
Abstract
Despite the progress made in understanding the management and outcomes of Moyamoya angiopathy (MMA), several aspects of the disease remain largely unknown. In particular, evidence on the disease history and management of MMA is lacking, mainly due to methodological and selection biases in the available studies and the lack of large, randomized prospective studies. Therefore, the care of MMA patients remains limited to a few expert centers worldwide, and management is often based on local expertise and available resources. Over the years, recommendations or expert opinions have been written to provide guidance to physicians in the treatment of this condition with the goal of reducing the risk of stroke recurrence and long-term disability. However, there is no complete agreement between the available guidelines and recommendations due to differences in the articles addressed, methodologies, expertise, and validated approaches to literature review. This lack of consensus on the management of MMA may confuse clinicians and highlight some important issues and points. The aim of this comprehensive review article is to critically examine three recent guidelines and recommendations on MMA, discussing their differences and similarities and highlighting gaps in MMA care that need to be covered.
Introduction
Moyamoya angiopathy (MMA) is a rare cerebrovascular disorder characterized by a progressive occlusion of the internal carotid arteries termination and/or of its proximal branches with the compensatory development of a network of fragile collateral vessels (Figure 1). The disease presents in childhood or adult age.1–3 The most important clinical features include transient or permanent cerebral ischemic events and intracranial hemorrhages but also cognitive deficits, migraine-like episodes, and psychiatric and movement disorders. 4 Although the disease is less frequent in Western than in Eastern countries, MMA is increasingly identified worldwide, and its interest is growing. However, evidence on the disease history and management is still poor, mostly due to methodological and selection biases of available studies and to the lack of randomized and large prospective studies. To date, no treatment limiting the progression of the vessel wall lesions is available. Surgical revascularization is used in selected patients to enhance cerebral perfusion and reduce the risk of further cerebrovascular events. However, several aspects of the disease remain poorly known, making it difficult to decide which patients are worthy of surgery and when is the best time for and which type of intervention. In addition, the diagnostic workup and the management of the disease remain heterogeneous worldwide.5,6
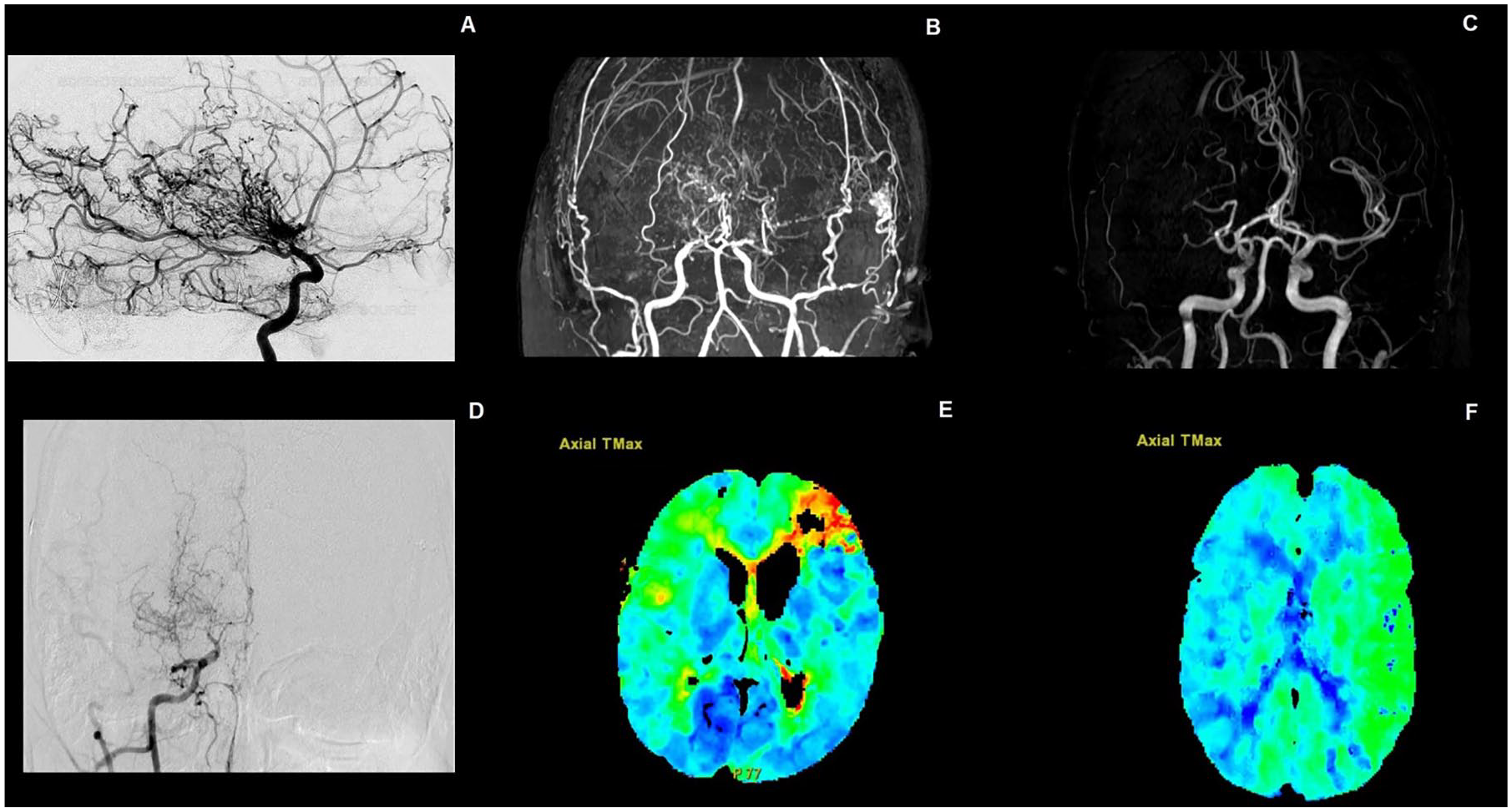
(a) Abnormal net-like vessels proliferate giving the characteristic “puff of smoke” appearance on direct angiography. (b) MR angiography showing bilateral middle cerebral artery stenosis. (c) MR angiography showing unilateral stenosis of the right middle cerebral artery. (d) Anteroposterior digital subtraction angiography showing a severe stenosis of the right middle cerebral artery. (e) Perfusion CT scan showing a marked increase in T max bilaterally and (f) only in the left hemisphere.
