
Abstract
Background:
There is a need for accessible and affordable rehabilitation services in low-resource settings (low- and middle-income countries) to support the increasing number of survivors of stroke.
Aims:
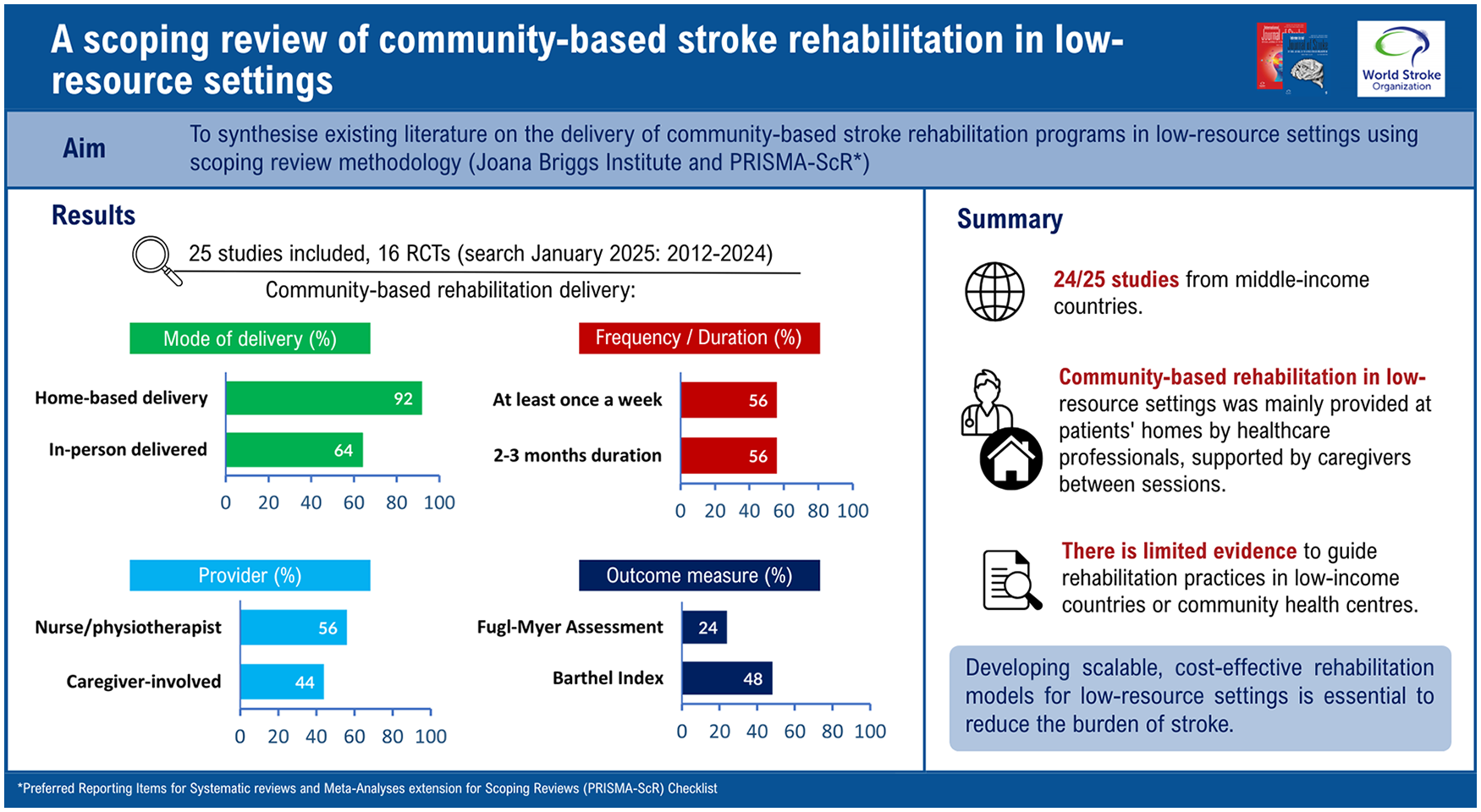
To synthesize existing literature on the delivery of community-based stroke rehabilitation programs in low-resource settings.
Summary of review:
We followed the PRISMA Scoping Review guidelines. Seven databases (including MEDLINE, PsycINFO, and CINAHL) were searched to identify relevant articles published between January 2012 and December 2024. Studies were considered if they included physical rehabilitation strategies as part of a community-based rehabilitation program for individuals with stroke aged ⩾18 years in low-resource settings. Titles, abstracts, and full texts were screened by multiple authors for inclusion. A predefined template that covered physical rehabilitation strategies, setting, providers, frequency, session duration, and program duration was used for data extraction. Results were synthesized narratively. After screening 2892 abstracts, 25 studies were included from 11 countries throughout Asia, Africa, and South America. Most studies were carried out in middle-income countries, with only one study taking place in a low-income country (Uganda). Over half of the studies (n = 16) were randomized controlled trials (RCTs). The physical rehabilitation programs were primarily delivered at home, in person, by a single healthcare professional, typically a physiotherapist or nurse. Session duration was not specified for more than half of the studies. Where reported, sessions were 1 h or less, usually occurring at least once weekly over a 2-to-3-month period. Over 36 different outcome measures were identified, with the Barthel Index being the most common (48%). Overall, 10 RCTs showed a statistically significant difference between intervention and control groups, while five RCTs had no significant difference at the post-intervention outcome evaluation. None of the included publications reported costs or cost-effectiveness data.
