
Abstract
Background:
Disparities in the availability of reperfusion services for acute ischemic stroke are considerable globally and require urgent attention. Contemporary data on the availability of reperfusion services in different countries are used to provide the necessary evidence to prioritize where access to acute stroke treatment is needed.
Aims:
To provide a snapshot of published literature on the provision of reperfusion services globally, including when facilitated by telemedicine or mobile stroke unit services.
Methods:
We searched PubMed to identify original articles, published up to January 2023 for the most recent, representative, and relevant patient-level data for each country. Keywords included thrombolysis, endovascular thrombectomy and telemedicine. We also screened reference lists of review articles, citation history of articles, and the gray literature. The information is provided as a narrative summary.
Results:
Of 11,222 potentially eligible articles retrieved, 148 were included for review following de-duplications and full-text review. Data were also obtained from national stroke clinical registry reports, Registry of Stroke Care Quality (RES-Q) and PRE-hospital Stroke Treatment Organization (PRESTO) repositories, and other national sources. Overall, we found evidence of the provision of intravenous thrombolysis services in 70 countries (63% high-income countries (HICs)) and endovascular thrombectomy services in 33 countries (68% HICs), corresponding to far less than half of the countries in the world. Recent data (from 2019 or later) were lacking for 35 of 67 countries with known year of data (52%). We found published data on 74 different stroke telemedicine programs (93% in HICs) and 14 active mobile stroke unit pre-hospital ambulance services (80% in HICs) around the world.
Conclusion:
Despite remarkable advancements in reperfusion therapies for stroke, it is evident from available patient-level data that their availability remains unevenly distributed globally. Contemporary published data on availability of reperfusion services remain scarce, even in HICs, thereby making it difficult to reliably ascertain current gaps in the provision of this vital acute stroke treatment around the world.
Introduction
Stroke is a complex and time-sensitive medical emergency. To improve outcomes following stroke, there is a need for systems of acute care that will optimize timely access to evidence-based therapies, 1 particularly the provision of reperfusion treatments (intravenous thrombolysis or endovascular thrombectomy) for patients with ischemic stroke. Reperfusion services are provided by interdisciplinary stroke units in hospitals often designated as a comprehensive or primary stroke center. 1 Where stroke centers are unavailable, telemedicine networks can be used to coordinate the provision of reperfusion therapies with specialist investigations and interventions in stroke-capable hospitals often situated in nonurban locations. 1 In addition, with the advent of mobile stroke unit (MSU) pre-hospital ambulance services, reperfusion therapies are now also provided in the pre-hospital setting.
Due to the increasing burden of stroke globally, the World Stroke Organization (WSO) is leading a global call to action to increase access to reperfusion services for acute stroke. 2 Availability of country-level data on the provision of reperfusion services is important for guiding national health care planning and policy, or funding/resource allocation decisions, to improve outcomes after stroke. We have previously reported stroke statistics (incidence, case fatality, and mortality) by country,3–6 and described the global access to stroke units, and the use of national clinical quality registries for routine monitoring of the quality of acute stroke care.3,4 In this new Global Stroke Statistics article, we present an overview of the provision of reperfusion services (i.e. intravenous thrombolysis and endovascular thrombectomy) for treating acute ischemic stroke. Specifically, we provided a repository of the latest published country-specific data on the provision of reperfusion services, either directly or as facilitated by telemedicine or MSU ambulance services.
Methods
We undertook a comprehensive search of PubMed for peer-reviewed literature on the provision of thrombolytic therapy (intravenous thrombolysis), endovascular thrombectomy, stroke telemedicine services, or MSU pre-hospital ambulances services, for acute stroke care, using the search terms described previously. 3 Original peer-reviewed articles and review articles published in English, as of January 2023, were identified. The most recent report from national clinical stroke registries was also identified, since these reports comprised a standardized overview of country-specific acute stroke care treatments. 6 We included articles in which nationally representative patient-level data on the provision of reperfusion services were reported. Where multiple studies from one country were identified, data were extracted from the most recent and nationally representative source only. For countries in which nationally representative patient-level data were not available, we included patient-level data from regional or single-center studies.
