
Abstract
This study aimed to investigate the association between training load indices and Upper Respiratory Tract Infection (URTI) across different lag periods in elite soccer players. Internal training load was collected from 15 elite soccer players over one full season (40 weeks). Acute, chronic, Acute:Chronic Workload Ratio (ACWR), Exponentially Weighted Moving Averages (EWMA) ACWR, 2, 3 and 4-week cumulative load, training strain and training monotony were calculated on a rolling weekly basis. Players completed a daily illness log, documenting any signs and symptoms, to help determine an URTI. Multilevel logistic regression was used to analyze the associations between training load indices and URTIs across different lag periods (1 to 7-days). The results found a significant association between 2-week cumulative load and an increased likelihood of a player contracting an URTI 3 days later (Odds Ratio, 95% Confidence Interval: OR = 2.07, 95% CI = 0.026-1.431). Additionally, a significant association was found between 3-week cumulative load and a players’ increased risk of contracting an URTI 4 days later (OR = 1.66, 95% CI = 0.013–1.006). These results indicate that accumulated periods of high training load (2- and 3-week) associated with an increased risk of a player contracting an URTI, which may lead to performance decrements, missed training sessions or even competitions.
Introduction
A coach’s role is to optimize a player’s performance while also making efforts to ensure the protection of a players’ health and welfare. 1 Illness has been found to be the second most common reason for missed training and matches in soccer, 2 which can have a considerable impact on a team’s performance. 3 Upper Respiratory Tract Infections (URTIs), also known as the ‘common cold’, 4 have been reported as the most common illness in soccer (74.5%). 1 Training load is widely used to manage fatigue and reduce the risk of overtraining, injuries and illness. 5 Training load data can be quantified from internal and/or external measures. Internal load is a player’s physiological and/or psychological response to an external load, and can be measured by session Ratings of Perceived Exertion (sRPE). 6 External load is the objective physical load applied to the athlete and can be measured through a variety of methods including, Global Positioning Systems (GPS) using metrics such as total distance covered, high-speed distance covered during matches or training sessions. 6 Where possible, training load monitoring should incorporate several measures of internal and external load, to provide coaches and support staff with a holistic view of a player’s training response. 5 However, this may not always be possible due to time and financial constraints, logistics and resources (e.g. number of coaches). sRPE is a valid and reliable,7–9 simple method used to calculate and quantify an individual’s internal training load, making it a time-efficient practical tool for coaches. 10 For the purpose of this study and clarity, internal training load (sRPE) is defined as the perception of effort to indicate the physical load experienced by an athlete. 11
Moderate intensity exercise has been found to protect an individual from an URTI, while heavy exertion or prolonged intensive exercise increases the risk of an URTI. 12 It has previously been reported that a period of increased training intensity 13 or a high training load 14 can result in higher incidences of URTIs in elite Rugby Union, 13 tennis, 14 and futsal players. 15 Although the study by Cunniffe et al. 13 in Rugby Union players was completed over a full season, only mean weekly training load data were analyzed and illness logs were collected weekly, rather than daily. Daily data collection may provide a greater insight and an earlier time-point to identify when an URTI may have occurred. Moreover, their finding that peaks in URTIs occurred after periods of intensified training was an observed trend, and not statistically significant. 13 Novas et al. 14 found that symptoms of URTIs increased with higher training duration and load but not training intensity in tennis players. However, the study was conducted over 12 weeks and training load was quantified as an estimation of energy cost, while competition load was collected and analyzed separately as RPE (a measure of match intensity), match duration, numbers of matches played and relative importance of a match. It should be noted that RPE and duration were not multiplied to provide sRPE, which is more widely used as an internal load marker of training load, which incorporates all training sessions and competitions).6,16 These differences in training load calculations make comparisons between studies more difficult. Moreira et al. 15 found high intensity training increased the severity of URTI symptoms in futsal players, and that a decrease in training load (∼50%) was accompanied with a significant reduction (p < 0.05) in incidences of URTIs. The authors stated that the taper phase may be an appropriate strategy to minimize fatigue and optimize the health status of the athletes. This may be due to the taper phase having a reduction in training load after an intensified period of training, which was found to associate with a decrease in URTI symptoms. A limitation of this study was the acute nature of data collection, which was conducted over a 4-week intensive training period. The acute nature of this study, 4 weeks, 15 the infrequent collection of illness logs, 13 and testing over an intensified period of training, 15 highlights that longitudinal research over an entire soccer season, collecting daily data, is required to investigate the association between training load and URTI. A longitudinal study with more frequent data collection may help to explore trends of URTI across a season, and allow for the investigation of any change or accumulation of training load, which may be associated with a greater risk of illness. 3
In contrast to the previous research, Anderson et al. 17 found no relationship between training load and illness, in collegiate basketball players, over a 21-week period. However, all illnesses were analyzed together rather than separated illness categories (e.g. URTI). Additionally, training load data were averaged for each week, which meant it may not have taken into account the individual fluctuations or variance of players. A previous study in elite Rugby Union players 18 found no association between training load and URTIs, over a pre-season period (10 weeks). However, training load data in these studies13–15,17,18 were analyzed in weekly blocks (e.g. Monday-Sunday) rather than rolling weekly analysis (Table 1). Rolling weekly analysis means training load data can be analyzed from the exact incidence day rather than a specific week, where the illness may have occurred at the beginning or end of the training week and thus, omitting training load data. Furthermore, none of the previous studies13–15,17,18 investigated the lag period between training load and the onset of an URTI. Lag period has been defined as the period between the training load and the subsequent illness. 11 This may be beneficial for a coach to provide the earliest time-point in which to alter training load, if required.