Guidelines on clinical management have been recently developed in different countries. In 2021, the guidelines for the management of MMA were published by the Japan Stroke Society, providing graded recommendation on medical treatment and surgical approach.7,8 However, some aspect of the disease, including the hemodynamic and posterior circulation assessment, have not been considered.
In February 2023, the European Stroke Organisation (ESO) published the first European guidelines on MMA. 6 A panel of methodologists, neurologist, neurosurgeons, and geneticists with expertise in the disease was brought together to identify relevant questions on the disease, to determine outcome measures, and to elaborate evidence-based recommendation or expert consensus statements, following a rigorous statistical methodology (GRADE).
More recently, a group of international MMA experts published scientific statements on the disease on behalf of the American Heart Association (AHA) to provide recommendations on the best management strategies for MMA patients. 9 AHA recommendations were a systematic review of 120 articles selected from a consensus opinion of experienced neurosurgeons, neurologists, and neuroradiologists.
The purpose of the present article is to critically review these three recent guidelines and recommendations, discussing point by point their differences and similarities with the aim of highlighting gaps in the care of MMA that need to be covered.
Ethical approval was not required for this study, as it did not involve human participants, patient data, or animal research.
Guidelines methodology
The 2021 Japanese guidelines for the management of MMA were drafted by the Research Committee on Moyamoya Disease approved by the Japanese Ministry of Health, Labour and Welfare, the Japan Stroke Society, the Japanese Society on Surgery for Cerebral Stroke, and the Japan Neurosurgical Society. 8 Recommendations were given by neurosurgeons with expertise in MMA, using the classification of evidence level (high, middle and low) and the recommendation grade, from strong (A) to harmful (E). Recommendations on surgical and medical treatment as well as management of cerebral hemorrhage were provided.
The European guidelines were developed according to the ESO standard operating procedure, which is based on the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework. 6 Ten European experts in cerebrovascular disease with a special interest in MMA worked together to prepare and answer relevant clinical questions about the management of MMA. The Working group included six vascular neurologists, three neurosurgeons, and one geneticist, experts in MMA. Questions were developed using the PICO (Population, Intervention, Comparator and Outcome) approach. Outcomes were defined as critical (any stroke, major stroke, and disability) or important (TIA; death and cognitive impairment) for making a decision. A systematic literature review was performed. PUBMED, EMBASE, and Cochrane Library databases up to February 2022, but also reference lists of review articles, authors’ personal reference libraries, and previous guidelines were used to select relevant records that were finally uploaded for assessment into the Covidence web platform (Health Innovation, Melbourne, Australia), to collect evidence to answer each PICO question. The research prioritized randomized controlled trials (RCTs), health registry data analyses, large observational studies, and systematic reviews or meta-analyses of observational studies.
The Scientific Statement from AHA and American Stroke Association (ASA) selected 10 writing group members among neurosurgeons, neurologists, and neuroradiologists, experts in MMA to create and review a scientific consensus on the current perspectives of MMA. 9 The working group dealt with and had to provide consensus on seven sections: Definitions, Epidemiology, Genetics, Diagnosis and Evaluation, Medical Treatment, Surgical Treatment, and Future Research Directions. A literature review from PubMed and Cochrane Databases up to 12 July 2022 was performed and 120 suitable publications were selected for review.
Definition
The definition of MMA is largely accepted, and MMA is defined as a chronic condition characterized by progressive bilateral steno-occlusion of the terminal portion on the internal carotid artery and its main branches, with the formation of an abnormal network of dilated, fragile perforators at the base of the brain, in the absence of other causes. 10 However, the distinction between “definite cases” and “probable cases” had been used for a long time since 1978. A “definite case” was described by the presence of a stenotic lesion in both terminal portions of the internal carotid arteries, while patients with unilateral stenosis were defined as “probable cases.” This difference was abolished in the 2015 revision of the Japanese criteria for MMA, but it had not widely been recognized. Therefore, in the 2021 version of the Japanese diagnostic criteria, it was highlighted as a note that both bilateral and unilateral cases can be diagnosed as MMA. 8
Regarding the criteria applied in the ESO guidelines, the angiographic diagnostic criteria of Fukui 10 were applied to MMA diagnosis, considering only bilateral cases. Patients were defined as symptomatic when presenting with TIA, ischemic or hemorrhagic stroke, headache, movement disorders, or cognitive disturbances. Unilateral presentation was considered only in syndromic cases.