Three authors (JK, MTO, and TT) undertook the (a) screening of articles by title and abstract; (b) initial review of articles to confirm eligibility; (c) development of templates for data extraction; and (d) extraction of relevant data from included articles or reports. Templates used for data extraction were reviewed by a senior author (DAC) and approved by all authors. Co-authors scrutinized the list of identified articles and reports to assess whether relevant data were missing and contributed any additional relevant original peer-reviewed articles or recent registry reports that were missed in the initial search. Co-authors from Sweden, Denmark, Canada, and Singapore provided unpublished, but verified, latest data from relevant national stroke clinical registries. For the availability of MSUs, we compared published articles with information available in the PRE-hospital Stroke Treatment Organization (PRESTO) website. 7
Data extracted included (a) the availability of intravenous thrombolysis services in a country; (b) proportions of patients with ischemic stroke provided with intravenous thrombolysis, and proportions of hospitals providing intravenous thrombolysis, in countries where such services were reported to be available; (c) the availability of endovascular thrombectomy services in a country; (d) proportions of patients with ischemic stroke provided with endovascular thrombectomy, and proportions of hospitals providing endovascular thrombectomy, in countries where such services were reported to be available; (e) availability of stroke telemedicine programs, including the name, location (city and country), and model/composition (number of hospitals, hubs, and spokes) of such programs; and (f) availability of MSU pre-hospital ambulance services, including the location (city and country).
Results
Overall, 11,222 publications were identified from electronic databases, and four published articles and one report recommended by a co-authors DADS and JB. Data were also obtained from reports from national stroke clinical quality registries of nine countries, the PRESTO, and the Registry of Stroke Care Quality (RES-Q) repositories. Overall, 148 records with data from 70 countries met our inclusion criteria (Figure 1). Data were mostly from the regions of Western Europe (25.7%), Central Europe (12.9%), Southeast Asia (10.0%), and North Africa and the Middle East (10.0%; Table 1). Data from 26 countries (37.1%) were nationally representative, including 17 from national registry sources and nine from other sources (Table 1). For 35 of 67 countries in which the year of data was known (52.2%), the latest data reported were from 2019 onwards.
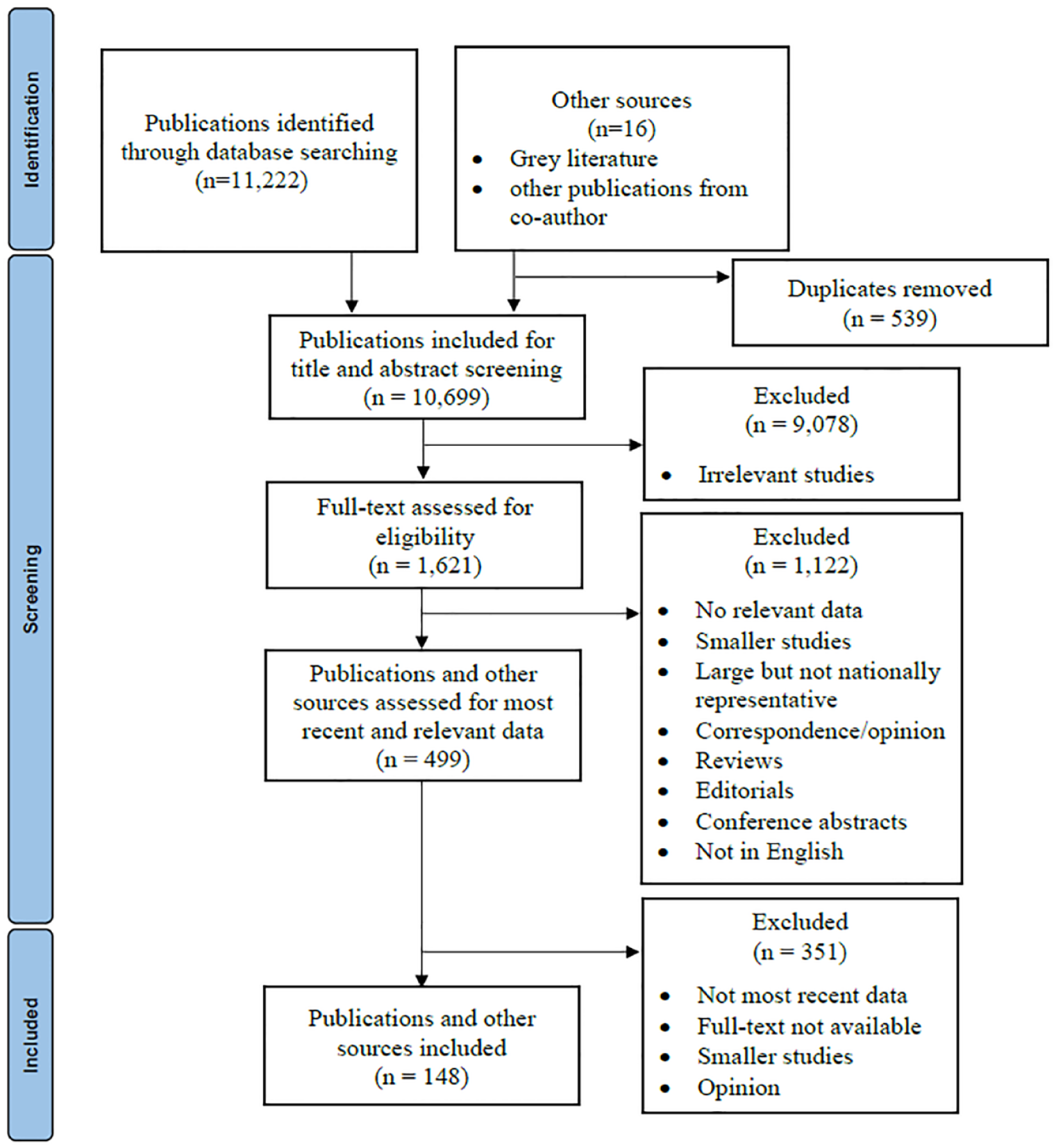
Screening and selection of published articles and relevant reports.
