0.7%) from consuming water. 16 The low frequency (LF) and high frequency (HF) power responses were attenuated in the hypohydrated condition for 45 minutes after exercise. Similarly, college athletes performed an exercise dehydration protocol (change in body mass –3.4 ± 0.4%) followed by rehydration (Usg ∼1.007) or refraining from fluid intake (Usg ∼1.023). 10 Results indicated the root mean square of successive differences (RMSSD) recovered quicker (returned to ∼19% vs. ∼35% of baseline, respectively) when rehydrating during the 4-hour post-exercise period. In another study, RMSSD recovered more quickly during the first hour after exercise when fluid intake matched sweat loss during exercise compared with remaining dehydrated (change in body mass ∼ –2%). 19 Following a military peace patrol (∼6 km over 2.5 hr) the loss in body mass (–2.2 ± 0.5%) correlated (r = 0.53) with changes in the LF:HF power ratio. 17 Additionally, a relationship (r = 0.62) was also observed between the change in RMSSD and percent dehydration (–6.1% plasmas volume) in a group of fighter pilots following a 1-hour test flight. 18 Taken together these studies highlight a link between hydration status and HRV, but they all examined the acute response following exercise/physical exertion. However, in high-performance sport settings HRV is typically measured in the morning and used to evaluate the ‘readiness’ from stressors that occurred on the previous day(s). Thus, there is additional time between the end of training/competition on a given day and the next morning to rehydrate and help facilitate parasympathetic reactivation.
Taken within the context of international field hockey events, where match schedules are congested (i.e., 6–7 matches in 9–10 days), male players tend to have acute reductions in body mass between –1.0 to –2.8% following matches. 20 Yet, indirect indicators highlight that hydration status the next morning is not necessarily fully restored even when fluids are consumed ad libitum. 20 Thus, to expand our understanding about the potential impact of hydration markers on HRV metrics it is important to align the measurements at the same time of the day and make assessments when they would be normally taken during high performance scenarios. It is currently unknown if morning hydration status is associated with morning HRV metrics. Therefore, the purpose of this study was to examine the relationship between morning HRV metrics and indirect indicators of hydration status (i.e., changes in morning-to-morning body mass and morning Usg) in elite male field hockey players during a pre-Olympic training camp.
Materials and methods
Design
This paper is derived from an observational study with a men’s national field hockey team during a training camp (10 days). The study was approved by the University of Toronto Research Ethics Board (protocol reference #30586) and conforms to the Declaration of Helsinki. Informed consent was signed by each participant following a verbal explanation of the protocol.
Participants and procedures
Twenty-two members of a men’s national field hockey team volunteered for this study (age 26.8 ± 3.4 yr; height 178.4 ± 6.3 cm; body mass 76.2 ± 7.4 kg). Players were highly trained, had on-field training volume of 10–15 hours per week and played international-level hockey for at least the previous five years. Details of data collection have been previously published. 21 Briefly, each morning upon waking athletes collected a urine sample, then had body mass measured on a digital scale (Seca 876, Hamburg) and finally performed an orthostatic test to assess HRV. No foods or fluids were consumed between waking and the orthostatic test.
