
Abstract
Background:
Among non-communicable disorders (NCDs), stroke remains the second leading cause of death and the third leading cause of death and disability combined (as expressed by disability-adjusted life-years lost—DALYs) in the world.
Aims:
The study was aimed to estimate global, regional and nationa burden of stroke and its risk factors from 1990 to 2021.
Methods:
Finding presented in this paper were derived mainly from the Global Burden of Disease 2021 Study on stroke burden published in The Lancet Neurology 2024:23:973-1003.
Results:
The estimated global cost of stroke is over US$890 billion (0.66% of the global GDP). From 1990 to 2021, the burden (in terms of the absolute number of cases) increased substantially (70.0% increase in incident strokes, 44.0% deaths from stroke, 86.0% prevalent strokes, and 32% DALYs), with the bulk of the global stroke burden (87.0% of deaths and 89.0% of DALYs) residing in lower-income and lower-middle-income countries (LMICs). Stroke attributable to metabolic risks constituted 69.0% of all strokes, environmental risks constituted 37.0%, and behavioral risks constituted 35.0%.
Conclusion:
This World Stroke Organization (WSO) Global Stroke Fact Sheet 2025 provides the most updated information that can be used to inform communication with all internal and external stakeholders; all statistics have been reviewed and approved for use by the WSO Executive Committee and leaders from the Global Burden of Disease research group.
Overview
The most recent Global Burden of Disease (GBD) 2021 stroke burden estimates 1 showed that among non-communicable disorders (NCDs), stroke remains the second leading cause of death (about 7 million) and the third leading cause of death and disability combined (as expressed by disability-adjusted life-years lost—DALYs; over 160 million DALYs) in the world. This is the most comprehensive GBD stroke epidemiology study to date, and showed that the number of people who suffer a stroke, die from, or live with a disability after a stroke has risen substantially worldwide between 1990 and 2021: incident strokes—by 70% (95% UI 66 to 75), deaths from stroke—by 44% (32 to 56), and DALYs—by 32% (22 to 43), with the bulk of the global stroke burden (87.2% of deaths and 89.4% of DALYs) residing in low-income and low-middle-income countries (LMICs). The estimated global cost of stroke is over US$890 billion (0.66% of the global GDP) per year, and is projected to almost double by 2050. 2
In 2021, there were 93.8 million (89.0 to 99.3) prevalent and 11.9 million (10.7 to 13.2) incident strokes. The study found disparities in stroke burden and risk factors by GBD region, country or territory, and sociodemographic index (SDI), and a stagnation in the reduction of incidence from 2015 onward, and even some increases in the stroke incidence, death, prevalence, and DALY rates in southeast Asia, east Asia, and Oceania, countries with lower SDI, and people younger than 70 years of age. 1 Globally, ischemic stroke (IS) constituted 65.3% (62.4 to 67.7), intracerebral hemorrhage (ICH) constituted 28.8% (28.3–28.8), and subarachnoid hemorrhage (SAH) constituted 5.8% (5.7 to 6.0) of incident strokes, with the highest proportion of IS in high-income countries (HICs 74.9% (72.3 to 84.1) vs 63.4% (53.6 to 73.7) in LMICs) and ICH in LMICs (31.1% (30.2 to 31.3) vs 17.8% (17.3 to 17.9) in HICs). The proportion of SAH in HICs (7.3% (7.2 to 8.3)) was higher than that in all LMICs combined (5.5% (5.4 to 5.7)). Among incident stroke, 6.3 million (95% UI 5.6 to 7.0); or 52.6% (52.4 to 53.1)) occurred in males and 5.7 million (5.1 to 6.3); or 47.4% (47.3 to 47.6)) in females.
The study also showed that stroke is highly preventable, with 84% of the stroke burden in 2021 attributable to 23 modifiable risk factors, including high blood pressure, air pollution, excess body weight, smoking, and physical inactivity—presenting a public health challenge and an opportunity for action. While from 1990 to 2021 there was a positive trend in the reduction of population-attributable fraction (PAF) of stroke DALYs due to diet high in sodium (−4.6% (−25.1 to 2.8)), smoking (−12.8% (−19.5 to −6.0)), secondhand smoking (−12.8% (−16.5 to −8.8)), diet low in fruits (−13.5% (−16.5 to −9.5), ambient particulate matter pollution (−20.4% (−27.3 to −12.9)), low ambient temperature (−20.8% (−24.7 to −16.9)), diet low in fiber (−25.1% (−31.0 to −19.0)), diet low in vegetables (−30.3% (−36.5 to −21.6)), and diet high in processed meat (−40.1% (−45.3 to −33.3)), there were substantial increases in DALYs attributable to high body mass index (BMI; 88·2% (53.4 to 117.7)), high ambient temperature (72.4% (51.1 to 179.5)), high fasting plasma glucose (32.1% (26.7 to 38.1)), diet high in sugar-sweetened beverages (23.4% (12.7 to 35.7)), low physical activity (11.3% (1.8 to 34.9)), high systolic blood pressure (6.7% (2.5 to 11.6)), lead exposure (6.5% (4.5 to 11.2)), and diet low in omega-6 polyunsaturated fatty acids (5.3% (0.5 to 10.5)). 1 Stroke attributable to metabolic risks constituted 68·8% (95% UI 57.6 to 77.5) of all strokes, environmental risks constituted 36.7% (29.0 to 44.2), and behavioral risks constituted 35.2% (26.9 to 44.7).
The study findings of the large global effect of high outdoor temperatures on stroke burden are of significant importance for public health, especially for elderly people. Between 2000–2004 and 2017–2021, the heat-related mortality from all causes in people older than 65 years has increased by approximately 85%. 3 Just in 2021, high outdoor temperature, globally, was responsible for almost 2 million DALYs from stroke, particularly in North and Central Africa, Middle East, and South Asia. 1 For the first time, the GBD 2021 study revealed the high contribution of particulate matter air pollution to SAH (14.2% (9.8 to 18.0) of SAH-related DALYs). 1
This WSO Global Stroke Fact Sheet 2024 provides the most updated information that can be used to inform communication with all internal and external stakeholders; all statistics have been reviewed and approved for use by the WSO Executive Committee and leaders from the GBD research group. The facts that are endorsed by the WSO will be updated every 1–2 years as new data emerge. Infographics of stroke burden and risk factors in the world is presented in Figure 1.
