
Abstract
Background:
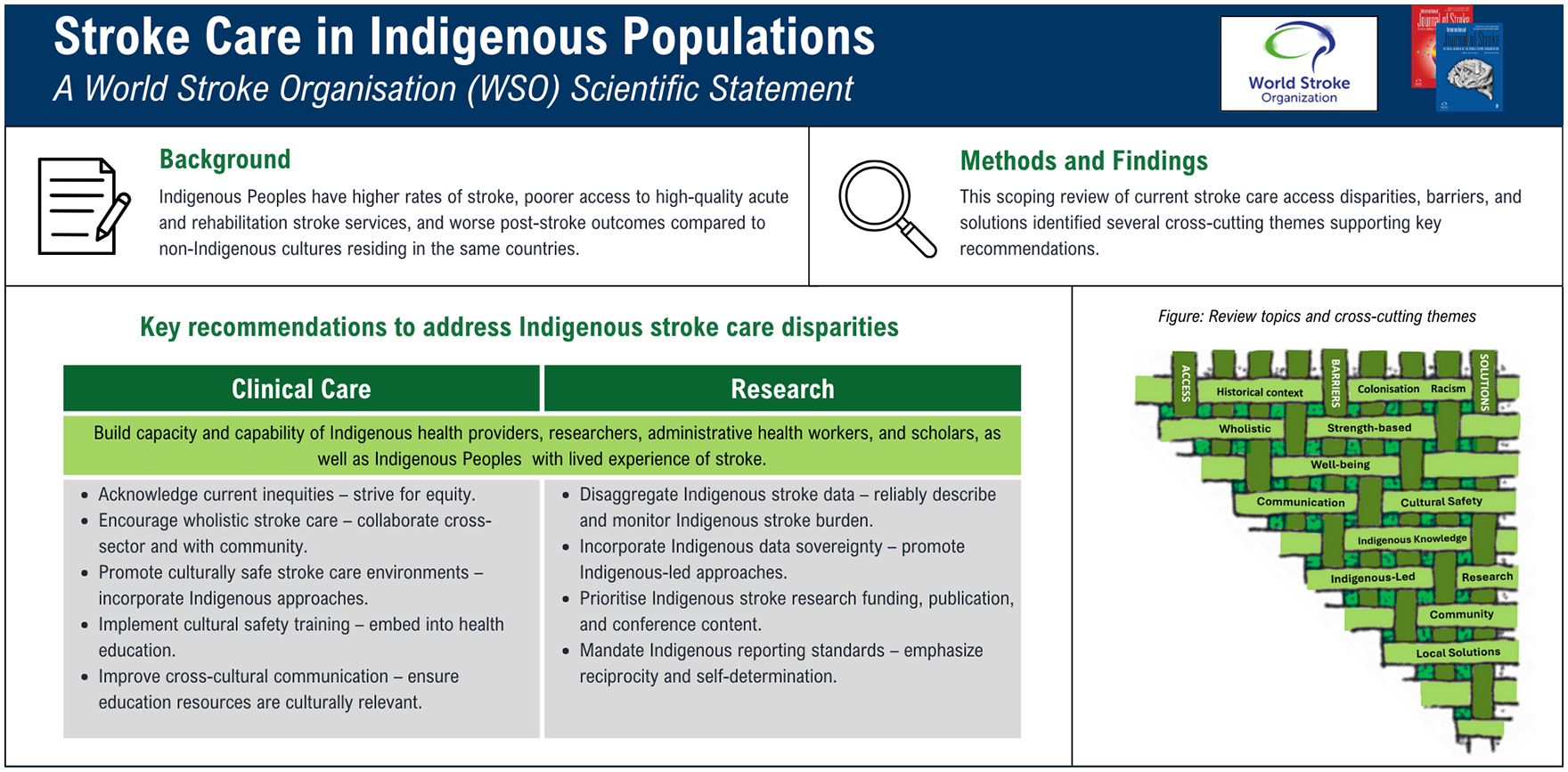
Indigenous Peoples have been reported to experience higher rates of stroke, poorer access to high-quality acute and rehabilitation stroke services, and worse post-stroke outcomes compared to dominant cultures residing in the same countries. The aim of this statement is to summarize available evidence on access barriers contributing to these inequities, effective solutions that have been deployed and tested, and present key recommendations to advance the field.
Methods:
We conducted a scoping review searching Medline, Embase, CINHAL, PubMed, Scopus, and Informit Indigenous Collection using the broad search terms “stroke” and “Indigenous” without date restriction until 1 August 2024. We screened 673 unique titles, 96 abstracts, and 80 full-text papers of which we retained 41. We added 10 additional key references known to authors. Articles were analyzed to identify key cross-cutting themes.
Results:
We identified five key themes: (1) Historical context, colonization and racism; (2) wholistic strength-based approaches to health, well-being, and recovery; (3) communication, health literacy, and cultural safety; (4) Indigenous knowledge systems, research principles, and community-led action; (5) achieving local acceptance versus wide generalizability.
Recommendations:
Key priority areas, detailed in the form of 11 specific recommendations and based on six core values, include improving stroke service responsiveness, Indigenous Peoples empowerment, and Indigenous research support to better meet the needs of Indigenous Populations globally. The statement has been reviewed and approved by the WSO Executive Committee.
Purpose
The purpose of this scientific statement is to provide guidance to the scientific and clinical stroke community on how to approach the care for individuals with stroke who self-identify as Indigenous or belong to Indigenous communities, to support strategies to eliminate current inequities both at individual and system levels, and guide research approaches.
Background
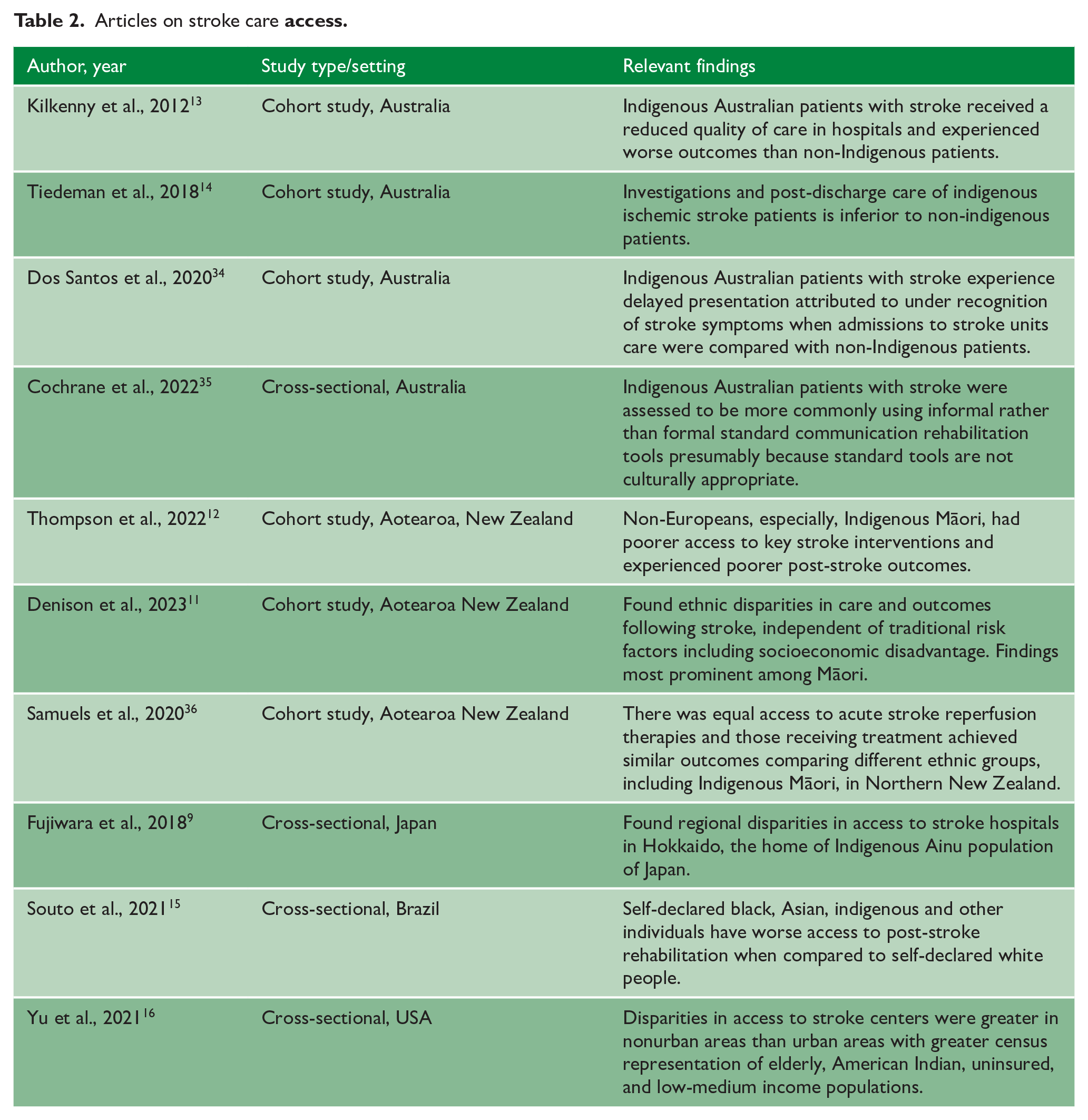
Stroke is one of the leading causes of death and adult disability globally. 1 Indigenous Peoples have been reported to experience increased stroke risk factors and disparities in stroke incidence, with stroke often occurring at a younger age.2–5 A few Indigenous populations have been reported to experience overall excellent health-status and similar or even lower stroke incidence compared with the dominant culture; however, these benefits appear linked to their ability to retain traditional practices and life-styles, benefits that are increasingly at risk of being lost and replaced by accumulated stress related to loss of land, culture, and inability to maintain traditional practices.6–8 Regardless of incidence and risk factors, Indigenous Peoples experience reduced access to high-quality acute and rehabilitation stroke care9–16 and poorer post-stroke outcomes including higher mortality.2,4,11,12,17,18
Methodological complexities
Conducting a “scientific” review on the topic of stroke care in Indigenous Populations is not straight forward due to incongruence around definitions, data collection, and methodologies.
