
Abstract
Objective:
Hypotension is recognized as a common complication after carotid artery stenting, but its incidence and the risk factors associated with it are uncertain. Therefore, we performed a systematic review and meta-analysis to investigate and identify risk factors for hypotension after surgery.
Methods:
We retrieved risk factors from eight databases for case-control and cross-sectional studies of hypotension after carotid artery stenting according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines on 28 November 2022. Data were analyzed by using R4.2.1 and Review Manager 5.3.
Results:
A total of 2843 samples were searched, and 17 publications were included in the analysis. The meta-analysis results showed that the incidence of hypotension after surgery was 28.6% (95% confidence interval [CI] (0.225, 0.347)). Age ⩾ 65 years (odds ratio [OR] = 4.55, 95% CI (2.50, 8.29), P < 0.00001), stenosis site (bulb) (OR = 4.41, 95% CI (2.50, 7.79), P < 0.00001), severe stenosis (OR = 3.56, 95% CI (1.62, 7.85), P = 0.002), stenosis proximity (⩽ 10 mm) to bifurcation (OR = 2.69, 95% CI (1.74, 4.15), P < 0.00001), calcified plaques (OR = 4.64, 95% CI (1.93, 11.14), P = 0.0006), post-balloon dilation (OR = 5.95, 95% CI (2.31, 15.31), P = 0.0002), bilateral carotid stenting (OR = 30.51, 95% CI (2.33, 399.89), P = 0.009), and intravenous fluid intake/mL on the first postoperative day (mean difference = 444.99, 95% CI (141.40, 748.59), P = 0.004) were risk factors for hypotension after surgery.
Conclusions:
A high incidence of hypotension was observed after carotid artery stenting. Age, stenosis site, severe stenosis, stenosis proximity to bifurcation, calcified plaques, post-balloon dilation, type of surgery, and intravenous fluid intake were identified as risk factors.
Introduction
Carotid artery stenting (CAS) is a minimally invasive procedure for the treatment of carotid stenosis in patients with 50%–99% carotid stenosis who are intolerant to carotid endarterectomy (CEA) therapy.1,2 The 2023 European Society for Vascular Surgery guidelines recommended that statin therapy should be started preoperatively for patients planning to undergo endarterectomy or stenting. 2 Also, to prevent hemodynamic instability during CAS procedures, the management procedures included hydration, discontinuation of antihypertensive medications on the morning of the operation, continuous ECG/blood pressure monitoring, and venous access. 2 Some studies have demonstrated that hypotension, hypertension, and hyperperfusion syndrome sometimes happen after CEA and CAS, and hypotension is more common after intervention; about 23.1%–31.2% of cases.3 –5 Studies confirmed that hypotension after CAS may increase the risk of stroke, extensively prolong the in-hospital time, and even cause death.6 –9 Previous studies have shown that severe stenosis and post-balloon dilatation represent some risk factors for hypotension in CAS.10 –12 Hypotension is a state in which the arterial pressure in the body’s circulation is lower than normal. There are no uniform criteria for the diagnosis of hypotension. Blood pressure below 90/60 mmHg in the upper extremities of adults is generally considered to indicate hypotension. 13 To our knowledge, no systematic evaluation has comprehensively summarized the risk factors for hypotension after CAS. Knowledge of these risk factors can help identify high-risk patients and manage them in a targeted manner. Thus, in this study, we performed a systematic review and meta-analysis to review the literature and identify risk factors for hypotension after CAS.
Materials and methods
This systematic review and meta-analysis were registered in the National Institute for Health Research PROSPERO database with registration number CRD42022364651. This study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 14
Literature search strategy
The incidence and risk of hypotension after CAS case-control studies and cross-sectional studies were independently searched by two investigators in eight databases, according to the PRISMA guidelines. 14 The searched databases included PubMed, Cochrane Library, Embase, Web of Science, China Biomedical Literature Database, China Knowledge Network, Wanfang Database, and Chinese Science and Technology Journal Database (VIP) on 28 November 2022. The literature search strategies used a combination of Medical Subject Heading terms and entry terms. The search terms included CAS, carotid angioplasty and stent, carotid stenosis, risk factor, influence factors, relative factor, relative risk, predict, hypotension, low blood pressure, vascular hypotension, and hemodynamics.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) study type: all case-control and cross-sectional studies; (2) study population: patients with preoperative carotid stenosis clearly diagnosed by digital subtraction angiography who underwent unilateral or bilateral CAS, patient nationality and race were not restricted; (3) exposure factors: preoperative disease factors, intraoperative factors, and postoperative factors that may be related to the occurrence of hypotension after carotid stenting; (4) outcome indicators: risk factors for the occurrence of hypotension in patients after CAS. The exclusion criteria were (1) non-Chinese and English literature; (2) duplicate publications; (3) literature that had incorrect data; and (4) literature that was not published in the last 5 years. In addition, ⩾2 clinical studies reporting exposure factors were subjected to meta-analysis.