Conclusion:
Community-based rehabilitation programs in low-resource settings differ in their physical rehabilitation strategies and characteristics. While the evidence base in this field is growing, the lack of cost-effectiveness evaluations means there is limited guidance to inform investment in, or optimization of, these multi-component, community-based programs.
Keywords
Introduction
Worldwide, stroke is a leading cause of death and disability. In 2019, 101 million people globally were living with stroke, 1 and it was estimated that 85% would benefit from rehabilitation. 2 Concerningly, 89% of the 143 million stroke-related disability-adjusted life years occurred in low-resource settings (LRSs). 1
Rehabilitation is critical to ensuring optimal stroke recovery, 3 and should be widely accessible, offering sufficient therapy doses to support meaningful gains (e.g. at least 3 h/day). 4 However, various challenges exist in accessing rehabilitation. 5 In particular, for LRSs, there is a general lack of available rehabilitation services. 6 While in some LRSs, patients with acute stroke may receive rehabilitation therapy input while in hospital, 6 inpatient lengths of stay tend to be short (e.g. 7–11 days in LRS), 7 and there can be no access to outpatient rehabilitation services after discharge, particularly outside metropolitan areas. 8 Financial constraints can also hinder access if patients are unable to pay for therapy, which is usually an out-of-pocket expense in most LRSs. 9 Consequently, these challenges often contribute to increased disability and overall worse health outcomes in LRSs compared with high-resource settings (HRSs), 10 therefore placing a greater burden on family caregivers. 11
To address access to rehabilitation after discharge in LRS, stroke rehabilitation is increasingly being delivered in primary or community-based settings. 12 Various work-around strategies have been reported to address this rehabilitation shortfall, including the use of family caregivers, integrated care pathways, community health workers, and digital health. 12 However, more detailed information is needed to understand how community-based rehabilitation can be successfully implemented in LRSs.
The aim of this scoping review was to examine existing literature on stroke rehabilitation programs involving physical rehabilitation, delivered in community settings within LRSs, focusing on the components, location, various characteristics (i.e. how delivered, amount provided and what is provided, how accessed), and information on costs or cost-effectiveness.
Methods
The protocol for this scoping review was registered in the Open Science Framework 13 prior to data collection. A summary of the methods is provided below.
Design
We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) 14 guideline and the JBI methods. 15
Population, concept, and context of the scoping review
We focused on stroke rehabilitation programs that included physical rehabilitation strategies to improve or maintain function, such as movement, strength, and daily living activities after stroke. 16 The population, concept, and context for the review are provided in Table 1.
Population, concept, and context of the scoping review.
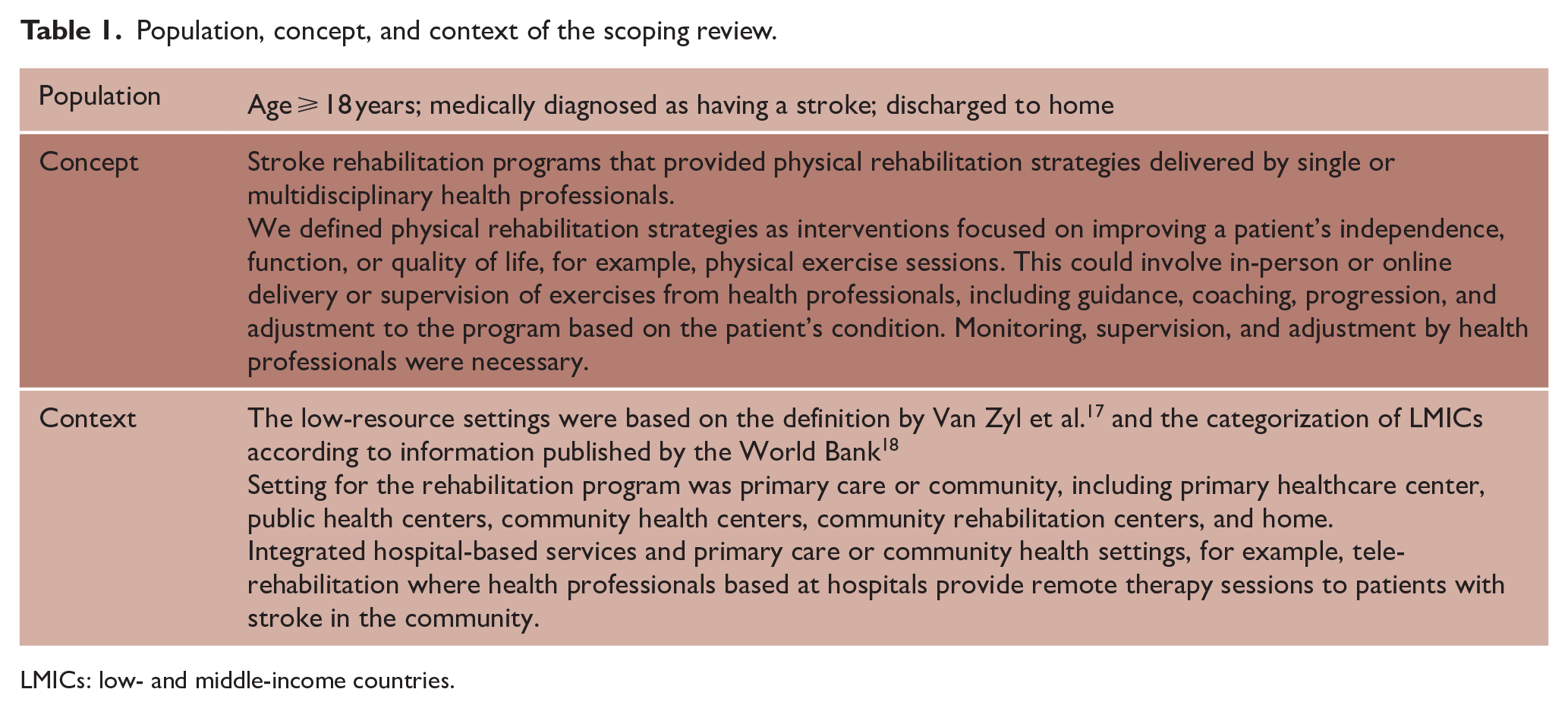
LMICs: low- and middle-income countries.
Search strategy and inclusion/exclusion criteria
One author (Y.H.) conducted searches in seven databases (Medline, PsycINFO, CINAHL, Embase, Global Index Medicus, and Web of Science) in January 2025 to identify relevant references. Gray literature was excluded from this review due to challenges in search and retrieval, language barriers, concerns about quality or reliability, and resource constraints. Keywords used include variations and synonymous terms for stroke, rehabilitation, primary, community, and low-resource settings. An academic librarian was consulted on developing the search strategy (Supplementary File, Table A).