Defining “Indigenous”
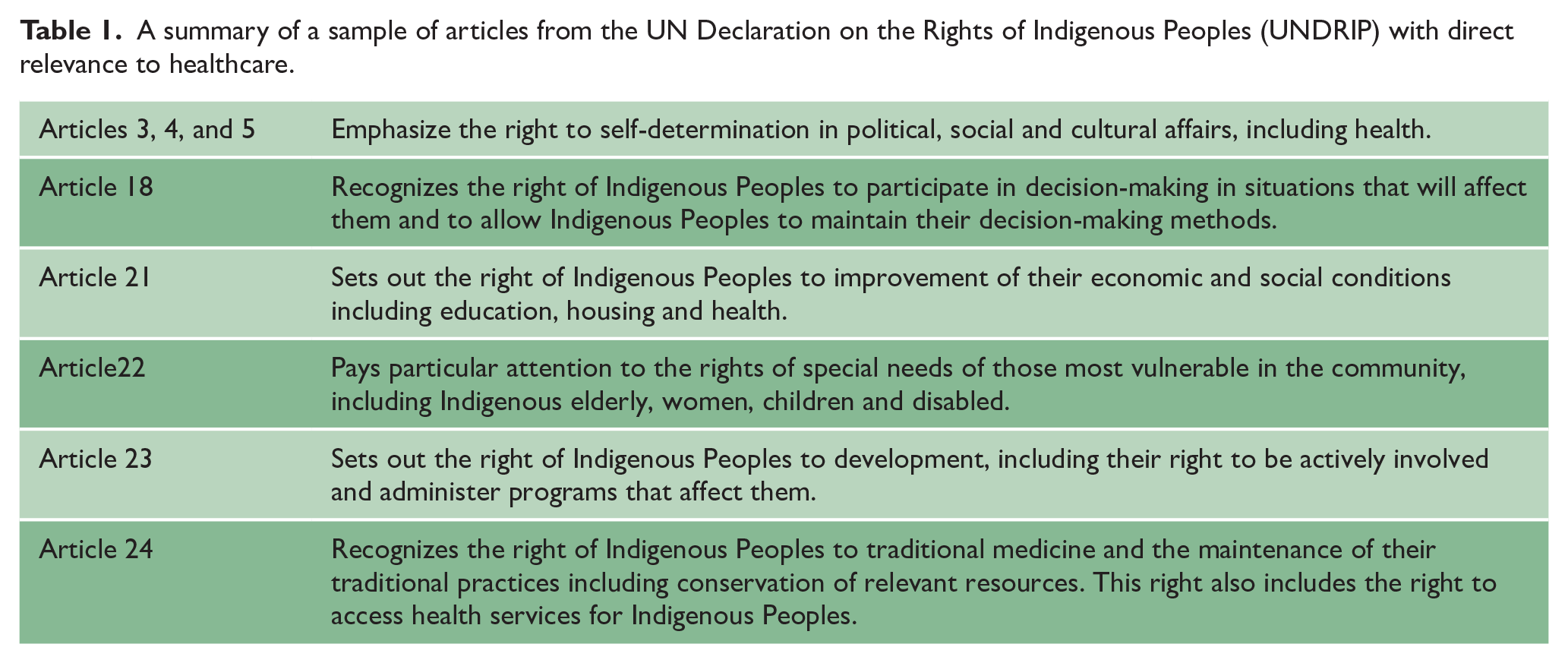
The word Indigenous has origins in Latin indigena, meaning “native” or “sprung from the land” and the World Health Organization defines “Indigenous Peoples [as being] custodians and practitioners of unique cultures and ways of relating to people and the environment. They possess social, cultural, economic, and political characteristics that are distinct from those of the dominant societies in which they live.” 19 As a grouping, “Indigenous People” have been recognized by the United Nations. The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) was passed as a non-binding resolution by the UN in 2007 and consists of 24 pre-ambular provisions and 46 articles that set out the minimum standards for the survival, dignity, and well-being of Indigenous Peoples throughout the world, including rights related to governance, health, community, culture, language, lands, territories and resources, and education (see Table 1 for key highlights).
A summary of a sample of articles from the UN Declaration on the Rights of Indigenous Peoples (UNDRIP) with direct relevance to healthcare.
However, it should be noted that, the term “Indigenous” is problematic as it suggests a single cohesive group of Indigenous populations yet the estimated 476 million Indigenous Peoples living across more than 90 countries worldwide are incredibly diverse even within a single country. 20 In addition, not all Peoples who meet the WHO definition and UNDRIP inclusion refer to themselves by that term. Other “umbrella” terminology is used such as “First Nations,” “Natives,” “Adavasi,” and “Aboriginal” to name just a few. To complicate things further, many Indigenous Peoples refer to themselves by names in their own language not consistently matching the names given to them by others. Which terms are used, and which are preferred, may also change over time with negative connotations associated with some more than others. From a global perspective, “Indigenous” has emerged as the currently preferred single umbrella term, when referring to these communities collectively and some important commonalities do exist. For the purposes of this article, we considered publications that were identified using the search terms “Indigenous” and “stroke” (see below for more detail on search strategy) excluding only those where “Indigenous” clearly referred to the dominant culture as in “indigenous Africans” in comparison to “African Americans.”
Impact of discrimination on data validity
In addition to the definition challenge, accurate population and disease estimates are complicated by the fact that many groups meeting the above criteria prefer not to use the term “Indigenous” due to factors including historical discrimination and marginalization. 21 This is the case, for example, for many Ryukyuans (primarily in present-day Okinawa, Japan). Although they are recognized as Indigenous by the United Nations and other organizations such as the International Work Group for Indigenous Affairs and the Minority Rights Group, most do not self-identify as Indigenous, with implications for health research. 22 Similarly, governments may not recognize the existence of Indigenous populations. 23 Many do not collect self-identification of Indigenous status in census or in public records as this is regarded as sensitive information. 24 Others continue to prioritize assimilation. 23 However, most Indigenous groups increasingly advocate for their recognition as Indigenous and demand ethnic disaggregated health data capture to help identify and address ongoing health and social disparities.23,24 There is also increasing emphasis on, and advocacy of, Indigenous data-sovereignty relating to increased involvement regarding how data about Indigenous people are designed, collected, overseen, stored, and used. 25
Differences in research methodologies
Finally, given cultural differences, “scientific research” in the Indigenous space can look very different than “dominant” or non-Indigenous research, and some initiatives will never result in journal publication due to parallel Indigenous knowledge systems often preferring other forms of dissemination such as verbal presentations to local communites.26,27 While the dominant mainstream scientific method focuses on the health of individuals and operates from a predominantly biomedical model of health, many Indigenous populations operate from a collectivist model, focussing on a wholistic community-specific approach that supports not only individual physical health, but also the mental and spiritual well-being that contribute to and also rely on the overall well-being of the extended family and community. 28 This Indigenous well-being model is less suited to being assessed by Western positivist methodologies such as randomized controlled trials or even large scale observational studies. As a result, the available literature on “Indigenous stroke” is generally dominated by non-Indigenous researchers using dominant scientific approaches “doing research on Indigenous Peoples.” This carries a significant risk of disempowerment and perpetuating historical injustices. Alternatively, the literature may take the form of more Indigenous congruent ethnographic, narrative and/or qualitative methodologies that are preferably community driven and focus on “by and for Indigenous Peoples” that may be dismissed by the dominant culture as “inferior” or even entirely “unscientific.” This tension is profound and should be a primary focus for reconciliation.