Literature screening
Literature screening was independently performed by two investigators. Duplicated literature was excluded by using the literature management software Endnote. By reading the titles and abstracts, the literature that did not meet the inclusion criteria was initially excluded. The full text of the potentially eligible literature was further screened. During the full-text screening, we carefully retrieved items among the potentially eligible literature from the initial screening. If the information report was incomplete, the corresponding authors of the literature were contacted to obtain more relevant information. We tracked the references and the cited references to include other potentially relevant studies as much as possible.
Data extraction
Two researchers used Excel 2019 to collect extracted data from the included studies. Extraction encompassed literature ID (first author + year of publication), study type, sample size, the incidence of postoperative hypotension in CAS, exposure factors, and outcome measures. Two researchers independently conducted the “data extraction and methodological quality assessment.”
The hypotension in our study was defined as a state in which the arterial pressure in the body’s circulation is lower than normal. There were no uniform criteria for the diagnosis of hypotension, so the definition of hypotension in our study was not standardized and depended on the included studies with a clear source of the criteria of hypotension in their method part.
Risk of bias assessment
Any disagreement was resolved via communication with a third researcher. The methodological quality of case-control studies was evaluated according to the Newcastle–Ottawa Scale, 15 which includes 8 items with a total score of 9 points, with 1 point for meeting the target guidelines and 0 points for not meeting the guidelines. If the score was ⩾6, it was included in the meta-analysis. The quality of cross-sectional studies was evaluated according to the quality evaluation criteria for cross-sectional studies recommended by the Agency for Health Care Research and Quality. 16 One point was assigned for meeting the target guidelines, and 0 points were assigned for not meeting the guidelines. This method consisted of 11 items, with a total score of 11. A rating of 0–3 indicates low quality, 4–7 indicates medium quality, and 8–11 indicates high quality.
Statistical analysis
In this study, the incidence of hypotension after CAS and its 95% CI were calculated in R 4.2.1. The odds ratio (OR)/mean difference (MD) values and 95% CIs of risk factors for hypotension after CAS were also calculated by using Review Manager 5.3. The OR and 95% CI were used to express the count data, and the MD and 95% CI were selected for the measurement data. Moreover, the χ2 test and I2 were used to evaluate the statistical heterogeneity. In addition, a meta-analysis was performed by using a fixed-effects model when P ⩾ 0.10 and I2 ⩽ 50%. When P < 0.10 and/or I2 > 50%, the data were retested by using a random-effects model. Egger linear regression tests and funnel plots were combined to assess potential publication bias in the literature at a test level of α = 0.05 by R4.2.1.
Results
Literature search and screening results
A total of 1430 literature records were retrieved, including 435 records in Chinese and 995 records in English. Finally, 173 –5,7,10 –12,17 –26 studies were finally included in the meta-analysis. The flow of the literature screening process is shown in Figure 1.

PRISMA flowchart of eligible studies.
Basic characteristics of the included literature
The 173 –5,7,10 –12,17 –26 studies included 73,7,11,17 –20 case-control studies and 104,5,10,12,21 –26 cross-sectional studies. In addition, the sample contained a total sample size of 2843 cases, as well as 897 patients with postoperative hypotension and 14 patients with exposure factors (Table 1).
Basic characteristics of the 17 included articles.

(1) Age ⩾ 65 years; (2) hypertension; (3) stenosis site (bulb); (4) severe stenosis; (5) severe contralateral carotid stenosis; (6) the stenosis proximity (⩽ 10 mm) to bifurcation; (7) symptomatic stenosis; (8) ulcerated plaques; (9) calcified plaques; (10) stent type; (11) bilateral carotid stenting; (12) post-balloon dilation; (13) intravenous fluid intake/mL in the first 24 h after surgery; (14) sex (male).
Methodological quality evaluation of the included literature
The quality scores of the included case-control studies ranged from 7 to 9. The quality scores of the included cross-sectional studies ranged from 7 to 11. All the studies were scored as being above-medium-quality literature.
The overall incidence of hypotension after CAS
The incidence of hypotension after carotid stenting was 28.6% (95% CI (0.225, 0.347)) (Figure 2). There was high heterogeneity between the studies (I2 = 96%, P < .01); therefore, a random-effects model was used. The sensitivity analysis was plotted in combination with R4.2.1. The results did not significantly change by converting to a fixed-effects model (Figure 3).