Availability of reperfusion services around the world.
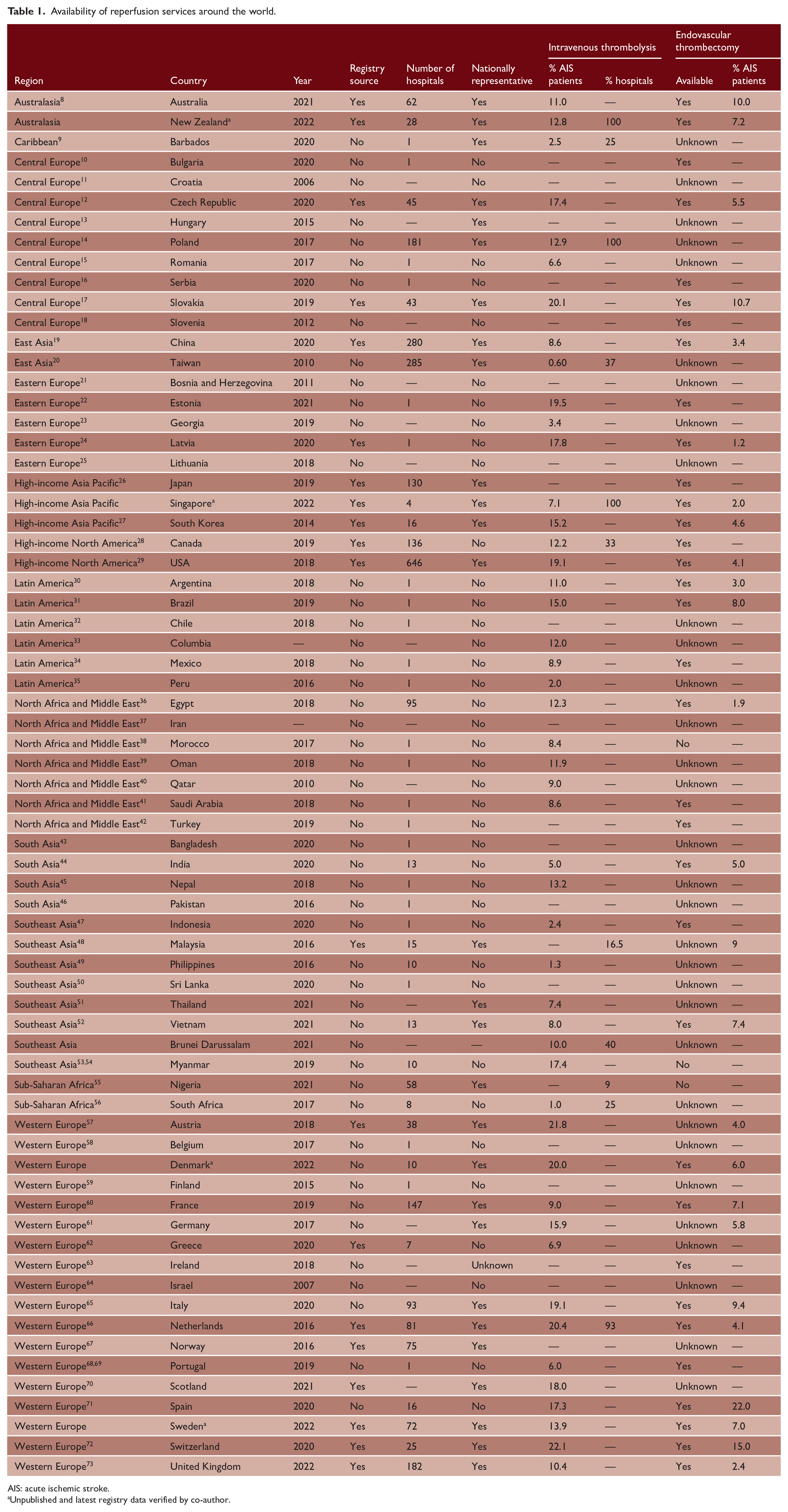
AIS: acute ischemic stroke.