The AHA/ASA Scientific statement highlighted the most recent guideline definition 8 where unilateral involvement is considered acceptable for making the diagnosis, after exclusion of other causes of steno-occlusive involvement of the terminal portion of the intracranial carotid arteries. 9
Diagnostic criteria
In 1957, the angiographic characteristics of MMA were first reported, 11 and Suzuki and Takaku first reported this disease entity as “moyamoya disease” in an English-written journal in 1969. 2 Since then, cerebral digital subtraction angiography (DSA) was considered the gold standard for the diagnosis for a long time.
Throughout the years, new techniques for the evaluation of cerebrovascular disease had been improved to optimize the diagnosis and minimize the risks for each patient. Magnetic resonance angiography (MRA) provides a noninvasive means for assessing cerebrovascular structures. Therefore, the 1997 revision of the guideline for the diagnosis of moyamoya disease stated for the first time that the diagnosis of MMA can be made without DSA only if the findings on MRA meet certain criteria. 10 According to the Japanese criteria published in 2012, MRA could be sufficient to diagnose MMA when all the typical findings are present. In this latter case, an invasive angiography can be omitted. 12 This concept is highlighted in the revised version of the 2021 Japanese diagnostic criteria, where radiological examination such as cerebral angiography is mandatory for diagnosis, especially in the case of unilateral lesions or lesions complicated by atherosclerosis. 8
More importantly, the revised version of the 2021 Japanese diagnostic criteria included the findings on heavy T2-weighted images as the essential feature for diagnosis of MMA without cerebral angiography. Thus, recent imaging studies have shown that the outer diameter of the involved arteries, including the supraclinoid portion of internal carotid artery and the horizontal portion of middle and anterior cerebral arteries, is particularly decreased in MMA. The finding is more prominent in the advanced cases and is quite useful to distinguish MMA from the intracranial arterial stenosis due to atherosclerosis. 8
For inclusion in the European guidelines, 6 MMA diagnosis should have been performed according to established angiographic diagnostic criteria, referring to the Japanese guidelines published in 1997. 10
In the AHA statement, cerebral angiography is still defined as the gold standard for the diagnosis of MMA and MRA is suggested only in certain cases, described by the recommendations from the Research Committee on Moyamoya Disease. 9
Moyamoya spectrum disease
A group of conditions can exhibit vascular features similar to MMA, characterized by progressive narrowing of the intracranial arteries and the formation of abnormal collateral vessels. In the 2021 revised version of the Japanese diagnostic criteria, the Research Committee on Moyamoya disease included autoimmune disease (SLE, antiphospholipid syndrome, polyarteritis nodosa, Sjögren syndrome, etc.), meningitis, brain tumors, Down syndrome, neurofibromatosis type 1, and cerebrovascular lesions after head irradiation as associated conditions. 8 For patients in whom these conditions are associated with MMA vascular features, the term moyamoya syndrome (MMS) is used. Atherosclerosis and hyperthyroidism were excluded from the list of conditions associated with MMS, according to recent knowledge, but consensus through international discussion is warranted in the future. MMS shares the characteristic angiographic appearance of MMA, including the development of compensatory collateral vessels, and patients with MMS are also at risk of both ischemic and hemorrhagic strokes. 4 However, despite the similarities in vascular presentation, MMS differs from MMA in its underlying causes, requiring tailored therapeutic approaches based on the associated conditions.
No specific recommendations on MMS have been published by the ESO, the Japanese guidelines, or the AHA statement.
Genetic testing
The etiopathogenesis of MMA remains unknown although a strong genetic component has been supposed, based on the observation that up to 12–20% of patients have a positive family history. 1 In 2011, an association between MMA and a single mutation (p.R4810K) in a gene encoding the ring finger protein 213 (RNF213) was reported in Japanese patients. 13 A founder effect has been found in East Asia, especially in Japan and Korean patients. However, the appropriateness of genetic testing of this RNF213 variant in MMA patients is still under discussion.
In the 2021 Japanese guidelines, there are no recommendations regarding the indication for testing the RNF213 p.R4810K variant. 8
Due to the lack of specific comparative studies comparing genetic versus nongenetic test, the ESO guidelines did not provide any recommendation regarding RNF213 genetic testing. An expert consensus statement suggested against systematic variant screening of RNF213 p.R4810K (vote 8/10). 6 The AHA experts claim that genetic tests in affected individuals may help shed light on the pathogenesis of the vasculopathy, although they point out its role for diagnosis and for genetic counseling as limited at this time. 9
RNF213 testing has the potential to become a valuable diagnostic tool, especially in cases where the diagnosis of MMA is uncertain and in regions with a high prevalence of the mutation. However, clear guidelines on which patients should undergo predictive genetic testing are currently lacking.
Hemodynamic assessment
The identification of a cerebral hemodynamic impairment in MMA patients has been shown to be a predictor of stroke. 14 Neuroimaging strategies investigating cerebral hemodynamic aspects are being continuously developed. These techniques, including cerebral magnetic resonance imaging (MRI) with arterial spin labeling, brain CT perfusion, Acetazolamide (ACZ)-99mTc-HMPAO-SPECT, or PET with ACZ challenge, are poorly validated and differently used depending on local facilities. In patients with MMA, there are still many uncertainties about which technique and timing is the best for hemodynamic assessment.