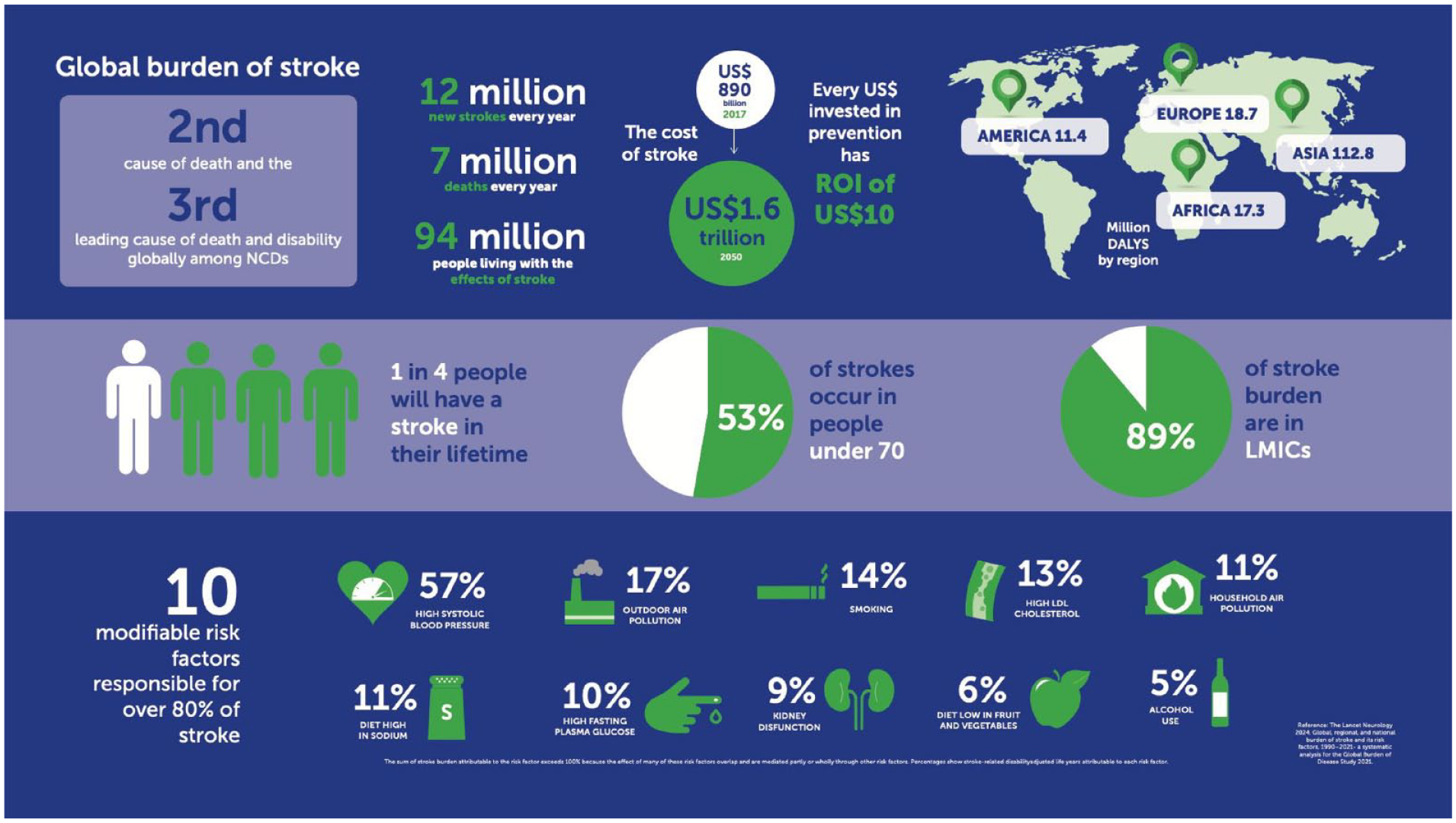
Infographics of stroke burden and risk factors in the world.
Methods
The values contained in this Fact Sheet have all been extracted from the most current GBD publication on stroke burden in The Lancet Neurology 1 (Tables 1 to 5) and online GBD Visualization Tool (http://ghdx.healthdata.org/gbd-results-tool).
GBD 2021 estimates for global incidence, prevalence, mortality, and DALYs for all stroke types combined.
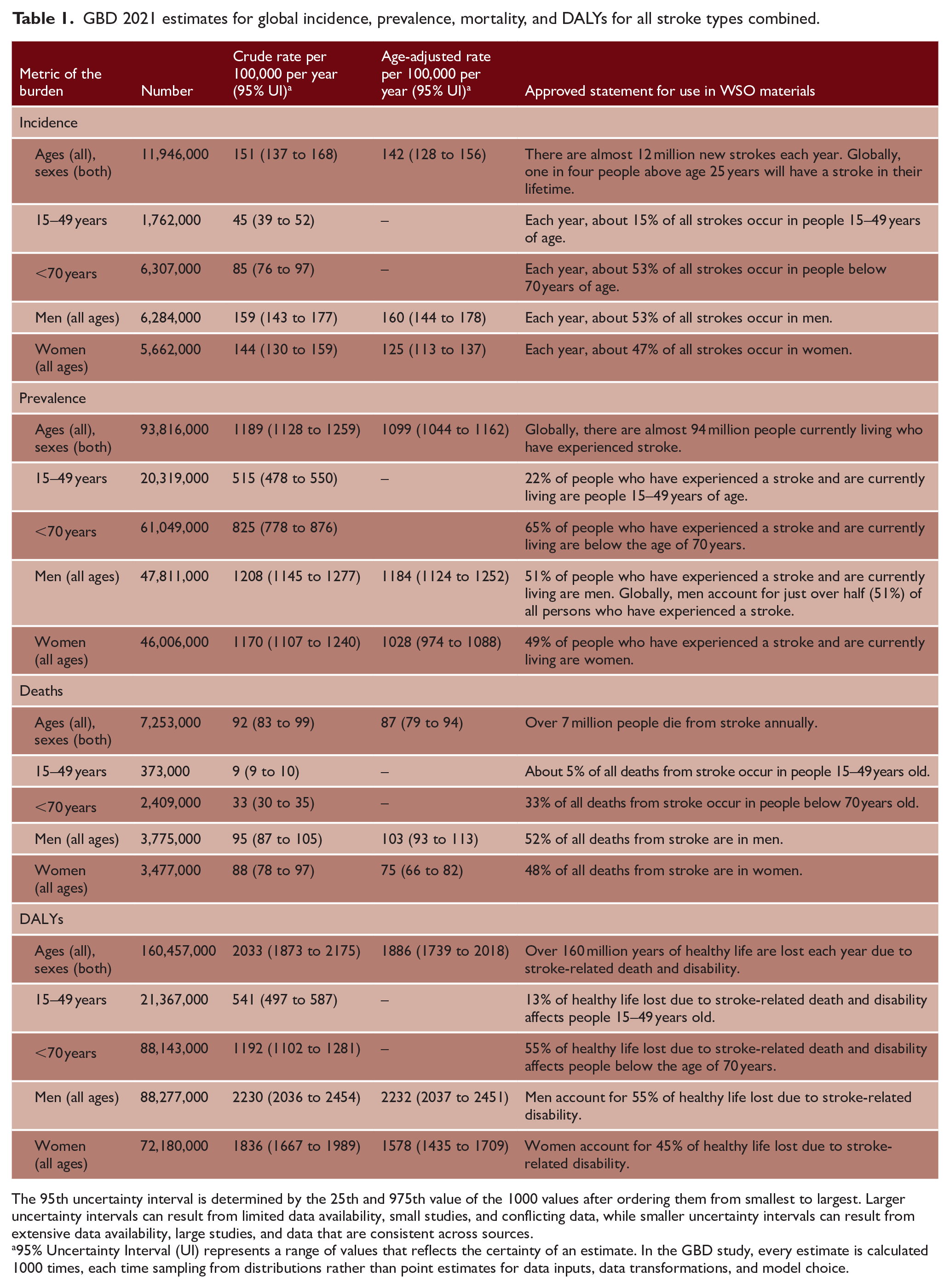
The 95th uncertainty interval is determined by the 25th and 975th value of the 1000 values after ordering them from smallest to largest. Larger uncertainty intervals can result from limited data availability, small studies, and conflicting data, while smaller uncertainty intervals can result from extensive data availability, large studies, and data that are consistent across sources.
95% Uncertainty Interval (UI) represents a range of values that reflects the certainty of an estimate. In the GBD study, every estimate is calculated 1000 times, each time sampling from distributions rather than point estimates for data inputs, data transformations, and model choice.
