
Abstract
This study examined dose-response effects of the Badminton World Federation (BWF) Shuttle Time programme on fundamental movement skills (FMS) and perceived FMS competence in 6–9-year olds. Children (n = 158, 83 boys, 75 girls, Mean ± SD age = 7.6 ± .97) were randomly allocated into three conditions: Shuttle Time 2Xweek; Shuttle Time 1Xweek; 3) control (CON) group. The intervention groups undertook the BWF Shuttle Time programme over a 10-week period in place of both or one of their statutory Physical Education lessons. FMS was assessed from the Test of Gross Motor Development 2. Perceived competence was assessed via the Pictorial Scale of Perceived Movement Skill Competence. Assessments were undertaken pre, post and 10 weeks post intervention. For FMS, a significant time X group interaction (P = .001) was evident. There was no significant difference in FMS between groups at pre (P > .05). Post intervention there were significant differences in FMS between 2X week and 1XWeek (P = .007), 2Xweek and control (P = .0001) and 1X Week and control (P = .007). From post to 10-weeks post there were significant improvements in FMS (P = .001) for the 2X week group. A significant time X group interaction (P = .0001) also indicated that perceived competence increased significantly pre to post for 1Xweek and 2Xweek groups, but not CON groups and was maintained at 10 weeks post (all P = .001).
Introduction
Fundamental movement skills (FMS) are widely recognised as an important determinant of physical activity, weight status, self-efficacy and educational attainment in children.1,2 Over the preceding decade, there has been an increasing interest in the topic of FMS development, particularly as it relates to lifelong health, well-being, and academic achievement.3,4 Mastery of FMS is purported to be essential for the development of more specialised movement patterns enabling youth to participate in organised and non-organised physical activities.5,6 FMS are globally defined as locomotor (e.g., running, jumping), object control (e.g., throwing, catching), and stability (e.g., balancing and twisting) movement categories,5,6 and, importantly, are not naturally acquired during the process of maturation. 7 In order to develop proficiency in FMS, there is a need to implement developmentally appropriate activities, specifically, teaching and coaching activities (with constructive and performance related feedback), alongside sufficient opportunities to practice for children and youth made available. 3 Consequently, developing proficiency in a range of FMS, has become prominent in school Physical Education (PE) curricula worldwide,8–10 with evidence to suggest that FMS improvement may be dose related. 11
Despite this focus on FMS, multiple research studies, drawn from samples in the United Kingdom, Ireland and Australia, identify concerns that FMS competency among children is low, and that children are not mastering these FMS to their expected age-related developmental capability.12–17 For example, recently, Duncan et al. 12 reported, in a British sample, that no children in School Year 2 (age 6–7) mastered the four key skills (run, jump, throw, catch) identified by the National Curriculum for PE, with only 25% of children in Year 4 (age 8–9) mastering these skills. This is despite the National Curriculum suggesting mastery of skills as a key target of the National Curriculum for PE by the end of Year 2. Thus, in line with conclusions drawn from systematic reviews and meta-analyses,18,19 demonstrating that there are low levels of FMS globally, there is a real need to develop effective strategies for children to develop their FMS to provide a solid foundation for future participation in sport, exercise and physical activity, and, indeed, better discern the dose required to elicit optimal responses. Importantly, work by Stodden et al. 20 suggested there is a reciprocal relationship between FMS and physical activity which is mediated by perceived competence in FMS. In the Stodden et al. model 20 the mediating effect of perceived competence is purported to differ depending on developmental stage, with a bidirectional effect suggested to occur between perceived FMS and actual FMS in middle and late childhood but a unidirectional effect where perceived FMS influences actual FMS being evident during early childhood. 20 Data also suggest that perceived competence in FMS is related to actual FMS competence in children,21,22 and that developing a positive perception of one’s own competence may lead to a positive trajectory of development where children with higher perceptions of their own competence are more likely to engage in physical activity and sport, which in turn facilitates development of actual FMS. 22 It would therefore seem pragmatic to examine the influence of such interventions on actual and perceived FMS competence simultaneously.