Inclusion criteria for studies:
Involved survivors of stroke (>50% of participants).
Full-text, peer-reviewed primary research study investigating the efficacy, feasibility, or cost-effectiveness of a stroke rehabilitation program that included physical rehabilitation strategies within the program.
Provided in community settings, for example, community health centers, outpatient rehabilitation centers, or homes with or without support from hospitals.
Conducted in low-resource settings or low- and middle-income countries based on World Bank categories. 18
Published between 1 January 2012 and 31 December 2024 to ensure recency for current contexts.
We excluded studies without a physical rehabilitation component or those that only provided rehabilitation in hospitals. Reviews, protocols, conference abstracts, cross-sectional studies, or effectiveness studies of isolated physical rehabilitation interventions that were not delivered as part of a broader, structured community-based program, for example, muscle strength or balance training alone, were also excluded.
Screening process
Identified references were imported into Covidence, with duplicates removed. Titles and abstracts were screened independently by two reviewers (Y.H. conducted the first screening, and the second screening was divided among A.M.I., T.K., E.L., T.P., and D.A.C.). Full texts were reviewed independently by two reviewers (Y.H. conducted the first review, and a second review was shared among A.M.I., T.K., E.L., T.P., and D.A.C.). Conflicts arising during the process were resolved through discussions among the reviewers.
Extracting and charting the data
A pre-determined extraction template was developed based on the template for the intervention description and replication (TIDieR) checklist. 19 We extracted physical rehabilitation strategies and characteristics (e.g. setting, provider, mode of delivery, session duration, frequency, and program duration), and information related to the following program components:
Stroke education: sessions provided by health professionals for patients and caregivers to improve their knowledge, behavior, and skills in stroke management.
Progress monitoring: any follow-ups/contacts (in-person or telephone) between health providers and patients/caregivers without changing or modifying intervention/therapy programs, for example, checking patients’ health status.
Self-directed exercise: exercises performed by patients at home with or without support from family caregivers.
One author (Y.H.) extracted data from all studies, with validation by a second author (A.M.I., D.A.C., E.L., or T.P.). Any conflict related to data extraction was resolved through discussion. Consistent with scoping review guidelines, the quality of included studies was not formally assessed. 20 However, selected domains of risk of bias for randomized trials (n = 16) were presented, including sample size calculation, blinding, randomization, allocation concealment, and drop-out (Supplementary File, Table D).
Data synthesis
Data were recorded in tables, and quantitative information was summarized descriptively. Results were synthesized narratively.
Results
We retrieved 4634 articles. After removing duplicates, 2892 titles and abstracts were screened, and 154 full texts were reviewed, whereby 25 studies were retained (Figure 1). While the inclusion criteria were not limited to English publications, all included studies were published in English. The most common reason for excluding studies was incorrect intervention (no rehabilitation program or no physical rehabilitation strategies).
