
Abstract
Background:
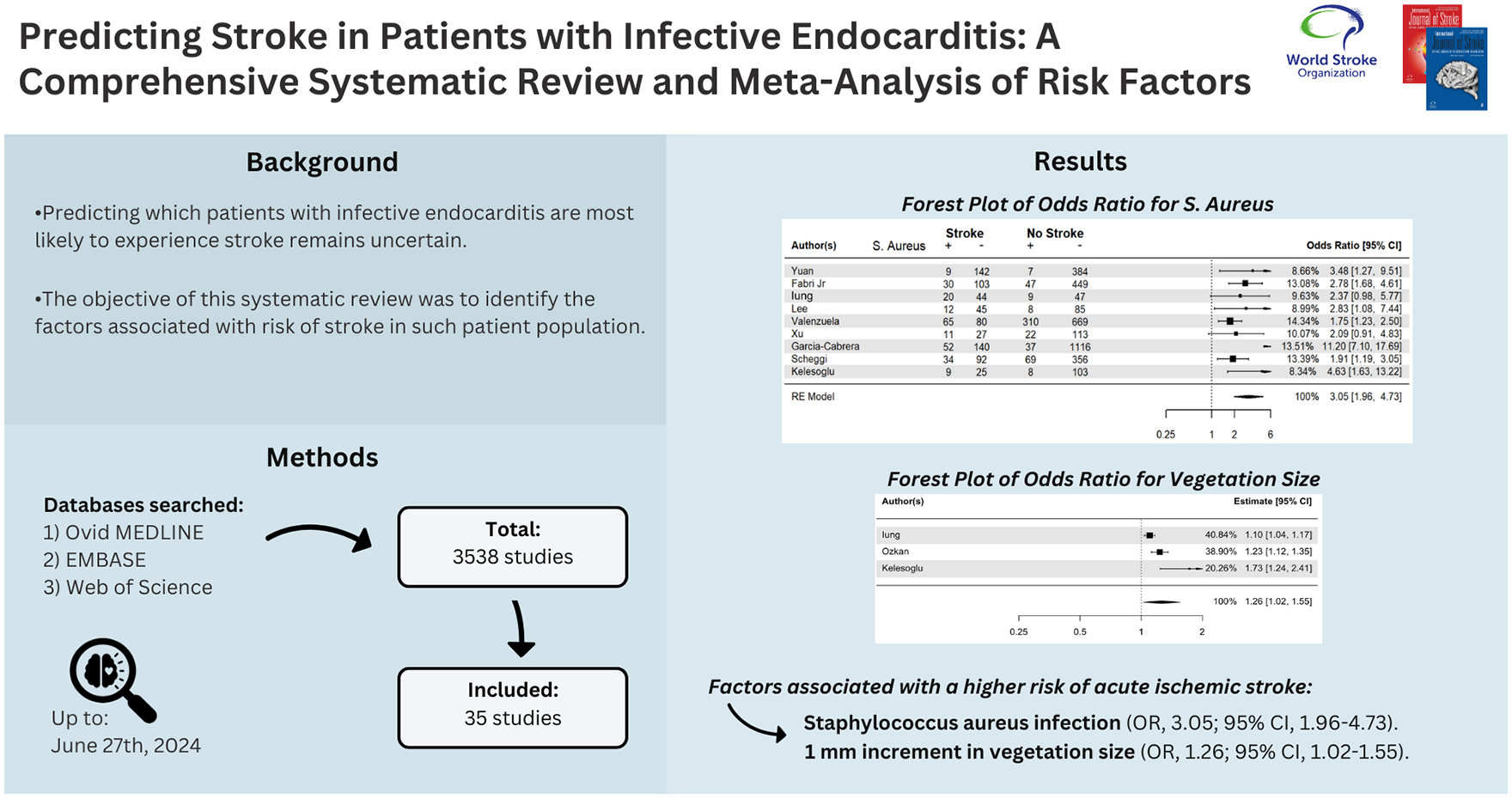
Neurological complications in patients with infective endocarditis (IE), such as ischemic and hemorrhagic stroke, are well described; however, predicting which patients are most likely to experience stroke remains uncertain.
Aims:
We conducted a systematic review and meta-analysis to identify the factors associated with the risk of stroke in patients hospitalized with IE.
Methods:
A systematic search of Ovid MEDLINE, EMBASE, and Web of Science up to 27 June 2024 was conducted. Articles evaluating risk of acute ischemic stroke (AIS) or intracranial hemorrhage (ICH) in patients with IE were included. Meta-analysis of odds ratios was feasible for only some predictive factors due to study heterogeneity. Cochrane’s Risk of Bias in Non-Randomized Studies of Exposure tool was used for risk-of-bias assessment.
Summary of Review:
Of 3538 studies identified, 35 were included: 9 prospective and 26 retrospective cohort. Staphylococcus aureus infection (odds ratio (OR) 3.05; 95% CI, 1.96–4.73, I2 = 77.2%; 9 studies) and 1-mm increment in vegetation size (OR, 1.26; 95% CI, 1.02–1.55, I2 = 90.1%; 3 studies) were associated with a higher risk of AIS, after adjusting for other covariates. High-intensity signals on transcranial Doppler, and comorbidities such as hypertension, atrial fibrillation, and hyperlipidemia were also found to be associated with a higher risk of AIS. The risk of ICH was increased by thrombocytopenia, mycotic aneurysms, prior ICH or AIS, and cerebral microbleeds.
Conclusion:
Our study has identified factors which are associated with increased stroke risk in IE and may help physicians predict risk. While echocardiographic and neuroimaging findings may be particularly informative, underlying comorbidities and various laboratory values may also contribute to predicting IE-associated strokes.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.