
Abstract
Background:
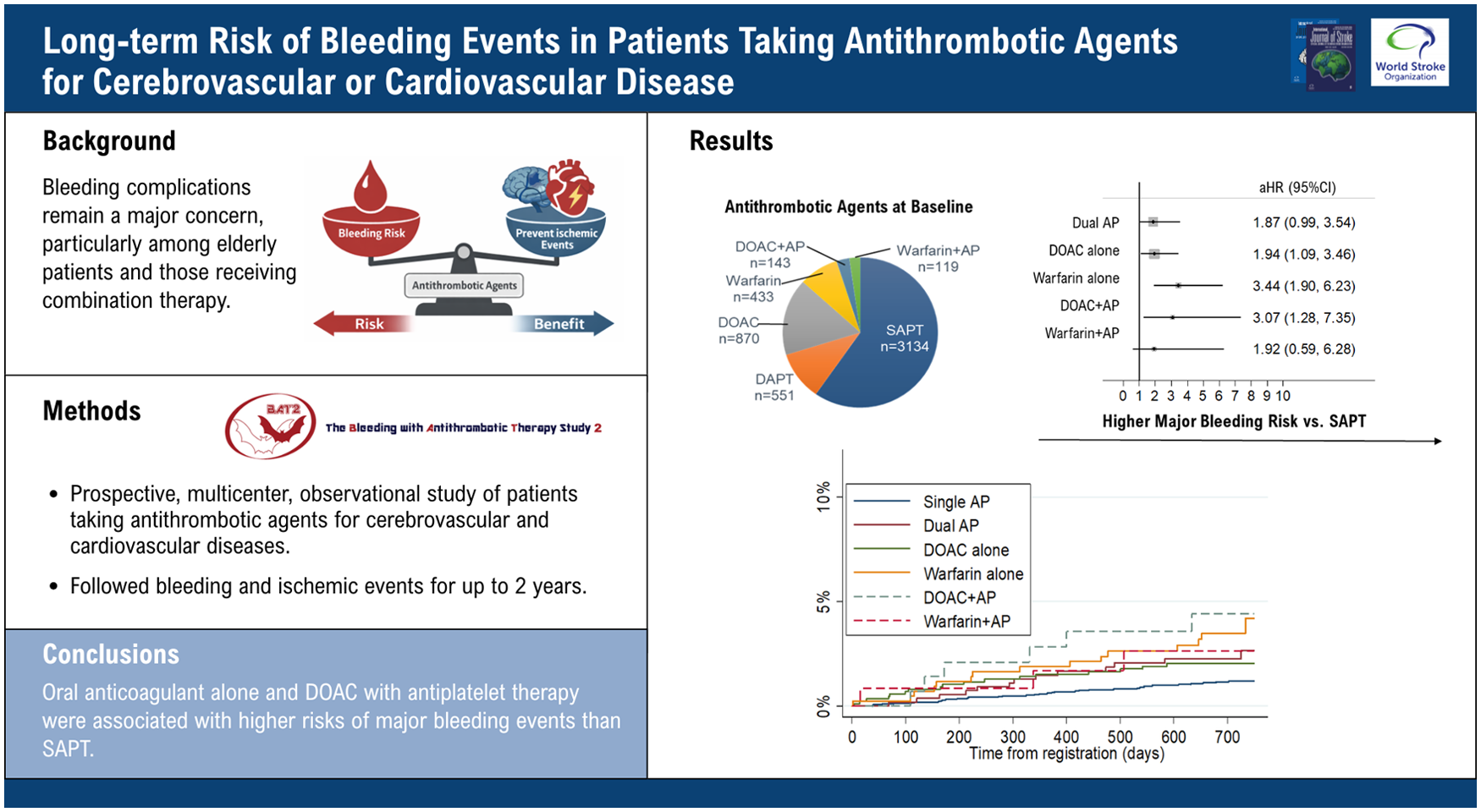
Antithrombotic agents are essential for preventing cerebrovascular and cardiovascular diseases; however, bleeding complications remain a major concern, particularly among elderly patients and those receiving combination therapy.
Aims:
We designed the Bleeding with Antithrombotic Therapy 2 (BAT2) Study, a prospective multicenter registry involving hospitals from a clinical research network in Japan, to clarify the risk of bleeding events in patients taking antithrombotic agents for cerebrovascular and cardiovascular diseases in recent clinical settings.
Methods:
This prospective, multicenter, observational study followed bleeding and ischemic events for up to 2 years in patients with cerebrovascular and cardiovascular diseases. The primary outcome was major bleeding, and secondary outcomes included intracranial hemorrhage (ICH).
Results:
The 5250 patients enrolled comprised 3134 (70 ± 11 years; male, 66.6%; HASBLED ⩾ 3, 32.8%) treated with single antiplatelet therapy (SAPT), 551 (71 ± 11 years; 25.8%; 40.8%, respectively) with dual antiplatelet therapy (DAPT), 870 (75 ± 10 years; 37.1%; 39.8%, respectively) with direct oral anticoagulant (DOAC) alone, 433 (72 ± 12 years; 34.2%; 41.4%, respectively) with warfarin alone, 143 (76 ± 8 years; 16.8%; 42.7%, respectively) with DOAC plus antiplatelet agents (AP), and 119 (73 ± 12 years; 18.5%; 47.5%, respectively) with warfarin plus AP. During follow-up (median, 1.98 years), 93 patients experienced major bleeding, and 55 developed ICH. Compared with the SAPT group (37 events, 0.63%/year), the DOAC (18 events, 1.12%/year; adjusted hazard ratio (aHR) = 1.94, 95% confidence interval (CI) = 1.09–3.46), warfarin (16 events, 2.02%/year; 3.44, 1.90–6.23), and DOAC plus AP groups (six events, 2.24%/year; 3.07, 1.28–7.35) exhibited significantly higher risks of major bleeding after multivariable adjustment. DAPT (aHR 2.47, 95% CI = 1.11–5.48), warfarin (5.38, 2.65–10.92), and DOAC plus AP (3.86, 1.30–11.47) had significantly higher risks of ICH than SAPT. The DAPT (2.28, 95% CI = 1.65–3.14), DOAC plus AP (1.96, 1.08–3.56), and warfarin plus AP (2.83, 1.62–4.92) groups showed significantly higher risks of ischemic events than the SAPT group.
Conclusion:
Oral anticoagulant alone and DOAC with antiplatelet therapy were associated with higher risks of major bleeding events than SAPT in long-term follow-up for patients with stroke and cardiovascular disease.
Get full access to this article
View all access options for this article.