An example of 1-day to 4-day lag period with rolling weekly training load data.
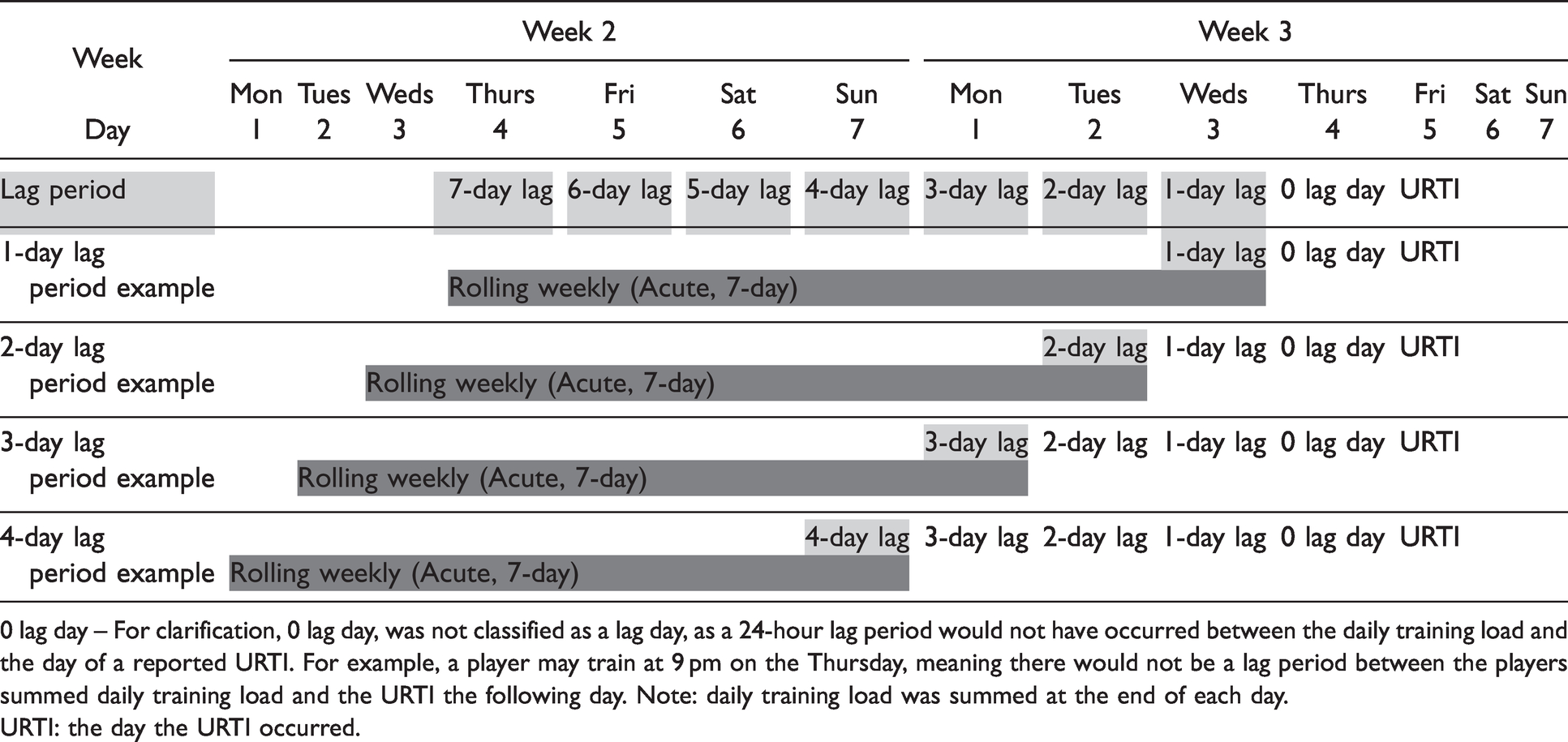
0 lag day – For clarification, 0 lag day, was not classified as a lag day, as a 24-hour lag period would not have occurred between the daily training load and the day of a reported URTI. For example, a player may train at 9 pm on the Thursday, meaning there would not be a lag period between the players summed daily training load and the URTI the following day. Note: daily training load was summed at the end of each day.