The Japanese guidelines recommended cerebral hemodynamics assessment only in the early postoperative period, to differentiate postoperative ischemia from hyperperfusion and to evaluate the effects of revascularization surgery. No indication is given as to whether hemodynamic tests should be performed during the initial assessment of patients with MMA, because this guideline only focuses on the standardization of treatments for MMA. 8
In the European ESO guidelines, it is specified that there is a continuous uncertainty over the advantages and disadvantages of performing hemodynamic assessment, due to the lack of comparative studies and to the heterogeneous populations. However, an expert consensus statement suggested the hemodynamic assessment for all patients with MMA (vote 9/9), during the diagnostic workup to help in decision-making. 6
The AHA statement also specified the importance of hemodynamic imaging techniques for assessing cerebrovascular reserve capacity and hemodynamic status of brain parenchyma in MMA but, as their ability to predict clinical outcomes has not been validated in large prospective cohorts to date, no further guidance is given as to when and for which patients these examinations are recommended. 9
Vascular risk factors
Managing cerebrovascular risk factors plays a crucial role in the medical control of MMA. Elevated homocysteine levels and increased body mass index have been associated with a higher risk of MMA. 15 Diabetes is also considered an independent factor influencing the recurrence of ischemic strokes in both surgically and nonsurgically treated MMA patients. 16
A 2020 retrospective analysis suggested that hypertension and dyslipidemia might increase the risk of cerebrovascular events in asymptomatic patients. 17 However, there is ongoing debate about the optimal treatment and timing of intervention. A 2020 prospective nonrandomized study from China demonstrated the benefit of daily atorvastatin (20 mg) in improving the formation of postoperative circulation on DSA. 18 In addition, a recent Korean cohort study highlighted the beneficial effects of statin treatment for MMA patients, reducing the risk of both ischemic and hemorrhagic strokes. 19
Despite these findings, no clear recommendations have been published on this topic by the ESO, the Japanese guidelines, or the AHA statement.
Acute stroke management
Acute ischemic stroke is one of the most frequent complications in MMA patients. 4 The use of tissue plasminogen activator (rt-PA) in MMA patients with acute ischemic stroke can be a major challenge for neurologists given the increasing bleeding risk due to the presence of fragile moyamoya compensatory vessels and the absence of clinical trial regarding this treatment strategy in MMA patients.
Although the level of evidence from the Japanese guidelines is low (Recommendation Grade: C, Level of Evidence: low), the use of the intravenous thrombolysis with recombinant tissue plasminogen activator is considered possible under careful evaluation of the risk of hemorrhagic complication. 8 Indications on antihypertensive treatment, glycerol use in case of edema or intracranial hypertension as well as on supportive treatment with antipyretics, anticonvulsivants, control of blood sugar, and oxygen are also provided. 8
No recommendations or consensus statements on acute stroke in MMA have been reported in the European guidelines and in the AHA statement, considering the scarce data regarding thrombolysis/mechanical thrombectomy in the setting of MMA-associated acute stroke.6,9
Antiplatelet therapy
Ischemic MMA
The use of antiplatelets in MMA ischemic stroke is suggested by different results,20–22 including the benefit in stroke recurrence prevention,8,23,24 but no randomized trial is available. The rate of hemorrhagic complication was not increased in the studies that have assessed this issue.20,21,25 The use of antiplatelets may improve bypass patency and functional outcome in patients undergoing surgery.23,24 Among antiplatelet agents, cilostazol has been proposed, as it may provide greater improvement in cerebral blood flow and cognitive status. 26
Current guidelines/recommendations substantially agree in suggesting platelet aggregation inhibitors in ischemic MMA patients, but several differences can be pointed. According to the Japanese guidelines, 8 oral administration of antiplatelet agents may be considered as medical treatment for ischemic MMA (Recommendation Grade: C, Level of Evidence: low) based on the indication for the treatment of atherothrombotic stroke. However, the Japanese group suggests caution in long-term administration, given the increased hemorrhagic risk, especially in patients with brain atrophy.
Also, in the European ESO guidelines, the use of long-term antiplatelet therapy to reduce the risk of embolic strokes is suggested as an expert consensus statement. However, it is specified that the quality of evidence is very low and that there is continuous uncertainty over the benefits and risks of long-term antiplatelet therapy. Continuation of antiplatelet treatment as monotherapy (aspirin) during bypass surgery to avoid complications is considered safe. 6
According to the AHA/American Stroke Association 2021 Guideline, antiplatelet use for prevention of ischemic events in surgical and nonsurgical patients with ischemic MMA is considered reasonable. 9
Hemorrhagic MMA
Intracranial hemorrhage (ICH) is one of the main manifestations of MMA and represents the major cause of death in these patients. Due to the paucity of longitudinal and comparative data on this topic, the medical management of MMA presenting with ICH is challenging. Although in 2019 the RESTART trial provided reassurance about the use of antiplatelet therapy in ICH survivors, 27 these findings cannot be easily applied in the cohort of MMA patients.
In the Japanese guidelines and in the AHA statement, there are no recommendations on this topic.8,9 This aspect is addressed in the ESO guidelines, where the only study that specifically analyzed the effect of antiplatelet therapy in a cohort of MMA patients initially presenting with ICH is cited. 6 In this study, patients treated with antiplatelets had reduced odds of long-term mortality as compared with no antiplatelet therapy. However, there is still not enough evidence to define recommendations in this regard.
Asymptomatic MMA
The optimal management of asymptomatic MMA, including the use of antiplatelet treatment remains uncertain and under active investigation.