One intervention, which has recently shown promise in improving FMS, is the Badminton World Federation (BWF) Shuttle Time programme. 23 The BWF Shuttle Time programme was introduced in 2012 to provide an effective means to develop FMS and badminton related skills, in community coaching and school settings for children aged 5–15 years. Given the multi-dimensional movement demands inherent in badminton, 24 effective development of FMS is a key foundation for later performance in the sport, as well as other racquet sports. Implicit within the activities included in the programme, are the embedding and development of FMS that, although badminton related, are suggested to apply to a range of sports and physical activities. 23 Recently, the efficacy of Shuttle Time in children aged 6–7 and 10–11 years was demonstrated. 25 In Duncan et al. 25 children undertook a once weekly Shuttle Time lesson, in lieu of statutory PE for a 6-week period, with the authors reporting significant short-term improvements in FMS for 10–11 year olds and 6–7 year olds. However, once Shuttle Time had finished, FMS scores began to regress, but in 10–11 year olds only. This prompted Duncan et al. 25 to conclude that the Shuttle Time programme is particularly beneficial in developing FMS and motor fitness for children who have not yet matured their FMS, further asserting the need to discern whether there is a dose-response in relation to FMS and motor fitness. 25 There are other good examples of FMS focused interventions, targeting similar groups and over similar durations which have shown promise in enhancing children’s movement skills and other variables such as physical activity and fitness.26–27 However, few studies to date have examined the dose-response effects of motor competence interventions in children. Only one study to date by Robinson et al. 28 appears to have examined this issue. They reported improvements in motor performance were evident, irrespective of specific dose, potentially representing a ceiling effect on the development of FMS. 26 The current study sought to advance the understanding of the efficacy of BWF Shuttle Time, by examining the dose-response effect of the BWF Shuttle Time Programme on FMS and perceived FMS competence in 6–9 year olds.
Methods
Design
This study employed a repeated-measures, cluster randomized intervention design, where six classes from three schools in central England were allocated into three conditions: 1) Shuttle Time intervention 2Xweek; 2) Shuttle Time intervention 1Xweek; 3) control (CON) group. Randomization occurred at the class level using research randomisation software (REF29). The pedagogic approach of the intervention, although not explicitly stated in the guidance for administration, is primarily based on directed learning with specific cues being provided by teachers to facilitate movement. Full details of the programme are available in the BWF Shuttle Time programme manual. 23 The intervention was administered by movement trained professionals. The schools involved were comparable in terms of ethnic makeup and were all within the mid-range of socio-economic status for the county in which they were located. The children were drawn from School Year 2 (ages 6–7) and School Year 4 (ages 8–9). This was based on the prior work of Duncan et al., 25 which demonstrated that Shuttle Time was more effective in children from Year 2 but did not influence FMS scores for Year 6 children and work by Bryant et al. 14 demonstrating that FMS interventions are effective for children in Year 4. We therefore took a pragmatic decision to examine Year 2 and Year 4 children The Shuttle Time groups undertook a structured Shuttle Time programme over a 10-week period in place of either both (2Xweek group) or one (1Xweek group) of their statutory PE sessions. Sessions lasted approximately 60 minutes in duration. Recognising the constraints on curriculum PE time we assessed time on task during each of the Shuttle Time sessions to provide an indication of how much of each 60 minute time slot was actually spent on the Shuttle Time activity, thus excluding time spent moving form class to school hall, etc. The Shuttle Time 1Xweek group undertook one lesson of Shuttle Time and one of their statutory PE sessions per week. The CON group attended their two statutory PE sessions per week. The PE activities engaged in during the statutory PE sessions were the same for the 1XWeek and the CON group in terms of focus and consisted of cricket, a sport also requiring object control skills. These sessions were designed by the authors and the school Physical Education teachers. The decision to employ statutory PE sessions was conceptualised as a form ‘usual care’ enabling comparison of the intervention, as administered, to the usual PE sessions experienced by the children. Prior to, immediately following and 10 weeks post the intervention, participants in both groups were assessed on measures of FMS and perceived FMS competence.
Participants
One hundred and fifty-eight children, aged 6–9 years (83 boys, 75 girls; Mean ± SD = 7.6 ± .97 years), participated in this study following protocol approval from institutional ethics committee, written informed parental consent and child assent. Participants were drawn from three classes in school Year 2 (n = 72, ages 6–7), and from two classes in school Year 4 (n = 86, ages 8–9). From school records, ethnic classifications of these participants were: 95% ‘Caucasian;’ 2% ‘South Asian’; 3% ‘Black’. The schools were selected using convenience sampling; they were located in areas ranked as 40–60% least deprived within England as a whole, using the Index of Multiple Deprivation. 30 A priori power analysis using GPower 31 indicated for repeated measures ANOVA to detect a medium effect size, at P = .05 and 80% power a total sample size of 128 participants was needed.
Measures
Anthropometry
Height (cm) and body mass (kg) were assessed with children barefoot wearing PE kit using a SECA stadiometer and weighing scales (SECA Instruments, Hamburg, Germany).