Heart rate variability was measured using a Polar RS800CX™ (Polar Electro, Kempele, Finland) heart rate monitor during a 10-minute orthostatic challenge. 21 The athletes were verbally informed to stand after seven minutes. A metronome set to 1-Hz was placed in the room to help athletes achieve day-to-day consistency with breathing. Visual inspection of R-R peaks and troughs demonstrated consistent breathing rates (∼8 breaths per minute) in all files. Data were transmitted from the chest strap to the watch, then files were downloaded from the watch (ProTrainer, Version 5.40.170), exported (.hrm file) and subsequently analyzed in Kubios (Version 2.2., Kuopio, Finland). 22 An artifact correction (low or medium) was used to remove irregular heartbeats if necessary. No more than 2% of heartbeats in any single file required correction. All HRV metrics were log-transformed: standard deviation of normal to normal intervals (SDNN, ms); square root of the mean squared difference of successive NN intervals (RMSSD, ms); high frequency power (HF; 0.15–0.4 Hz); low frequency power (LF; 0.04–0.15 Hz); the stress score (inverse of SD2 × 1000); and the sympathetic:parasympathetic ratio (stress score:SD1). 23 The stress score:SD1 ratio was first multiplied by 100 to ensure positive values when applying the natural-log transformation. Although LnRMSSD is the most widely used and generally accepted HRV parameters in sports,24,25 previous research has shown postural HRV patterns were independently modified by fatigue and included various time and frequency domain parameters. 26 Therefore, inclusion of more than one HRV parameter in supine and standing positions in the current study was warranted.
The athletes were provided with a urine specimen container and instructed to collect a small urine sample from the first void each morning. 27 Urine specific gravity (Usg) was measured using a handheld digital refractometer (Atago PAL-10S, Bellevue, WA). The refractometer was calibrated before the tests were performed. Hydration status included morning Usg as well as the percent change of body mass between consecutive mornings.