Unpublished and latest registry data verified by co-author.
Provision of acute stroke reperfusion services
There was evidence of the availability of intravenous thrombolysis services in all 70 countries (Table 1), including 44 high-income countries (HICs; 62.9%), 14 upper-middle-income countries (20.0%), 10 lower-middle-income countries (14.3%), and 2 low-income countries (i.e. Nepal and Democratic Republic of the Congo; 2.9%). We found evidence of the availability of endovascular thrombectomy services in 33 countries (Table 1), including 22 HICs (67.7%), 8 upper-middle-income countries (24.2%), and 3 from lower-middle-income countries (i.e. Egypt, India, and Vietnam; 9.1%). There was no evidence of the availability of endovascular thrombectomy services in any of the low-income countries with published data on intravenous thrombolysis services. Approximately half of the countries with evidence of endovascular thrombectomy services were in Western Europe (10 countries) or Central Europe (5 countries; Figure 2).
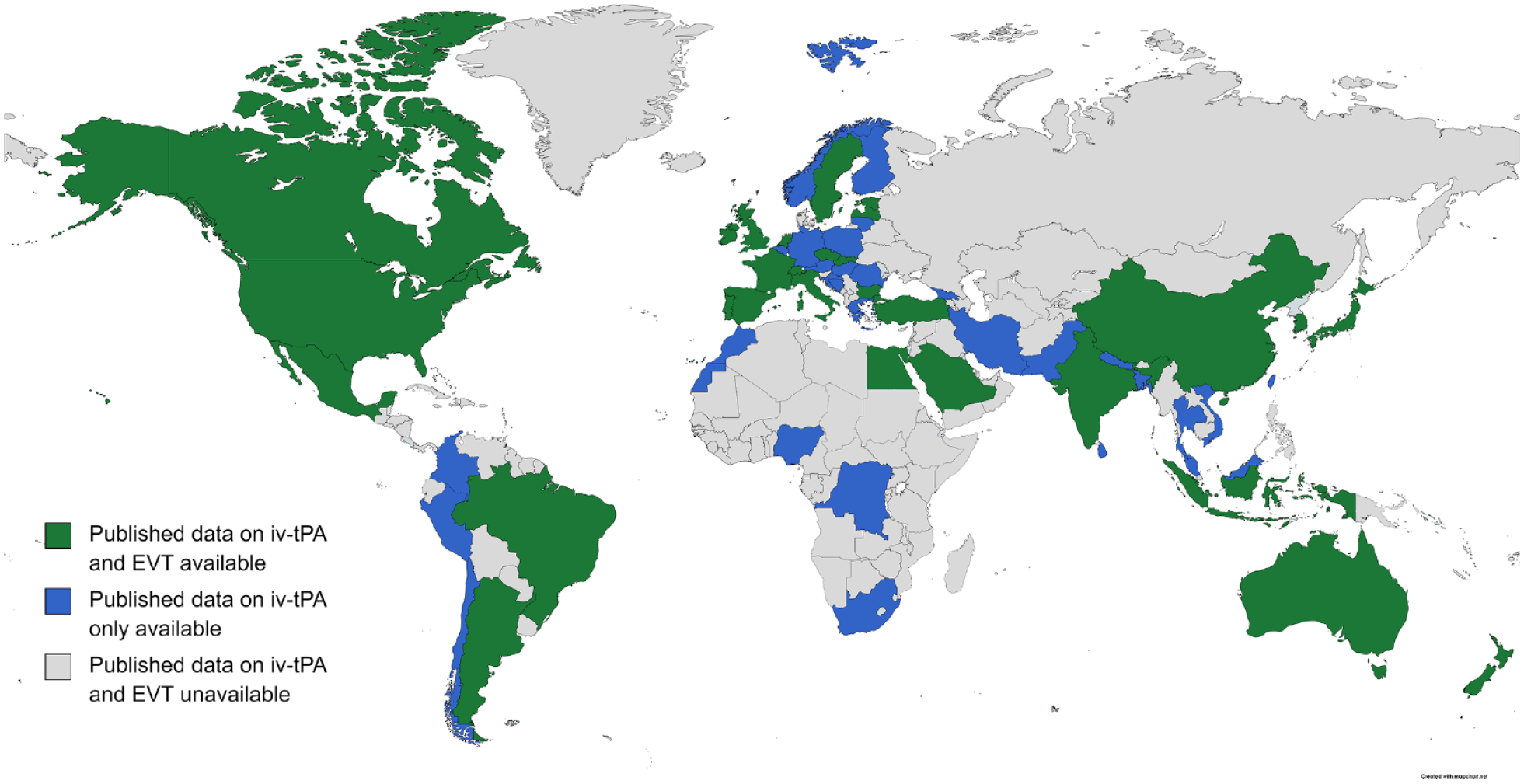
Map showing the availability of intravenous thrombolysis and endovascular thrombectomy services around the world.