URTI: the day the URTI occurred.
Similar to the dearth of research investigating rolling weekly analysis across different lag periods, there is currently a lack of research investigating associations between different training load indices with URTIs. Previous research has explored acute training load association with URTIs,12–14 while Piggott et al. 19 and Putlur et al. 20 explored training monotony and training strain association to all illnesses. Training monotony is the variability of practice (Table 2) and training strain is the stress demand on an athlete over a week (Table 2). 17 Putlur et al. 20 found that 55-64% of illnesses occurred with a proceeding spike (no percentage increase was provided) in training load, monotony or strain, in female soccer players over 9 weeks. Similarly, Piggott et al. 19 also found that 42% of illnesses occurred after a > 10% spike in training load, and 33% occurred with a spike in training monotony but no association with training strain was reported in AFL players, over a 15-week pre-season period. However, to the best of the authors’ knowledge, no previous studies to date have investigated the association between training load indices: Acute: Chronic workload Ratio (ACWR) uncoupled, Exponentially Weighted Moving Averages (EWMA) ACWR, cumulative load (2, 3 and 4 weeks), training strain and training monotony with URTIs in soccer players.
Training load indices and calculations.
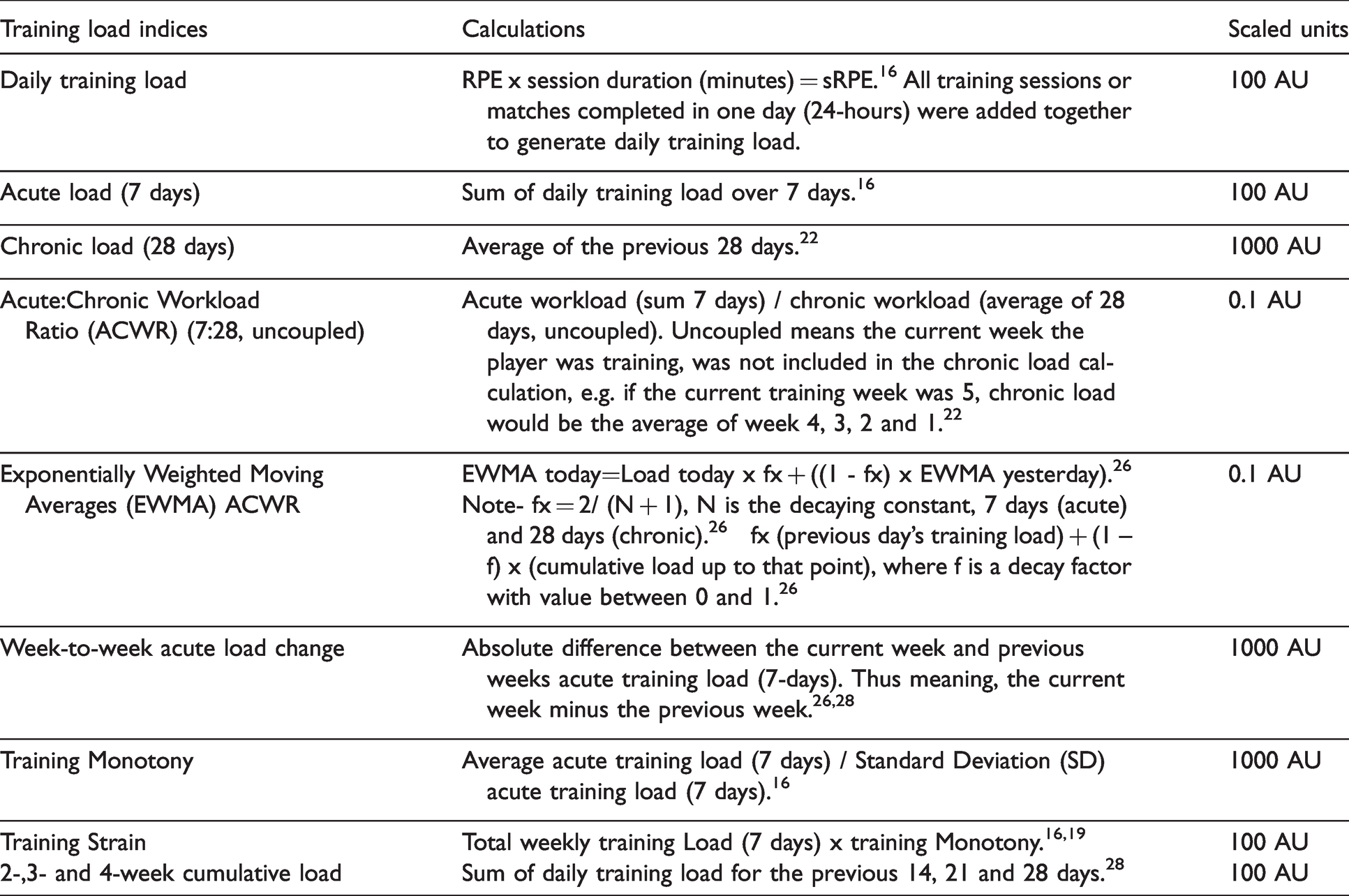
ACWR is the ratio between acute load (sum of 7 days training load) and chronic load (average of the previous 28 days training load), which indicates whether the acute load is greater, less or equal to the preceding chronic load. 21 The uncoupled approach should be used to ensure the most accurate calculation of ACWR, as the current week of training (acute) is not included in the chronic load. 22 In contrast, recent research has explored EWMA ACWR as another index of training load. This measure gives a greater weight to the most recent training load and a decreased weighting to the older training load, 23 while ACWR weights all training loads equally. It has been found that EWMA ACWR may be a more sensitive measure of training load. 23
To the authors’ knowledge, there is currently no longitudinal, ecologically valid research investigating the association between training load indices, using rolling weekly analysis, and URTIs in soccer. Therefore, the aim of this study was to investigate the association between training load indices and URTIs, across different lag periods in elite soccer players.
Methods
Approach to the problem