FMS
Process measurements of FMS were used in the present study to provide information relating to how the skill is performed. 32 Four tasks (2 locomotor, 2 object control) were employed to assess FMS using the Test of Gross Motor Development-2 (TGMD-2). 33 The following skills from the TGMD-2 were assessed: run, jump, catch, throw. These skills were selected as they are the key skills identified as targets for development by the UK National Curriculum for PE for children of the age participating. 9 Each skill comprises 3–4 components and the TGMD-2 assess whether each component of each skill was performed or not performed to determine the mastery of the skill. All skills were video-recorded (Sony video camera, Sony, UK) and subsequently edited into single film clips of individual skills on a computer using Quintic Biomechanics analysis software v21 (Quintic Consultancy Ltd., UK). The skills were then analysed using this software and a process-oriented checklist, enabling the videos to be slowed down, magnified, replayed and scored. Assessors were blinded to group allocation. Scores from two trials were summed to obtain a raw score for each skill. The scores for all the skills were then summed to create a total motor competence (scored 0–30) score. Scores from the run and jump were summed to create a locomotor competence score (0–16) and the catch and throw, summed to create an object control score (0–14) following recommended guidelines of administration of the TGMD-2. 33 Two researchers experienced in the assessment of children’s movement skills (having previously assessed movement skills in the context of a previous research study) analysed the motor competence videos. Both raters had been previously trained in two, separate sessions, lasting approx. 120 min, by watching videoed skills of children’s skill performances and rating these against a previously rated ‘gold standard’ rating. Congruent with prior research, 34 training was considered complete when each observer’s scores for the two trials differed by no more than one unit from the instructor score for each skill (>80% agreement). Inter- and intra-rater reliability analysis was performed for all the motor skills between the two researchers. Intraclass correlation coefficients for inter and intra-rater reliability were .92 (95% CI = .87–.95) and .98 (95% CI = .94–.98) respectively, demonstrating good reliability. 35
Perceived FMS competence
To assess perception of their own competence in FMS, children completed the Pictorial Scale of Perceived Movement Skill Competence (PMSC),
36
in the same four skills as measured by the TGMD-2. The PMSC has been described extensively elsewhere, and prior research showed it to have good validity and reliability for this purpose.
36
For each skill, children were shown two, sex-specific illustrations of a child performing the skill competently and less competently and were then asked, “This child is pretty good at: (insert skill, e.g., throwing), this child is not that good at: (insert skill, e.g., throwing); which child is most like you?” from the selected picture, children were asked to further indicate their perceived competence by endorsing more specific descriptions with either competent or less competent picture, including, for the competent picture – 4: Really good at … or 3: Pretty good at, etc. – and, for the not so competent picture – 2: Sort of good at … or 1: Not that good at. The PMSC was administered to children on an individual basis by trained researchers. Possible scores for the entire scale ranged from 4–16. Two week test-retest reliability data, available in a subsample of children (n = 43; 22 boys, 21 girls; mean age = 5.6, SD = .48 years), indicated good agreement (Intraclass correlation coefficient = .86, CI = .74–.92) and internal consistency (Cronbach’s
Shuttle time intervention
The present study employed a 10-week version of the BWF Shuttle Time programme. 23 No specific optimum duration of the Shuttle Time programme is specified by the BWF and a 10-week trial period was chosen as, pragmatically, it fits within a school term, therein making it attractive for teachers for potential roll out in multiple schools. This decision was taken in order to confer minimal disturbance on the school curriculum, to be time efficient, to create a design that could be realistically integrated into the school curriculum. Prior research studies that have focused on Shuttle Time have used a six-week intervention period with success, 25 but also demonstrated a lack of retention at six weeks follow up. The Shuttle Time programme was progressive, based on the exercises and activities specified by the BWF and consisted of a warm-up section (10 mins) and a main body section (approx. 40mins). The full programme that was administered including timings of each activity, feedback given, key teaching and differention points is provided in the supplementary material. The Shuttle Time 2Xweek group undertook two identical lessons of Shuttle Time each week, the Shuttle Time 1Xweek groups also undertook a second weekly PE lesson during the intervention period, as part of statutory PE, which was focused on cricket/basketball. The rationale for repeating sessions was to ensure that the content of sessions undertaken by the 2Xweek group was the same as that undertaken by the 1Xweek group. The CON group continued their twice-weekly statutory PE lessons with one weekly session focused on cricket and the other on Basketball. The duration of the CON groups PE session was the same as that undertaken by both Shuttle Time groups. In this way we tried to match the lessons the children undertook so the control group’s statutory PE sessions comprised an object control stimulus in lieu of the Shuttle Time intervention. There was no difference in the delivery and content of the statutory PE lessons for Shuttle Time 1XWeek and CON groups. The PE sessions followed the same format as the Shuttle Time sessions in terms of time allocation and warm-up/main-body and were designed in collaboration between the school PE teachers and the researchers.
The principal investigators delivered all the intervention sessions with the assistance of a primary school teacher. Those delivering had prior extensive experience in delivering motor competence interventions in schools and community settings and were qualified in PE and exercise science. The other PE session for the Shuttle Time group and PE sessions for the CON group were delivered by the class teacher and in accordance with guidelines for the National Curriculum for PE in England. The principal investigator documented adherence to the programme during the 10-week period. Any child who missed more than one session in the intervention period was not included in final analysis. This resulted in four exclusions from the final data set for analysis, one boy from the CON group, two girls from the Shuttle Time 2Xweek group and one boy from the Shuttle Time 1Xweek group due to the children being ill and away from school during the intervention period. In all these cases the children who were excluded missed four or more sessions of the intervention, and while an intention to treat protocol would have included all participants who undertook baseline assessment, by including children who did not receive the full ‘dose’ of intervention in the final sample for analysis, we would have been unable to fully estimate dose-response effects, as was the aim of the study.