We identified 14 countries with nationally representative and recent data (from 2019 onwards) on the proportion of patients with ischemic stroke provided with reperfusion services. This included 12 countries with information on both intravenous thrombolysis and endovascular thrombectomy, and two countries (Scotland and Barbados) with information on intravenous thrombolysis only. Among countries with nationally representative data, the proportion of patients with ischemic stroke treated with thrombolysis ranged from <10% (Singapore, China, France, Barbados), 10–14% (the United Kingdom, Australia, New Zealand, Sweden), and ⩾15% (Czech Republic, Scotland, Denmark, Italy, Slovakia, Switzerland; Table 1). This proportion ranged from <5% (Singapore, the United Kingdom, China), 5–9% (Denmark, Czech Republic, New Zealand, Sweden, France, Italy), and >10% (Australia, Slovakia, Switzerland) for the provision of endovascular thrombectomy.
Availability of stroke telemedicine services
We identified 74 stroke telemedicine programs, with 69 programs located in HICs (Table 2). The majority of the stroke telemedicine programs identified were located in the United States (n = 39; 52.7%; Figure 3). Other countries with multiple programs identified included Germany (n = 7), Spain (n = 4), Australia (n = 3), France (n = 3), Italy (n = 3), and India (n = 2). Only one program was identified in Hong Kong, Laos, New Zealand, Norway, Scotland, Singapore, Taiwan, Thailand, and England. Among 68 programs (91.9%) in which the model for the telemedicine program was reported, 56 (82.4%) operated with one central service (hub) providing telemedicine support to multiple spoke hospitals (i.e. “hub and spoke” model). There were three single-center programs, that is Aachen (Germany), Hallingdal (Norway), and Porto Alegre (Brazil), and one program in the East of England described as a horizontal hubless model (n = 7 hospitals). We identified only three stroke telemedicine programs in the United States described to have nationwide coverage, including the Veteran’s Affairs National Telestroke Program (n = 40 hospitals) TelaDoc Health (n = 132 hospitals), and the Telespecialist company (n = 171 hospitals). the largest identified stroke telemedicine program outside of the United States was based in India (100 hospitals: 22 hubs and 78 spokes).
Availability of stroke telemedicine services around the world.
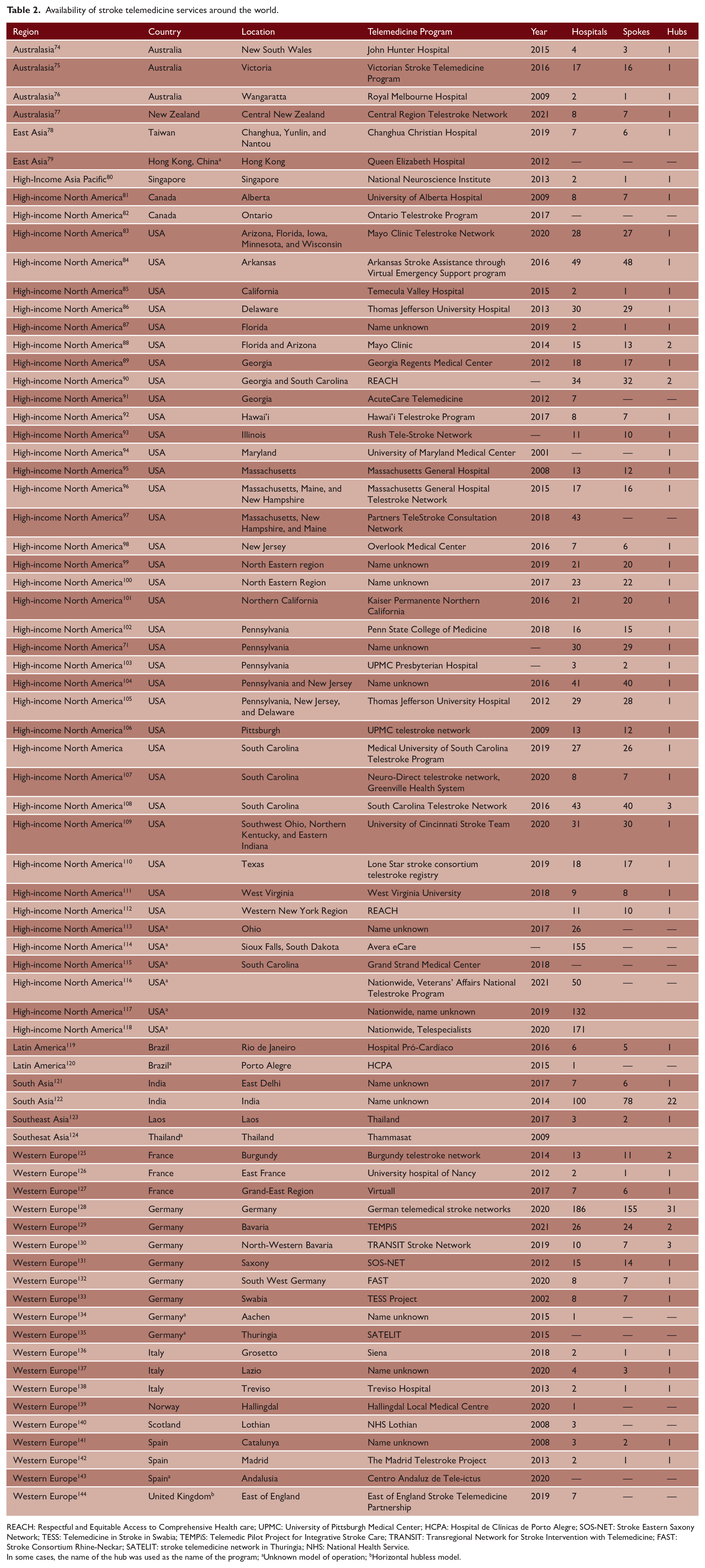
REACH: Respectful and Equitable Access to Comprehensive Health care; UPMC: University of Pittsburgh Medical Center; HCPA: Hospital de Clínicas de Porto Alegre; SOS-NET: Stroke Eastern Saxony Network; TESS: Telemedicine in Stroke in Swabia; TEMPiS: Telemedic Pilot Project for Integrative Stroke Care; TRANSIT: Transregional Network for Stroke Intervention with Telemedicine; FAST: Stroke Consortium Rhine-Neckar; SATELIT: stroke telemedicine network in Thuringia; NHS: National Health Service.