Approach and writing panel
With these considerations in mind, we aimed to interweave various knowledge systems to offer a collective way forward, acknowledging the goodwill of members of the dominant culture to support the health of Indigenous Peoples in their pursuit of well-being. However, it is also important that non-Indigenous audiences approach this topic with cultural humility and a genuine willingness to engage with Indigenous perspectives.
To support our effort, we have formed an international panel of researchers with expertise in the fields of stroke care, implementation science, health equity, and Indigenous health. Our panel included senior stroke clinicians, stroke researchers, and individuals with extensive experience in collaborating with Indigenous communities to improve Indigenous stroke care delivery and conduct stroke research. Importantly, more than 50% of the panel self-identifies as Indigenous and belonging to Indigenous communities with extensive research experience in the Indigenous health space. We deliberately prioritized Indigenous researchers with expertise in Indigenous stroke and wider relevant health research as we saw the Indigenous voice and expertise as most critical for this work. Prioritizing the involvement of Indigenous voices provides essential perspectives and represents an important step toward decolonizing current Indigenous research efforts. Many of our Indigenous researchers also hold important governance roles within their community, one is a stroke survivor, and another an Indigenous Elder. These diverse perspectives add further depth to the expertise of the panel and strengthen the community voice.
To ensure our work meets Indigenous cultural publication standards, we adhered to the “Consolidated criteria for strengthening reporting of health research involving Indigenous Peoples” (CONSIDER) framework (see Supplement). 29
Scope of evidence reviewed
Most of the available literature focusses on the epidemiology of stroke in Indigenous populations describing incidence and risk factors from a dominant scientific paradigm. Instead of reiterating recently published reviews on this topic2,17,30 and restating the problem, this statement explores underlying causes, identified solutions, and proposes a way forward. Due to the nature of this topic and the associated methodological challenges, the panel agreed that a systematic review employing standard evidence grading was not the appropriate methodology. Instead, we conducted a systematic literature search to underpin a narrative report.
Given the challenges around defining “Indigenous,” the panel discussed appropriate search terms. The initial proposal was to include various potential synonyms for the term “Indigenous” such as “First Nations,” ‘Aboriginal, “Natives,” and so on. However, it became clear that this would prioritize Western colonized populations that preferentially use these terms over groups that prefer using region specific or locally unique terms such as the South Asian “Adavsi,” and Japanese “Ainu.” When we considered adding these search terms, we realized many more would need to be added to achieve completeness. We considered adopting a recently compiled exhaustive list of Indigenous Peoples in high-income countries. 17 However, this would have missed Indigenous Peoples in low- and middle-income countries, some of which were not even included under UNDRIP, and realized that “completeness” was not, in fact, achievable. In addition, capturing all historical research involving Indigenous People would have required including terminology that was never approved by Indigenous People and is now viewed as inappropriately disempowering or even racist, and the panel preferred not to perpetuate the use of such historic terms. Reassuringly, trialing a few broader searchers, beyond the term “Indigenous,” for example, including “Adavasi,” or “First Nations,” did not, in fact, substantially change the number of identified relevant papers.
Therefore, after much deliberation, the panel agreed to limit the systematic search to the terms “Stroke” and “Indigenous” as the globally most accepted collective term for these diverse populations at this time in history, and supplement with relevant papers from other sources based on the panel’s expert opinion. We feel that this achieved the best balance between two conflicting scientific and cultural paradigms, and optimally achieves our goal to “interweave” approaches while also achieving reasonable data saturation. To further optimize the search, we expanded it to five databases including the Informit Indigenous Collection.
On 1 August 2024, we searched Medline, Embase, CINHAL, PubMed, Scopus, and Informit Indigenous Collection using the broad search terms “stroke” and “Indigenous.” We screened 673 unique titles, 96 abstracts, and 80 full-text papers of which we retained 41. We focussed on primary research although retained some key review articles to inform the discussion. We included papers of all types of methodology and highlighted publications that demonstrated cultural consideration in line with the CONSIDER framework as part of their methodology. We added additional key references known to authors (n = 10).
We collated articles into tabular format grouping to allow the reader easy reference by article topic. However, to interweave non-Indigenous and Indigenous methodologies, we present the narrative aspect of this report according to cross-cutting themes that we identified throughout the reviewed papers, regardless of topic type, aiming for a more wholistic thematic presentation. Within each cross-cutting theme we highlight specific access barriers, Indigenous principles and values, and present case studies of implemented solutions. We conclude with a set of recommendations.
Results of the literature search
Of the 41 full-text articles and policy papers included in this report, the majority came from Australia (n = 17), followed by Aotearoa New Zealand (n = 10), and much fewer from USA (n = 4), Japan (n = 4), Canada (n = 3), and South Asia (n = 3). We found single articles from Brazil, South Africa, Taiwan, Korea, Norway, and Southeast Asia, and included three multi-national reviews. Most of the evidence and resultant recommendations are based on experiences from high-income, English-speaking countries with a colonial past. However, there is clear evidence from the broader literature that there are also very similar challenges faced by Indigenous Peoples in other parts of the world including many parts of Asia, South America, and Africa and we have included some of these examples where feasible.15,23,24,31–33
Tables 2–5 summarize publications grouped by stroke care “Access,” “Barriers,” and “Solutions.” However, the below narrative summary is structured according to five cross-cutting themes that emerged from most if not all articles regardless of table category. These themes are “Historical context, colonisation and racism,” “Wholistic strength-based approaches to health, well-being, and recovery,” “Communication, health literacy, and cultural safety,” “Indigenous knowledge systems, research principles, and community-led action,” and “Achieving local acceptance versus striving for wide generalisability.” The reader should not attempt to marry up the table headings to cross-cutting themes. Data are presented deliberately in two formats to interweave dominant scientific and Indigenous approaches, with an emphasis on an Indigenous wholistic approach presented in the narrative portion of this statement (Figure 1). Table 5 summarizes key review articles and policy papers.
Articles on stroke care
Articles describing barriers and exploring principles and values when caring for Indigenous People.
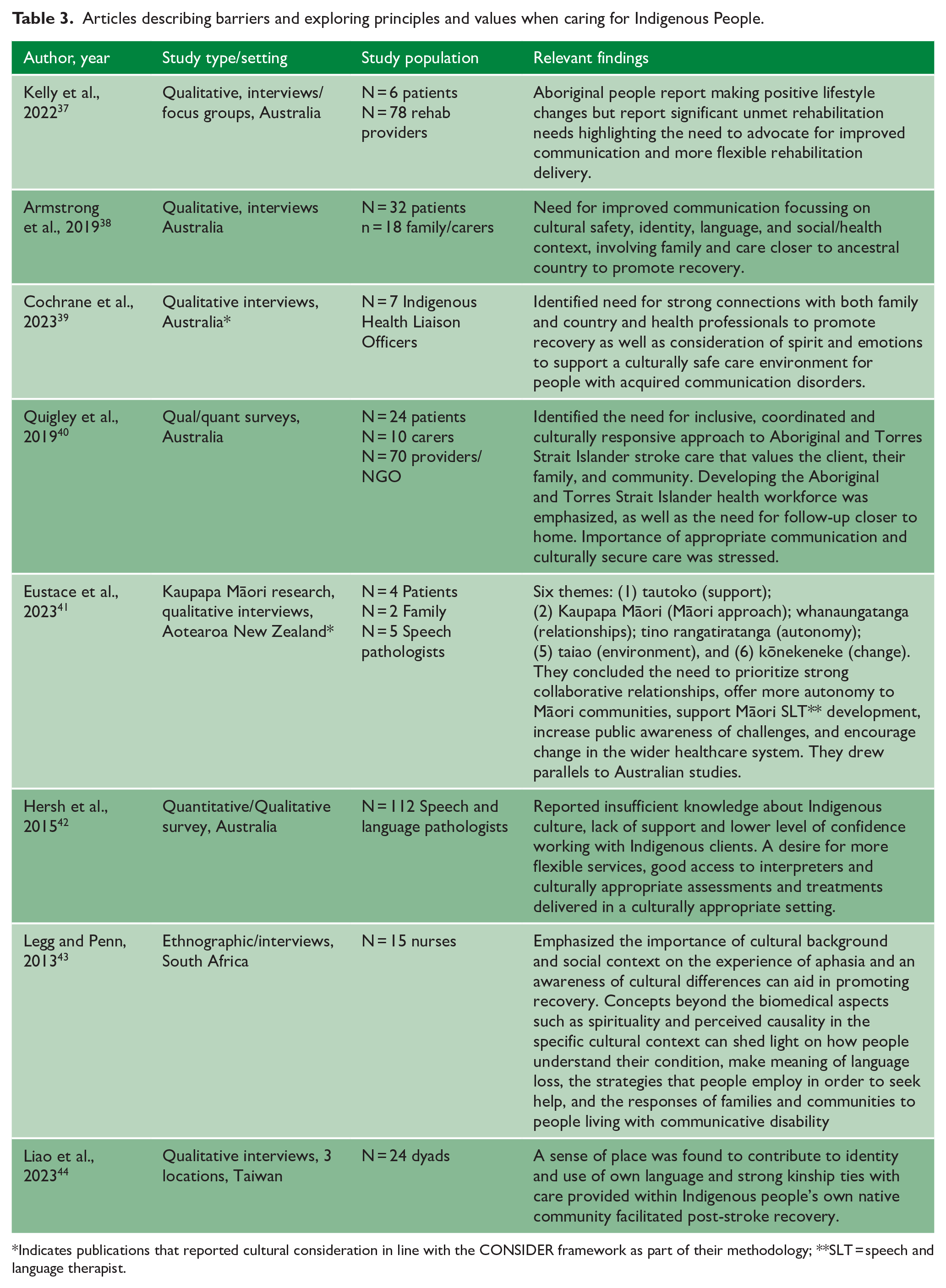
Indicates publications that reported cultural consideration in line with the CONSIDER framework as part of their methodology; **SLT = speech and language therapist.
