
Abstract
Often cognitive function is affected adversely during prolonged, high intensity exercise. We assessed whether hydrothermally modified corn starch (HMS) ingestion minimizes cognitive decline with soccer play. 11 men (177.7 ± 6.8 cm, 77.3 ± 7.9 kg, 22 ± 3 y, 12.8 ± 4.9% body fat,
Introduction
Cognitive function declines progressively during high intensity prolonged exercise, with reaction time being one of the most affected cognitive abilities. 1 In many sports, players must exercise intensely for extended time periods while having to make appropriate decisions rapidly. Thus, minimizing cognitive function decline while competing is critical for top performance. Further, carbohydrate (CHO) ingestion before and during exercise is well known to enhance performance2–4 and part of this may be related to the effects of CHO on brain function 5 , 6 via a better ability to maintain blood glucose. 2 , 7 , 8 Typically, glucose is the main fuel for the brain and because glucose storage in the brain is limited, a consistent supply from the blood can preserve optimal functioning. 9 Consistent with this are the data showing that hypoglycemia impairs cognitive function 10 and that the delivery rate of dietary CHO also affects cognition. 11 Moreover, fast absorbing (high glycemic index [GI]) CHO can cause transient decreases in blood glucose, if not ingested at regular intervals, and this could potentially impair cognition. Sport drinks contain high GI CHO and, therefore, must be ingested regularly throughout competition to avoid critical decreases in blood glucose. 12 In some team sports, regular CHO supplementation is more difficult because of the continuous play (e.g., players have more limited fluid ingestion opportunities and may even be restricted to before the match and/or at halftime). Consequently, a drink containing a slowly absorbable CHO (low GI) may be beneficial in such competitions. Hydrothermally modified corn starch (HMS) is a novel product (with modified physical properties by controlled heat–moisture processing, transforming it into a low GI CHO), 13 developed initially for children with a rare genetic disorder called glycogen storage disease. This condition is characterized by impaired liver glycogen metabolism, resulting in chronic hypoglycaemia and very poor exercise tolerance. HMS use is better than conventional treatments for these children because it helps to maintain more stable blood glucose values. 14 Consequently, HMS might improve cognitive function in long duration sports where liver and muscle glycogen stores are challenged, especially where limited supplementation opportunities are available. The observation that low GI breakfast food (slowly absorbed CHO) promotes better cognitive performance a few hours later in adults, 11 type 2 diabetics, 15 and children, 16 compared to a high GI breakfast food (rapidly absorbed CHO) is consistent with this hypothesis. However, to our knowledge, this possibility has not yet been assessed during repeated, intense, intermittent exercise, like that performed in many sport games. Therefore, the purpose of this study was to assess whether HMS ingestion can attenuate any decline in cognitive performance during a simulated soccer match when CHO is ingested only before and at 45 min of exercise, compared to a rapidly absorbed CHO.
Methods
Participants
Eleven healthy, men (177.7 ± 6.8 cm, 77.3 ± 7.9 kg, 22 ± 3 y, 12.8 ± 4.9%BF, and
Preliminary sessions
Participants visited the laboratory on two separate occasions prior to any experiments for familiarization sessions. During the initial visit, body composition (Bod Pod®, COSMED, Concord, CA),
Experimental sessions
A double blind, randomized, crossover research design was implemented involving two experimental treatments, HMS (UCAN Co., Woodbridge, CT, USA; GI = 30) 13 or dextrose monohydrate (DEX; GI = 100). The blinding was successful as only two of the 11 participants (18%) guessed the correct treatment. None of the participants reported any GI distress with any of the drinks. The experimental trials were separated by at least one week and were rotated systematically to prevent order effects. To minimize food intake differences across treatments, the athletes recorded their entire food/drink intake for the two days prior to the first experimental session and replicated this intake the two days preceding their second trial. Further, all were provided a standardized low CHO meal (9 kcal•kg−1 body mass with a CHO content of 1 g•kg body mass−1 [∼ 40% carbohydrate, 30% fat and 30% protein]) at ∼1930 h the night preceding testing to minimize the intra- and inter-variability of nutritional status and to ensure CHO stores would be low during the later stages of the subsequent simulated game.