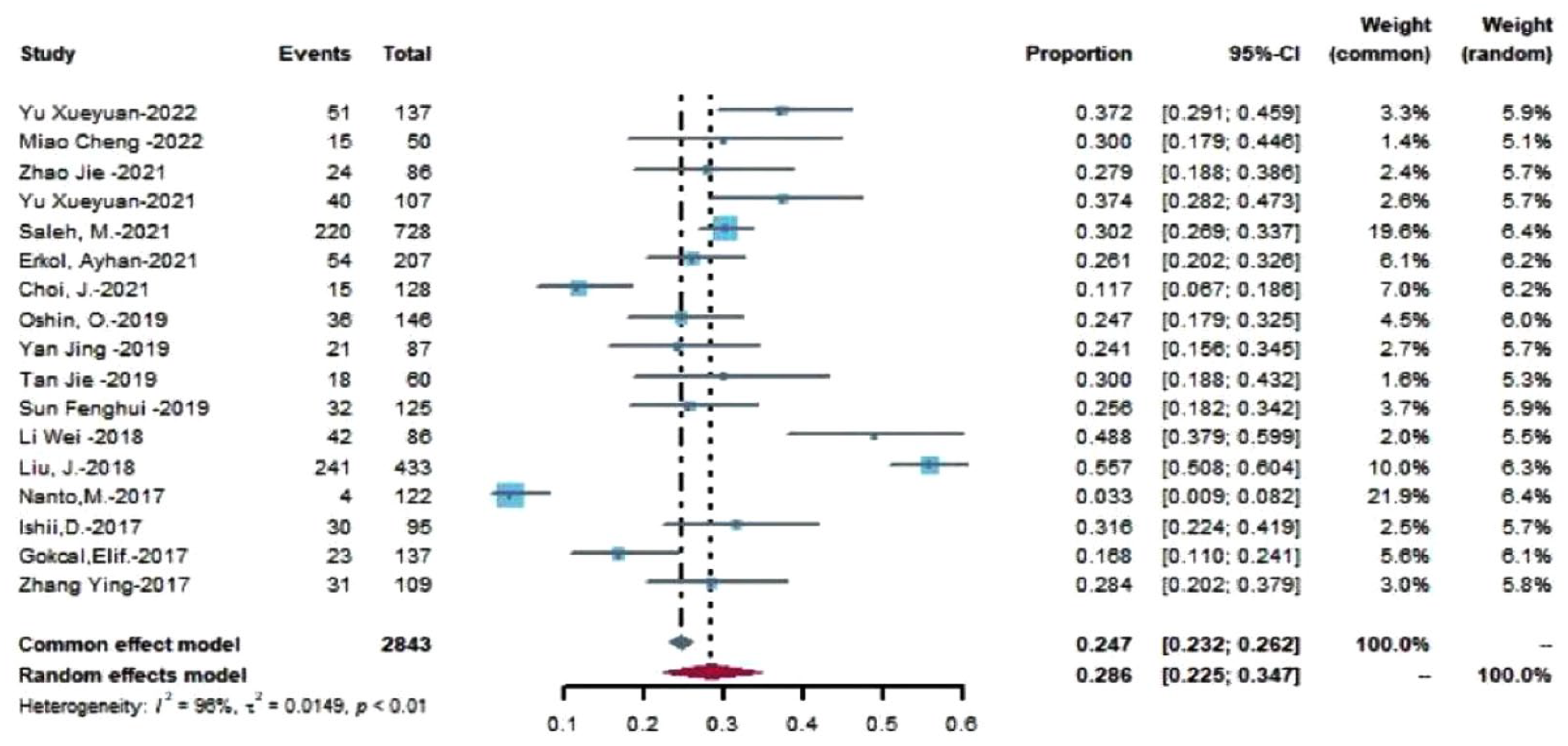
Meta-analysis of the incidence of hypotension after carotid artery stenting.