The content and schedule of the Shuttle Time programme the children engaged in is presented in the supplementary material. Similar to other research using this approach with children,14,37,38 participants in the intervention groups also received skill-specific feedback on the quality of each movement during intervention sessions. Time on task analysis was undertaken to assess the amount of time children engaged in each session, recognising that there will be variation in the time spent engaged in activities during any intervention. This process was undertaken as an indicator of intervention fidelity 39 and was completed by those administering the intervention sessions using a self-administered checklist after each session recording how much of each session was spent engaged in movement activities. 40 The projected time on task was 500 minutes for the Shuttle Time 1Xweek group and 1000 minutes for the Shuttle Time 2Xweek group. However, actual time on task was 450 minutes for the Shuttle Time 1Xweek group and 944 minutes for the Shuttle Time 2Xweek group. This discrepancy was largely due to delays in children attending their PE lessons or being required to finish early (on one occasion) due to another school commitment.
Statistical analysis
A series of repeated measures ANOVAs were used to examine any changes in dependant variables; FMS and perceived FMS, assessed pre, post and 10 weeks post the intervention period. Group (Shuttle Time 1XWeek vs Shuttle Time 2XWeek vs CON) and sex were used as between subjects variables. In this way we sought to assess any short term (pre-post) and sustained (post-10 weeks post) changes in dependant variables between intervention and control groups and between boys and girls. Where any differences were found Bonferroni post-hoc analysis was undertaken to determine where differences lay. Partial η 2 was used as a measure of effect size and alpha level was set as P = .05 to indicate statistical significance. The Statistical Package for Social Sciences (SPSS version 24) was used for all analysis.
Results
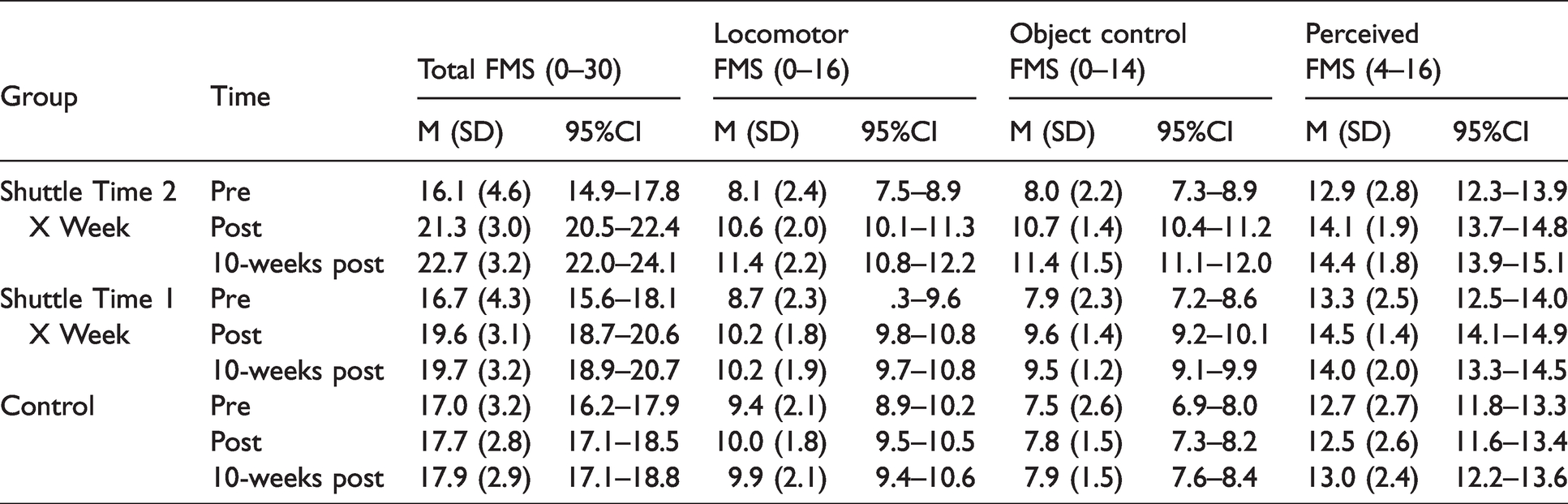
At baseline there were no significant differences in FMS and perceived FMS (all P > .05) between the Shuttle Time 2Xweek, Shuttle Time 1Xweek and control groups. Mean ± SD of all outcome variables pre, post and 10 weeks post for children in Shuttle Time 2Xweek, 1Xweek and control groups are presented in Table 1.