Participants reported to the laboratory at 0730 h after a 12 h overnight fast having abstained from strenuous exercise, caffeine or alcohol for the 24 h prior to testing. Ad libitum water intake was allowed during the fasting period. Upon arrival, baseline blood glucose (FreeStyle Freedom Lite®; Abbott Diabetes Care Limited, Mississauga, ON, Canada) concentration and resting metabolic rate (Vmax Legacy; Sensor-Medics, Yorba Linda, CA) were assessed. Subsequently, baseline cognitive function was estimated (the Eriksen-Flanker test and the Serial Seven subtraction test – see below for details). Afterwards, participants consumed the corresponding drink treatment, 30 min was provided prior to any exercise to allow for gastric emptying/absorption, and a 10 min pre-match warmup was completed. Both experimental drinks consisted of an 8% CHO solution containing a total of 0.7 g•kg body mass−1•h−1 (2.8 kcal•kg body mass−1•h−1) of the corresponding CHO (HMS or DEX) divided into two intakes (first intake was 497 ± 48 ml containing 0.5 g CHO•kg body mass−1; second intake was 199 ± 18 ml containing the remaining 0.2 g•kg body mass−1 and was consumed after 45 min of exercise, i.e., at half time of the simulated match). The quantity of CHO ingested and the volume of water used to prepare the beverages were determined based on ACSM guidelines. 19 The electrolyte concentration in both beverages was controlled using a non-energy flavoured electrolyte replacement powder (UCAN Hydrate®) that contained 94 mg•L−1 of magnesium, 282 mg•L−1 of chloride, 563 mg•L−1 of sodium, 188 mg•L−1 of potassium and 28 mg•L−1 of calcium. In addition, participants were allowed water ad libitum and the trial one intake was recorded (588 ± 258 ml) and reproduced during trial two.
The simulated soccer game was comprised of four x 15-min intermittent running blocks interspersed with three min of passive recovery, followed by some soccer skills testing (Figure 1) as described previously.
4
The intensities and times used during each block were full stopping (15 s), walking (35 s), jogging (46 s at 55%
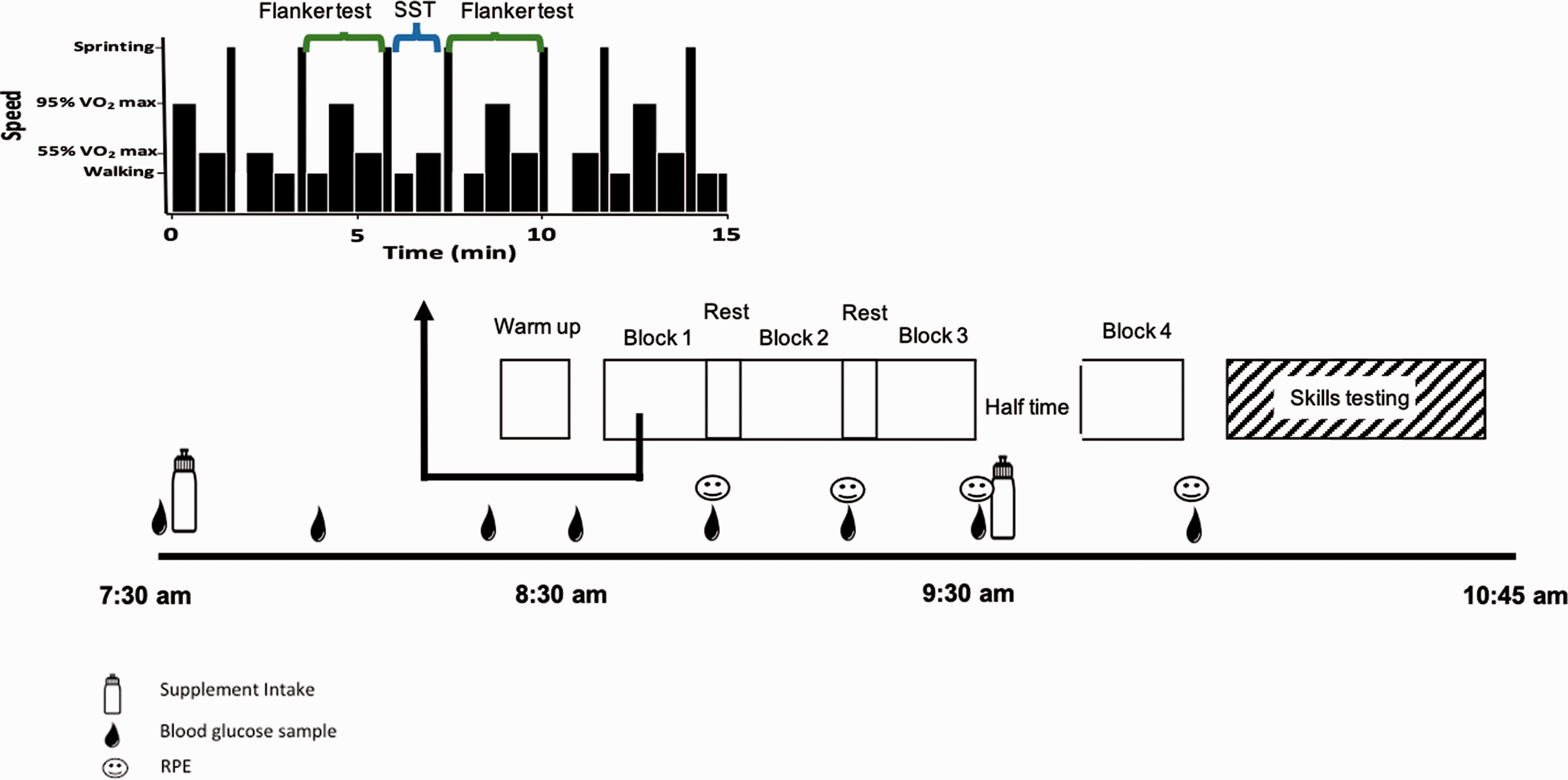
Study protocol.
Cognitive testing
Eriksen-Flanker test. 23