Data were collected daily over an entire soccer season, 40 weeks, resulting in 280 data points (observations) per player. The season comprised of 47 games, with 1-week off in June. A familiarization and verbal anchoring 24 period took place during the first week of pre-season, to ensure the players accurately provided RPE values, as this was the first time the players had completed RPE monitoring. All testing took place at the soccer team’s training facilities, to ensure minimal disruption to training and continuity with the players’ normal training schedule. The principal researcher (CT) was at every training session to ensure data were collected accurately.
Participants
Fifteen male elite outfield soccer players volunteered to take part in the study (mean ± SD, age 23.4 ± 4.8 years, height 180.8 ± 5.8 cm, body mass 77.1 ± 5.1 kg). All players were contracted and played for the senior first team, competing in the country’s highest level of competition (the Irish Premier League). A typical training week consisted of 4 team training days and a match. The weekly training and competition sessions included fitness conditioning, gym/resistance training, skills, conditioned games, friendly and competitive matches. All players were informed of the study requirements and provided written informed consent. The study was approved by the University Research Ethics Committee.
Procedures
Training load
sRPE was calculated by RPE x session duration (minutes), 16 and was collected after every training session and match, whether sessions were individual or team based. sRPE was recorded on a purpose built App, installed on the players phone, to avoid external influences. 25 For team sessions, the coach recorded the duration and type, whilst for individual sessions, the players recorded, through their app, the session duration and type. Where multiple sessions were completed in a day, the sRPE loads were summed to give a daily training load (Arbitrary Units, AU) (Table 2). 26 Recovery days were noted as 0. 27 All training load indices were derived from sRPE, using rolling weekly analysis. The calculation of all indices and their scaled units are presented in Table 2. RPE has been found to be a reliable and valid method of quantifying exercise intensity in soccer 7 and sRPE has been found to be a valid and reliable monitoring marker for internal load compared to heart rate8,9 and blood lactate. 16
Upper respiratory tract infection (URTI)
In addition to training load, players subjectively reported, on their mobile phone app, daily feelings of illness prior to training, by answering the following question: ‘Do you feel unwell/sick?’. If player’s answered yes, they were brought to a further form to complete the following questions shown in Table 3. 29
Subjective reporting of illness on a purpose-built app.