Articles exploring solutions, including specific interventions, to optimize Indigenous Stroke Care.
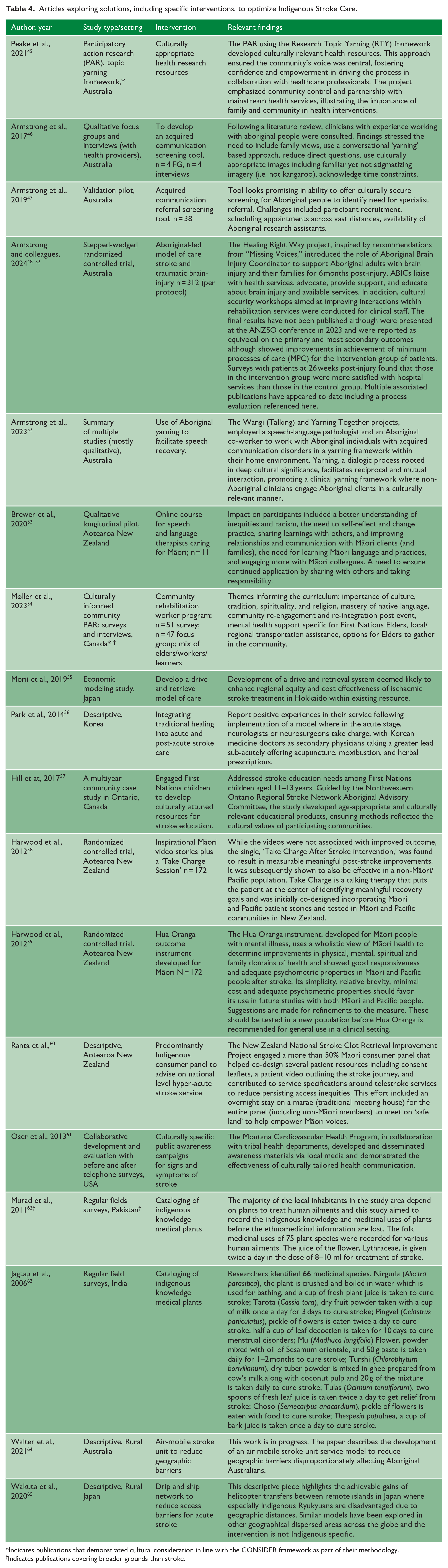
Indicates publications that demonstrated cultural consideration in line with the CONSIDER framework as part of their methodology.
Indicates publications covering broader grounds than stroke.
Key Review Articles, Statements, Policies, and Guidelines.
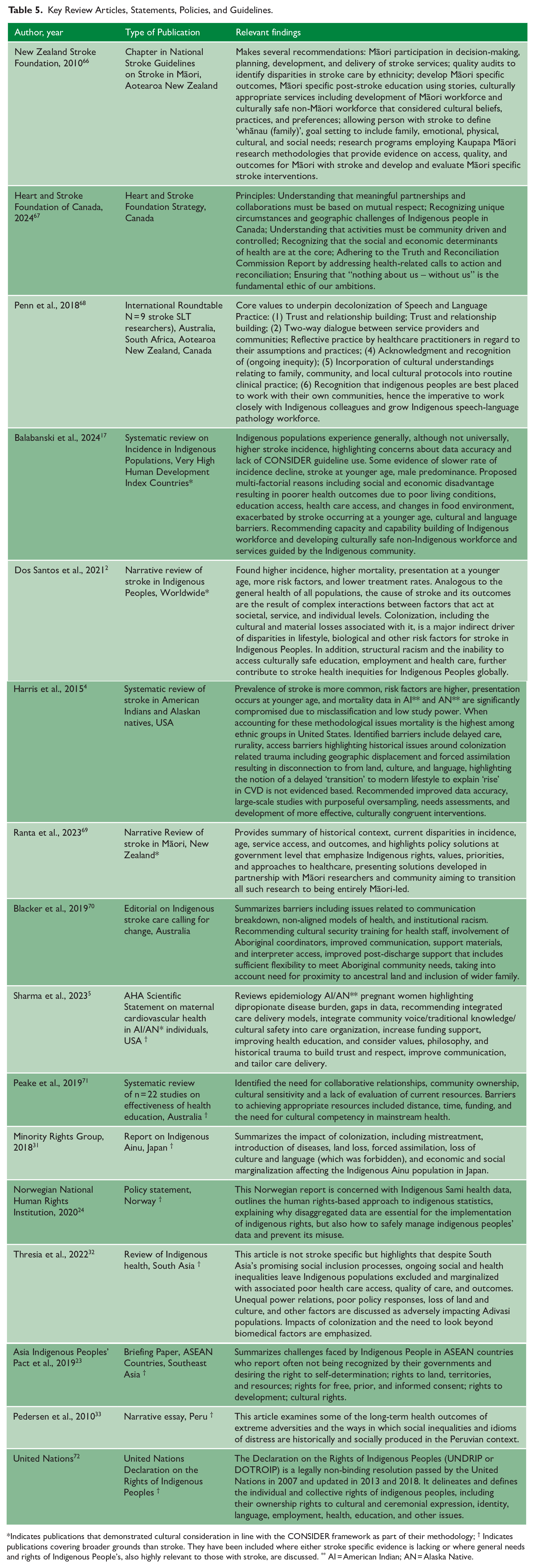
Indicates publications that demonstrated cultural consideration in line with the CONSIDER framework as part of their methodology; † Indicates publications covering broader grounds than stroke. They have been included where either stroke specific evidence is lacking or where general needs and rights of Indigenous People’s, also highly relevant to those with stroke, are discussed. ** AI = American Indian; AN = Alaska Native.
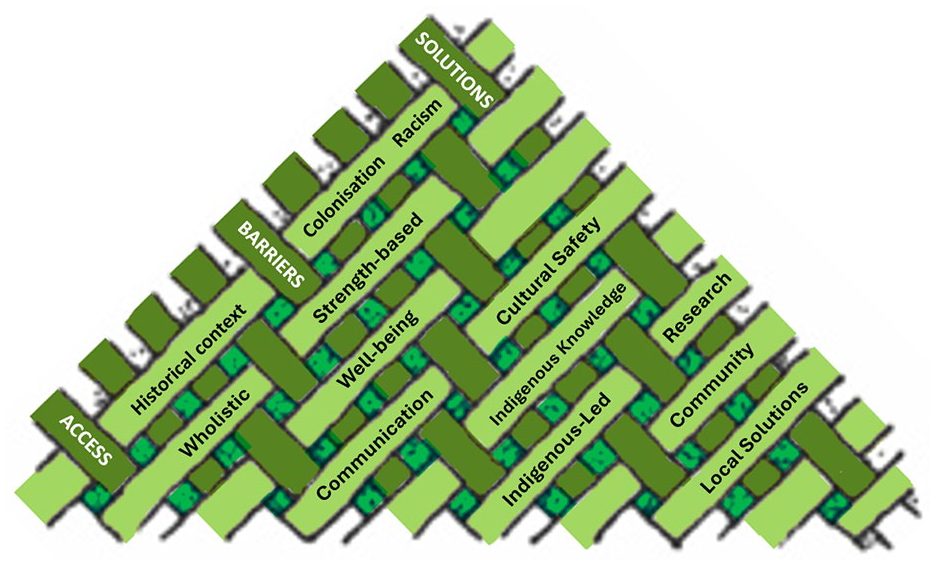
Interweaving approach to presenting literature review results.