The Japanese guidelines 8 considered that the use of antiplatelet agents requires caution in asymptomatic patients while considering the potential risk for a hemorrhagic event. For this reason, no clear recommendations on this topic have been published so far also by the ESO and the AHA.6,9 However, a recent 5-year interim analysis of the asymptomatic moyamoya (AMORE) registry in Japan showed that 7 of 103 asymptomatic MMA patients developed a stroke, of which 6 had a hemorrhagic stroke. The annual risk of stroke was 1.4% per person. In particular, microhemorrhages on initial imaging and markedly developed choroidal channel were significant predictors of hemorrhagic stroke. 28
Surgical treatment
Surgical revascularization is worldwide considered the only treatment able to reduce the recurrence of ischemic and hemorrhagic stroke risk.
Three types of surgical approaches, including direct, indirect, or combined bypass, are currently used. Direct revascularization involves connecting a healthy blood vessel, typically one or two of the branches of STA, directly to a superficial cortical brain artery, usually an M4 branch of MCA, with the aim of immediately improving cerebral blood flow. Indirect revascularization can be achieved using various techniques such as encephalomyosynangiosis (EMS), encephalodurosynangiosis (EDS), encefaphaloarteriosinangiosis (EAS), or their combination, and much more rarely omental-cerebral transposition. With indirect techniques, an unaffected tissue (dura, temporal muscle, omentum) or artery (STA or occipital artery (OA)) is placed in direct contact to the surface of the brain, to progressively stimulate growth of new blood vessels and compensate for the reduced blood flow caused by the disease. Finally, combined revascularization techniques include a combination of direct and indirect revascularization strategies.4,29
No prospective randomized trials have addressed revascularization surgery for ischemic stroke prevention in MMA. The efficacy of bypass surgery for ischemic MMA has been so widely recognized for so many years, thus it would be ethically difficult to not perform surgery on half of the patients in an RCT now. The only RCT available is the Japan Adult Moyamoya (JAM) trial, which compared surgical revascularization (direct bypass) versus medical therapy in adult patients with hemorrhagic MMA. This study demonstrated the superiority of surgery in preventing rebleeding (2.7% vs. 7.6% p = 0.04). 29 Posterior hemorrhages due to bleeding from the thalamic or choroidal arteries were observed to be at increased risk of rebleeding, and patients with hemorrhages in this location benefit the most from surgery. 29
Hemorrhagic MMA
In MMA patients with hemorrhagic presentation, there is a common indication for revascularization surgery.
According to the Japanese guidelines, direct or combined bypass surgery is reasonable, especially for patients with posterior hemorrhage to prevent recurrences (Recommendation Grade: B, Level of Evidence: middle). 8 It should be noted, however, that the JAM study only enrolled patients with a modified Rankin scale of 0–2. Interestingly, patients with posterior hemorrhage, who by nature are at a higher risk of rebleeding, appeared to benefit more from bypass surgery than those with anterior hemorrhage. As indicated by the distribution of collateral vessels and rebleeding sites, choroidal collaterals are a significant source of bleeding with a high risk for hemorrhagic recurrence and serve as an independent predictor of rebleeding in hemorrhagic MMA, due to their fragile structure and the increased hemodynamic burden they bear. Particularly in these patients, bypass surgery can reduce the rebleeding rate.30,31 However, due to the small sample size and the limited inclusion of patients with posterior hemorrhages, careful interpretation of the results is suggested. 29
The European guideline recommends revascularization surgery (evidence only for direct STA-MCA bypass) in hemorrhagic MMA in the case of cerebral hemodynamic impairment and presence of choroidal collaterals, with a low quality of evidence and a weak strength of recommendation. Recommendation was also very low for pediatric patients. 6
In the AHA/ASA guidelines, the experts considered that there is sufficient evidence and Class 2a recommendation for surgical revascularization in adults with symptomatic, hemorrhagic MMA. 9
Ischemic MMA
In the Japanese guidelines, surgical revascularization for MMA associated with cerebral ischemic symptoms had the same recommendation grade as hemorrhagic MMA but with a lower level of evidence (Recommendation Grade B, Level of Evidence: low). 8
The European guideline pointed out a continuing uncertainty over the risks and benefits of cerebral revascularization for these patients according to the quality of evidence, which is considered low. 6 In these patients, revascularization surgery should be considered in the case of clinical symptoms and/or imaging markers of hemodynamic impairment.
In the AHA/American Stroke Association 2021 Guideline, surgical revascularization (both direct or indirect) is considered potentially beneficial for the prevention of ischemic stroke or transient ischemic attack, with a C level of evidence. 9 The authors suggest also a careful anesthetic management and prompt recognition of surgical complications.
Asymptomatic MMA
In the European guidelines, as an expert consensus statement, conservative treatment is suggested in asymptomatic MMA patients, except for those with both cerebral hemodynamic impairment and silent ischemic lesions in the same cerebral region. 6
Japanese guidelines and AHA statement do not provide specific indications on the management of asymptomatic MMA patients.8,9 However, the results of the AMORE study report that asymptomatic moyamoya hemispheres may carry a 1.0% annual risk of stroke in the first 5 years. Although the study is still ongoing, it would favor conservative treatment for asymptomatic patients, except for cases with markedly developed choroidal anastomosis. 28
Type of surgical procedures
Revascularization surgery plays a central role in the management of patients with MMA to reduce the ischemic and hemorrhagic stroke rate, but a plethora of surgical techniques are applied without strong comparative data between them.
