
Abstract
Background:
Lumbar drainage (LD) and external ventricular drainage (EVD) are used in patients with aneurysmal subarachnoid hemorrhage (aSAH) for cerebrospinal fluid diversion and blood clearance. While both have potential benefits, the relative efficacy and safety of LD versus EVD remain unclear, particularly given their use in differing clinical contexts. This study aims to provide a crude comparison of LD and EVD in the context of aSAH using the most updated and comprehensive meta-analysis.
Methods:
Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we performed a systematic review and pair-wise meta-analyses of 28 studies (4390 patients). Cohorts were analyzed across three contrasts—LD versus non-LD, EVD versus non-EVD, and LD versus EVD-using random-effects models. Outcomes included rebleeding, clinical vasospasm, delayed ischemic neurological deficit (DIND)/ischemic stroke, functional status (mRS 0–2 early and late; Glasgow Outcome Scale (GOS) ⩽ 2), mortality, infection, and shunt dependency.
Results:
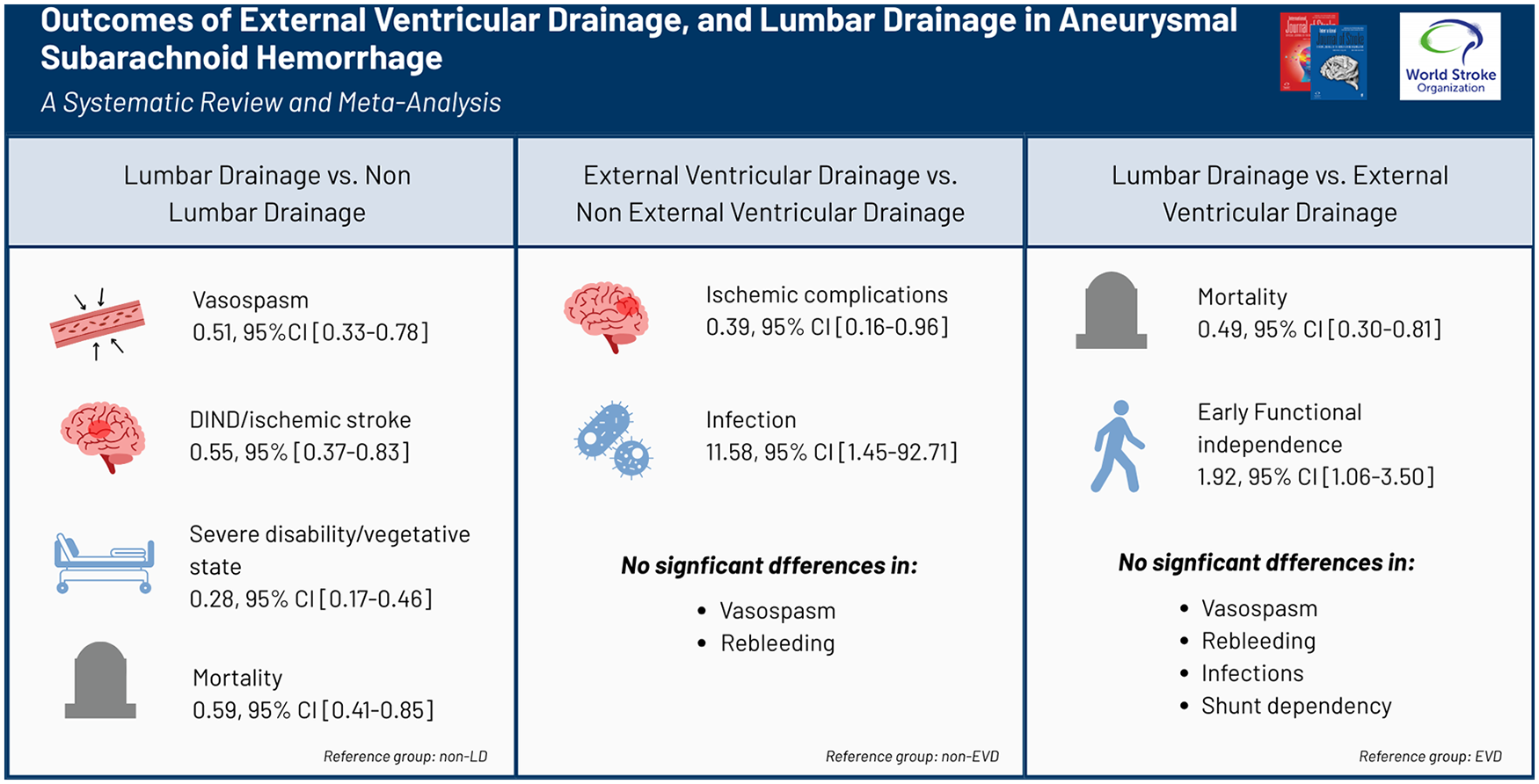
Compared with non-LD, LD lowered the odds of vasospasm (odds ratio (OR): 0.51, 95% confidence interval (CI): 0.33 to 0.78), DIND/ischemic stroke (OR: 0.55, 0.37 to 0.83), severe disability/vegetative state (GOS ⩽ 2) (OR: 0.28, 0.17 to 0.46), and mortality (OR: 0.59, 0.41 to 0.85) without affecting rebleeding rates. Versus non-EVD, EVD reduced ischemic complications (OR: 0.39, 0.16 to 0.96) but increased infection risk (OR: 11.58, 1.45 to 92.71); vasospasm and rebleeding were similar. Direct comparison showed LD superior to EVD for early functional independence (OR: 1.92, 1.06 to 3.50) and mortality (OR: 0.49, 0.30 to 0.81), while rebleeding, vasospasm, infections, and shunt dependency were similar.
Conclusion:
LD was associated with lower rates of vasospasm, ischemic complications, severe disability, and mortality compared to non-LD, without increasing rebleeding risk. EVD reduced ischemic complications but was linked to higher infection rates. When directly compared, LD was favored for early functional recovery and survival. These findings should be interpreted in light of differing clinical indications and baseline severity. Further studies are needed.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.