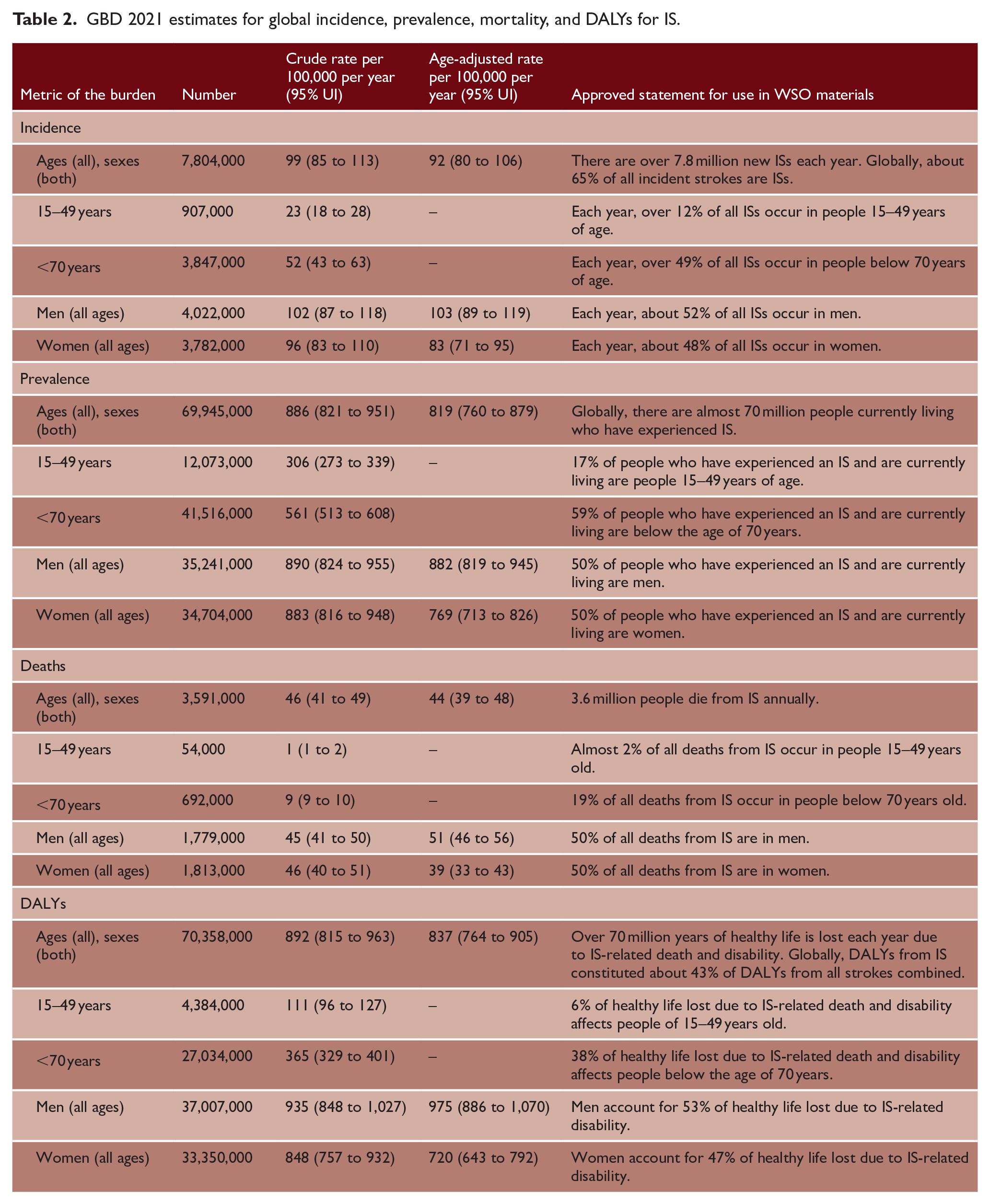
GBD 2021 estimates for global incidence, prevalence, mortality, and DALYs for IS.
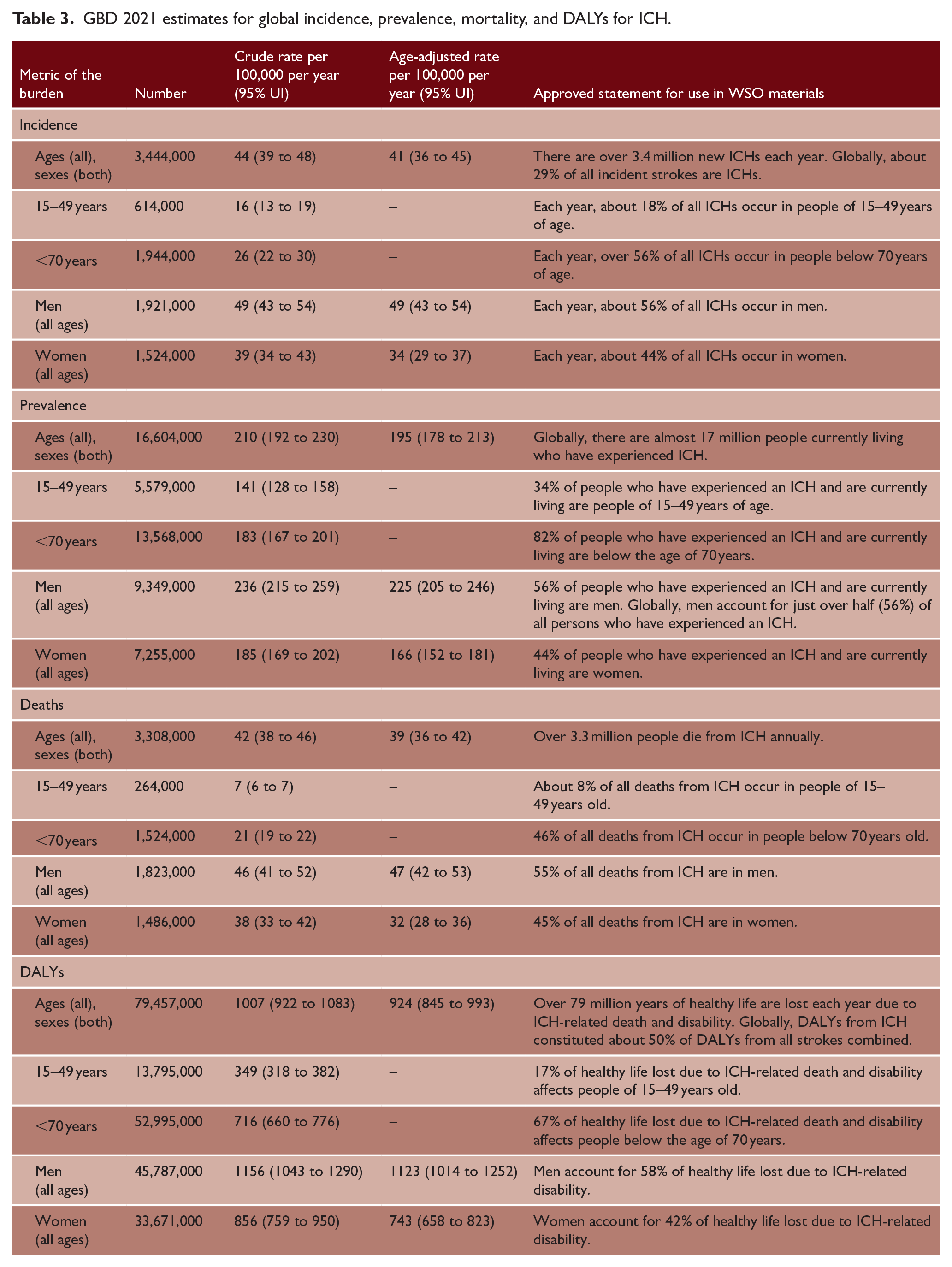
GBD 2021 estimates for global incidence, prevalence, mortality, and DALYs for ICH.