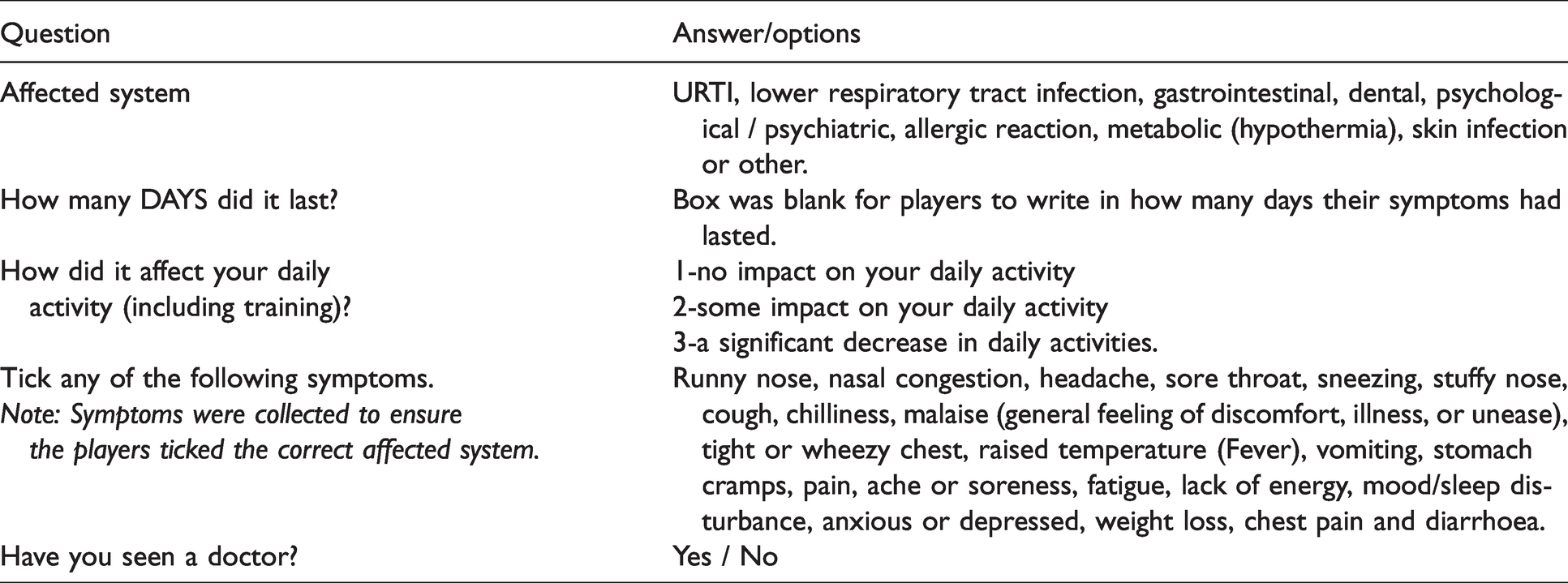
An URTI was classified as lasting two or more days, with players presenting at least two of the following symptoms: a runny nose, nasal congestion, headache, sore throat, sneezing, stuffy nose, cough, nasal discharge, tight or wheezy chest, malaise and chilliness.30,31 If the player met the criteria of 2+ symptoms for 2+ days,30,31 the researcher followed up with the player to ensure it was an URTI and not another illness (e.g. fever, aches) or an allergic reaction. If the researcher was uncertain of the nature of the illness, the player was sent to a doctor for diagnosis. However, in the current study this did not apply.
Lag period analysis
The lag period for the current study was analyzed daily using a sequential assessment, 1 to 7 days prior to an URTI. The reason for a sequential assessment was due to rolling weekly training load being used, if set lag periods e.g. 3-day or 7-day were analyzed, training load data would be omitted. For clarification, lag period in the current study was classified as at least 24 hours preceding an URTI (Table 1). For example, if an URTI occurred on a Friday, 1-day lag would be the preceding Wednesday (Table 1). This was to ensure there was a 1-day (24-hour) lag period before the potential URTI, as daily training load data were summed at the end of each day.
Statistical analysis
All statistical analyses were conducted using MLwin software (version 3.01). Descriptive statistics were calculated for all variables, and assumptions for parametric analysis were explored. Odds Ratio (OR) and 95% Confidence Intervals (CI) were calculated. Where an OR was greater than 1, an increased odds of an illness was reported and an OR less than 1, a decreased odds of an illness was reported. 28 A multilevel logistic regression, level 1 (days) and level 2 (players), was used to analyze the data for URTI (dependent variable) and the training load indices (independent variable). Training load indices were scaled by the units as shown in Table 2. Significance levels were set at p ≤ 0.05.