Mean ± SD of all FMS and perceived FMS variables pre, post and 10 weeks post intervention for Shuttle Time 2Xweek, Shuttle Time 1Xweek and control groups.
FMS
When data for total FMS scores were considered results revealed a time X group interaction (P = .001, Pη2 = .404, see Figure 1). There was also a significant main effect for gender (P = .001, Pη 2 = .085). Bonferroni post-hoc analysis indicated that there was no significant difference in total FMS in Shuttle Time 2Xweek, Shuttle Time 1Xweek and control groups at pre (all P > .05). Post intervention there were significant differences between Shuttle Time 2Xweek and Shuttle Time 1Xweek (P = .007), Shuttle Time 2Xweek and control (P = .0001) and Shuttle Time 1Xweek and control (P = .007). The greatest magnitude of change pre to post was observed for the Shuttle Time 2Xweek group (Δ = 5.2), compared to the Shuttle Time 1Xweek group (Δ = 2.9) and control groups (Δ = 0.6). Total FMS scores at 10 weeks post intervention mirrored those at post with significant differences between Shuttle Time 2Xweek and Shuttle Time 1Xweek (P = .0001), Shuttle Time 2Xweek and control (P = .0001) and Shuttle Time 1Xweek and control (P = .008). From pre, to post to 10-weeks post there were significant improvements in total FMS (all P = .001) for the Shuttle Time X2week group. However, there were significant increases in total FMS pre to post for the Shuttle Time 1Xweek group and control groups (all P<.05) at which point total FMS scored plateaued with no significant differences from post to 10-weeks post (all P > .05) the Shuttle Time 1Xweek group and control groups. Concerning the main effect due to gender, irrespective of intervention group, boys also had significantly higher total FMS scores than girls. Mean ± SE of total FMS was 19.7 ± .34 for boys and 17.8 ± .37 for girls.
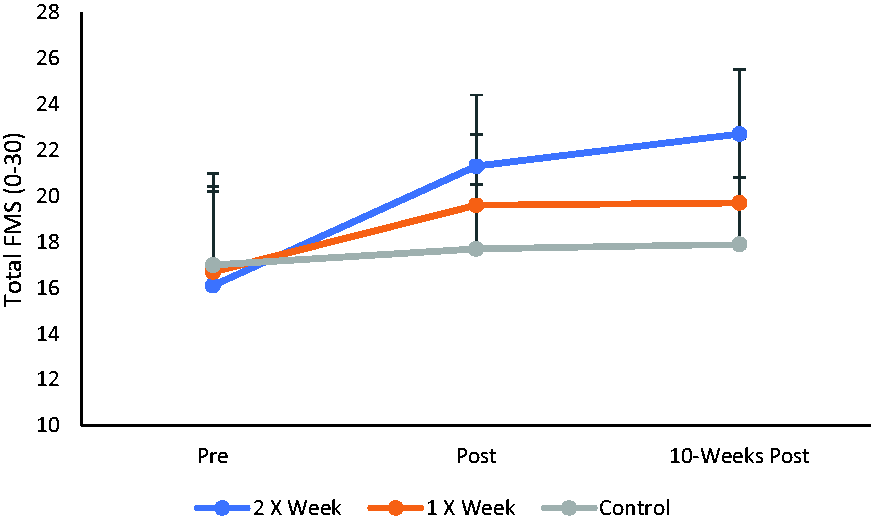
Mean ± SD of total FMS for children in Shuttle Time 2Xweek, Shuttle Time 1Xweek and control groups.
FMS data were subsequently reanalysed split into locomotor FMS and object control FMS subsets. For this analysis there were also significant group X time interactions for locomotor FMS (P = .001, Pη 2 = .315, see Figure 2) and object control FMS (P = .001, Pη 2 = .322, see Figure 3). Bonferroni post-hoc analysis revealed patterns identical in nature to those described for total FMS where both locomotor and object control FMS significantly increased for all groups pre to post but locomotor and object control FMS significantly improved only for the Shuttle Time 2Xweek group.
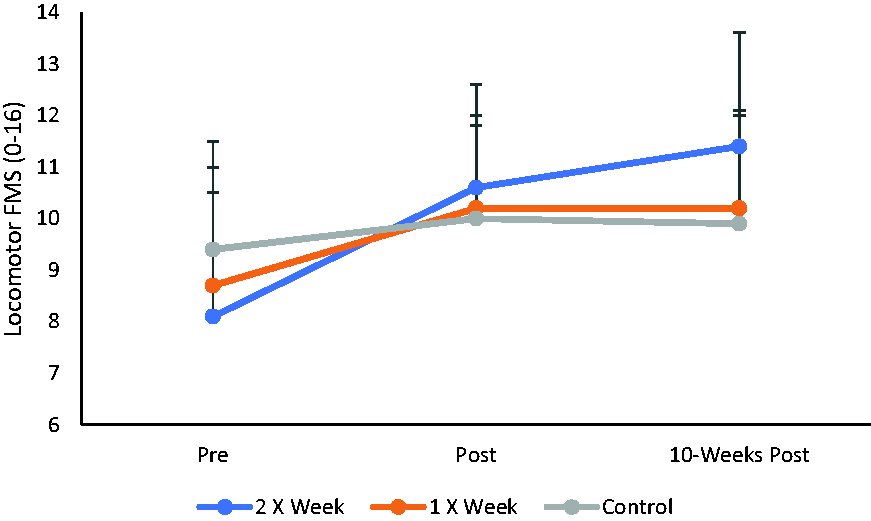
Mean ± SD of locomotor FMS for children in Shuttle Time 2Xweek, Shuttle Time 1Xweek and control groups.