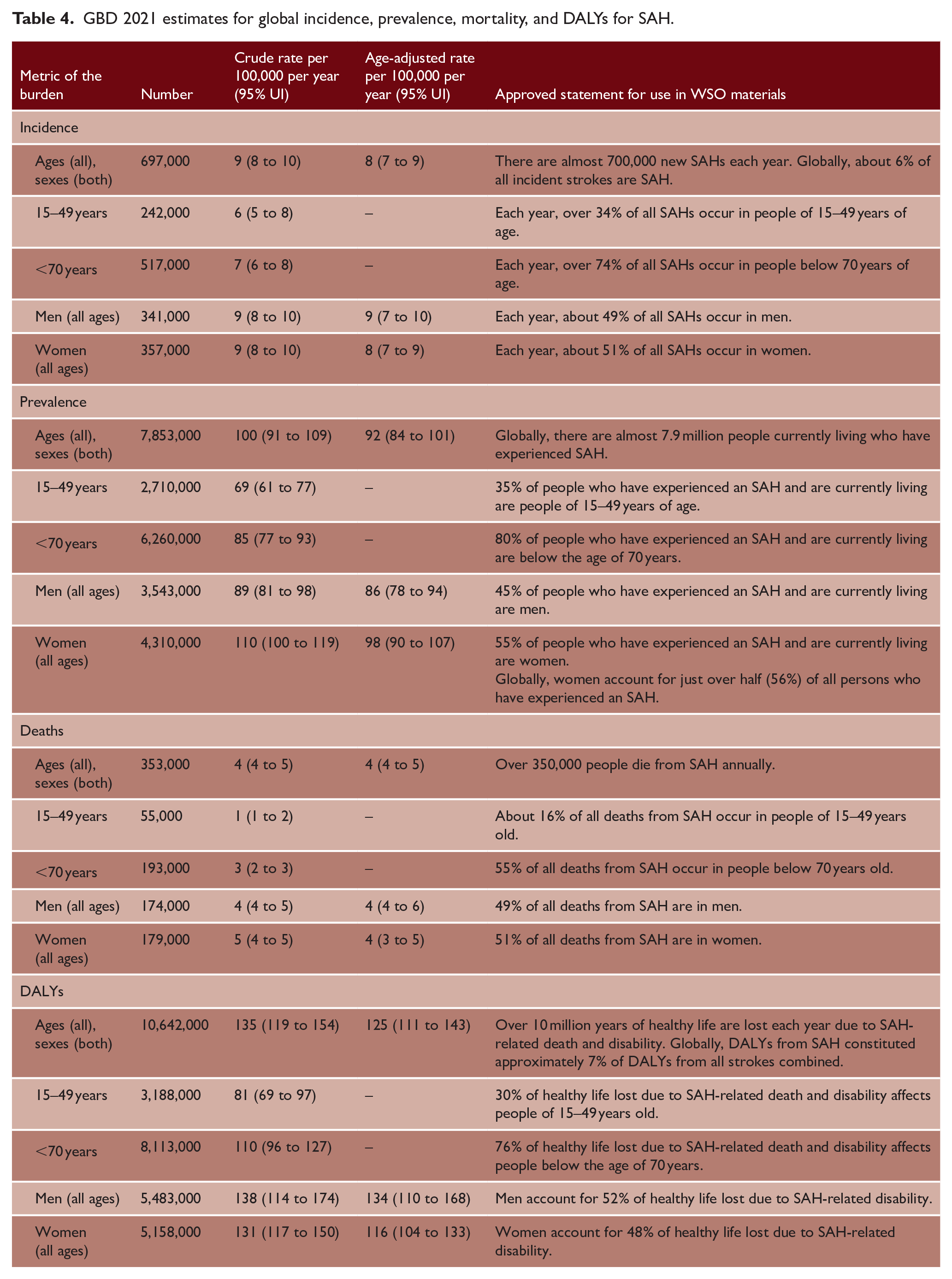
GBD 2021 estimates for global incidence, prevalence, mortality, and DALYs for SAH.
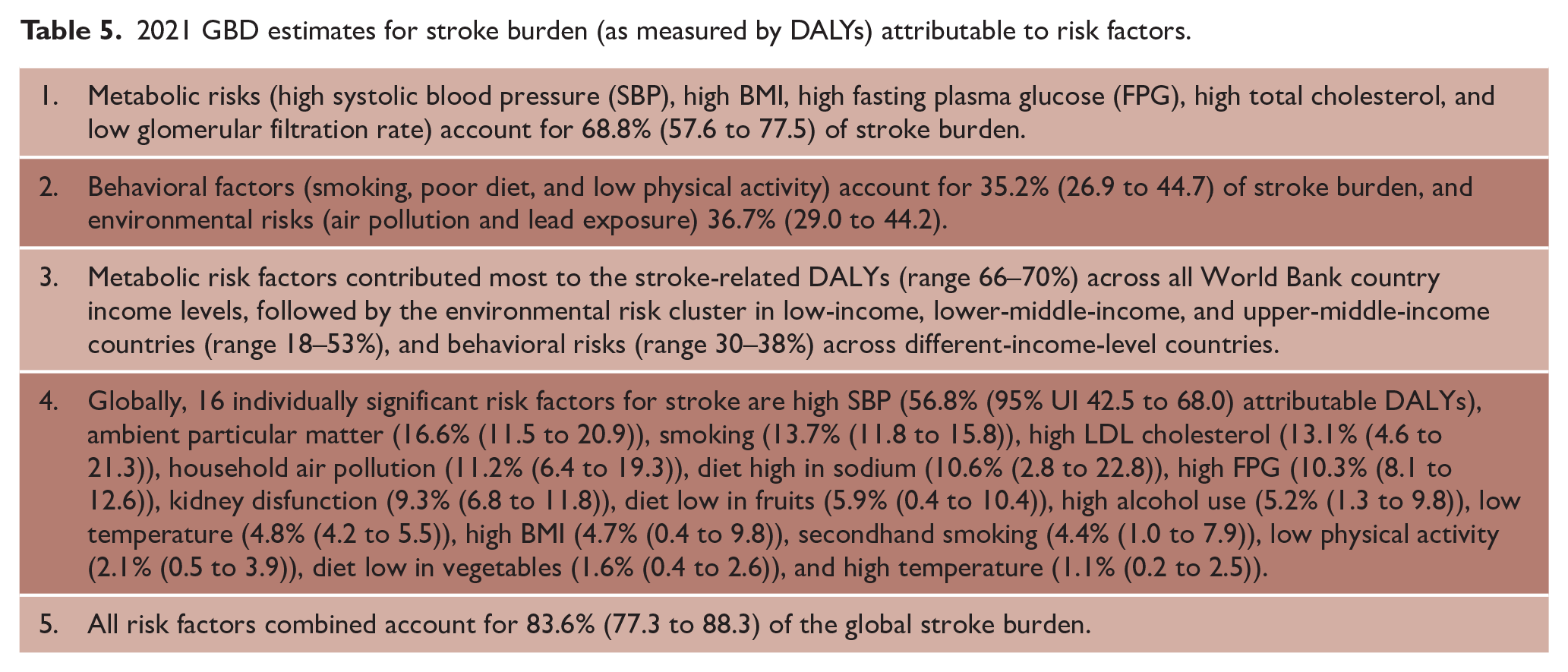
2021 GBD estimates for stroke burden (as measured by DALYs) attributable to risk factors.
Discussion
As for all GBD updates, the latest GBD 2021 stroke burden estimates supersede all previously published stroke burden estimates. The GBD 2021 findings showed that although overall global age-standardized stroke incidence, prevalence, death, and DALY rates have reduced around the world, an aging population and population growth together with unfavorable trends in the PAF of some major risk factors (such as high BMI, high ambient temperature, high fasting plasma glucose, diet high in sugar-sweetened beverages, low physical activity, high SBP, lead exposure, and diet low in omega-6 polyunsaturated fatty acids) have continued to push the total burden in terms of absolute numbers ever higher, which threatens to overwhelm the health care system over the coming decades. However, the analysis also suggests that a lack of, and unequal access to, high-quality prevention, acute, and rehabilitation services is significant, especially in low- and middle-income countries. To improve stroke prevention, we need (1) improved awareness of stroke and stroke risk factors; (2) better and more equitable access to prevention services and support; (3) more support at the societal, individual, public health, and economic levels to felicitate behavioral change; and (4) more research in stroke prevention in different populations.
