
Abstract
Background:
For neurodegenerative diseases, the inter-individual variability in the functional response to pathology is explained by the construct of cognitive reserve (CR). We aimed to evaluate the association of CR with stroke outcome to improve the understanding of its inter-individual variability and prediction.
Methods:
The peer-reviewed protocol was preregistered on PROSPERO (CRD42021256175). The systematic review and meta-analysis followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), Meta-analysis of Observational Studies in Epidemiology (MOOSE), and CHecklist for critical Appraisal and data extraction for systematic Reviews of prediction Modelling Studies (CHARMS) reporting guidelines. Original studies reporting the association between CR-proxies (e.g. level or years of education, occupational attainment) and measures of non-cognitive stroke outcome (e.g. National Institute of Health Stroke Scale (NIHSS), modified Rankin Scale, Barthel Index, Functional Independence Measure) were selected. Risk of bias was assessed using Quality In Prognosis Studies (QUIPS). Estimates were pooled using a random-effects model.
Results:
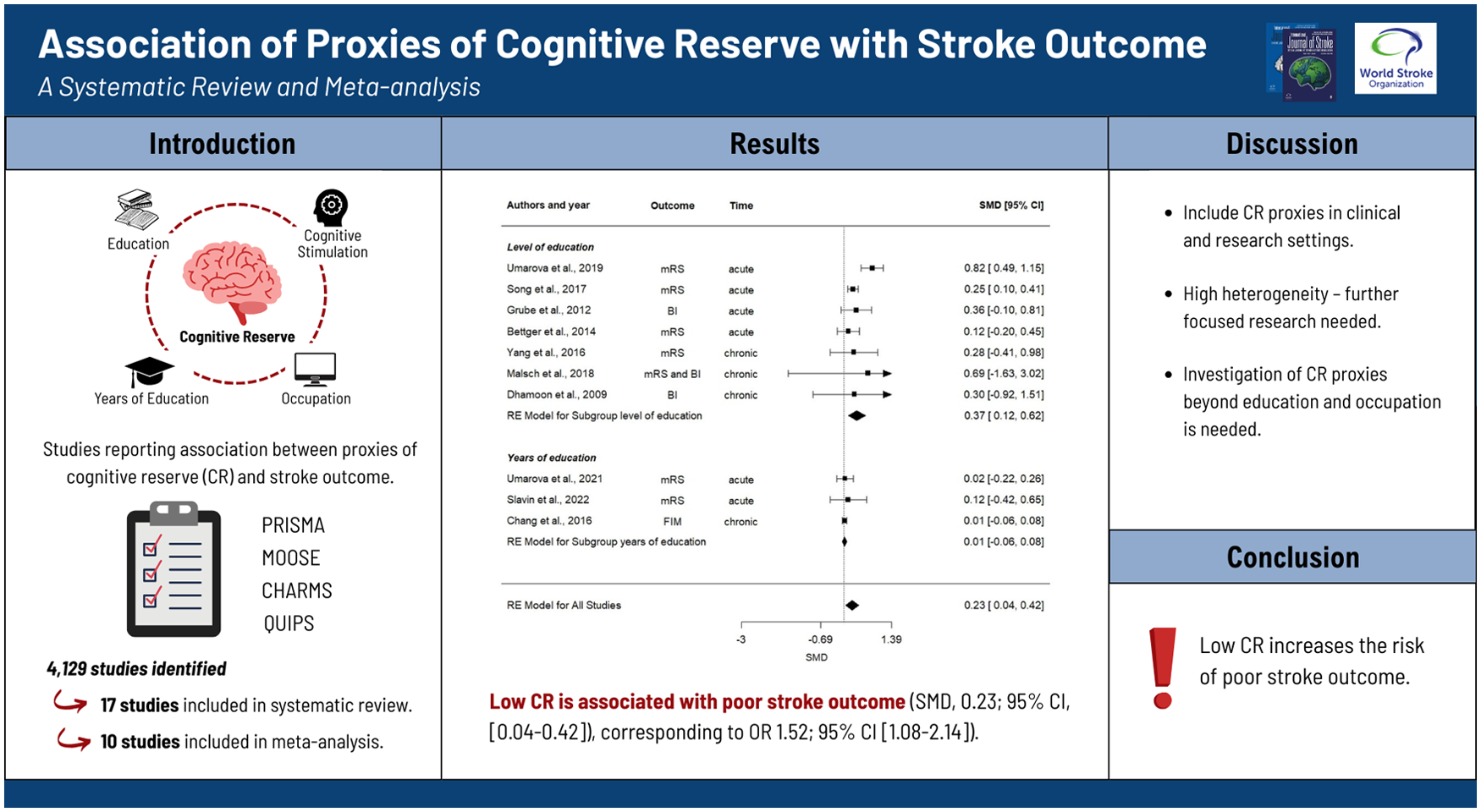
Of 4129 studies identified, 17 were included in the systematic review. Based on the quality check, 10 of them involving 19,308 patients were included in the meta-analysis, whereby only five studies directly addressed the association of CR-proxies with stroke outcome. Pooled standardized mean differences (SMDs) showed evidence for the association of low CR with poor stroke outcome (SMD = 0.23; 95% confidence interval (CI) = 0.04 to 0.42 corresponding to odds ratio (OR) = 1.52; 95% CI = 1.08 to 2.14). Subgroup analysis showed a greater association of level of education (SMD = 0.37; 95% CI = 0.12 to 0.62) and occupational attainment (SMD = 0.34; 95% CI = 0.10 to 0.57) with stroke outcome, as compared to years of education (SMD = 0.01; 95% CI = −0.06 to 0.08). The effect of CR was greater in the acute-subacute stroke phase (⩽3 months post-stroke, SMD = 0.28; 95% CI = 0.04 to 0.52) than in the chronic phase (SMD = 0.01; 95% CI = −0.06 to 0.08).
Conclusion:
We found evidence that CR explains inter-individual variability in stroke outcome and thus may improve its prediction. Low CR increases the risk of poor stroke outcome, and its proxies should be considered in both clinical and research settings. However, we observed high heterogeneity across studies, and further research with specific focus on this topic and CR-proxies extending beyond educational and occupational attainment is needed.
Get full access to this article
View all access options for this article.