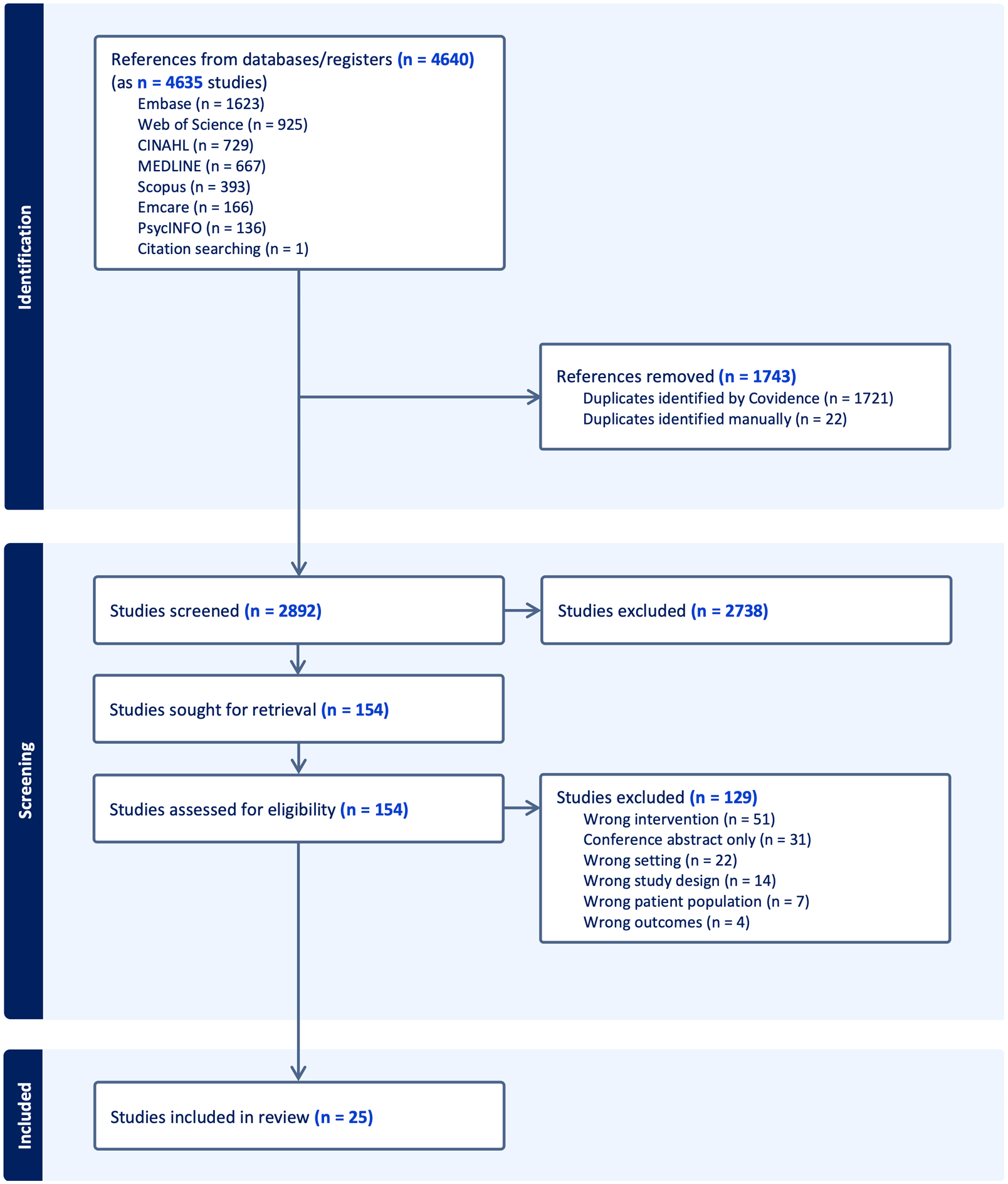
PRISMA flow chart for search results and study selection.
Description of included studies and participants
Over half of the included studies were randomized controlled trials (RCTs) (n = 16, 64%) (Figure 2).