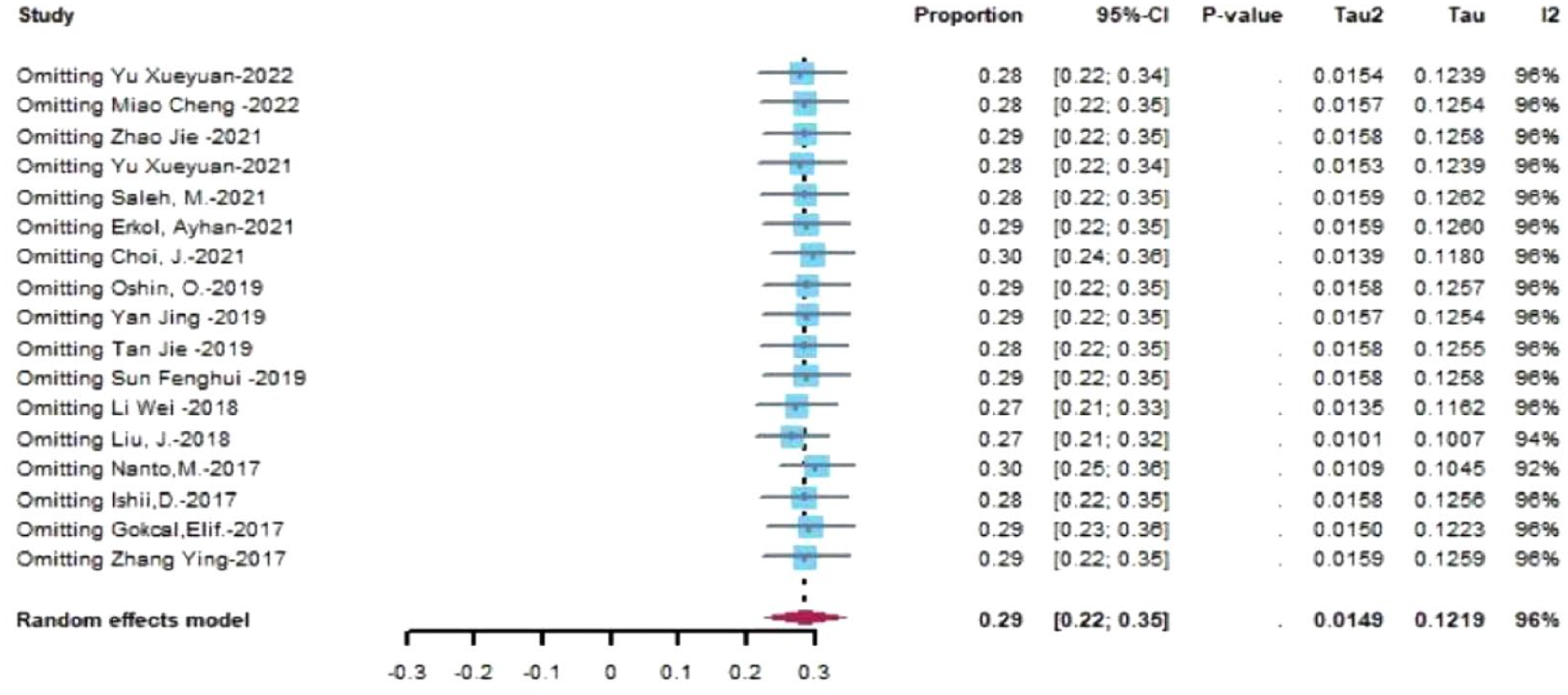
Sensitivity analysis of a meta-analysis of the incidence of hypotension after carotid artery stenting.
Meta-analysis results
Preoperative factors
The meta-analysis showed that age ⩾ 65 years (OR = 4.55, 95% CI (2.50, 8.29), P < 0.00001), stenosis site (bulb) (OR = 4.41, 95% CI (2.50, 7.79), P < 0.00001), severe stenosis (OR = 3.56, 95% CI (1.62, 7.85), P = 0.002), stenosis proximity (⩽10 mm) to bifurcation (OR = 2.69, 95% CI (1.74, 4.15), P < 0.00001), and calcified plaques (OR = 4.64, 95% CI (1.93, 11.14), P = 0.0006) were risk factors for hypotension in patients after CAS. Moreover, sex (male) (OR = 1.09, 95% CI (0.89, 1.33), P = 0.42), hypertension (OR = 1.59, 95% CI (0.58, 4.36), P = 0.36), severe contralateral carotid stenosis (OR = 2.69, 95% CI (0.76, 9.48), P = 0.12), symptomatic stenosis (OR = 1.66, 95% CI (0.66, 4.22), P = 0.28), and ulcerated plaques (OR = 2.00, 95% CI (0.53, 7.55), P = 0.30) were not associated with the development of hypotension in patients after CAS (Table 2).
Meta-analysis results of risk factors for the development of hypotension after CAS.