For the Japanese guideline, the indirect procedure alone is not considered sufficient, and a direct procedure or combined procedure is considered necessary for adult MMA patients. 8
The European guideline, despite the continuous uncertainty over the best procedure to be applied, suggested, as consensus statement, the direct/combined revascularization, instead of an indirect approach. 6
Finally, the AHA/ASA statement specified that the direct bypass or combined approach has advantages over the indirect approach for stroke prevention, although no strong conclusions can be made. 6
Endovascular treatment
Endovascular treatment of ischemic MMA with angioplasty or stent has been proposed over the years. 32 However, a high complication rate and a low rate of success has been reported. 32 The fragility of the moyamoya vessels, arterial shrinkage (negative remodeling) of the diseased vessel wall, and isolated luminal stenosis could be part of the presumed cause of this failure. In addition, a high rate of restenosis was observed in the few reports available. 33
Both the Japanese guidelines and the AHA statements agree that endovascular treatment of steno-occlusive lesions is not advisable.8,9 The ESO guidelines do not provide any recommendations in this regard. 6
Discussion and conclusion
Despite being rare, MMA is considered a significant cause of stroke and disability in young adults. 4
Although progress has been made in understanding the management and outcomes of MMA, several aspects of the disease remain largely unknown. This is mainly due to the lack of randomized clinical trials and well-conducted observational studies, 34 especially in Western countries. Moreover, the results of the available studies suffer from important methodological biases, such as heterogeneous phenotype inclusion, inappropriate patient selection, small sample size, but also variability in the diagnostic tools and therapeutic approaches applied.6,9 The continuous evolution and revision of diagnostic criteria over the years has also contributed to the heterogeneity of the collected populations, making it difficult to compare the results of different studies.
Due to the lack of reliable studies and of evidence, MMA patient care is still reserved to few expert centers worldwide and its management is often provided according to local experience and facilities.
Recommendations or expert opinions have been drafted over the years to provide guidance to clinicians in the treatment of this disorder and to ensure the best diagnostic and therapeutic management strategies with the final objective of reducing the risk of stroke recurrence and long-term disability.