In some cases, the name of the hub was used as the name of the program; aUnknown model of operation; bHorizontal hubless model.
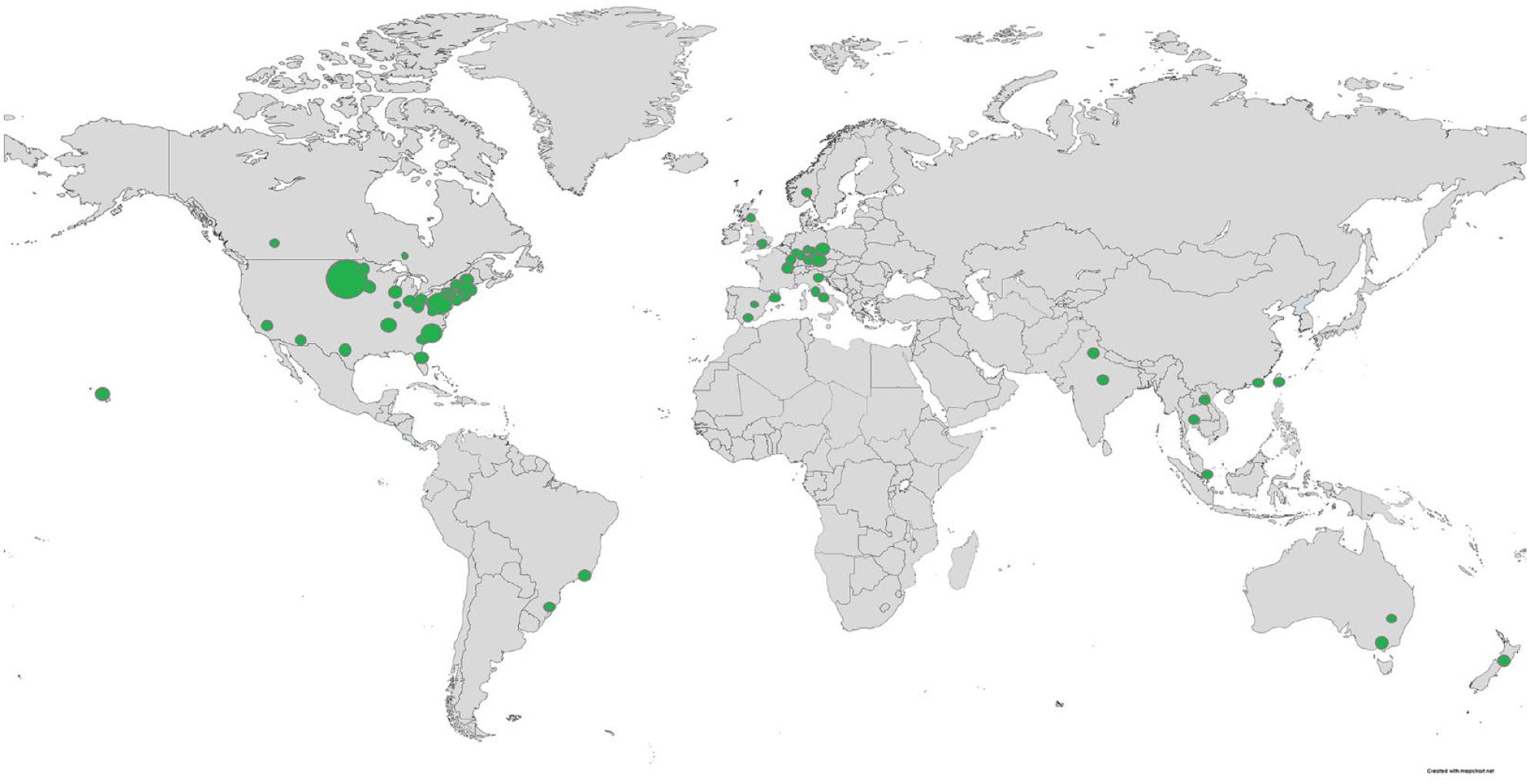
Map illustrating the number of stroke telemedicine services around the world. The size of the dot in a location reflects the number of services available in that location.
Availability of mobile stroke unit pre-hospital ambulance services
We identified 16 MSUs in the literature, 14 of which were already listed in the PRESTO repository of active MSUs. We found one MSU in Homburg (Germany) that appeared to be inactive (https://www.mobile-stroke-unit.org/), and another in Tennessee, USA, in implementation phase. 145 In the PRESTO registry, there were 30 active MSU services as of August 2023. Twenty-four of these active MSUs (80%) were located in HICs, 19 of which were located in the United States alone. Other MSU programs present in the American region included those located in Edmonton (Canada), Brasilia (Brazil), and Buenos Aires (Argentina). Four MSUs were present in Europe, all located in Western Europe, including in Berlin (Germany), Hamburg (Germany), Drobak (Norway), and Ipswich (England). Similarly, four MSUs were present in Southeast Asia, located in Assam (India), Coimbatore (India), Bangkok (Thailand), and Sichuan (China). There was one MSU present in Imo (Nigeria) and Melbourne (Australia).
Discussion
In this article, we presented a repository of the latest published country-specific data on the availability of reperfusion services directly within hospitals, and those facilitated via telemedicine or MSU services. We described the worldwide coverage of reperfusion services and highlighted regions where data are limited or not recent.
The information presented likely illustrates disparities in access to reperfusion services for acute stroke around the world. Currently, the WSO is leading a call to action for increasing access to thrombectomy provision as a game-changing treatment for stroke. The policy objectives of the Stroke Action Plan for Europe also include targets by 2030 for guaranteeing access to reperfusion services to 95% of eligible patients, and achieving intravenous thrombolysis rates above 15% and endovascular therapy above 5% in all European countries. 2 Therefore, the data reported in this review are necessary for underpinning these objectives and targets, commensurate with investments in workforce and system improvements that are required to ensure equitable access to reperfusion services.