The WSO/Lancet Neurology Commission on Stroke 2 forecasts that globally, between 2020 and 2050, deaths from stroke will increase by 50% (from 6.6 million people per year to 9.7 million), with the bulk of the burden (77% prevalent, 87% fatal strokes, and 89% DALYs due to stroke) residing in low- to middle-income countries. 1 The number of people who die from stroke or are disabled by it has almost doubled in the last three decades and, worldwide, stroke is (1) the second leading cause of death; (2) the third leading cause of death and disability combined (DALYs); and (3) one of the main causes of dementia. 2 These GBD 2021 stroke burden estimates are of crucial importance for evidence-based health care planning, prevention, resource allocation, priority setting, and stroke advocacy.
The GBD 2021 study emphasizes that currently used stroke prevention strategies are not sufficiently effective to halt, let alone reduce, the fast-growing stroke burden. Additional measures to reduce stroke burden were recently outlined by the WSO—Lancet Neurology Commission on Stroke 2 and include evidence-based pragmatic recommendations to reduce the global stroke burden, including measures to improve stroke surveillance, prevention, acute care, and rehabilitation. Key recommendations include as follows: (1) Establishing low-cost surveillance systems to provide accurate epidemiological stroke data to guide prevention and treatment; (2) Raising public awareness and action to improve healthy lifestyles and prevent stroke through population-wide use of mobile and digital technologies, such as training and awareness-raising videos and apps; (3) Prioritizing effective planning of acute stroke care services (Figures 2 and 3), capacity building, training, provision of appropriate equipment, treatment and affordable medicines, and adequate resource allocation at national and regional levels; (4) Adapting evidence-based recommendations to regional contexts, including training, support, and supervision of community health workers to assist in long-term stroke care; and (5) Establishing local, national, and regional ecosystems involving all relevant stakeholders to co-create, co-implement and monitor stroke surveillance, prevention, acute care, and rehabilitation. Without scaling up these innovative evidence-based strategies and policies that target local, national, regional, and global stroke prevention and care disparities, the burden of the stroke continues to grow, thus threatening the sustainability of the health system across the globe.
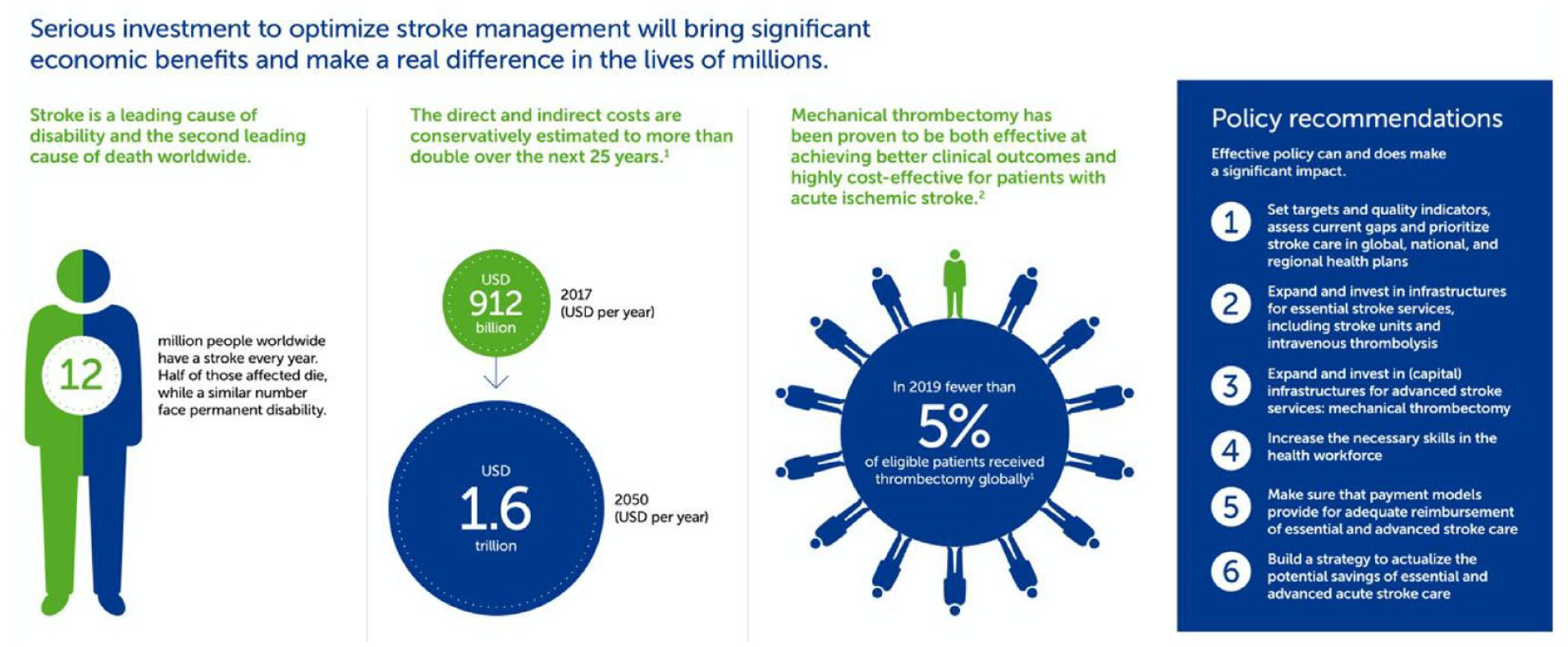
Time for a revolution in stroke care.