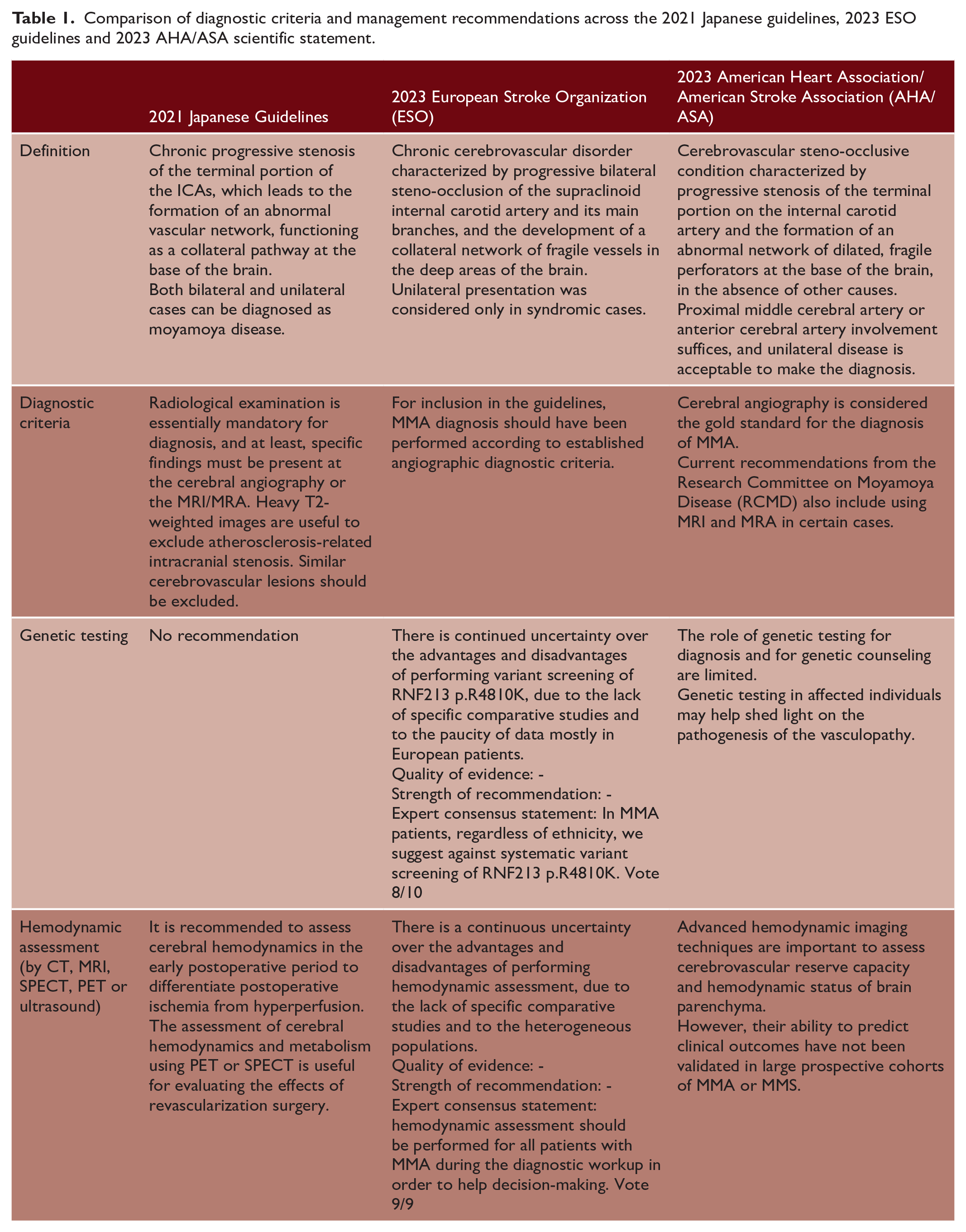
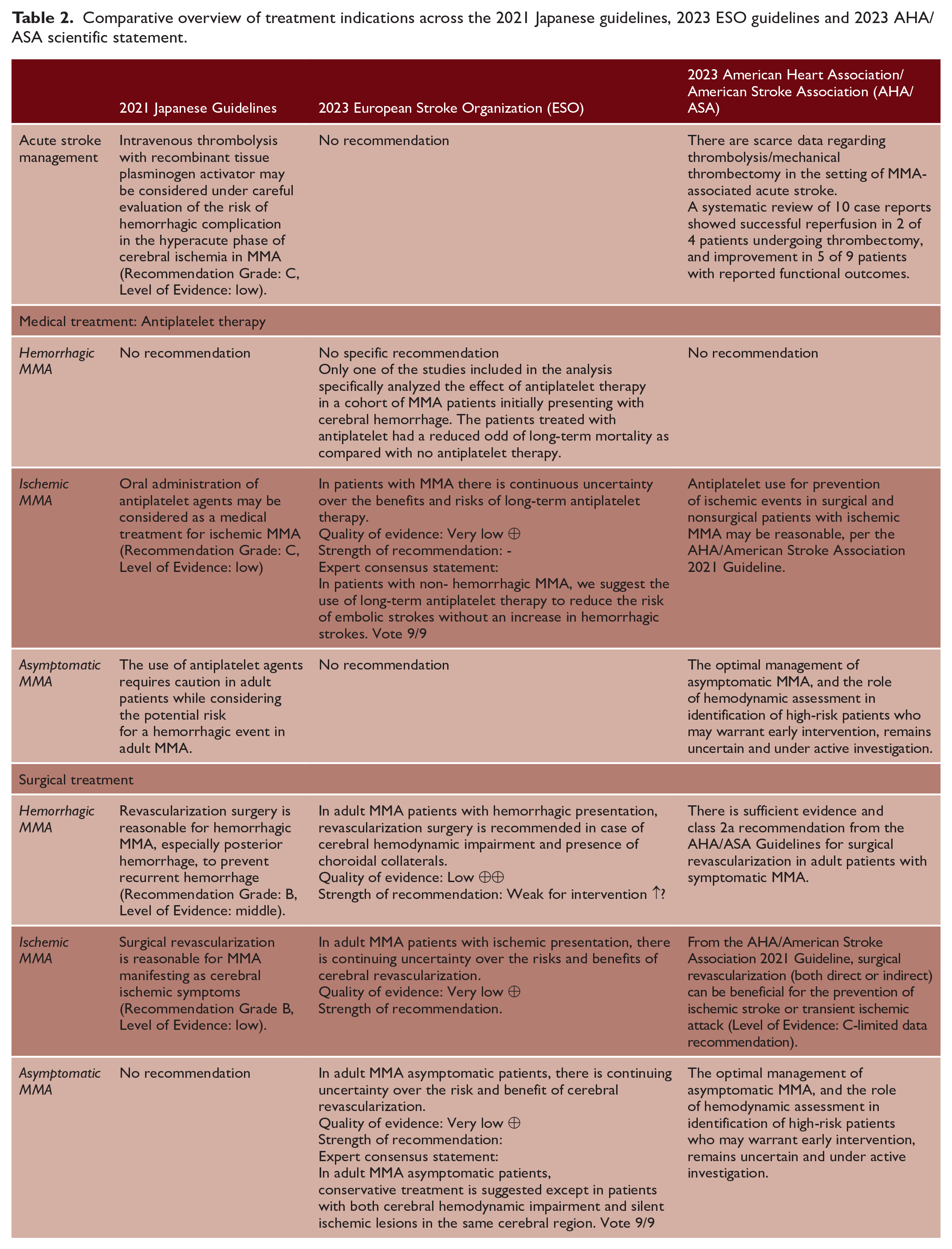
Herein, the comparison and analysis of the available guidelines and statements revealed significant differences (Tables 1 and 2). These could be mainly explained by their methodologies which strongly differ between guidelines, including different expertise (neurosurgeons for Japanese guidelines, neurologists, neurosurgeons and geneticists for ESO guidelines and neurosurgeons, neurologists, and neuroradiologists for AHA/ASA statement) and the use of a less or more standardized and validated approach for the literature analysis (consensus vs. GRADE methodology). Moreover, the items addressed by these guidelines differ and the recommendations provided in the management of MMA patients do not completely fit.
Comparison of diagnostic criteria and management recommendations across the 2021 Japanese guidelines, 2023 ESO guidelines and 2023 AHA/ASA scientific statement.
Comparative overview of treatment indications across the 2021 Japanese guidelines, 2023 ESO guidelines and 2023 AHA/ ASA scientific statement.
This lack of a consensus on the management of MMA may be confusing for clinicians and highlights some important questions and points.
First, the need for high quality and methodologically adequate registries and studies, including shared diagnostic definitions and longitudinal data collection. They should be useful to investigate the natural history of the disease and to identify predictors of clinical worsening. Innovative and well-designed randomized clinical trials with relevant outcome measures should also be implemented for therapeutic purposes to understand the best medical and surgical treatment.
Second, the usefulness of such guidelines is questionable. Indeed, clinical guidelines are defined as statements systematically developed to assist practitioner and patient decisions about appropriate healthcare for specific clinical circumstances. 35 However, despite some benefits in improving the consistency of care, therefore reducing disability and mortality, they have some limitations. In fact, scientific evidence supporting recommendation is often lacking, misleading, or misinterpreted and therefore judgment is influenced by opinions, clinical experience, and the composition of the guideline working group. Moreover, patients’ needs may not be considered in the selected recommendations 36 and translating the results into clinical practice as well as through different ethnicities is sometimes difficult.