Key cross-cutting themes
Historical context, colonization, and racism
Our own history influences our approaches to health. Western stroke clinicians and scientists typically focus on biomedical aspects of health to explain stroke risk and outcomes. However, there is little evidence to indicate that Indigenous Peoples worldwide share specific biological attributes that explain the common patterns of increased stroke risk factors,2–5 stroke incidence, stroke care access barriers,9–16 and poor post-stroke outcomes.2,4,11,12,17,18 Some of the shared disparities may be attributed to geographic access challenges, as many Indigenous Peoples reside rurally. We found evidence of effectively addressing, or planning to address, rural access to stroke care, especially related to reperfusion access disparities, through well-organized hyper-acute stroke networks and novel technologies such as air mobile stroke units.9,36,57 Addressing geographic access barriers to acute and rehabilitation services is important and should continue.
However, geographic distance cannot fully explain Indigenous stroke disparities. Many studies have effectively controlled for geographic and other biological patient factors, concluding that significant aspects of access inequity could only be explained by historical and resultant social factors.11,12,70 Nearly all of the reviewed literature from across the globe identified that many, if not all, of the stroke-related health inequities experienced by Indigenous Peoples today relate to socioeconomic, cultural, and environmental consequences attributed to colonization, marginalization, systemic racism, and underlying power hierachies.2,4,5,69 Some of the consequences relate to socioeconomic disadvantages including poverty and lack of educational opportunity. Others relate to service provision that does not align with cultural values (see below). Finally, there is persistent distrust due to inter-generational trauma related to forced assimilation and destruction of culture and language, forced migration and loss of ancestral land and territories, systemic mistreatment and subjugation, widespread violations of their human rights, and other forms of systemic racism.2,4,69,70,72
The parallels around systemically enforced assimilation by separating Indigenous children from their families and placing them in often very unsafe boarding schools is remarkable across nations and cultures, as are governmental policies of assimilation, forbidding the use of Indigenous languages, cultural customs, knowledge systems, and healing practices resulting in a dramatic power imbalances and the loss of self-determination.2,4,23,32,53,69,70,73
One example of persistent modern systemic racism is the ban, in some countries, on collecting disaggregated ethnicity data that precludes the identification of the stroke burden and access disparities. Even where these data are collected, common misclassification of ethnicity has led to profound misrepresentation of stroke burden that can present a highly inaccurate picture downplaying disparities.4,24,74
Similarly, the mistrust of healthcare and research settings has been perpetuated by untrustworthy and unethical research that has exposed Indigenous populations to undue harms. 75 It is our collective responsibility to rebuild eroded trust. 76
Wholistic 1 strength-based approaches to health, well-being, and recovery
An important aspect for Indigenous populations is the value placed on extended family and community,38-40,44 connection to ancestral land,38,39,69,70 and a general preference for a wholistic approach to well-being that considers not only physical, but also spiritual, emotional, mental and community health and well-being.5,39,41,43,54,59 Prioritizing these needs in the setting of a sterile inpatient ward away from their own community, with little space to accommodate large families and limited therapies that focus exclusively on physical health create obvious barriers.
Many Indigenous Peoples view health as the presence of well-being rather than the absence of disease, creating incongruence with concepts such as “rehabilitation” which generally focusses on current deficits instead of future aspirations. While goal setting is a well-supported approach to achieving outcomes in dominant health systems, the type of priorities goals set may differ substantially between cultures yet there may be very little interest in exploring the consideration of Indigenous patient centered outcomes.37,79
The dominant health system thus continues to evoke paternalistic approaches with the expectation for people from different cultures to simply accept dominant approaches and it is probably not surprising that uptake and trust often remain limited; this is especially likely on the backdrop of the historical practices mentioned above. Insisting that “dominant approaches work better” risks being perceived as patronizing and insensitive and fails to support a move toward decolonization and restorative practice. On top of this, the presumption that dominant practices are necessarily superior is inaccurate, as evidenced by persisting gaps in stroke incidence and outcomes between Indigenous and non-Indigenous populations worldwide.4,12,17,80
We found several examples of stoke interventions tailored to Indigenous needs that achieve improved post-stroke outcomes compared to usual approaches. One randomized controlled trial tested the benefits of a co-designed “talking therapy” called “Take-Charge After Stroke” that incorporates Indigenous values and aspects of health beyond physical recovery. This intervention achieved significantly reduced disability compared to usual care. 58
The Wangi (Talking) and Yarning Together intervention, employed a speech-language pathologist and an Aboriginal co-worker to work with Aboriginal individuals with acquired communication disorders in a “yarning framework” within their home environment. Yarning is a dialogic process rooted in deep cultural significance, that facilitates reciprocal and mutual interaction. It promotes a clinical yarning framework where non-Aboriginal clinicians engage Aboriginal clients in a culturally relevant manner. 52
A group in Korea reported positive experiences in their service following implementation of a model where in the acute stage, neurologists or neurosurgeons take charge, with Korean medicine doctors as secondary physicians taking a greater role in the sub-acute phase offering acupuncture, moxibustion, and herbal prescriptions. 56
There are more opportunities to integrate traditional, wholistic therapies, such as therapeutic massage, prayer, ceremonial practices and other forms of spiritual healing, and traditional native or herbal remedies, which have been actively promoted by some guidelines.5,66 As interest in traditional and wholistic healing approaches continue to grow, it is essential to support efforts that prevent the loss of traditional Indigenous medicinal knowledges. Such efforts are reported in South Asia where researchers are working with local communities to document traditionally used healing plants.62,63 However, when undertaking such projects it is critical that Indigenous communities are not exploited or harmed as part of this process. These efforts can be very extractive, result in “biopiracy,” with little to no acknowledgment, compensation, or support for participating Indigenous communities. 81 For instance in Okinawa, southern Japan, although locals have contributed to a plethora of studies and documentaries exploring their exceptional longevity, local life expectancy has been rapidly declining over the past few decades, raising questions of what practices responsible and ethical research entails. 7
Communication, health literacy, and cultural safety
Many reviewed papers stressed the importance of improving communication between stroke healthcare providers and Indigenous Peoples and their families with or at risk of stroke.5,37,38-40,42,53,61,70,77 Many, especially elder Indigenous Peoples, are not fluent in the country’s dominant language and interpreter services can be critical to improve communication and stroke care. However, often even more subtle challenges present major barriers. Educational materials, whether paper or digital, are often very “white” and mono-cultural in their imagery including the people in the pictures and the environment and activities they display (e.g. NIHSS “cookie theft” picture https://www.ninds.nih.gov/health-information/stroke/assess-and-treat/nih-stroke-scale). This can create unexpected barriers in communication including in the evaluation of stroke symptoms and outcomes. Armstrong et al. 47 developed a culturally secure and tailored communication assessment tool for Aboriginal Peoples with stroke and found a high degree of validity in their pilot to accurately identify the need for specialist referral. They employed more of a storytelling approach than yes/no questions. When developing such tools, it is imperative to involve Indigenous Peoples with lived experience to inform the design and ensure stigmatizing imagery (e.g. kangaroos for Aboriginal Peoples) is avoided. An exemplary approach to this was demonstrated by Peake et al. 45 using Participatory Action Research (PAR) and the Research Topic Yarning (RTY) methodology, putting community voice at the center.