This is a response inhibition task which measures the ability to suppress responses that are inappropriate in a particular context. Briefly, this test presented five arrows centered linearly on a computer screen. Athletes were instructed to indicate the direction of the center (target) arrow while ignoring the four flanking it. Each test was comprised of 40 random trials (20 congruent and 20 incongruent). The congruent trials consisted of the target arrow being flanked by arrows that faced the same direction (e.g., ←← ← ←← or →→ → →→) while the incongruent trials consisted of the target arrow being flanked by other arrows that faced the opposite direction (e.g., ←← → ←← or →→ ← →→). To respond, participants pressed a button on a handheld device interfaced with a computer, while running on the treadmill. The button for each hand also corresponded to the direction of the center arrow on the computer screen, regardless of the trial (congruent or incongruent). This test was performed twice within each exercise block for a total of 320 trials (160 congruent and 160 incongruent) during the soccer match simulation. The task was scored as mean choice reaction time (ms), accuracy (%), and conflict cost (also known as the ‘Flanker effect’) (ms). Eriksen-Flanker conflict cost was quantified as the difference in mean choice-reaction time between congruent and incongruent trials.
Serial seven subtraction. 24
Participants completed a one min verbal version of the serial-seven subtraction task once for each of the four exercise blocks throughout the protocol. The starting number for all trials was between 800–999 and chosen by means of a random number generator. Participants were instructed to subtract seven recursively from the starting number as quickly and as accurately as possible within the allotted one min. Time commenced once participants repeated the original number. If a mistake was realized, participants were encouraged to not correct themselves but to continue subtracting seven from the erroneous value and subsequent responses were scored in relation to the incorrect number. All verbal responses were recorded audibly to ensure answers were quantified accurately. To minimize any potential learning curve, participants completed practice trials during familiarization visits, as mentioned, as well as before each simulated match. Each trial was quantified as the proportion of correct responses over one min.