Third, the lack of guidance on the management and workup of other MMA clinical aspects as cognitive impairment, movement disorders, seizures, and psychiatric symptoms. Social aspects and patient engagement are also poorly studied. These aspects are important for MMA care, as they could influence study results and should be considered a topic for future studies (Figure 2).
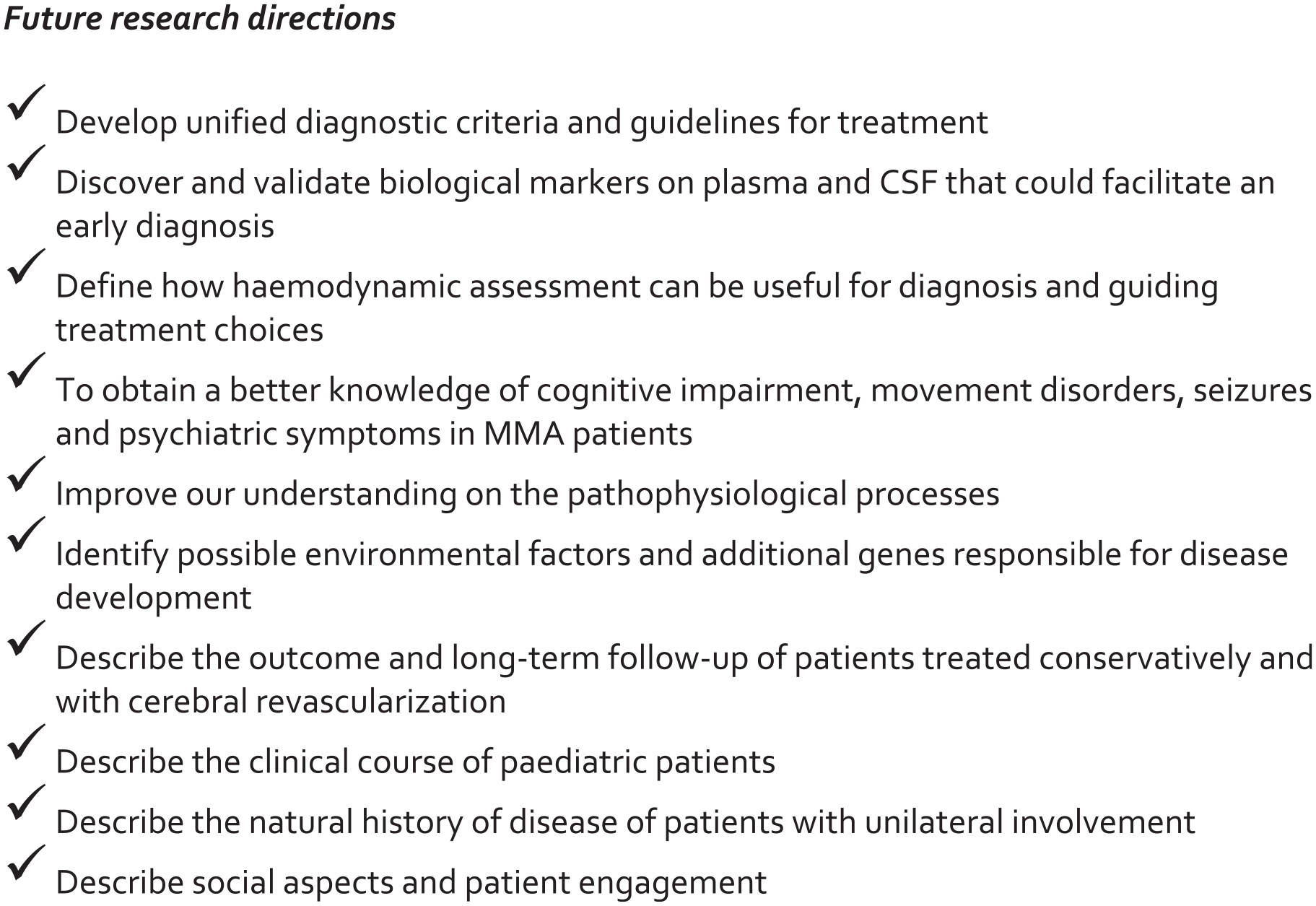
Future research directions in moyamoya angiopathy: key areas to advance diagnostic precision, treatment, and patient outcomes.
In conclusion, our analysis highlights the critical need for cohesive international multidisciplinary agreements to define the best diagnostic workup and treatment strategies. It is mandatory that this effort includes expertise of different specialists (neurologists, neurosurgeons, neuroradiologists, and geneticists), complies with rigorous methodological approaches to obtain evidence, overcomes ethnic differences, and provides comprehensive guidance on all clinical aspects of MMA.
In response to these needs, European Reference Networks (ERNs) have been recently developed to facilitate discussion on complex or rare conditions requiring highly specialized treatment and a concentration of knowledge and resources. Among the ERNs on rare multisystemic vascular diseases (VASCERN), a new working group dedicated to rare cerebrovascular diseases (NEUROVASC), including MMA, has been recently created. 37
Although this can be considered a first step toward homogeneity of guidelines at the international level, it is hoped that further efforts among various working groups at the global level will contribute to define unambiguous and widely shared guidelines worldwide.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.