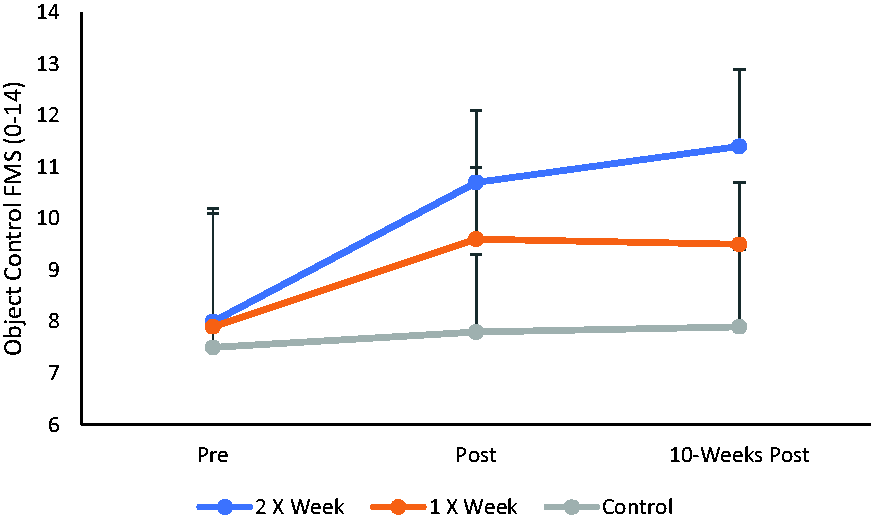
Mean ± SD of object control FMS for children in Shuttle Time 2Xweek, Shuttle Time 1Xweek and control groups.
Perceived FMS
For perceived FMS results indicated no higher order interactions or main effects due to age stage (all P > .05). There was a significant time X group interaction (P = .0001, Pη 2 = .119, see Figure 4) and a significant time X gender interaction (P = .001, Pη 2 = .096, see Figure 5). For the time X group interaction, Bonferroni post-hoc pairwise comparisons indicated no significant differences in perceived FMS pre-post to 10-weeks post for the control group (P > .05). For the Shuttle Time 2Xweek group there was a significant increase in perceived FMS pre to post (P = .001) but no difference post to 10 weeks post (P > .05). This pattern was mirrored for the Shuttle Time 1Xweek group with a significant increase pre to post (P = .001) but not post to 10 weeks post (P > .05). At pre there was no difference between groups (P > .05) but perceived FMS was significantly higher for the Shuttle Time 1Xweek and Shuttle Time 2XWeek groups compared to the control group at post (both P = .001) and 10 weeks post (both P = .01).
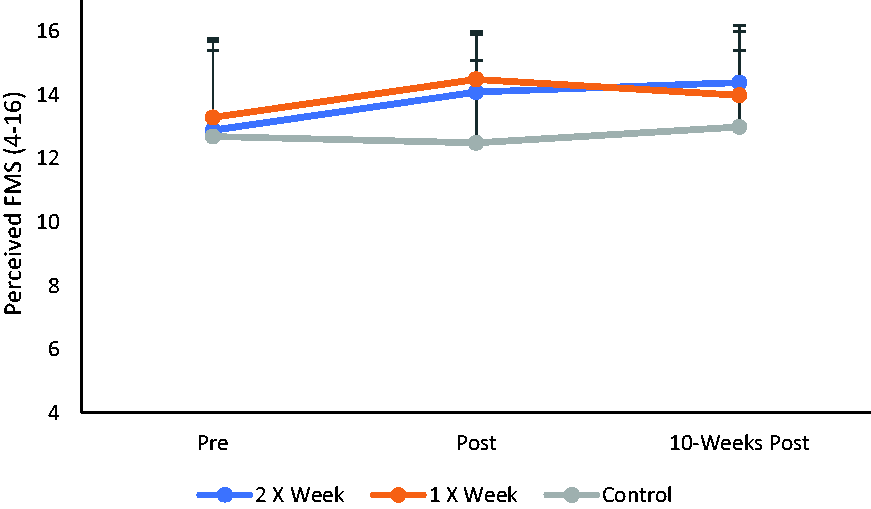
Mean ± SD of perceived FMS for children in Shuttle Time 2Xweek, Shuttle Time 1Xweek and control groups.