Statistical analysis
Statistical analyses were performed using SigmaPlot for Windows (Version 12.0, SYSTAT, San Jose, CA). All data were checked for normality and sphericity. A power test to justify sample size was also performed. Blood glucose concentrations and RPE were analyzed using two-way (condition by time) repeated-measures ANOVA. Post hoc Tukey’s Honest Significant Difference (HSD) testing was used, where necessary. The Eriksen-Flanker test and serial seven-subtraction test were analyzed using paired t tests. Significance was set at p ≤ 0.05. Data are presented as means±SD.
Results
Blood glucose
There was a main effect of time (p < 0.001) and treatment (p = 0.006), as well as a significant interaction (p < 0.001) for blood glucose concentration, as reported previously. 4 Blood glucose concentration was lower (p < 0.001) for HMS at both 15 (5.3 ± 0.6 vs 7.7 ± 1.4 mmol•L−1) and 30 min (5.6 ± 0.6 vs 8.3 ± 1.0 mmol•L−1) post treatment ingestion and greater (5.8 ± 0.5 vs 5.1 ± 0.6 mmol•L−1, p = 0.004) after the first exercise block (55 min post ingestion) compared to DEX.
Ratings of perceived exertion (RPE)
A main effect of time (p < 0.001) was detected for RPE (Figure 2). As expected, average RPE for block 1 was lower than both block 3 and block 4. No treatment effect (p = 0.24) was observed but there was a treatment x time interaction (p = 0.013). Pairwise post hoc comparisons indicated that the average RPE for block 1 was lower with HMS (p = 0.025) compare to DEX.
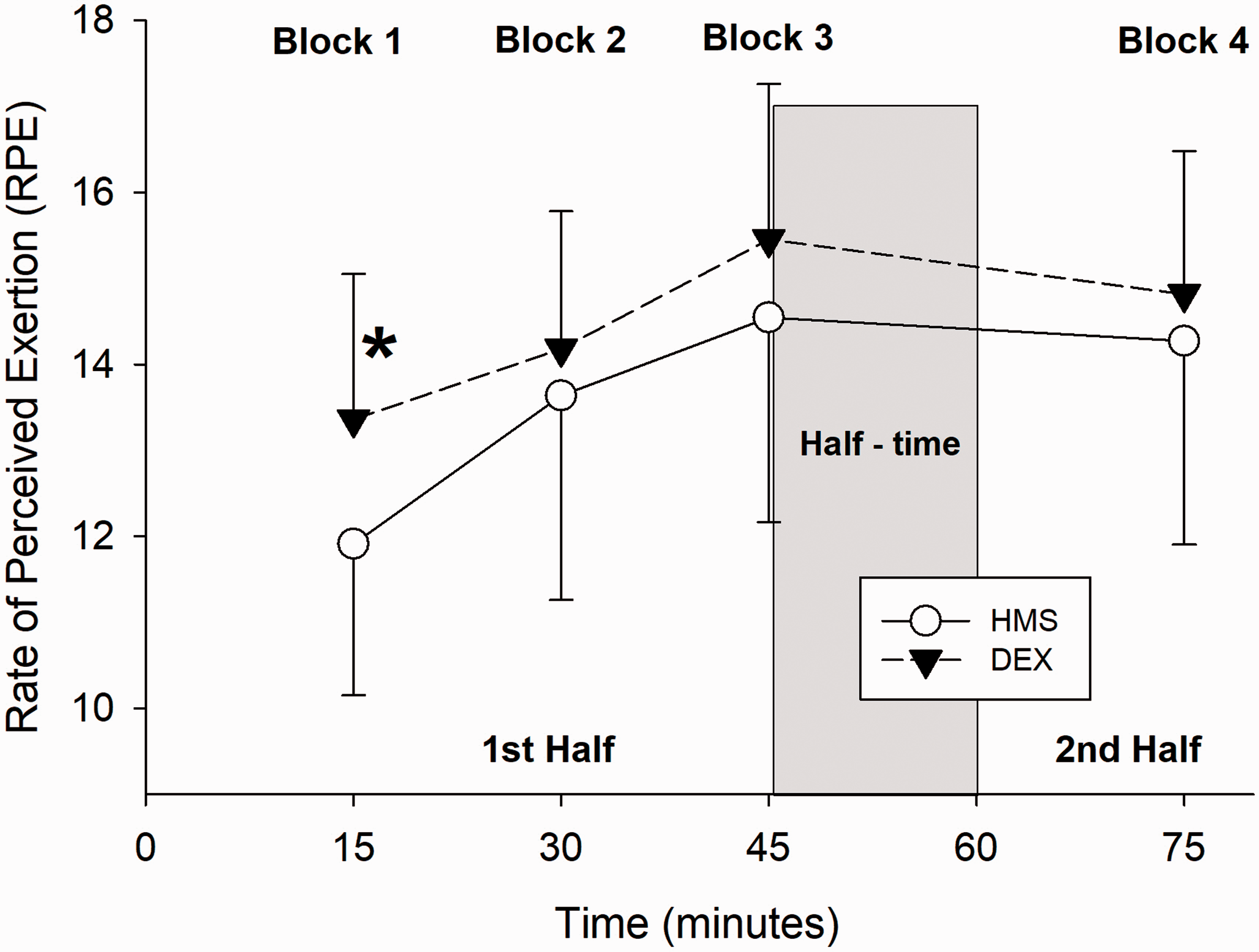
Ratings of perceived exertion during a simulated soccer match. Values are means ± SD for DEX (filled triangles, n = 11) and HMS (open circles, n = 11). *p = 0.025 vs HMS.
Measures of cognition
Eriksen-Flanker task
There was no significant difference in reaction time (p = 0.48) nor accuracy (p = 0.81) for the congruent trials. However, the reaction times during the incongruent trials were faster (p = 0.04) with HMS supplementation compared to DEX without compromising accuracy (p = 0.43) (Figure 3). As a result, better cognitive control or lower conflict cost (p = 0.019) was observed with HMS supplementation compared to DEX.
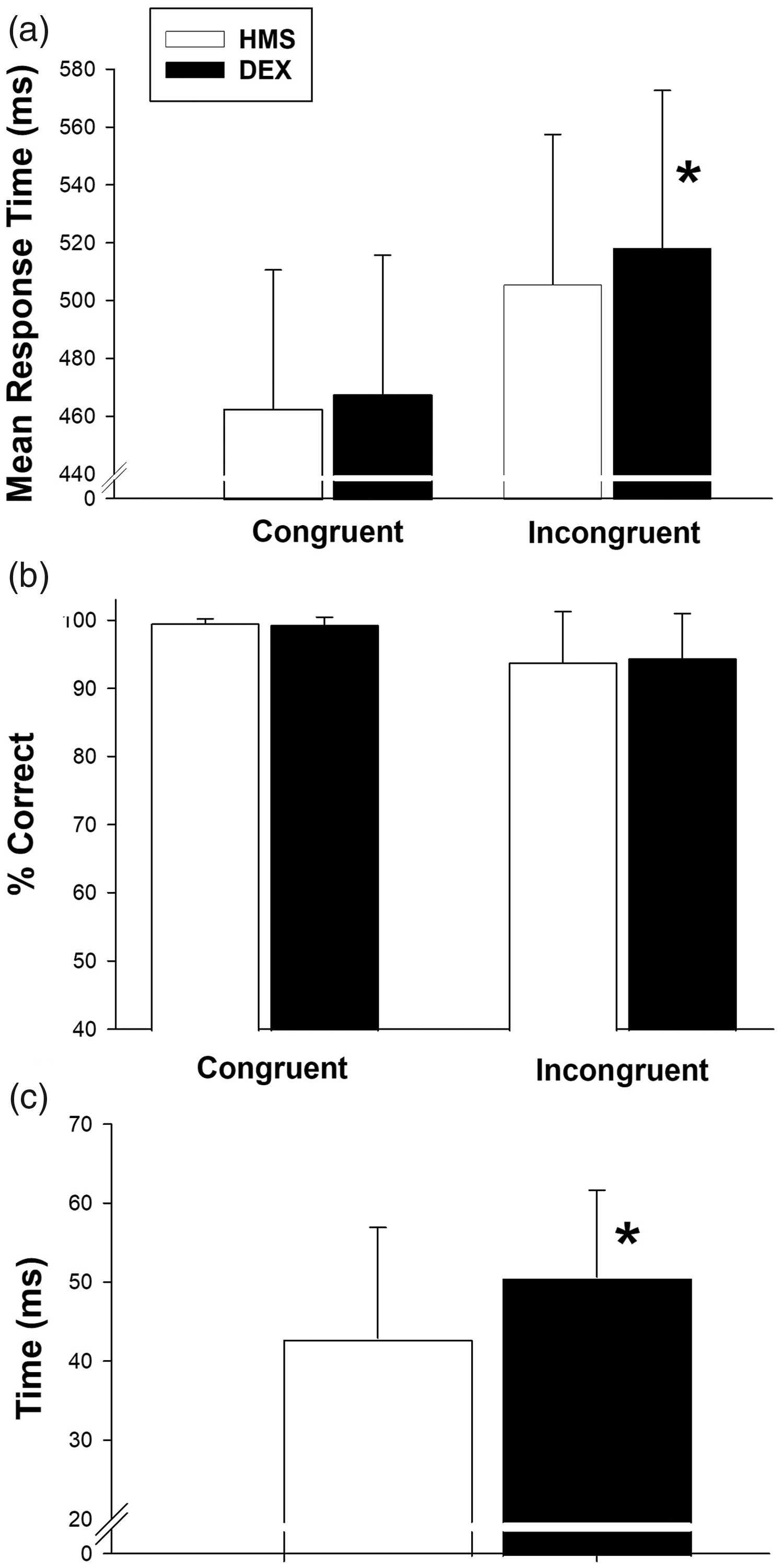
Cognitive function during a simulated soccer match. Values are means ± SD. A) HMS (white bars) improved (*p = 0.04) reaction time vs DEX (black bars) during the incongruent trials. B) There were no differences in accuracy between treatments. C) Conflict cost (or interference) was reduced (*p = 0.019) with HMS (white bars) vs DEX (black bars).