Several of the papers we identified highlighted delays in presentation to hospitals as a key reason for access disparities.4,64,82 This has also been identified to be of relevance to non-Indigenous people and has resulted in much attention on public awareness campaigns such as FAST (i.e. “Face,” ‘Arm, “Speech,” and “Time” to guide stroke recognition and emphasize urgent action). While these efforts are undoubtedly helpful in general and potentially for Indigenous populations, many such “health literacy” attempts have failed to consider the cultural relevance of such materials.61,83 In Aotearoa New Zealand, the Stroke Foundation and Ministry of Health partnered with the Health Promotions Agency in a Māori-led team that prioritized culturally relevant materials, which was associated with improved uptake of the message. 84 The Montana Cardiovascular Health Program collaborated with tribal health departments to develop and disseminate culturally tailored awareness materials, 61 and the Northwestern Ontario Regional Stroke Network Aboriginal Advisory Committee guided the development of an age-appropriate and culturally relevant educational program to raise stroke awareness among children aged 11–13 years. 57
These successful efforts highlight a key shift in the approach to “health literacy,” de-emphasizing the presumed lack of “health literacy” among Indigenous Peoples when mainstream messages are slower to resonate and instead ensuring messages are tailored culturally appropriately to achieve the desired effect. In other words, we must acknowledge that much of the responsibility lies with the “communicator” if communication is ineffective, not simply the audience. This notion also plays a crucial part in the provision of “culturally safe” or “secure” stroke services. Many publications stressed the importance of provider awareness of not only cultural differences traditionally associated with the concept of gaining “cultural competence,” but to shift the focus to “cultural safety,” which requires associated self-reflective humility that acknowledges historical trauma, continued power imbalances, one’s own cultural background and associated biases, and the need to create space for Indigenous Peoples to retain autonomy and self-determination.2,5,38,40,47,66,69
To this end, cultural safety programs have emerged, and some of these have been evaluated, indicating significant utility. Brewer et al. 53 developed an online course for speech and language therapists caring for Māori patients, and their evaluation found that participants gained a better understanding of health inequities, the need to self-reflect, change practice, and improve relationships and communication with Māori. Møller et al. 54 (Figure 2) used participatory action involving Indigenous elders in Canada to develop a community rehabilitation worker program. Engagement with community resulted in the prioritization of culture, tradition, spirituality, religion, mastery of native language, community re-integration, and mental health support specific to First Nation’s Elders as key aspects for workers to internalize when offering rehabilitation programs. Some service improvement activities will relate to both Indigenous and non-Indigenous communities and when involving people with lived experience of stroke it can be important to ensure membership is at least half Indigenous, instead of a “token” single person who is often then drowned out, marginalized, and dominated by the non-Indigenous members perpetuating power imbalances. A successful example of such a power-balanced, lived-experience panel took place in Aotearoa New Zealand as part of the National Stroke Clot Retrieval Service Improvement Project. 60
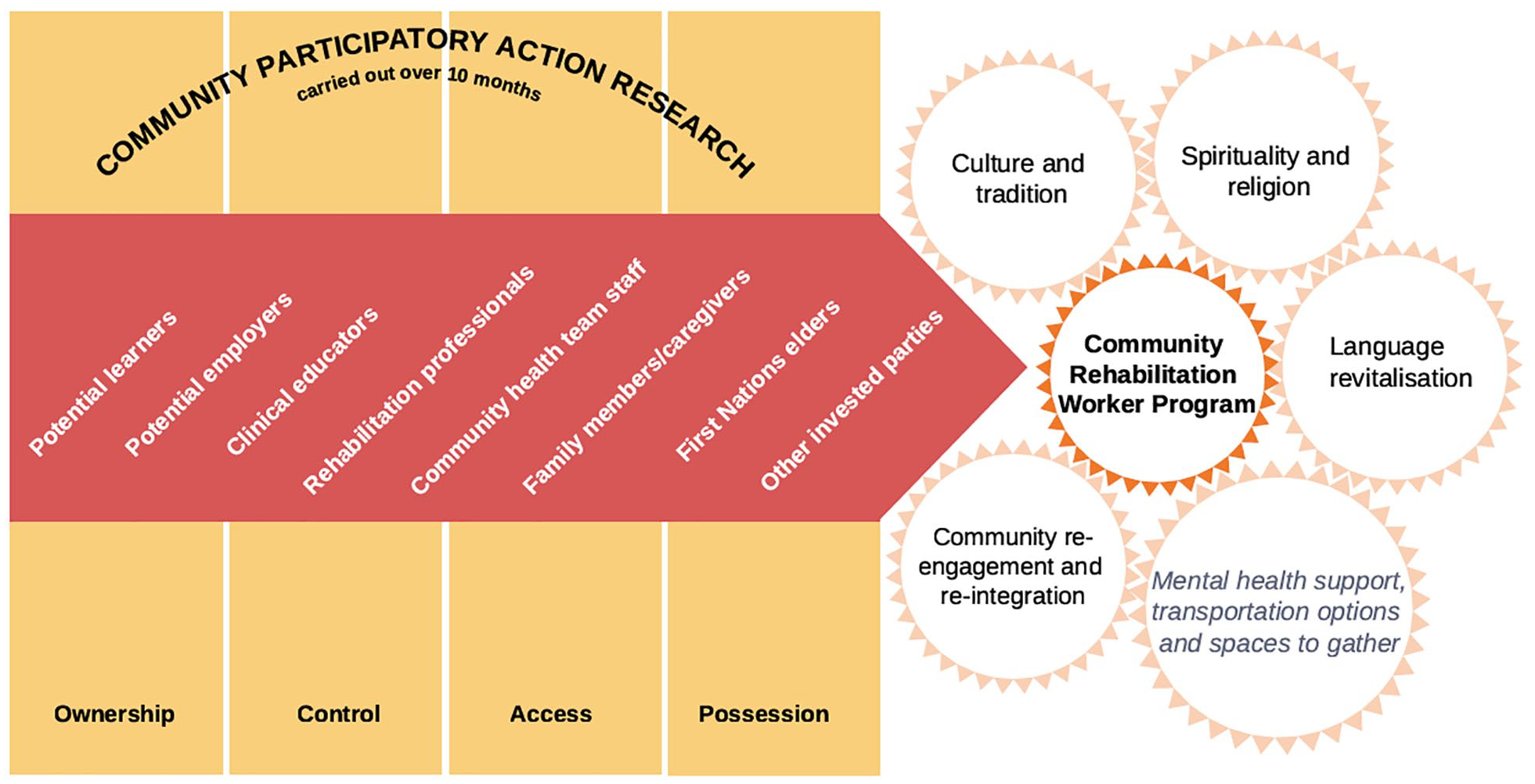
Ontario Community Stroke Rehabilitation Program.
These efforts are more effective if they are systematized, incorporated into general and preventive health care curricula, and continued during specialist stroke training. Examples of the former exist, 29 although we are not aware of any examples specific to stroke. It should be noted that attaining “cultural safety” may not be achievable in culturally incongruent settings, and for this reason some panelists proposed the terms “culturally safer” or “cultural humility” to be more appropriate moving forward.
Indigenous knowledge systems, research principles, and community-led action
It is crucial to prioritize cultural safety or cultural humility training for stroke health workers as the first step in decolonizing stroke services and taking restorative action. However, true transformative change will only occur when Indigenous health and research leadership is fully entrusted to Indigenous Peoples themselves. The importance of self-determination cannot be overstated.
As already demonstrated, Indigenous communities have existent health systems that sit within broader Indigenous knowledge systems that include their own traditionally based research methodologies. These are often entirely incongruent to the dominant analytic reductionist approaches 26 and despite tremendous advances achieved by mainstream health systems, an expectation that Indigenous Peoples completely abandon their own knowledge systems, perpetuating erasure and assimilation, is unsurprisingly viewed as paternalistic, unacceptable and inappropriate. This is especially significant as key domains, such as spirituality, connection to land, ancestry, community and wholistic well-being have been excluded from dominant models. In effect, the current imposed approach to health means well-being, as defined from an Indigenous worldview, is essentially impossible to achieve.2,69,70 Table 6 presents a comparison between the two approaches.
Comparisons of key aspects of approaches to health and health research.