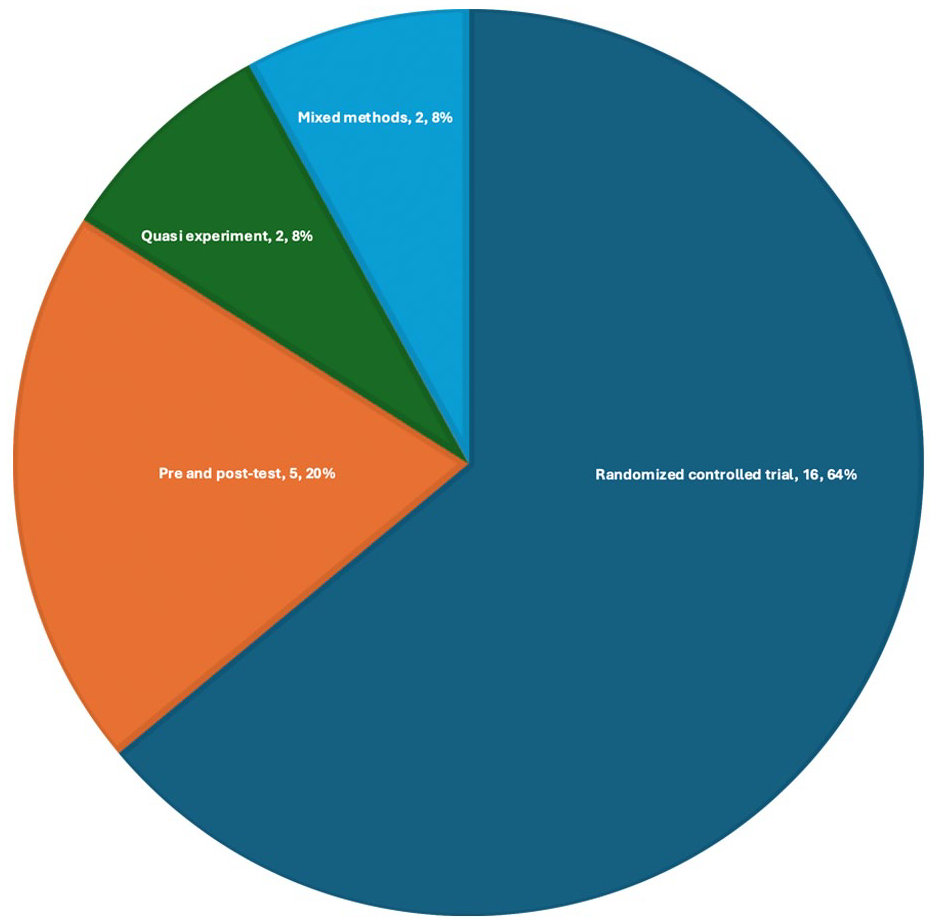
Distribution of studies based on study design (N = 25).
Included studies were conducted in 11 countries, most commonly China (n = 10, 40%). Almost all studies were conducted in middle-income countries, both upper (Brazil, China, Iran, Malaysia, Thailand, and Turkey) and lower (Benin, India, Nigeria, and Vietnam), with only one study conducted in a low-income country (Uganda) 21 (Figure 3). Over half (n = 14, 56%) of the studies included participants in the acute to early subacute phase post stroke (less than 3 months). Nine studies also included participants in the chronic phase (more than 6 months), while two studies did not specify the time period post stroke. The number of participants ranged from 20 22 to 2412 23 (Supplementary File, Table B).

Global heatmap of the distribution of studies based on countries.
Selected domains of risk of bias for randomized trials
Of 16 RCTs, 7 (43%) studies did not report the sample size calculations, 4 (25%) studies did not report blinding, 3 (19%) studies did not report randomization method, 7 (43%) studies did not report allocation concealment, and 3 (19%) studies had relatively high dropout rates (e.g. 29–32%), whereby in two of these RCTs the intervention group had a relatively higher dropout rate compared to the control group (29% vs. 6% and 32% vs. 7%) (Supplementary File, Table D).
Access to community-based rehabilitation programs from acute care
In a majority of studies (n = 15), participants were recruited at hospitals during their acute and subacute stages. Less frequently, participants were recruited from home physiotherapy services, community agencies, municipalities, or outpatient rehabilitation clinics (Supplementary File, Table B). When recruited in hospital, participants and caregivers tended to be provided with stroke education (e.g. guidance on risk factor management, role of medication, daily activity planning), training (e.g. home exercises, functional task practice), or setup (e.g. provision of equipment) to prepare them for home-based rehabilitation. Additional resources included self-rehabilitation kits or manuals describing rehabilitation exercises (Supplementary File, Table C).
Patients were then discharged and expected to manage their rehabilitation program at home with or without support from caregivers. Health providers or trained volunteers visited the participants at home or used virtual communication to provide physical rehabilitation strategies (Supplementary File, Table C).
Caregivers and volunteers received training from health professionals in delivering a stroke rehabilitation program at home, including education on impairment and disability assessment, communication strategies, and goal setting for daily activities. They were equipped to deliver simplified, evidence-based rehabilitation, assist with functional tasks (e.g. mobility, feeding, dressing), support limb positioning, encourage task-specific activities, and help patients maximize functional skills. Training also included tailored exercise programs and active participation in home visits and rehabilitation planning (Supplementary File, Table C).
Components included in the rehabilitation program
The physical rehabilitation strategies included goal setting/re-setting, prescription of self-exercises, education on self-exercises, hands-on therapy sessions, supervised exercises, evaluation and adjustment of exercise plan, addressing challenges, and ongoing guidance on self-directed exercises (Table 2).
Characteristics of interventions.