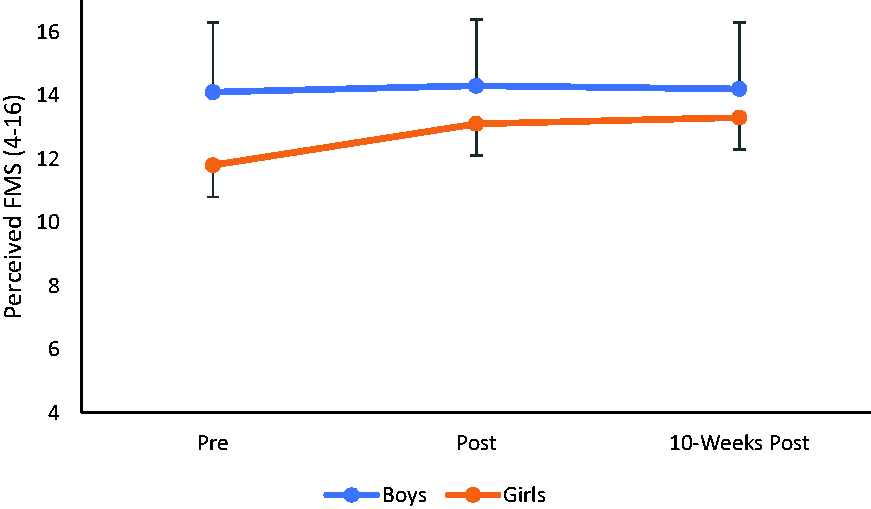
Mean ± SD of perceived FMS across time for the boys and girls.
For the significant time X gender interaction, Bonferroni post-hoc pairwise comparisons indicated that there was no significant difference in perceived FMS pre to post and to 10-weeks post for boys (all P > .05) whereas for girls, perceived FMS significantly increased pre to post (P = .0001) and then plateaued with no difference in girls’ perceived FMS from post to 10 weeks post (P = .395). Irrespective of time point, perceived FMS was significantly higher in boys compared to girls (all P<.01).
Discussion
The results of the present study are the first to demonstrate a dose response effect for the BWF Shuttle Time programme. Although prior research has demonstrated the efficacy of other motor competence-based interventions on FMS and motor fitness, 19 only one study to date has examined the possibility of dose response effects in motor competence intervention, but reported improvements were manifest, irrespective of dose, potentially representing a ceiling effect in the development of FMS from the Children’s Health Activity Motor Program. 28 The results of the current study suggest otherwise in our sample of 6-9 year olds. Unlike the present study, Robinson et al. 28 investigated the dose-response in pre-school children, which may be a viable reason for no added benefits being observed for increased dose in their study. 28
Irrespective of dose, the results presented here suggest that the BWF Shuttle Time programme has a positive short term (pre-post) and sustained (post-10-weeks post) effect on children’s FMS and perceived FMS. However, for process FMS measures (ie the quality of movement), there was a greater benefit to undertaking Shuttle Time 2Xweek in comparison to 1Xweek. This was evident for total FMS scores, as well as for locomotor and object control subsets, at post intervention assessment. Importantly, at post 10 weeks, FMS scores for the 2Xweek group continued to improve beyond those scores achieved at post assessment. This trend was not seen for the 1Xweek group where improvements in FMS were sustained, but plateaued at the 10-weeks post assessment.
Given the findings of the current study it is important to consider why the Shuttle Time programme improved FMS in a dose response manner, and in a manner that was superior to statutory PE. The Shuttle Time programme consists of a framework deliberately designed to facilitate development of FMS, whereas statutory PE typically focuses more on sports skill development. Likewise, in the present study Shuttle Time sessions were delivered by movement trained professionals and statutory PE was delivered by school PE teachers. This was deliberate in order to compare Shuttle Time to what could be considered ‘usual care’. However, it is important to acknowledge that the results of the present study reflect the effect of Shuttle Time delivered 1XWeek vs 2XWeek by specifically trained personnel to a usual care condition delivered by teachers, who were not trained in movement skills to the same extent. A key next step, now that efficacy of Shuttle Time has been established, would be to replicate the programme with teachers administering the programme alongside a full process evaluation including video of teaching sessions, rather than relying on self-report alone.