Statistical analysis
The assumption of linearity was met for all variables in all analyses as determined by scatter plots. However, several variables were not normally distributed, therefore individual generalized linear mixed models (GLMM) evaluated the relationships between Usg and each HRV variable. In some instances, Gamma and Inverse Gaussian distributions were closer approximations of the observed distributions and were specified with an identity link function. Relationships between HRV metrics and Usg were entered as fixed effects, and a participant-level random intercept was included to account for the within-subject correlation. In case of non-convergence, the random intercept was removed from the model and subsequently convergence was achieved in each case. Statistical significance was accepted at p < 0.05. All analyses were completed using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA).
Results
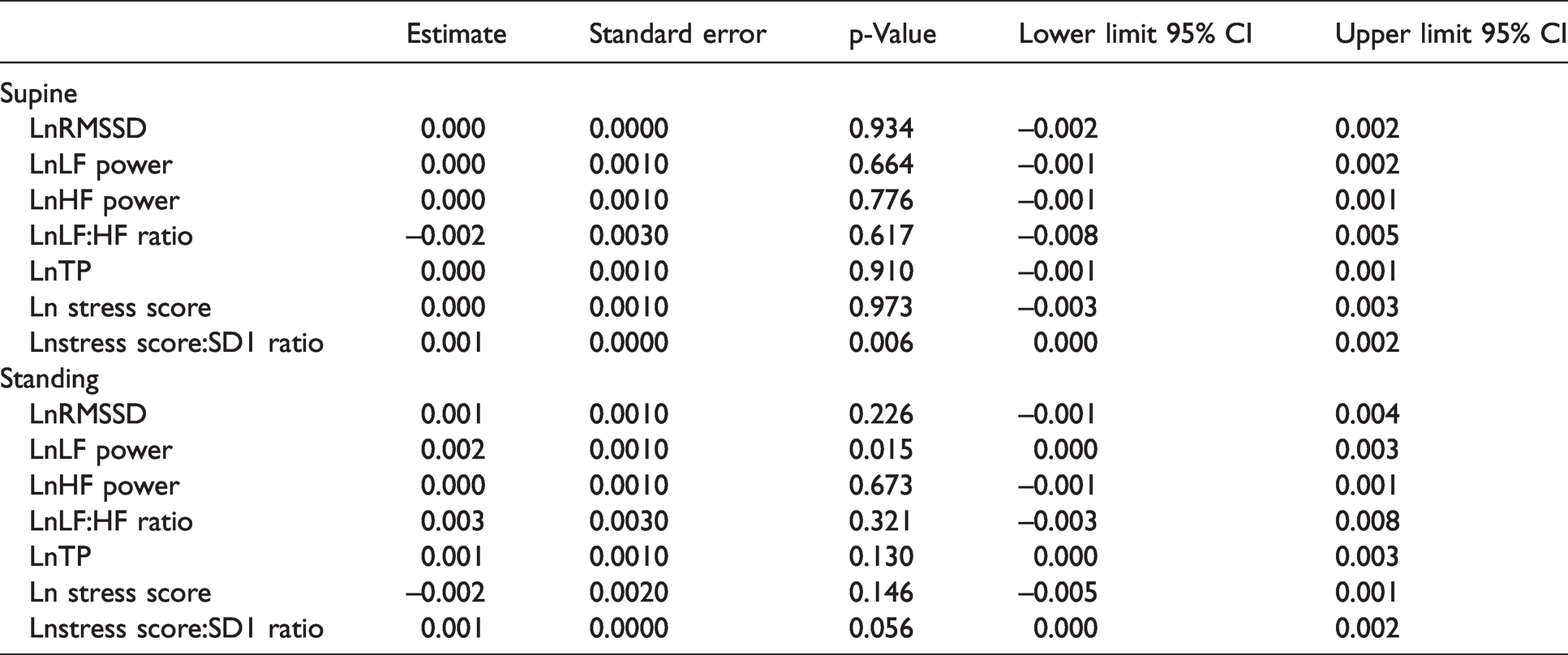
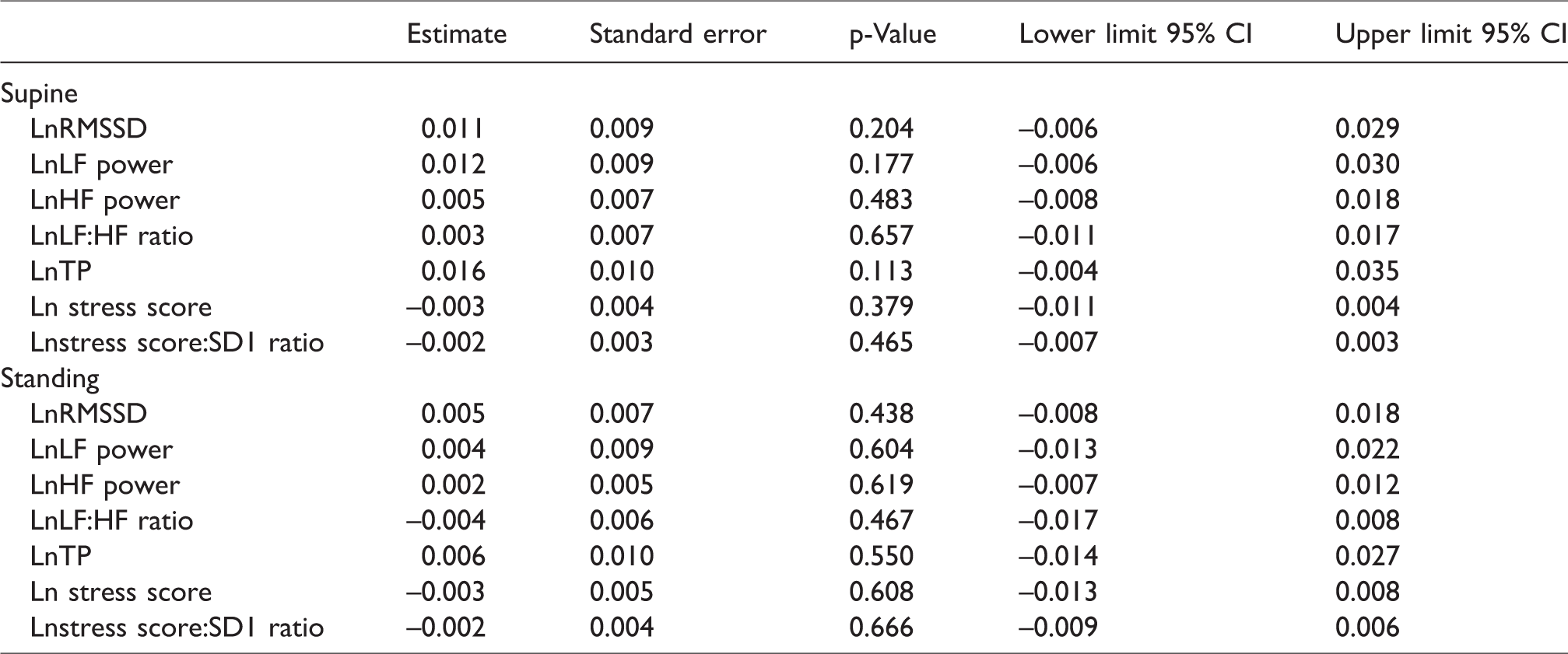