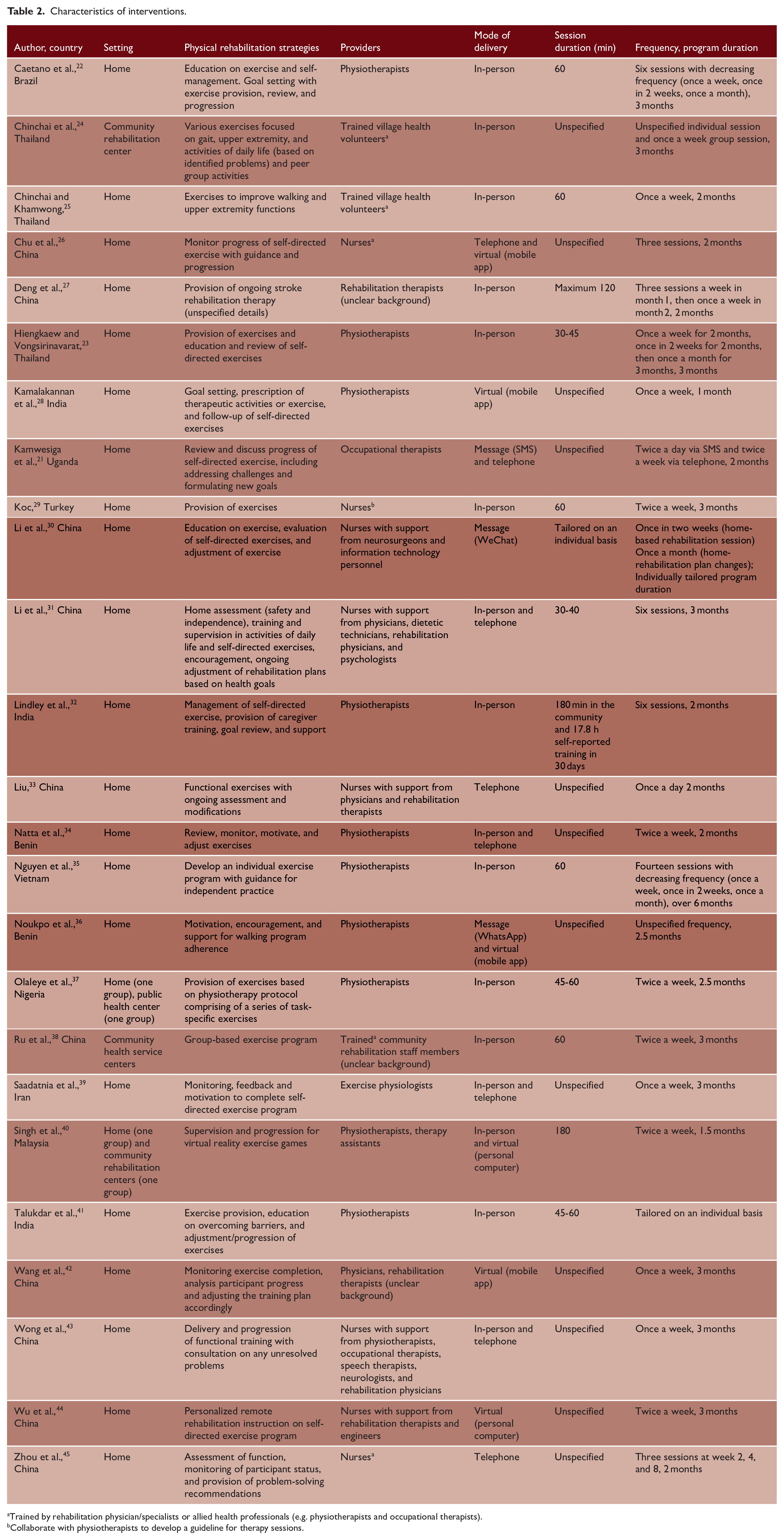
Trained by rehabilitation physician/specialists or allied health professionals (e.g. physiotherapists and occupational therapists).
Collaborate with physiotherapists to develop a guideline for therapy sessions.
In addition to physical rehabilitation strategies, three other core components were common: self-directed exercises (n = 21, 84%), progress monitoring (n = 13, 52%), and stroke education (n = 6, 24%) (Supplementary File, Table C).
Self-directed exercises included those performed independently by participants with or without support from family caregivers or without direct involvement of healthcare providers. Progress monitoring involved evaluation and assessment of progress without providing modification or adjustment to the rehabilitation program. Stroke education covered general stroke knowledge, such as precautions, risk factors of stroke, and secondary preventions (Supplementary File, Table C).
Where and how the physical rehabilitation strategies were provided
In most studies (n = 22, 88%), the physical rehabilitation strategies were conducted at participants’ homes, mostly delivered in-person (n = 16, 64%) (Table 2). Authors of 14 studies reported remotely delivering some physical rehabilitation strategies via telephone (n = 7, 28%), text message or chat (n = 3, 12%), or other virtual approaches including videoconferencing and real-time monitoring via mobile apps (n = 4, 16%) or computer software (n = 2, 8%). In five studies (20%), combined in-person and remote delivery was used.