Multilevel logistic regression was used as it allowed within participant analysis for each player across 40-weeks, this allowed for repeated measures resulting in 280 observations per player. This analytical (multi-level) approach reduced the independent observation assumption, thus allowing within participant comparisons. This provides the opportunity to analyze within player changes over time, which is fundamentally important in the context of this research, as each player is individual and will react/respond differently to the same training.
Results
Over the 40-week period, 22 illnesses were recorded from the 15 players included in this study. URTIs was the highest occurring illness over the season (n = 10; 45%). The URTI lasted a minimum of 2 days and maximum of 10 days, with the average URTI lasting 4 days. Of the 10 reported URTI’s, 9 highlighted the URTI had ‘some impact on their daily activity’, which included training. A typical training week included 2 gym sessions, 3 pitch sessions and a match. The training load for a typical gym session, training pitch session and match were 202 ± 94 AU, 310 ± 150 AU and 523 ± 240 AU, respectively. The overall training load across a typical week was 1,614 ± 586 AU.
The results of the multilevel logistic regression analysis, used to identify associations between a number of training load indices and an URTI, are given in Table 4. There was a significant association found between 2-week cumulative load and URTIs, 3 days prior to an URTI (OR = 2.07, 95% CI = 0.026-1.431; p = 0.042) (Table 4). Where 2-week cumulative load increased by 1-unit (1000 AU) over 3142 AU (e.g. 3142 to 4142 AU) a player was at a 73% increased risk of contracting an URTI 3 days’ later.
Odds ratio (OR), 95% Confidence Intervals (95% CI) for daily lag period (1 to 7 days) from the multi-level analysis.
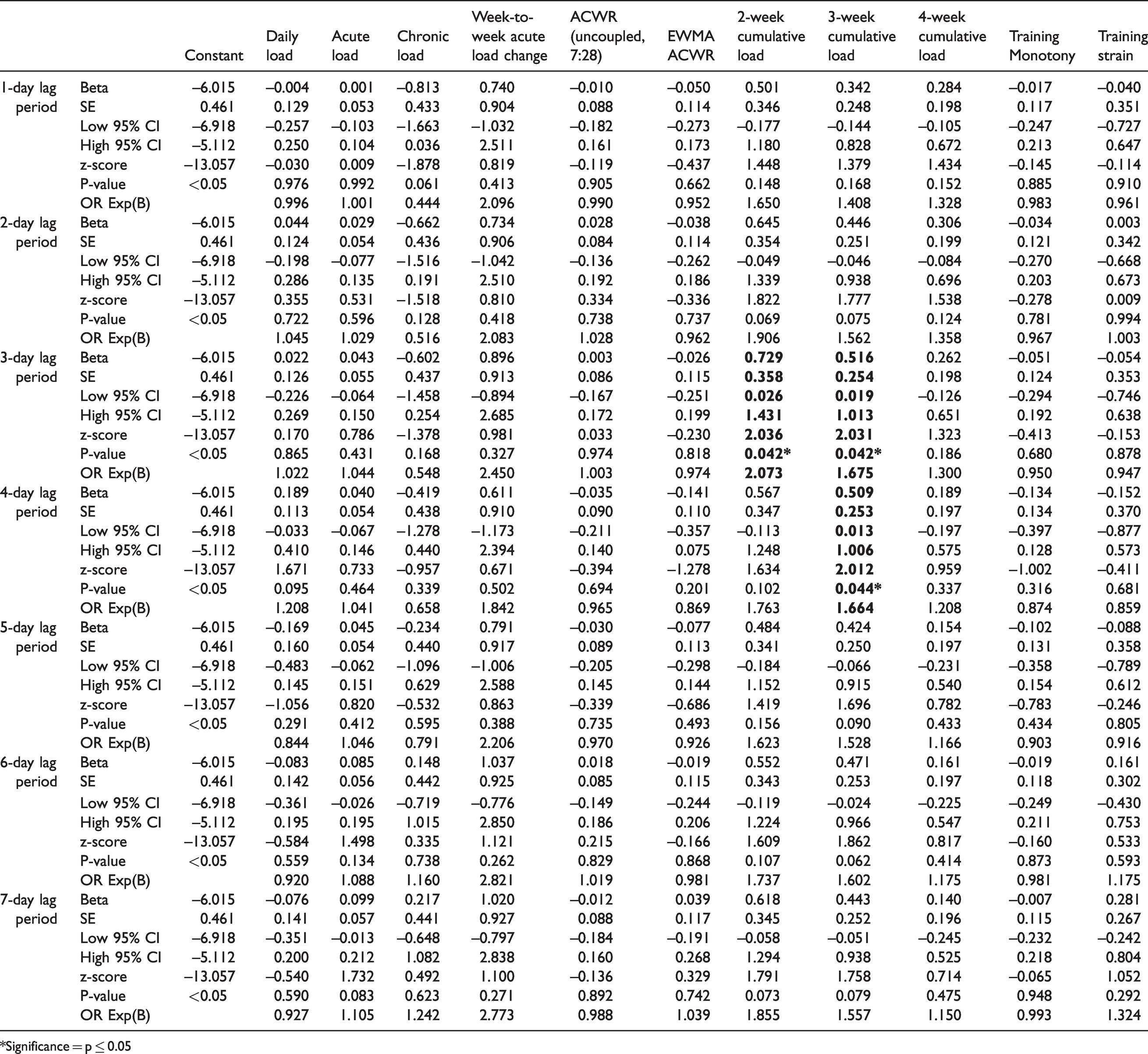
*Significance = p ≤ 0.05
There was a significant association found between 3-week cumulative load and an URTI, 4 days prior to the incidence of an URTI (OR = 1.66, 95% CI = 0.013–1.006; p = 0.044) (Table 4). Additionally, where 3-week cumulative load increased by 1-unit (1000 AU) over 4723 AU (e.g. 4723 to 5723), 4 days’ later a player was at a 51% higher risk of contracting an URTI.
No significant association was found between the remaining training load indices (acute, chronic, ACWR, EWMA ACWR, training monotony or strain) and URTIs across the daily lag periods (1 to 7 days) (Table 4).
Discussion
This is the first study of its kind to conduct longitudinal research investigating the association between a number of training load indices and URTIs, across daily lag periods in elite soccer players. The findings make an original contribution to the existing literature by providing coaches and practitioners with practically applied results that may indicate a player at a higher risk of contracting an URTI, as an URTI, may lead to performance decrements, missed training sessions or