The current results also align with the positive response to Shuttle Time over a 6-week period documented by Duncan et al, 25 but highlight that twice weekly Shuttle Time may be preferable to elicit more robust benefits compared to undertaking the programme once per week. Such an assertion is congruent with theories of motor development in children4–6 that time is needed to master FMS and that FMS are not naturally acquired but instead need to be developed through teaching with appropriate feedback. In the present study a 10-week intervention period was employed. In comparison to the Duncan et al. 25 study where a six week intervention was employed, participants in the current study would have engaged in a greater volume of Shuttle Time activity, irrespective of whether they undertook activities once or twice per week. This may have enabled more secure embedding of FMS patterns in the participants in the current study than in that of Duncan et al. 25 This is however speculative and additional research would be needed to examine how duration of intervention might impact acquisition and retention of FMS. Prior systematic reviews and meta-analysis examining efficacy of FMS intervention18,19 were unable to draw conclusions relating to this issue, which another, focusing on pre-schoolers, 11 concluded that interventions lasting less than six months in duration produced larger effects than those lasting six months or longer. Likewise, Duncan et al. 25 examined children aged 6–7 years and 10–11 years, suggesting that Shuttle Time was more effective for the younger age group. In the present study we found similar positive gains in FMS for children in School Year 2 (aged 6–7 years) and School Year 4 (aged 8-9 years).
Furthermore, irrespective of whether Shuttle Time was undertaken 1Xweek or 2Xweek, perceived competence in FMS significantly increased compared to the control group. Perceived competence in FMS is a key mediator in the association between FMS and physical activity according to the Stodden model, 20 whilst perception of FMS is a key correlate of actual FMS in children 21 and is positively associated with physical activity in both children and adolescents. 22 The fact that perceived competence in FMS increased due to undertaking the Shuttle Time programme should be considered a positive impact, given the role of perceived competence in future physical activity and overall self-concept. 21 In this respect, the BWF Shuttle Time programme appears to have a positive psychological impact on children that undertook it. This is important because programmes that enhance perceived competence may lead to a pathway to being habitually physical activity and for children to engage in sport participation. Those children who perceive themselves to be more competent in FMS, may be more likely to engage in opportunities to practice their movement skills through sport and physical activity leading to a reinforcing loop where perceived FMS competence feeds actual FMS through participation in sport, which then reinforces child’s perceptions of their competence in a positive manner.20,22,41
A key tenet of the Shuttle Time programme is the development of competence in FMS that are developed through badminton, but are applicable to a range of different sports. 23 The results of the present study support the assertion that Shuttle Time enhances FMS, and is superior to statutory PE and that improvements are enhanced when Shuttle Time is undertaken 2Xweek.
Although the present study represents a novel addition to the literature, there are some limitations that must be considered. We conceptualised ‘dose’ in terms of the number of sessions undertaken by participants in the 10-week intervention period. Thus ‘dose’ was modified by increasing the frequency of Shuttle Time sessions. This was pragmatic given the demands a crowded school curriculum. However, there are other ways to modify the dose of activity undertaken, for example by changing the volume of activity undertaken in a given session. Understanding how frequency, volume and intensity of FMS intervention sessions might be best manipulated to positively influence FMS and other health related variables would be a useful next step in producing guidance on intervention design. In addition, future studies which examine if the positive changes in FMS resulting from participation in Shuttle Time also result in changes in habitual physical activity would be pragmatic. The Stodden et al. 20 conceptual model suggests this may be the case, but undertaking such a study would be practically and logistically challenging and concluding any changes in habitual physical activity were attributable to Shuttle Time alone would be difficult to ascertain. Similarly, the results of the current study are representative of children aged 6-9 years old and different responses may be seen in older children and adolescents. It is also important to highlight that only run, jump, throw and catch were assessed in terms of FMS. While these skills are identified as those children need to master within the English school curriculum, FMS comprise more than the skills assessed in the current study including skills such as the strike and the hoop, which may have relevance for any intervention focused on racquet sports. Future research should therefore seek to assess a wider range of FMS than those examined in the current study. Furthermore, the present study was not conducted to discern individual responses to intervention, under or over-estimators, or realists, 41 and this would, therefore, represent a sensible avenue for future research. Further investigation with larger samples and taught by classrooms teachers is a key next step in order to provide real world evidence for a scalable and sustainable movement intervention programme.
The principal finding from the current project is that: the BWF Shuttle Time programme is beneficial in developing FMS and perceived competence in FMS for children aged 6-9 years. A frequency of Shuttle Time 1xweek will produce positive changes in the aforementioned variables, but greater, and more sustained, improvements in process FMS (i.e. quality of movement) are seen when Shuttle Time is undertaken 2xweek over a 10-week period.
Supplemental Material
sj-pdf-1-spo-10.1177_17479541211007886 - Supplemental material for Dose response effects of the BWF Shuttle Time Programme on children’s actual and perceived fundamental movement skill competence
Supplemental material, sj-pdf-1-spo-10.1177_17479541211007886 for Dose response effects of the BWF Shuttle Time Programme on children’s actual and perceived fundamental movement skill competence by Michael J Duncan, Mark Noon, Cain CT Clark and Emma LJ Eyre in International Journal of Sports Science & Coaching
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded in part by a research grant from the Badminton World Federation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.