Provider of physical rehabilitation strategies
The physical rehabilitation strategies were commonly delivered by primary providers or supporting providers; not all were health professionals (Table 2). Most primary providers had health professional training, including physiotherapists (n = 9, 36%) and nurses (n = 5, 20%), occupational therapists (n = 1, 4%), and exercise physiologists (n = 1, 4%). Primary providers without health professional training included trained village health volunteers (n = 2, 8%) and community rehabilitation staff (unclear background) (n = 1, 4%).
Supporting providers reported in five studies included a wider multidisciplinary team (e.g. neurologists, rehabilitation physicians, dietetic technicians, psychologists, or speech therapists) that supported the primary providers (nurses) to address participants’ specific needs.
Frequency and duration of physical rehabilitation strategies
More than half of physical rehabilitation programs (56%) lasted between 2 and 3 months, ranging from 1 to 7 months. Frequencies of delivery varied widely, with the majority of programs provided at least once a week (n = 14, 56%) (Table 2). In some studies (n = 6, 24%), the frequency changed throughout the intervention duration, for example, starting from weekly in the earlier stages and tapering to monthly support. Session durations were unspecified in more than half of the studies (n = 13, 52%). Where reported, sessions typically lasted 30–120 min, with the average being 73 min.
Outcome measures and clinical effectiveness of the community-based rehabilitation program
Overall, 36 different primary outcome measures were reported. The most common were the Barthel Index or Modified Barthel Index (n = 12, 48%) and the Fugl-Meyer Assessment (n = 6, 24%) (Supplementary File, Table B).
Most RCTs compared community-based rehabilitation intervention with usual care or no active intervention (Supplementary File, Table B). Overall, the authors of 10/16 RCTs found a significant improvement for their selected primary outcomes for the intervention group compared to controls. Conversely, five RCTs were neutral for the primary outcomes. One RCT 35 had mixed results for their five primary outcomes.
For the non-randomized studies, there were mixed results, whereby among these nine studies, six showed evidence of effectiveness compared with the comparator data, while in two25,36 others, significant improvements occurred for one outcome, but not others.
Costs and cost-effectiveness
None of the included publications had information on costs or cost-effectiveness.
Discussion
In this scoping review, we provide comprehensive and contemporary evidence in support of community-based rehabilitation programs in LRSs, which differ in their physical rehabilitation strategies and characteristics. We acknowledge that overall, the evidence base is only just emerging and currently lacks sufficient detail and strength of evidence to support any standardized model of care. The findings provide insights and directions to support this critical area of need that seeks to ensure equity of access to rehabilitation services after stroke and its practical implementation in LRSs.
Our review provides more detailed and new current information in contrast to a previous scoping review, 12 given this fast-growing field of research that is striving to support options for increasing effective and scalable rehabilitation services in LRSs. The findings may be helpful for designing a rehabilitation program to be implemented in LRSs and indicating to researchers the gaps that most urgently need attention.
In general, patients with stroke were recruited during acute and subacute hospital care (within 1–6 weeks of onset), received education for community/home-based rehabilitation, and were discharged to manage their own rehabilitation programs at home, with or without caregiver or trained/untrained health worker support. This is a typical pathway in LRSs with the lack of inpatient rehabilitation facilities, 8 commonly available in HRSs. 46 This appears similar to early supported discharge implemented in many HRSs. 47 However, the support provided to post-discharge patients with stroke in LRSs is less comprehensive or intensive compared to that in HRSs. 8
Many of the included studies used healthcare providers to make regular home visits and encouraged patients to continue exercises with caregiver support between sessions. Uses of digital or remote methods of support were also common to the programs we reviewed. These findings are consistent with an increasing trend of using teleservices to deliver rehabilitation,28,36,42 offering promising solutions to increase reach and capacity in remote or underserved areas.
Physiotherapists or nurses generally delivered the physical rehabilitation strategies once or twice weekly for up to 1 h. The amount of therapy delivered in the studies we reviewed is below recommendations for effective stroke rehabilitation,4,48 for example, at least 2 h of active task practice daily performed with allied health therapists. Strategies such as group-based activities, supervised virtual programs, and monitored self-directed exercises are progressive methods to meet the recommended guideline for effective therapy dose.
The evidence for the effectiveness of community-based stroke rehabilitation over usual care was seen mainly in very small trials (an average of less than 50 participants per group) that might be prone to type 1 errors due to the play of chance (or publication bias). Two relatively large studies in China 45 (n = 246) and India 32 (n = 1250) reported neutral outcomes. The trial by Lindley et al. 32 in India found no difference between family-led (hospital and community-based stroke rehabilitation) and usual care (access to rehabilitation, timelines of discharge, and follow-up) in terms of death and disability at 6 months. This suggests that the benefits of community-based rehabilitation are either negligible or only applicable to specific patient groups. Further research is required to determine which patient populations, if any, may genuinely benefit from the intervention.
The absence of program costs or cost-effectiveness data are critical gaps, since implementation costs are a key consideration 49 for implementing health programs, especially in LRSs where budget is a common barrier to implementing rehabilitation programs. 50 Without cost-effectiveness evidence, it remains unclear whether investing in community-based stroke rehabilitation services in LRSs is justified.