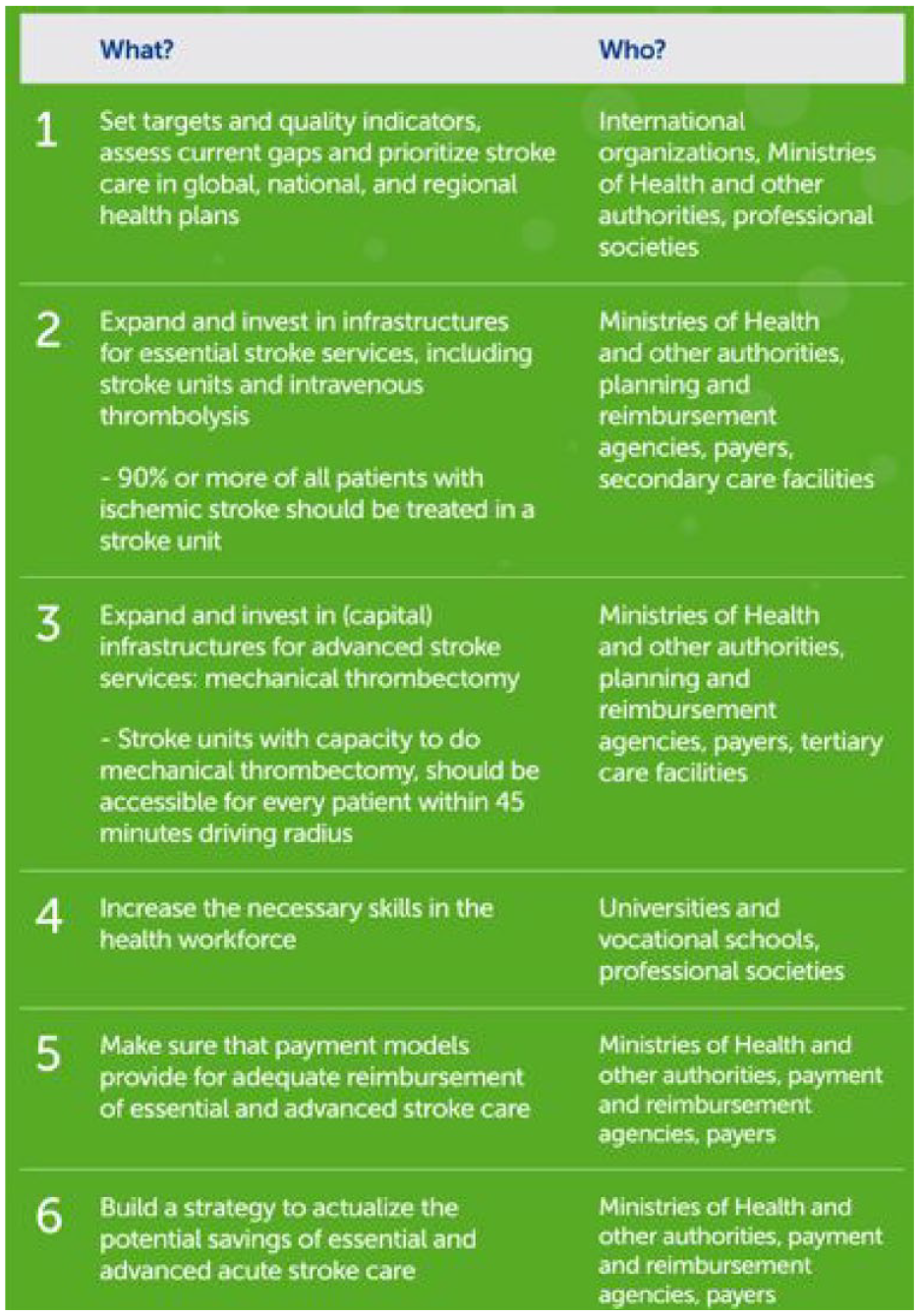
A collaborative policy agenda for better stroke care.
The WSO outlines key challenges and opportunities to reduce the global burden of stroke through evidence-based interventions at policy and health care system level. The brief draws on WHO NCD Policy Best Buys 4 and the WSO–Lancet Neurology Commission “Pragmatic solutions to reduce the global burden of stroke.” 2 These documents set out key actions that will assist governments to deliver on their commitments on reduction of non-communicable disease (NCD) and identified a series of evidence-based prevention interventions for policy makers that, if implemented across the globe, would reverse the trajectory of stroke burden through effective prevention, treatment, and rehabilitation strategies.
Primordial stroke prevention is about tackling and reducing the risk factors for stroke before they are manifested in individuals as conditions, such as high blood pressure or diabetes. It involves creating the social and economic conditions in which societal factors that increase stroke risk are tackled. Around the world, governments have initiated awareness and educational campaigns on anti-smoking, or healthy eating, for example. These initiatives have largely been targeted at changing individuals’ behaviors and are an important part of the mix of primordial prevention interventions that governments can make. However, they are only part of the picture.
As Carol Brayne argued in The Lancet Neurology Anniversary Lecture 2022, 5 targeting individual-level intervention “ignores the magnitude of influence that commercial influences, social environment, and material circumstances have on options, opportunities, and behaviours.” The Lancet adds in their editorial: “Addressing the social and commercial determinants of neurological health is an essential component for tackling the burden of stroke that should not be overlooked.” 6 Social and commercial determinants include poverty, air pollution from traffic and industry; the costs and availability of healthy foods versus highly processed foods; urban design that inhibits exercise and exposes people to air pollution; inequality; and people’s access to information and education about stroke risk. To tackle the increased risk of stroke caused by pollution, governments could (1) regulate vehicle/industry emissions; (2) restrict traffic in urban areas (e.g. low-emission zones); (3) improve public transport and promote green transport, cycling, and walking; and (4) incentivize the use of clean-energy economy, cleaner fuels in the home and for cooking (e.g. indoor air pollution has been substantially reduced in India through government subsidies on cooking gas).
The World Health Organization (WHO) argues that: “At the root of many of the world’s most pressing threats to human, animal and planetary health, are unhealthy, inequitable and unsustainable food systems. Around 11 million deaths are caused by unhealthy diets annually. Our diets have become the leading contributor to global environmental degradation, affecting land, water and oceans, biodiversity, our climate and our air quality.” 7 Measures that governments could take to reduce stroke risk caused by unhealthy diets include: (1) subsidies for fruit and vegetables; (2) financial measures, such as sugar and alcohol taxes; (3) reducing salt in processed food; (4) tackling fast food through licensing and pricing; (5) clear food labeling; (6) banning of unhealthy ingredients, such as trans-fats; (7) regulating the amounts of salt, sugar, and fat in processed foods; (8) providing healthy menus (e.g. unprocessed plant-food choices) in all public facilities; (9) phasing out industrialized animal farming; (10) strengthening the regulation of food production, advertising, and marketing; and (11) information and education campaigns. Governments can also encourage urban planning that (1) makes taking exercise easier and improves “walkability”; (2) provides green space and reduces population density; (3) separates people from cars and trucks; (4) ensures that housing and schools are built away from roads and pollution-emitting industry; and (5) limits/licenses fast food outlets by district.
WSO-recommended government measures to reduce smoking include: (1) awareness campaigns; (2) bans on tobacco advertising; (3) age restrictions on the purchase of tobacco products; (4) taxation and pricing of tobacco products; (5) legal restrictions on where people can smoke; and (6) smoking cessation services. While there are many examples of awareness campaigns, especially in HICs, more research is needed to better understand what motivates the behavior change that those awareness campaigns seek to induce. Unhealthy foods, such as highly processed snacks, red meat, sugary drinks, and alcohol, are promoted with extensive marketing budgets with many supermarket aisles devoted to their promotion. Governments should look at how to counter this—for example, the United Kingdom has announced banning junk food advertisements before 9.00 pm on television. Weekly TV educational campaigns about stroke prevention and warning signs of stroke should be encouraged.
Primary prevention involves early detection and control of risk factors, such as hypertension, dyslipidemia, obesity, and diabetes to avoid a first stroke event. While some non-modifiable risk factors, such as age, can be used as triggers for investigation of potential stroke risk, many modifiable risk factors, such as hypertension or diabetes, can remain undetected. Worldwide (and especially in low- and middle-income countries), undetected and uncontrolled hypertension, high-risk behaviors, such as poor diet, smoking, and lack of exercise, rising obesity, and air pollution continue to contribute to stroke risk.