There were no relationships observed between any HRV metrics and Usg (Table 1). Participant-level random intercepts were initially included to account for the correlations within participants; however, the random intercept could only be included for one HRV metric (LnLF-HF ratio), as none of the other models would converge with the inclusion of a random intercept. As a result, all other models solely included the main effects of the HRV metrics. Table 1 shows that two HRV parameters had statistical significance associated with morning Usg – the Lnstress score:SD1 ratio (supine) and LnLF power (standing). These two outcomes are most likely Type I errors since the estimates are practically zero and the scatter plots are notably absent of any trends (Figure 1). Additionally, the scatter plots for the relationships between morning Usg and any HRV metric demonstrated no trends, which confirmed the GLMM outcomes (Figure 2 – LnRMSSD shown as a representative example). To help visualize the differing relationships between LnRMSSD and Usg, Figure 3 includes the scatterplot for 3 athletes. Similar to the outcomes with morning Usg, there were no relationships observed between percent changes in daily morning body mass and HRV metrics (Table 2). Participant-level random intercepts could not be included for HRV metrics due to convergence issues.
Fixed effects for the relationships between Usg and HRV metrics.
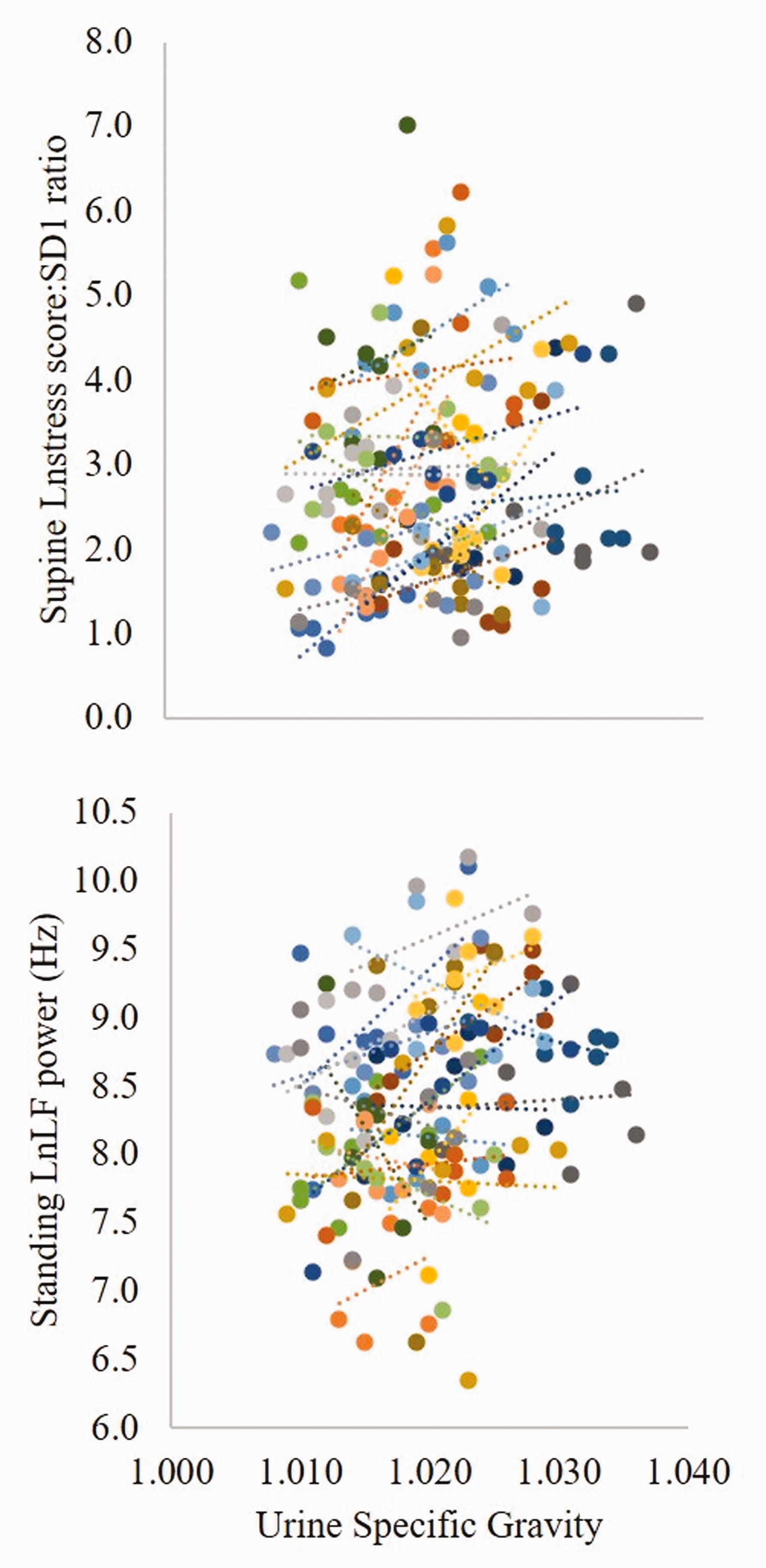
Scatter plots showing the relationships between LnStress score:SD1 ratio (supine) and Usg; and LnLF power (standing) and Usg. Individual trend lines were varied with some positive, some negative, and some without a relationship.
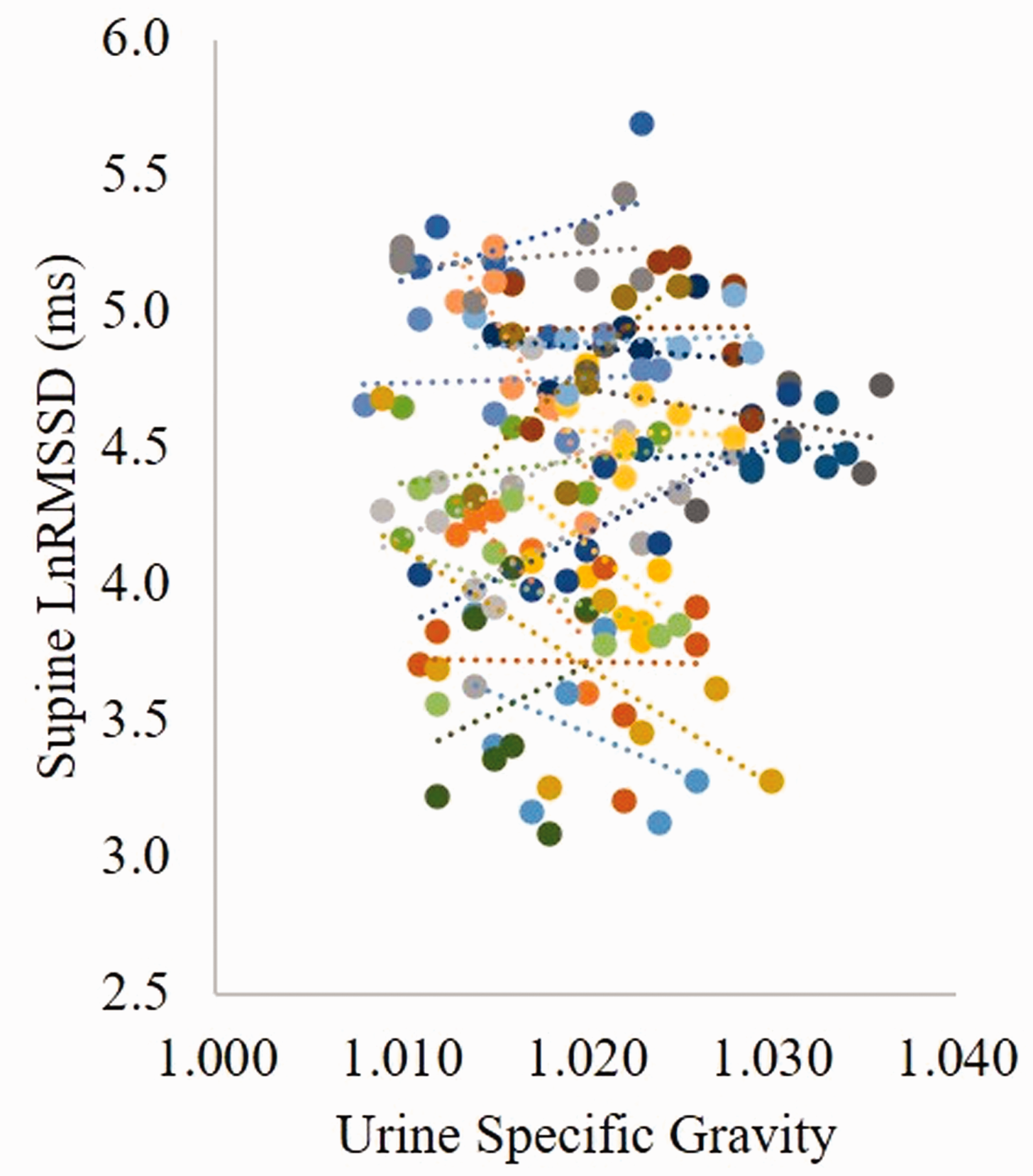
Scatter plot showing the relationship between LnRMSSD (supine) and Usg. Scatter plots between each HRV metric and Usg were nearly identical to what is shown here and omitted from the paper to save space.
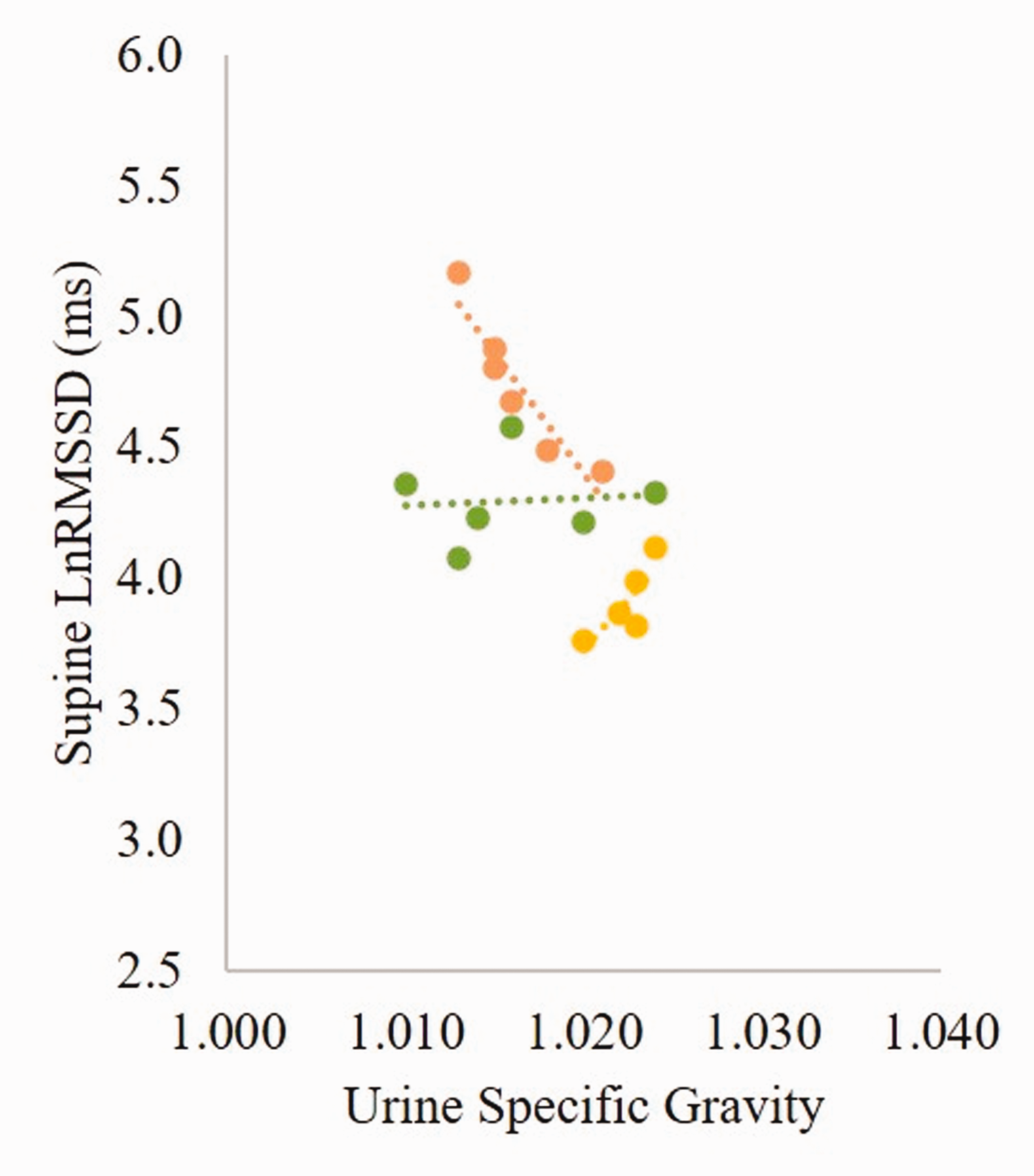
Scatter plot showing the relationship between LnRMSSD (supine) and Usg for 3 athletes to help visualize the different associations.
Fixed effects for the relationships between relative change in body mass and HRV metrics.
Discussion
The current outcomes demonstrate that morning resting HRV metrics were not related with morning-to-morning change in body mass or morning Usg in a field-based study of elite male athletes. The absence of relationships was observed for both supine and standing HRV indices. Previous studies indicated a link between HRV and dehydration,10,16–19 however, those relationships were likely context dependent. The assessment in these studies occurred during an acute window following exercise (i.e., 1–4 hr post-exercise) and often had slightly larger decrements in hydration markers than the current group of athletes. Therefore, several mechanisms may still influence post-exercise HRV when physiological homeostasis has not yet returned to normal, despite the consumption of fluids. Furthermore, all of the studies were focused on the effects of acute dehydration, so directionality as well as the magnitude of the change in hydration status could have possibly impacted the associations found.