Limitations
We acknowledge several limitations of this review from this emerging field of research. We only included studies from peer-reviewed journals found in selected databases, and we may have missed relevant research from gray literature or non-peer-reviewed sources. No non-English studies were included in this review, because most studies in the searched databases were published in English or were found to not be relevant based on our inclusion critiera during the screening process.
Since authors of many studies did not report the session duration limit, this made it difficult to determine if the recommended duration was met. Furthermore, some community-based stroke rehabilitation studies were excluded because they lacked physical rehabilitation components. For example, Aziz et al. 51 described a multidisciplinary team model in Malaysia that provided evidence of feasibility and cost-effectiveness but lacked information on the physical therapy delivered. Our focus on rehabilitation programs requiring the use of physical rehabilitation strategies means other services, for example, communication or psychological therapy programs, were not considered, unless part of a program including physical rehabilitation. The scope of the included studies was dominated by middle-income countries (e.g. China) with only one study 21 conducted in a low-income country (i.e. Uganda), and trials with relatively small sample sizes (e.g. <50 participants per group) highlight potential issues with generalizability. In addition, because we limited our review to home or community health centers, rehabilitation programs offered by hospitals (inpatient or outpatient) were not included.
Recommendations
We found a major gap in understanding community rehabilitation delivery in low-income countries. This disparity is particularly concerning given that low-income countries face a substantial stroke burden 1 and lack rehabilitation resources and infrastructure. 52 There is an urgent need to develop, implement, and evaluate cost-effective community-based stroke rehabilitation programs in these underserved regions while considering their unique healthcare challenges and resource constraints.
Ultimately, to advance the field, there is a need for standardized reporting on community-based stroke rehabilitation studies conducted in LRSs to improve comparability, replicability, and translatability to other contexts. The wide variety of outcome measures reported will undermine efforts to gather high-quality data necessary to strengthen the evidence base for this field. Researchers should adopt the recommendations of the international Stroke Recovery and Rehabilitation Roundtable 53 (e.g. Fugl-Meyer Motor Assessment for motor function, action research arm test for upper-limb function) to ensure standardized and comparable outcome measurement in their trials. In addition, following a reporting guideline such as TIDieR-Rehab 54 is crucial for informing replication and implementation of interventions in different contexts.
There is a clear and urgent need to implement the core components of effective rehabilitation in LRSs. A major challenge is providing active therapy rather than just education, especially when nursing and allied health staff lack autonomy and training in stroke rehabilitation. None of the studies explored the hub-and-spoke model, 55 where a trained expert at a central hub supports less experienced clinicians at satellite “spoke” locations. This model, currently exemplified in Australia 56 and other countries, 57 could be a solution to evaluate in LRSs, particularly given the increasing use of teleservices.
Future research needs to identify the optimal combination of rehabilitation strategies (e.g. goal setting, supervised exercises and education on self-directed exercises) and characteristics for each local population, recognizing that effective solutions may vary based on available resources. There is likely no “one-size-fits-all” solution; each country or region needs to determine the most suitable post-stroke services based on their local and national circumstances and resources.
Conclusion
This review outlines the characteristics of rehabilitation programs delivered outside hospital settings in LRSs. Most community-based rehabilitation was provided in patients’ homes by healthcare professionals, who encouraged continued exercise with caregiver support between sessions. However, there is limited evidence to guide rehabilitation practices in low-income countries or community health centers. To bridge this evidence-practice gap, larger and higher-quality studies using standardized methodologies, interventions, and outcome measures are urgently needed.
In summary, community-based stroke rehabilitation in LRSs is largely home-based and supported by caregivers, yet lacks a strong evidence base to guide practice. Addressing this gap requires well-designed studies using standardized approaches. Effective service development depends on strategic planning, clear reporting, and prioritization of feasible, evidence-based interventions. Collaborations with HRSs, use of telehealth, and adoption of established frameworks can enhance capacity and research quality. These efforts are essential to create scalable, cost-effective rehabilitation models that meet the needs of populations in LRSs.
Supplemental Material
sj-docx-1-wso-10.1177_17474930251368899 – Supplemental material for A scoping review of community-based stroke rehabilitation in low-resource settings
Supplemental material, sj-docx-1-wso-10.1177_17474930251368899 for A scoping review of community-based stroke rehabilitation in low-resource settings by Yudi Hardianto, Elizabeth Lynch, Andi Masyitha Irwan, Thoshenthri Kandasamy, Tara Purvis, Michele L Callisaya, Richard I Lindley, Dorcas Gandhi, Ning Liu, Noor Azah Abd Aziz, Jeyaraj Pandian and Dominique A Cadilhac in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.I.L., J.P., and D.G. conducted one of the included studies. Otherwise, the authors declare no other conflicts of interest associated with this review.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Y.H. received an Indonesian Endowment Fund for Education (LPDP) #202203220808188. D.A.C. received a National Health Medical Research Council (NHMRC) Fellowship (Australian government; #1154273). R.I.L. was supported by the NHMRC Program Grant #1149987.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.