Telemedicine services facilitate access to intravenous thrombolysis, especially in more remote areas or smaller hospitals, with this service requiring a robust technical setup, both at the hub and spoke hospitals. Targets to provide all people within a country access to acute stroke reperfusion services may be ambitious. For example in France, a national strategy to have a stroke telemedicine service that began in 2011 is still in progress. 146 However, the required investments are economical compared with other solutions (e.g. MSUs or stroke air ambulances).147,148 In addition, stroke telemedicine services are used in many regions, but nationwide approaches are rare, and solutions are often regionally based and not standardized. Significant progress has been made in the United States (2019), where it was estimated that 96% of the population had access to a stroke center or stroke telemedicine service. 149 Also, there is evidence from Germany that wider adoption of stroke telemedicine service is feasible and safe, with 38,895 consultations successfully undertaken across 14 telemedicine networks in nine German states. 128
The availability and extent of MSU services varied widely within each country, and implementation was often limited to specific regions or cities. MSUs were more common in the United States, with several cities successfully integrating MSUs into their emergency response systems. Investments to establish MSUs are considerable, including costs of procuring equipment, training, and integrating into existing health care systems. However, the benefits offset the upfront investment with reductions in time to diagnosis and earlier provision of time-critical treatments, especially in settings requiring extensive time to travel to hospital. 150
An important finding from this review is that contemporary patient-level data on availability of reperfusion services remain scarce, even in HICs. Based on published data, intravenous thrombolysis and endovascular thrombectomy services were notably absent in low-income countries. Potential barriers to providing reperfusion services in these countries include lack of necessary infrastructure, equipment, and trained personnel, and high costs associated with procuring reperfusion drugs/devices. For countries with no data available on provision of reperfusion services, it is difficult to ascertain current gaps in this important aspect of stroke in these countries. We also found huge variations in access to reperfusion services in HICs, which underlines the need for investment in robust stroke care services and infrastructure globally.