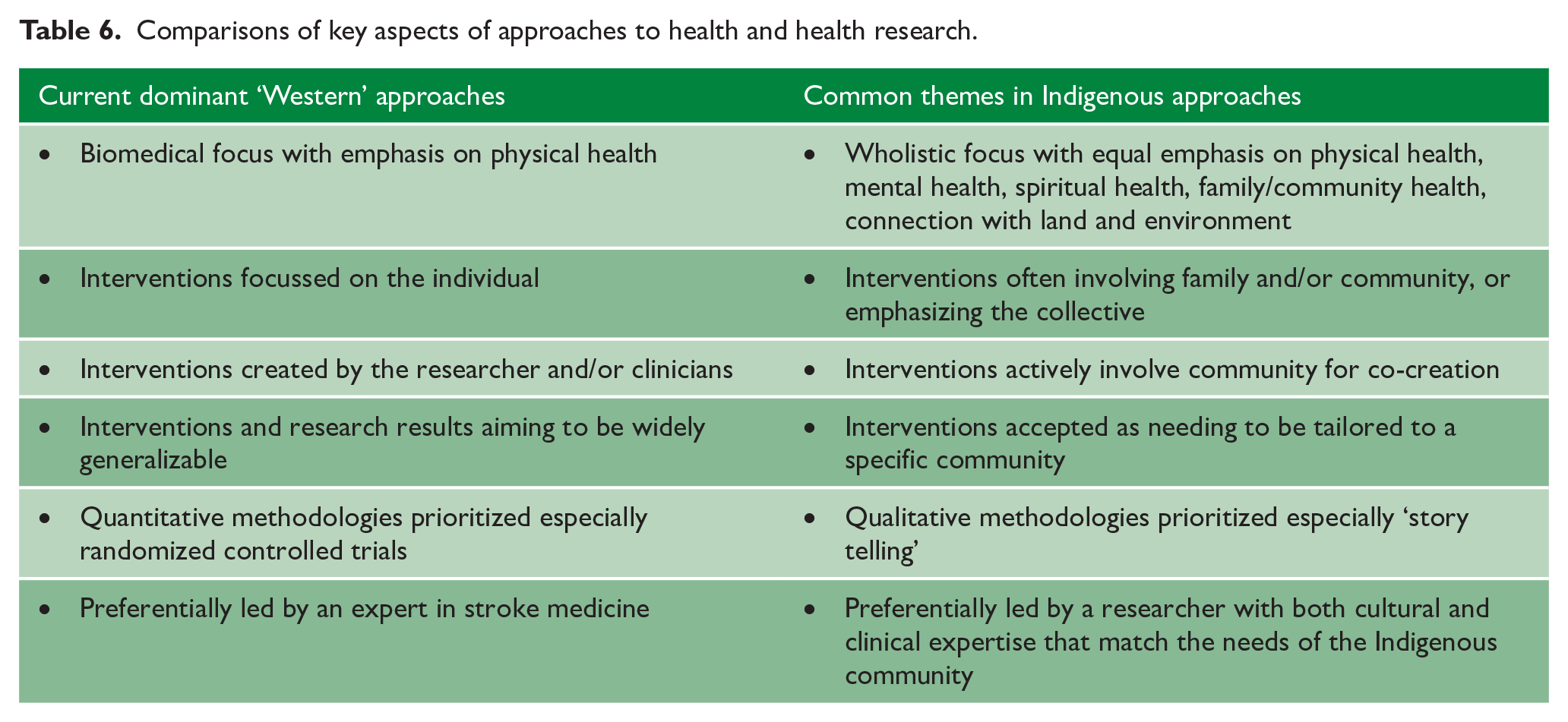
While attempts to integrate the two approaches is laudable and should be encouraged, it is also important that Indigenous Peoples have the autonomy to progress their own systems of care, using their own research methodologies, that is led by Indigenous researchers themselves.2,66,69,70 The concept of community-led research is critical in the Indigenous space. Multiple studies have emphasized the need for an approach of “by Indigenous for Indigenous” instead of imposing systems designed by clinicians and researchers from the dominant health care and knowledge systems. This principle forms the foundation of many Indigenous research approaches and is well-described in the influential work on “Decolonising Methodologies” by Linda Tuhiwai Smith. 26 Two examples of Indigenous research methodologies include the Aotearoa New Zealand Kaupapa Māori framework based on earlier work by Smith et al. 85 and applied to stroke care by Eustace et al. 41 and the Australian RTY framework 87 as used by Peake et al. 45 Both tools incorporate storytelling as a data collection methodology, emphasize community participation, and other core values such as trust, relationships, and reciprocity. The application of such a framework was well demonstrated in the consideration and evaluation of the Hua Oranga outcome instrument in stroke survivors to measure more wholistic and culturally appropriate outcomes that are actually meaningful to Māori. 59 It is entirely conceivable that non-indigenous researchers would have never considered that different approaches to analyses or outcome measures may be required for culturally distinct populations. 86
To facilitate meaningful change, the dominant scientific community must consider Indigenous research as highly valuable and meaningful, and as such support these transformative research approaches if equitable outcomes in stroke services are to be achieved. 26 However, even if such support was universal, a separate major barrier to advancing these concepts is a persistent shortage of Indigenous scholars generally and in stroke care specifically. There is a wealth of evidence that diversifying the clinical workforce improves outcomes for minority populations, 88 and this has also been shown to be critical among Indigenous Peoples.89,90 Efforts such as affirmative action are often viewed as controversial or even unfair. However, this perspective emerges primarily when the historical context is not considered, inequitable outcomes are ignored, and population health is deprioritized over individual rights. These are dominant colonial perspectives that require reflection and recognition that workforce development programs should focus on effective clinical outcomes among diverse populations.
Even once an academic degree is achieved, Indigenous clinicians and researchers have to navigate a potentially unfamiliar and non-preferred paradigm and often face ongoing challenges. This relates not only to the methodologies used, but also a de-emphasis on journal publication, the individual ownership and leadership of research being devalued in collectivist participatory programs, and local publications, favored by Indigenous scholars, being viewed of less general interest by dominant academic institutions than large multi-center and multi-country research. Even simple aspects of promotion applications such as identifying international referees can be extremely challenging if their research is highly focussed on the local community. Finally, the few Indigenous researchers we do have are frequently overburdened by requests to serve on a variety of committees, projects, and studies. This leaves them with much less time for their own research priorities.
Important first steps include removing barriers for new Indigenous researchers to allow building greater capability and capacity among the Indigenous research community and training Indigenous Peoples with lived experience to contribute to and conduct their own research. It is essential to provide strong and supportive mentorship programs that advance these individuals in a culturally safe environment.
A key step for scientific communities is to value and even prioritize Indigenous research and methodologies for stipend and grant funding allocation, journal publication, and conference presentations. At a minimum, funders and journals could ensure adequate reporting guidelines are followed when funding, reviewing, or publishing research involving Indigenous Peoples. 29 The CONSIDER guideline is an excellent option for journals to adapt as it incorporates all of the above outlined principles. 29
Achieving local acceptance versus striving for wide Generalizability
One of the key challenges in Indigenous stroke care and research is the conflict between prioritizing local development and ownership on one hand and on the other, a desire for large sample sizes, across wide reaching geography, to achieve greater study power and generalizability. The former better meets the Indigenous community needs, the latter achieves higher scientific community accolades and potentially greater and more efficient scientific impact. The need for local ownership is partly driven from local differences that, perhaps, are more important in a model that focusses less on biomedical and more on social mechanisms of health and well-being. 26 Ignoring these factors is problematic when imposing interventions on an Indigenous community. However, undoubtedly there is also a component of distrust when it comes to introducing models developed by outsiders who have historically taken rather than shared and while large scale multi-national randomized controlled trials may result in very accurate scientific data, the impact will be massively curtailed if the results are not accepted by local communities.7,75,76 This may, in fact, explain some of the delays in knowledge translation across other marginalized communities globally and contribute to widening disparity gaps in some areas.
Perhaps the optimal approach is to continue with large scale studies, but place more effort on partnering with Indigenous Peoples, including those with lived experience, from the start to give them a voice when it comes to designing interventions and also determining meaningful outcome measures. The dominant scientific community could also consider being more open to allowing amendments to non-Indigenous “evidence-based treatments” to meet local needs without always demanding additional costly randomized controlled trial evidence. For example, as observed during the pandemic, Indigenous-led health approaches were leveraged to support direct healthcare for community members. 91 More importantly, clinicians and academics need to place more value on resourcing and testing novel interventions within an Indigenous research framework before forcing local adaptation or dismissing the lack of adoption of non-Indigenous medicine as attributable to limited understanding.
These are challenging concepts, but they will need to be considered and embraced if there is a genuine desire to help improve Indigenous health and achieve equity in stroke outcomes.
Recommendations
The totality of the literature we reviewed emphasizes the need for innovation and transformative change in our approach to Indigenous Peoples at risk of and experiencing stroke by acknowledging historical and societal context as well as cultural differences and being more open toward incorporating Indigenous knowledge systems. This along with the need for locally tailored and culturally specific approaches to stroke care preclude sweeping recommendations advocating for a specific intervention or approach. Rather, there is a need for underpinning values and principles on how the stroke community ought to approach Indigenous Peoples with stroke and their supporting communities.