competitions. The results in the current study found that a player was at a higher risk of contracting an URTI (OR= 2.07) 3 days later with a high 2-week cumulative load (1-unit (1000 AU) over 3142 AU). Additionally, it was found that 3-week cumulative load (1-unit (1000 AU) over 4723 AU) also associated with an increased risk of a player contracting an URTI 4 days later (OR= 1.66). No other training load indices (acute, chronic, ACWR, EWMA ACWR, training monotony or strain) were found to associate with URTIs.
A novel finding of this study was that 2-week cumulative load, which was found to associate with an increased risk of an URTI 3 days later, had a higher OR (2.07) than 3-week cumulative load 4 days prior to an URTI (OR = 1.66). This has not been found in research studies to date. These findings indicate that a player was at a higher risk of contracting an URTI 3 days later if they had a high 2-week cumulative load, compared to a high 3-week cumulative load. Furthermore, a more detailed analysis found that 6 of the 10 reported URTIs had a 2-week cumulative load of >3500 AU. Despite the fact that 2-week cumulative load OR was higher than 3-week cumulative load, a significant association was still found between 3-week cumulative load and an increased risk of a player contracting an URTI (OR = 1.66, p = 0.044). Therefore this means 3-week cumulative load, therefore, can also be used by coaches to indicate if a player is at an increased risk of an URTI. The more detailed analysis found that 7 of the 10 reported URTIs had a 3-week cumulative load of >5193 AU. For a coach, these findings indicate that if 2-week cumulative load was >3500 AU, a player was at a greater risk of contracting an URTI, 3 days later. Additionally, if 3-week cumulative load was >5193 AU, a player was also at risk of contracting an URTI but 4 days later.
A review paper by Martin et al. 4 investigating ‘exercise and respiratory tract viral infections’ reported that prolonged periods of intense exercise increased the risk of an URTI. Novas et al. 14 found higher training loads resulted in higher incidences of URTIs. The current study found a high 2- and 3-week cumulative load, which may be interpreted as accumulated (prolonged) load, also associated with incidences of URTIs. These results could indicate that the accumulated training load may have resulted in cumulative fatigue, 26 due to a player having insufficient recovery, which can lead to an immune system compromise, 32 and possibly increasing the potential risk of an URTI. Interestingly, Moreira et al. 15 found that a decrease in training load (∼50%), after an intense period of training, was accompanied with reduced incidences of URTIs in futsal players over a 4-week period. These findings may have practical implications for coaches, who can monitor 2- and 3-week cumulative loads to ensure high training loads are not prolonged, and thereby reducing the risk of a player potentially contracting an URTI.