Serial seven subtraction test
No significant differences were found for either the number of responses (p = 0.82) or the accuracy (p = 0.39) of those responses during this test (Table 1).
Serial seven subtraction test.
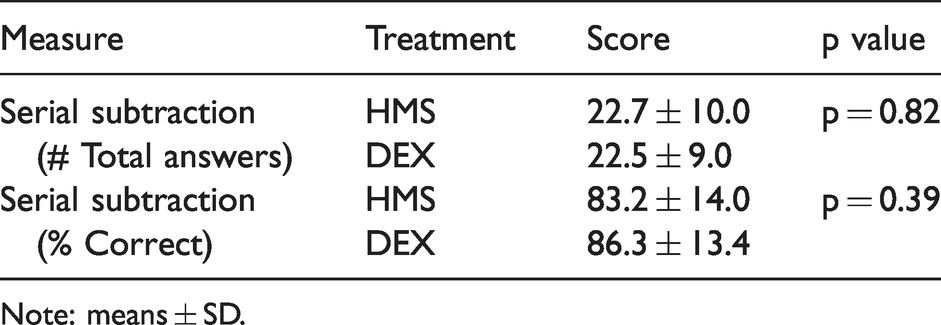
Note: means ± SD.
Discussion
The main finding of this study was that HMS supplementation before and at half-time of a simulated soccer match reduced Flanker interference significantly and improved reaction time significantly during the incongruent trials while maintaining response accuracy vs isoenergetic DEX. This is important as reaction time, response interference, accuracy, and number of responses were measured using cognitive tasks validated for assessing mental processes related to executive functions such as working memory, selective attention and inhibitory control. 23 , 25 , 26 Moreover, HMS displayed more stable blood glucose concentrations and reduced perceived exertion during the simulated match.
To our knowledge, this is the first study to assess cognitive performance during a prolonged, intense, intermittent exercise protocol while consuming a high GI CHO (DEX) vs a low GI CHO (HMS) and suggests the latter can enhance at least some aspects of cognitive function during athletic contests.