A recent international roundtable proposed a set of such core values for managing Indigenous Peoples with acquired communication disorders, predominantly stroke, that nicely summarizes the concepts discussed in detail above. 67 We have adapted these values slightly to provide a solid foundation to guide broader stroke care in Indigenous Peoples:
Acknowledgment and recognition of ongoing inequity.
Reflective practice by stroke practitioners regarding assumptions built into practice.
Trust and relationship building.
Incorporate cultural understandings relating to extended family, community, and local cultural protocols into routine clinical practice.
Two-way dialogue between service providers and communities.
Recognize that health initiatives involving Indigenous communities should be led by Indigenous Peoples.
Based on the presented literature and supported by their own experience, the panel makes the following recommendations to drive effective service improvement and research activities:
While recognizing the strengths and resilience of Indigenous Peoples, openly acknowledge current inequities and focus on achieving equitable access to high-quality stroke services for Indigenous Peoples globally;
Encourage a more wholistic model of stroke care for Indigenous Peoples that emphasizes wellness and stroke prevention in collaboration with primary care, community providers and Indigenous communities;
Address current knowledge gaps and develop, evaluate, and implement systems of care that promote culturally safe stroke care environments across all phases of stroke care that meet the local needs of Indigenous Peoples and incorporate Indigenous approaches;
Provide systematic cultural safety training for all stroke care staff, including active development of healthcare curriculum content on locally relevant Indigenous history, culture, knowledge system, and cultural safety;
Improve cross-cultural communication and educational materials using a co-design methodology with Indigenous communities during development to meet cultural expectations;
Increase workforce capacity and capability of Indigenous health providers, researchers, administrative health workers, and scholars, as well as Indigenous Peoples with lived experience of stroke including funding support and mentorship;
Disaggregate and achieve reliable Indigenous data to accurately describe and monitor Indigenous stroke burden;
Incorporate Indigenous data sovereignty guidelines across collection and control of all Indigenous stroke data, which includes evaluating traditional Indigenous medicinal knowledge using safe, respectful, ideally Indigenous-led approaches that adhere to intellectual property standards;
Prioritize Indigenous research for funding, publication, and conference content rewarding or even mandating use of Indigenous Research Frameworks, with a focus on projects being community and Indigenous led;
Increase rigor around funding and publication reporting guidelines for Indigenous research that meet CONSIDER (or similar) standards and adhere to the concepts such as reciprocity and self-determination.
Finally, we call for organizations to actively support collaboration between Indigenous and non-Indigenous Peoples with lived experience, clinicians, and researchers from different geographic locations across the globe, to actively explore ways to address tensions between dominant scientific and Indigenous knowledge systems including the “locally grown” versus “optimized generalizability” challenge. (Figure 3)
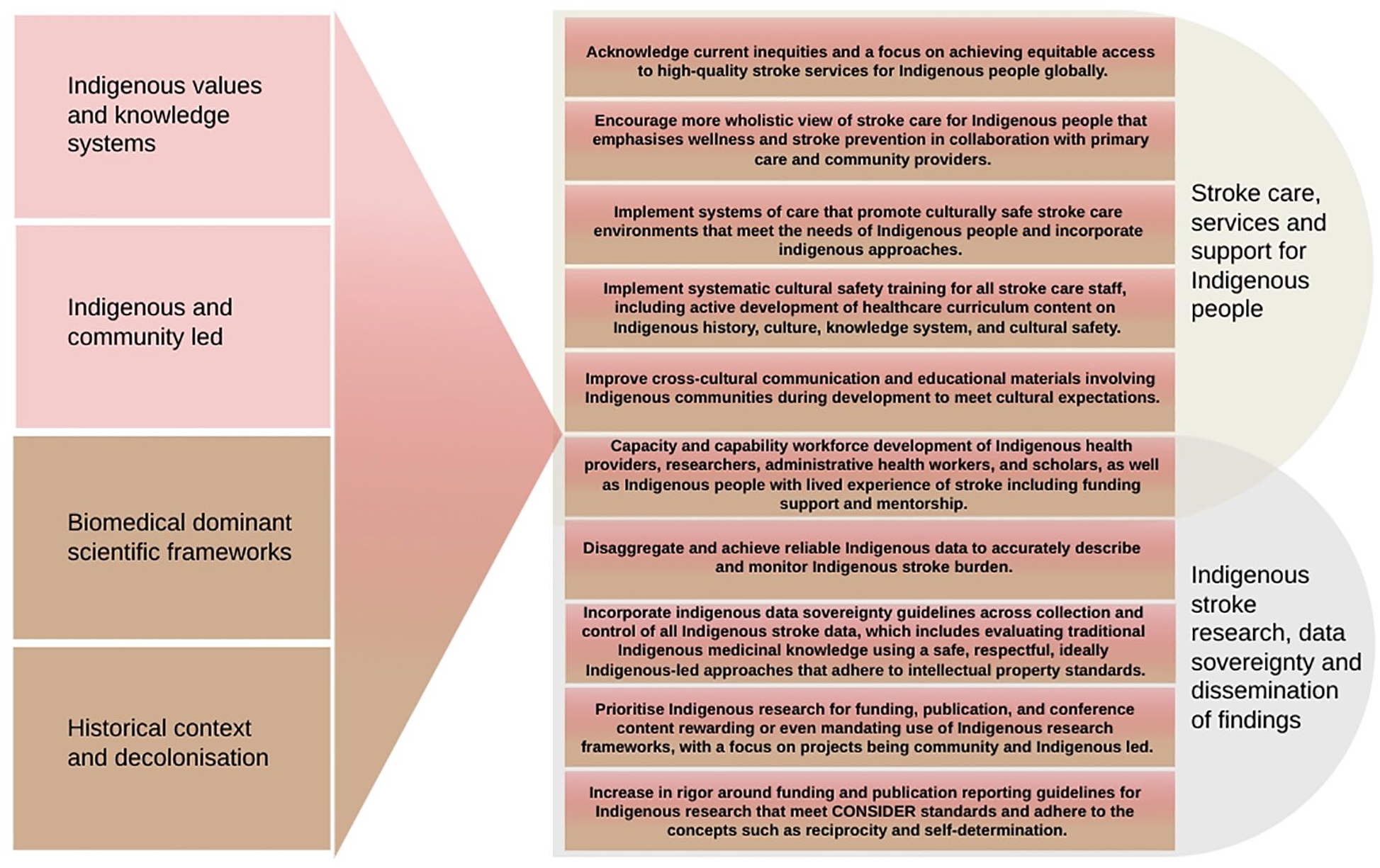
Summary of Key Recommendations.
In addition to the above clinical and stroke research priorities, it is important to bear in mind that many social determinants of health, such as a safe living environment, education, access to clean water and affordable food, play a critical role in vascular health. Current systemic discrimination often reaches beyond the health into the social and political sector. We should, within our roles in the stroke community, acknowledge these issues as intrinsically unfair and advocate finding solutions at individual or organizational levels. Of importance, the issues discussed in this article focus on common themes identified via our literature search across Indigenous populations, but some aspects will not universally apply and there will always be important differences between these diverse cultures to consider. All broad recommendations need to be considered within the local context.
We also acknowledge that many of the above principles may also be relevant to other marginalized populations and those from different cultures who have immigrated to a new country. We encourage others to apply these principles to these broader populations as appropriate. However, it is equally important to recognize that Indigenous Peoples have a unique experience in the way that changes were forced upon them by others invading their lands and imposing their culture. Many Indigenous Peoples have been subjected to extreme forms of forced assimilation, cultural extinction or near extinction, and systematic abuse. This has resulted in extreme distrust of the dominant culture. The dominant cultures have designed and govern current health systems and to rebuild the trust that has been destroyed the outlined recommendations are especially critical.
We believe that through open, genuine, trustworthy, respectful, and culturally safe engagement, Indigenous and non-Indigenous researchers and practitioners can build strong collaborative relationships locally, regionally, nationally, and internationally to learn from each other and achieve high-quality and equitable stroke care and outcomes for all people.
Footnotes
Acknowledgements
The authors thank Dr. Med, PhD Ann Ragnhild Broderstad (Skáit-Erna Ánne-Rávdná) and researcher, PhD Inger Johanne Dagsvold (Jusságohpi Piera-Niillasa-Márjja-Inger) from the Center of Sámi Health Research at The Arctic University of Norway in Tromsø (Norway) who supported and advised panel member Susanna Ragnhild Andersdatter Siri (Fimbenáilluántte ja Gárenniillasmáhte Susánna) during this work. In addition, they would like to acknowledge the contribution of Ms Janice Kang who provided administrative support in the preparation of this manuscript including with literature searches and figure design.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.