However, it would be mistaken to exclusively target primary prevention at those who have a high risk because most strokes occur in people with medium to low risk. Therefore, primary prevention activity on a population level by governments needs to be aimed at the whole population, while primary prevention activity on an individual level by health professionals needs to be aimed at all individual with increased risk of stroke regardless of the level of the risk. In addition, while primary stroke prevention is often presented solely as being about individual lifestyle “choices,” in fact substantial and effective policy on prevention is needed from government and health systems.
For example, identifying and treating high blood pressure (which is the biggest risk factor for stroke and should therefore be a priority) requires extensive data gathering and population-level diagnostic checks; reducing salt content in the processed food often requires legislative changes from the government. Once identified, people with high blood pressure need access to affordable medicines, regular health checks, advice and expertise, and be able to source and afford to eat a healthy diet.
The challenge, especially for low- and middle-income countries, is to deliver comprehensive prevention services which do more than just target those deemed high risk—90% of strokes occur in people with low-to-medium stroke risk. That is why cost-effective digital tools, such as the Stroke Riskometer app, are referenced by the WSO. Successful primary prevention requires countries to have health systems that (1) have good health data about their populations; (2) provide universal health coverage and provide services and advice across all geographic areas, rural and urban; (3) have universal health care coverage; (4) have trained staff; (5) provide affordable medicines and treatment; (6) have the political commitment from national and regional government to sustain delivery; (7) involve stroke support organizations; implement Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders (IGAP); 8 and (8) aim at achieving the WHO Sustainable Development Goal 3.4—by 2030: to reduce by one-third the premature mortality from NCDs through prevention and treatment and promotion of mental health and well-being.
Assessment of the incidence, prevalence, management, and control of cardiovascular risk factors at the population level is vital and should be based on reliable measurements, for example, measurement of blood pressure rather than self-reported hypertension. Good data require enough adequately trained people to collect and analyze it. Where resources are limited, efforts should be focused on collecting high-quality data for risk factors that (1) strongly predict stroke (e.g., blood pressure, physical activity, lipid profile, diet, body weight, psychosocial factors, smoking, diabetes); (2) are highly prevalent; (3) are amenable to individual-level and population-level intervention; and (4) are relatively easy and cheap to monitor. Tools such as the WHO’s STEPS program are valid and reliable systems for the surveillance of risk factors as are the free Stroke Riskometer app for the general population and PreventS-MD for health professionals. Governments should establish comprehensive and universal nationwide systems for monitoring stroke through registries, electronic health records, and vital statistics systems. Governments need to ensure enough adequately trained people to collect and analyze the data. Protocol-based and regulated systems for task-shifting from doctors to nurses and from nurses to community health workers can support the efficient use of specialist clinical staff within the health care system.
Countries with universal health coverage can provide a wide range of stroke prevention services free or at low cost. The absence of universal health care exacerbates inequalities in access to stroke prevention services, and people tend to prioritize out-of-pocket costs for treatment rather than prevention, with few or no regular health checks for stroke risk factors.
Shifting or sharing of tasks from highly trained health care professionals, such as physicians and nurses, to supervised and trained paramedical health care workers, particularly community health workers (following regulatory protocols) can facilitate primary stroke prevention interventions at the individual level, and incentives for health care staff in rural areas should be improved to encourage relocation and retention.
Lack of trained health care staff is a major barrier to providing primary and secondary stroke prevention services. The unequal distribution of health care staff and socioeconomic differences between urban and rural areas create inequalities in access to services, and negatively affect health literacy. Countries with a wide network of service delivery by a mixture of staff (e.g. doctors, nurses, community health workers) with stroke-specific training can provide a wide range of stroke prevention services.
Once a person’s stroke risk has been assessed, and conditions such as hypertension or diabetes have been identified, it is vital that patients have access to and can afford the appropriate treatments and medicines. The WSO—Lancet Neurology commission 2 recommend that access to affordable medications for primary and secondary stroke prevention should be improved, with a focus on essential medications (such as polypills including blood pressure and lipid-lowering drugs on the WHO list of essential medications) and tools. Essential drugs for primary and secondary prevention should be subsidized and made available at all hospitals and outpatient clinics.
The WSO—Lancet Neurology Commission also suggests that a tripartite approach to stroke prevention comprising behavioral, pharmacological, and health system level and societal interventions (based on the socioecological model) could minimize the fragmentation and inefficiency of primary stroke prevention. Health care system-level interventions would include screening for stroke risk factors at every clinical encounter, while societal interventions should include ensuring availability of affordable healthy foods, clean air, and spaces for physical activity. An absence of effective government-led primary stroke prevention activities is linked to low population health literacy about stroke prevention. Strong governance in stroke prevention facilitates high-quality services. A political commitment to stroke prevention and a national strategy to control risk factors enhance both primary and secondary stroke prevention. Active participation of stroke organizations enhances governance. Countries with strong governance use health data for decision-making and evidence-based interventions, whereas a lack of government commitment to prevention of cerebrovascular diseases along with lack of evidence-based national prevention guidelines hinder prevention. Stroke support organizations can also be effective in working with health professionals at the community level to raise awareness of stroke risk.
Reducing stroke burden also requires effective secondary stroke prevention interventions. People who have had a stroke or transient ischemic attack (TIA) are at much higher risk of having a second one. However, 2–3% of survivors of a first stroke have another stroke within the first 30 days, 9% in the first 6 months, and 10–16% within a year. After a year, the figure is 5%. 9 It is vital that everyone who has a stroke or TIA has all the interventions and information needed to reduce their risk of a recurrent stroke. Most stroke survivors already have an underlying medical condition that increased their risk of stroke. These underlying conditions remain a risk after the first stroke event and must be treated. They are modifiable, so secondary prevention interventions can make a big difference. Most of these risk factors are symptomless and require tests and investigations to diagnose. Assessment of stroke risk factors should begin as soon as possible after the initial stroke or TIA. Everyone should have access to screening and appropriate management of underlying conditions, such as hypertension, diabetes, carotid stenosis, and atrial fibrillation.
People who have had a stroke should have a plan for secondary stroke prevention, including access to regular monitoring, medication, and support for behavioral change. Helping people understand the medical conditions that may have caused their stroke will help them to know how they can reduce the risk of a further stroke. Ensuring stroke survivors have access to advice from health professionals is vital. Stroke survivors need specific advice and support for healthy lifestyle measures, such as diet considerations when there are swallowing limitations, and exercise and activity levels especially if they have been disabled by their stroke. Clinicians, medical practitioners, and stroke support organizations have a vital opportunity and role to play in supporting people to manage behaviors to reduce the risk of having another stroke. Regular post-stroke reviews and check-ups are very important, especially as many stroke survivors feel they do not get the support they need to stay healthy. Stroke survivors need to understand the way they can tackle the modifiable lifestyle risk factors they face. Ensuring stroke survivors have access to ongoing support, resources, and opportunities to sustain lifestyle changes is crucial.
As with primary stroke prevention, secondary stroke prevention services should be free and easily accessed as part of universal health coverage. National and regional health budgets should be allocated to primary and secondary stroke prevention, and effective treatment and rehabilitation services.