Of course, diminishing CHO availability over the course of a soccer match could result in mental fatigue. 27 Although regular (every 15 min) CHO supplementation before and during exercise has been shown to attenuate this decline, 5 , 6 it is difficult to ingest CHO at regular intervals in some sporting activities due to their nature or the rules. This could lower blood glucose concentration and impair cognitive abilities. 10 The results of our study suggest that supplementing with a slowly absorbable CHO results in better cognitive performance, compared to a more rapidly absorbed CHO, at least when supplementation occurs only before the game and at halftime.
One possible limitation in our study was the unique dietary guidelines our participants followed previous to the evaluations. Although it is true that most soccer players would not follow our pre-match dietary strategy, it is known that soccer match play lowers muscle glycogen by 40–90%. 28 We utilized a reduced and controlled pre-study dietary CHO approach in order to ensure that significant glycogen depletion occurred during our simulated soccer match as well as to control CHO availability under both our experimental treatments.
As expected, reaction time was quicker and accuracy better during the congruent trials of the Eriksen-Flanker test with both treatments, compared to the incongruent trials. Further, as reported by Eriksen & Eriksen, 23 often participants respond more slowly to incongruent trials because of the need to utilize top-down control. Importantly, reaction time during the incongruent trials was improved with HMS supplementation, compared to DEX. Moreover, conflict cost or Flanker interference was improved as well with HMS supplementation. This would likely be beneficial for any athlete competing in activities involving repeated, intense, intermittent exercise, i.e., in activities when glycogen availability is challenged, especially as numerous split-second decisions are often required. 29 , 30 But of course, this hypothesis would have to be tested during real play.
In contrast, differences were not observed with the SST, which is considered a measure of working memory. 26 In hindsight, this task requires a reasonable level of arithmetic skill and perhaps that is the critical determinant of performance with this type of test. Alternatively, this test may not be difficult enough to differentiate between conditions, i.e., it may not be the best predictor of decision-making in sports.
It is interesting that these differences in cognitive function were seen despite participants not being in a hypoglycemic state; however, as mentioned, cognitive function is not only affected by hypoglycemia but also by the delivery rate of CHO to the brain. 11 Given the differences in GI of both treatments, it is plausible that DEX resulted in greater insulin release, directing glucose more towards other insulin sensitive tissues and thereby reducing the flow of glucose from the blood to the brain.
During our simulated soccer game, RPE was also lower with HMS (significantly during the first 15 min of exercise, p = 0.025), suggesting that the participants found the exercise to be less difficult, particularly at the beginning. Others have also shown that ingesting low GI CHO prior to exercise can result in lower exercise RPE. 31 , 32 Further, in our study, there were significant differences in blood glucose in the first stages of exercise that correlated with RPE, i.e., the athletes felt the standard exercise bout studied was less rigorous initially with HMS, consistent with the observed more modest changes in blood glucose. This could mean that in an actual soccer game when intensity is not fixed, athletes ingesting HMS would be able to exercise harder and, therefore, perform even better, assuming a comparable skill set.
Practical application
This study provides insight into what type of CHO ingestion is best during activities that challenge CHO stores and have limited opportunities for supplementation. Based on these data, low GI CHO ingestion before and at halftime may attenuate decrements in decision-making often seen in sporting activities where CHO availability is compromised.
Conclusion
HMS supplementation vs isoenergetic DEX prior to and at halftime of a simulated soccer match affected blood glucose favourably, reduced perceived exertion, and displayed better cognitive function during the simulated match. These data suggest HMS can improve some aspects of cognitive function during sports characterized by repeated, intense, intermittent exercise at least when in match CHO supplementation is limited. More study is needed to assess fully the possible cognitive benefits of HMS for athletes.
Footnotes
Acknowledgements
The authors would like to thank Victor Nguyen and Aaron Rode for their help with the data collection as well as the participants for their dedication and commitment.
Authors’ contribution
The study was designed by Manuel D. Quinones and Peter W.R. Lemon; data was collected and analyzed by MDQ; data interpretation and manuscript preparation were undertaken by MDQ and PWRL. Both authors approved the final version of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received financial support from Generation UCAN®, but no one from the company was involved in the data collection, interpretation, or study conclusions.