
Abstract
Background:
Although endovascular therapy (EVT) improves functional outcomes in acute ischemic stroke patients, some with large hemispheric infarction (LHI) post-EVT may still require decompressive hemicraniectomy (DHC). This study aimed to explore whether DHC benefits all patients with post-EVT LHI and to identify which patients are more likely to benefit from DHC.
Methods:
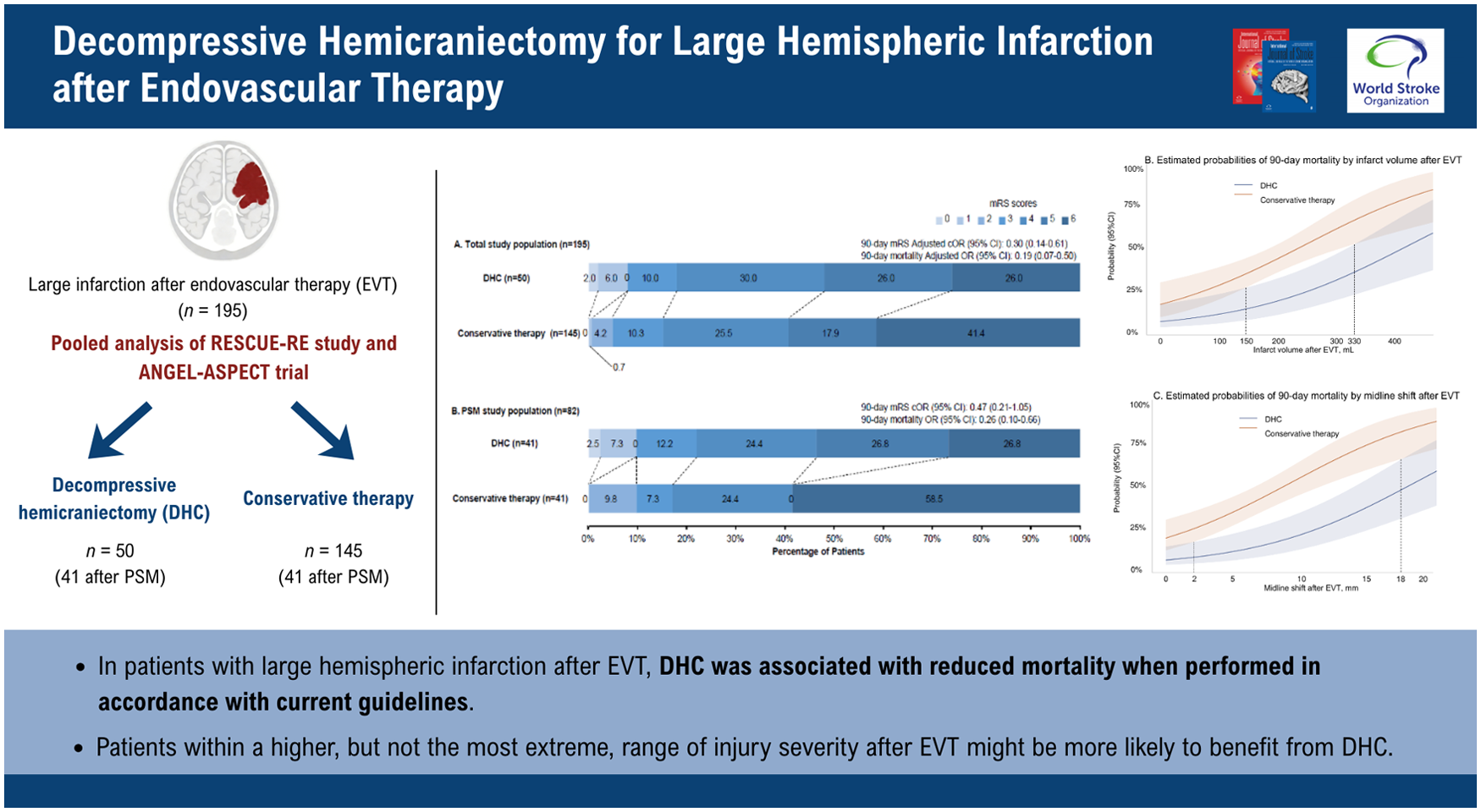
This pooled analysis of the RESCUE-RE study and the ANGEL-ASPECT trial enrolled patients with LHI and severe neurological deficits after EVT. According to the treatment received, patients were categorized into DHC and conservative therapy groups. The primary outcome was 90-day mortality. Propensity score matching (PSM) analysis was used to control for differences between groups.
Results:
In total, 136 of 2036 EVT-treated patients (6.7%) in the RESCUE-RE study and 59 of 230 (25.6%) in the ANGEL-ASPECT trial met inclusion criteria. Among the 195 patients included, 50 (25.6%) underwent DHC (41 after PSM), while 145 (74.4%) received conservative therapy (41 after PSM). Patients undergoing DHC after EVT had significantly lower 90-day mortality rates compared with those receiving conservative therapy (odds ratio (OR) = 0.26; 95% confidence interval (CI), 0.10–0.66; p = 0.005), but no significant improvement was observed in 90-day modified Rankin Scale (mRS) distribution (common OR = 0.47; 95% CI = 0.21–1.05; p = 0.06). Patients within an overlapping range of post-EVT midline shift (approximately 10–17 mm) or infarct volume (approximately 250–330 mL), where both 90-day mortality and ordinal mRS distribution models favored DHC, appeared more likely to derive a comprehensive clinical benefit. Baseline infarct-core volume was not associated with the treatment effect of DHC.
Conclusion:
In patients with LHI after EVT, DHC was associated with reduced mortality when performed in accordance with current guidelines. Moreover, patients within a higher, but not the most extreme, range of injury severity after EVT might be more likely to benefit from DHC.
Get full access to this article
View all access options for this article.