Contradictory to the current study, Piggott et al. 19 found that a > 10% increase in acute load and training monotony in AFL players, increased the risk of all types of illness. Putlur et al. 20 also found that a proceeding spike in training load, monotony or strain increased the risk of illness, in female soccer players. In contrast, Anderson et al. 17 found no relationship between training load and illness, in collegiate basketball players. However, each of these studies17,19,20 examined all illnesses combined (e.g. lower respiratory tract infection, gastrointestinal and URTI) and did not solely analyze URTIs, like the current study. This is a potentially important distinction, as previous research has found an association between training load and URTIs,14,15 which has been reported as the most common illness in soccer, and may have a negative impact on the players performance. 1 This underpinned the current study rationale.
The lack of association between the remaining training load indices and URTI in the current study compared to the previous research,14,15 may be due to the acute nature of data collection. Data were collected over acute periods (12 weeks), 14 or during acute intense periods of training (4 weeks), 15 while the current study collected and analyzed all training sessions and matches over a whole season (40 weeks). Interestingly, Tiernan et al. 18 found no association between acute or chronic training load and URTI in elite Rugby union players, during a pre-season training period (10 weeks). These findings support the current study’s results, where no association was found between the remaining training load indices (including acute and chronic load) and URTIs. However, training load data were analyzed in weekly blocks rather than rolling weekly training load data, and no lag periods were analyzed in these studies,14,15,18 meaning training load data may have been omitted. Additionally, different calculations for training load were used, 14 and a limited number of training load indices were collected (acute13,14 or acute and chronic). 18 This may also highlight why previous research found contrasting results. It should be noted, in the current study, that the illness and training load data were provided to the coaches. However, no interpretation or recommendations were provided by the principal researcher (CT). Previous research has found that appropriately planned training load, ensuring sufficient recovery, may reduce the incidences of URTIs. 15 However, further research is required to explore if incidences of URTI differ between coaches with access to all data (ability to appropriately adjust training load) compared to coaches with no access to data.
It should be noted that the number of players for the current study represented the full senior team (n = 15), who were with the club for the whole season. Additionally, there were a large number of data points per player (280 observations), over the 40-week period, which is a strength of this study. However, the low number of URTIs found in this cohort of players, means the results must be interpreted with care. It must also be highlighted that there are a number of factors that may influence the contraction of an URTI. These include exposures to different bacteria/pathogens, individual immune responses, 33 other sick teammates that train in close proximities, 30 and personal hygiene practices of players (e.g. washing hands, sharing water bottles). These other factors draw attention to the fact that training load cannot be solely used to reduce the risk of an URTI. Previous research has found that salivary Immunoglobulin A (sIgA) may be a predictor of URTI,18,34 which implies that a combination of training load monitoring (2- and 3-week cumulative load) and other markers (e.g. sIgA) may be used to reduce the risk of a player contracting an URTI. However, further research is required.
The data in this study represents a particular cohort of players from one team over a season, which may be another reason for the low number of URTIs. Further research is required over several seasons, to investigate the association between training load indices and URTIs. Additionally, sRPE represents one marker of internal training load. Future research could also explore external training load markers (e.g. GPS data), additional internal training load markers (e.g. heart rate), or the separation of physiological and biomechanical training load.35,36 Exploring additional training load markers may provide further insights into a player’s training load response and association with URTIs. Such research may also explore the severity of an URTI in association with training load data.
Practical applications
Two-week cumulative load was found to associate with an URTI at a higher OR (2.07) than 3-week cumulative load (OR = 1.66). This indicated a player with a high 2-week cumulative load (> 3500 AU) was at a greater risk of contracting an URTI 3 days later. However, a player was still at a high risk of contracting an URTI, 4 days later, with a high 3-week cumulative load (> 5193 AU). The remaining training load indices (acute, chronic, ACWR, EWMA ACWR, training monotony and strain) were found to have no significant association with an URTI. For a coach, these results imply that the appropriate prescription and management of training load (e.g. reduced training load), specifically 2- and 3-week cumulative load, may help reduce the risk of players developing an URTI. This is beneficial for players and coaches as an URTI may lead to performance decrements, missed training sessions or even competitions. It is important that coaches individually analyze player’s data, tailor training to the individual player requirements, thus ensuring that their load is appropriately planned and adjusted.
Footnotes
Acknowledgments
We thank the head coach, strength and conditioning coach and the players from the soccer team for their participation in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.