While effective treatments are available, access to care is limited to just a fraction of stroke patients. Technologies such as mechanical thrombectomy are not just another tool but a beacon of hope, offering the potential to improve the lives of millions of people who experience the impact of stroke every year. Policymakers and other stakeholders should recognize the potential these treatments have to strengthen their health systems and increase access. Improving access to mechanical thrombectomy and developing the 24/7 infrastructure networks needed to support this treatment will require concrete actions, but the potential for positive change is within our grasp. Investing in stroke care and research is not just a financial commitment but also a highly effective investment. The current human and economic cost of stroke is enormous, and without targeted efforts, it will only escalate. The efficacy of intravenous thrombolysis and especially mechanical thrombectomy surpasses that of treatments for comparable NCDs by a wide margin. Investing in these treatments will yield long-term savings on the direct costs for nursing and rehabilitation, and help to alleviate the strain on health care budgets regardless of a country’s income level. Investing in stroke care will increase the quality of life and reduce costs. Governments, providers, professional societies, and patient groups all have a crucial role to play in combatting this disease. Their collaborative efforts can bring meaningful change. This entails not only increasing the capacity of stroke units as the first level of care but also significantly boosting the proportion of patients receiving effective advanced treatment, thereby preventing lifelong disability and ensuring functional independence after a stroke. It means educating health workers, individuals, communities, and the entire care pathway, about the importance of swift action in the event of a stroke. By taking these steps, governments can empower their citizens and take responsibility for improving the health of their nations.
To demonstrate the feasibility and efficacy of the implementation of some of these preventive strategies, we would like to present several success stories. For example, over 50% of South African adults are overweight or obese, with 69% of obese adults living in food-insecure households where families have little dietary choice and are forced to eat food with low nutritional value. The country has implemented a multidimensional approach, including data collection via the National Food and Nutrition Security Survey (https://foodsecurity.ac.za/publications/national-food-and-nutrition-security-survey-national-report/). In 2018, the government introduced a 10% tax on sugary soft drinks (SSBs) as part of a strategy to reduce obesity and NCD risk in the population. Following implementation of the tax in 2018, the country has seen a 29% average reduction in purchases of SSBs. 10 The impact on those in low-income urban households has been even more pronounced with purchases in these households reduced by 57%. 11
To support public understanding and promote healthier nutritional choices, the Heart and Stroke Foundation South Africa established a Nutrition Science Team, ensuring that all nutritional information communicated to the public is evidence-based, understandable, practical and cost-effective. The Nutrition Science and Health Promotion teams present health talks for the School Health Promotion Initiative (https://heartfoundation.co.za/healthy-schools/#:~:text=The%20whole%20of%20the%20school’s,undergoing%20a%20health%20risk%20assessment) and the Mended Hearts and Stroke Group in community-based settings and is also engaged in private sector employee wellness work. They also send monthly CVD updates with peer-reviewed articles to health professionals and respond to public health-related and nutrition questions. The team also works with all Foundation programs for key public health events, including health promotions, disease prevention activities, virtual talks, and health risk assessments (HRAs). The School Health Promotion Initiative (SHPI) is aimed at “all of the school” programs to raise awareness among young South Africans on the importance of adopting healthy behaviors and to encourage all staff at the targeted schools to know their health status. The Health Promotion team at an SHPI event conducts HRAs by screening of the population. A typical SHPI event adopts a holistic approach and includes a Health Talk for all the learners at the school, which focuses on the importance of a “healthy heart and brain” and what behaviors to adopt to stay healthy.
In 2022 under the leadership of Prof. Sheila Martins, and with support from the government of Brazil and industry partners, a program of training of health volunteers (community health workers (CHWs)) for stroke prevention activities to facilitate task-shifting of this work from clinicians to CHWs was initiated and hundreds of CHWs were deployed throughout the country. CHW joined online training on stroke risk factors and prevention, behavior modification, screening and management of hypertension, and atrial fibrillation (irregular heartbeat). The training layered onto existing WHO HEARTS and Better Cities initiatives to provide a holistic approach to prevention. CHWs were provided with translated public information resources developed by WSO and sensitized to the use of mobile technologies, such as Stroke Riskometer app, to measure, track stroke risk factors in the community, and motivate individual behavior change. Following the training, the Stroke Riskometer app was used by the trained CHWs in communities to conduct assessments and familiarize individuals with their lifetime risk of stroke, highlighting where this can be reduced, and sharing information on relevant risk factors and prevention. Motivational push notifications were designed to help keep 3350 participating individuals engaged over the course of the program that also included a randomized clinical trial. A follow-up survey with a sample of program individuals participating in the RCT (n = 367) 12 was conducted at 6 months with 79% indicating increased knowledge of stroke risk factors and 62% indicating that participation had led them to take action to modify their risks resulting in noticeable reduction in SBP and increased physical activity compared to controls (usual care).
The Australian Stroke Foundation’s Living Well After Stroke (https://strokefoundation.org.au/what-we-do/prevention-programs/living-well-after-stroke#:~:text=Living%20Well%20After%20Stroke%20is%20a%20group%2Dbased%20program%20that, healthy%20changes%20on%20your%20own) (LWAS) program is an evidence-based, 8-week group intervention designed to help stroke survivors make lasting health behavior changes, such as healthy eating, increasing physical activity, and managing medication. Based on the Health Action Process Approach (HAPA) model, it equips participants with a “toolkit” of skills and strategies to sustain these changes.
LWAS was piloted in 2023. Of the 62 participants, 94% reported the program exceeded their expectations. Not only did participants implement their chosen behavior but they also independently applied the LWAS “toolkit” to change an addition behavior after the program. Furthermore, a significant and sustained improvements in well-being were observed. The program is currently being run in Tasmania, with many participants from the areas of the state with little to no access to health services post-stroke. LWAS will be expanded nationally in 2025.
In conclusion, prevention is one of the most effective and cost-efficient ways to reduce the increasing stroke burden which has devastating impacts on individual and societal level. Moreover, the impactful prevention initiatives can be implemented in low- and middle-income countries which experience the greatest stroke burden and the most significant challenges in relation to providing acute stroke care. By enacting stroke prevention policies at social, health care, and individual levels, countries can significantly reduce their health care costs and support sustainable development of stroke care across the care pathway. Governments must act to (1) reduce inequities and other social determinants of stroke and cardiovascular disease; (2) promote and support access to healthy lifestyles Implement taxation and control measures to address the impact of harmful substances; (3) establish multisectoral public health partnerships to address the socioeconomic and environmental drivers; (4) provide universal health coverage to support management of clinical risk factors for stroke; (5) establish reliable and comprehensive data collection systems for stroke; (6) establish strategies that identify and manage people at any level of increased risk of CVD; (7) provide employment and training of community-based health workers supported by eHealth technologies; (8) develop culturally relevant primary and secondary prevention strategies; and (9) deliver ongoing stroke awareness campaigns.
Footnotes
Acknowledgements
The authors thank Anita Wiseman (WSO), Lisa Murphy (Stroke Foundation Australia), Joe Korner (Stroke Alliance for Europe), and Pamela Naidoo (Heart and Stroke Foundation South Africa) for their preparation of case studies; and Sarah Belson (WSO and Stroke Alliance) and Joe Korner (Stroke Alliance) for reviewing the article.
Author contributions
V.L.F. conducted the literature reviews, calculated the statistics, and developed the draft Fact Sheet. I.R. prepared Tables 1 to ![]() . B.N., M.B., S.O.M., J.P., M.F.G., and P.L. provided guidance, input, and edits throughout the development of this work. All authors reviewed and approved the final version of the article.
. B.N., M.B., S.O.M., J.P., M.F.G., and P.L. provided guidance, input, and edits throughout the development of this work. All authors reviewed and approved the final version of the article.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: V.L.F. declares that free Stroke Riskometer app and PreventS-MD are owned and copyrighted by PreventS-MD Ltd (a spin-off of the Auckland University of Technology Ventures Ltd), he is a Chief Scientific Adviser and shareholder of. B.N. has received honoraria for Data Safaty and Monitoring Board work for the HOVID trial (Simbec-Orion). None of the other authors declared any conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.