National stroke clinical registries are an important source of recent standardized data. To allow for reliable comparison of performance in stroke care (e.g. the provision of intravenous thrombolysis) within and between countries over time, the Action Plan for Stroke in Europe has recently established a tool (Stroke Service Tracker) for reporting stroke data in European countries on an annual basis. 151 This initiative also supports development of reliable stroke registries in European countries. Establishment of such tools in other regions could facilitate collection of data essential for reliably monitoring the provision of reperfusion services, globally.
There are also current initiatives to map the availability of reperfusion services in certain regions. In Europe, although there was an increase in reperfusion therapy rates in many countries between 2016 and 2019 (based on expert opinion), this was halted in 2020. 152 The authors highlighted the ongoing inequalities in acute stroke treatment across Europe. 152 Similarly, there is variability in the standard of acute stroke care reported in Latin America, with reperfusion services reported to be available for a small proportion of the population in several countries.153,154 In addition, efforts to map reperfusion services are being conducted in Southeast Asia (personal communication with DADS).
Much can be learned from countries identified in this report that represent similar socio-demographic and economic profiles. International collaborations and partnerships between HICs, and lower-middle-income or low-income countries could promote knowledge transfer, training opportunities, and resource sharing. One such initiative is the international stroke telemedicine service. This new model of care appears feasible and has the potential to improve access to specialist care, and timely reperfusion services, in regions (e.g. lower-middle-income and low-income countries) where stroke specialist input is limited.123,155 These alliances may build local capacity, improve infrastructure, and enhance stroke care networks.
There are some limitations of this review. For nearly half of the countries, the most recent data on the availability of intravenous thrombolysis, endovascular thrombectomy, and stroke telemedicine services were collected prior to 2019. We acknowledge there may be delays in publishing recent data that may have impeded our ability to know with certainty the current gaps in these aspects of stroke care, and our findings may not fully represent the current state of stroke care services in all countries. Indeed, there is evidence from surveys of national organizations that reperfusion services are available in more countries than identified in this review.152–154 Our findings rely on published patient-level data, and there may be bias in favor of countries with more research infrastructure or motivation to publish data on stroke services. Where possible, data from publications were supplemented by unpublished and verified data available from co-authors or trusted websites (e.g. PRESTO and RES-Q repositories) which are routinely updated. Also, some countries may have made significant strides in acute stroke care that have not yet been published or are published in languages other than English. The quality and reliability of data may also vary across different countries and sources. To keep the repository up-to-date and to assist us in updating this review, we encourage readers to submit any relevant unpublished country-specific data on reperfusion services to the corresponding author.
Conclusion
Despite remarkable advancements in reperfusion therapies for stroke, it is evident from published data that their availability and provision remain unevenly distributed globally. Bridging this treatment gap requires a multifaceted approach, including advocacy on the importance of reperfusion therapies to drive policy changes and secure additional funding for stroke programs, investment in infrastructure, workforce training, awareness campaigns, and collaborative efforts. By providing an updated repository of the latest country-specific data on stroke care services, this review can inform future policy and funding decisions aimed at improving access to evidence-based stroke care worldwide, and can inform organizations, such as the WSO, to advocate for gaps in coverage to be addressed. By prioritizing stroke care as a global health priority, we can strive toward equitable access to reperfusion therapies and improve stroke outcomes worldwide.
Footnotes
Acknowledgements
Analyses and interpretations of the data are of the authors alone.
Author contributions
J.K., M.T.O., T.T., and D.A.C. contributed equally. J.K., M.T.O., and T.T. contributed to the design, undertook literature search, data collection, data analyses, and interpretation, wrote the first draft of the article. D.A.C. contributed to the design, data interpretation, and wrote the first draft of the article, and revised the article. All authors interpreted the data, provided additional data reports as relevant, revised and approved the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: D.A.C. reports Research Fellowship support from the National Health and Medical Research Council (grant no. 1154273).