In contrast, the morning assessment of body mass, Usg and HRV in the current study were performed 10–15 hours after the previous day’s final session, which is typical in these settings. This provided a longer period of time for rehydration, dinner and recovery (i.e., sleep). Indeed, the mean morning Usg and change in morning body mass was ∼1.020 and –0.17 kg (<–0.2%), respectively, suggestive that (on average) players were euhydrated each morning. However, the day-to-day ranges among the entire team were 1.010 to 1.035 and +1.3 to –2.0 kg, highlighting that these indirect indicators of hydration status spanned from hyperhydrated to hypohydrated. 20 These wide inter-individual ranges could result from variation in physical demands 21 and fluid consumption the prior day. Although players were regularly encouraged (and provided ample options) to rehydrate, actual fluid consumption in this group was not tracked. Unfortunately conducting a field-based study with elite athletes preparing for the Olympic Games imposes some limitations around monitoring all relevant components of fluid balance that are often included in laboratory studies. Regardless, perhaps the elongated time between training and measurements (the next morning) as well as attention to good nutrition and hydration practices enabled blood plasma volume to return to normal despite total body water deficits being observed in some players. These factors, when taken together with the high fitness levels of these players as well as the diligent planning of physical demands and recovery during this camp, seemed to result in adequate HRV reactivation 21 and subsequent absence of any relationship with indirect markers of hydration status.
Despite differences in processes that would normally be implemented in laboratory-based research, there was general standardization surrounding the measurements taken during this training camp and overall consistency in the daily routine.20,21 For example, all measurements occurred at the same time each morning following identical procedures. Upon waking, players voided their bladder to collect a first morning urine sample and Usg was measured within 15 minutes as a matter of standard practice. Monitoring Usg is suitable for field-based environments because of the relative ease of implementation and reasonably definable thresholds for practitioners to interpret.15,28 For HRV, a metronome was used to help regulate breathing frequency while monitoring heart rate during the orthostatic challenge. While there is some debate whether or not paced breathing is necessary while assessing HRV,29,30 similar to implementing a cadence during maximal exercise tests, it was believed the consistency in breathing would improve the ability to observe any intra-individual fluctuations in HRV metrics. 21
The athletes were allowed to hydrate freely throughout the day and meals were prepared by a nutritional specialist and provided at consistent times each day. While it might be possible that some changes in morning body mass were related to food consumption, to our knowledge none of the players were actively attempting to gain (over-consume) or lose (under-consume) body mass during this training camp. Indeed, the intra-individual variation of body mass was low 20 and aligned with previous research. 13 Therefore, the influence that food consumption the previous day might have on morning body mass was likely minimal and we are confident that changes in day-to-day body mass was a strong indirect indicator of hydration status.
A few of limitations should be noted. First, fluid consumption was not tracked in this study and so fluid balance could not be assessed. However, the day-to-day variation in morning body mass was low 20 suggestive of overall fluid recovery by these athletes. Second, there are other factors (e.g., daily physical demands) associated with heart rate variability metrics but the data included in the current analysis was so random that convergence was an issue even with the most basic models. In conjunction with the small sample size, it was decided to limit the amount of complexity introduced into the models and remain focused on HRV and hydration markers. Lastly, perhaps the magnitude of variability for the included parameters influenced the outcomes. For example, previous studies found relationships between HRV and dehydration when evaluated immediately after exercise when somewhat larger reductions in hydration markers were observed.10,16–19 However, this does not represent the typical approach to measuring HRV in athletic settings, therefore, smaller day-to-day variations are expected. 31 Future research that includes a greater time frame, wider physiological fluctuations of key metrics, and additional co-variates could offer additional insights.
The current study provides novel insights that demonstrate morning resting HRV indies (supine or standing) were not related with indirect markers of hydration status in elite male athletes during a training camp environment. Regardless of these outcomes, it is important to note that hypohydration and severe hypohydration identified by Usg (>1.020 and >1.030, respectively) occurred daily in a portion of players. Therefore, practitioners and coaches should consistently encourage their athletes to stay well hydrated, provide an environment to freely consume fluids, and monitor players daily to ensure beneficial changes are taking place for those who struggle with rehydrating.
Footnotes
Acknowledgements
Thanks to the athletes for participating and the coaches for their support. This study was supported in part by a grant from the Research Program in Applied Sport Sciences from the Ministry of Tourism, Culture and Sport (Ontario, Canada). The sponsor had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.