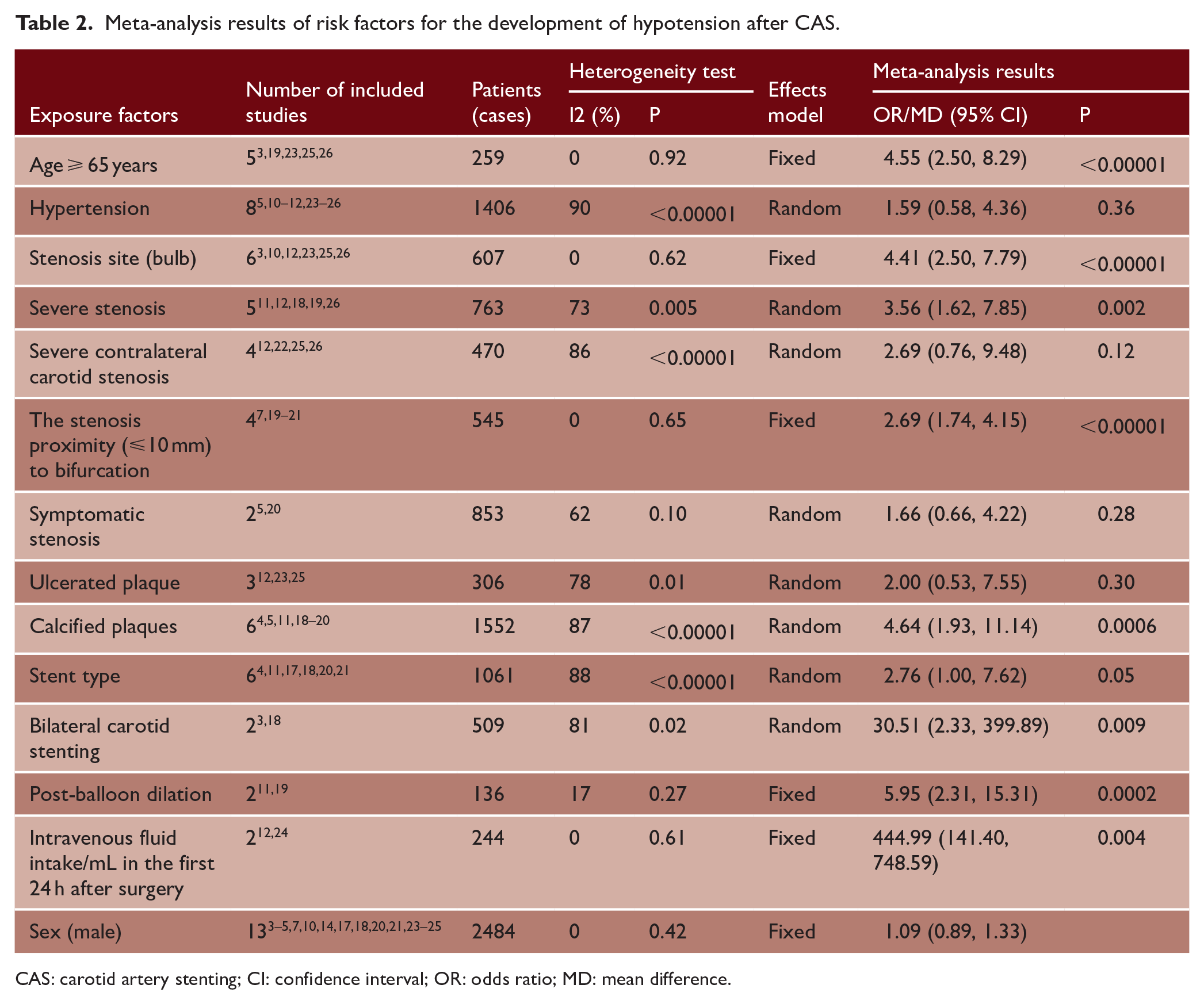
CAS: carotid artery stenting; CI: confidence interval; OR: odds ratio; MD: mean difference.
Intraoperative factors
The meta-analysis showed that post-balloon dilation (OR = 5.95, 95% CI (2.31, 15.31), P = 0.0002) and bilateral carotid stenting (OR = 30.51, 95% CI (2.33, 399.89), P = 0.009) were risk factors for the development of hypotension in patients after CAS (Table 2). However, stent type (OR = 2.76, 95% CI (1.00, 7.62), P = 0.05) was not associated with the development of hypotension in patients after CAS (Table 2).
Postoperative factors
The meta-analysis showed that IV fluid intake/mL on the first postoperative day (MD = 444.99, 95% CI (141.40, 748.59), P = 0.004) was a risk factor for the development of hypotension in patients with CAS after surgery (Table 2).
Sensitivity analysis and publication bias
A sensitivity analysis was performed by converting the fixed-effects model and the random-effects model. Specifically, the combined OR/MD values of the 13 risk factors and their 95% CIs were calculated under the fixed-effects model and the random-effects model, respectively. The results did not significantly change (Table 3).
Results of sensitivity analysis of risk factors.
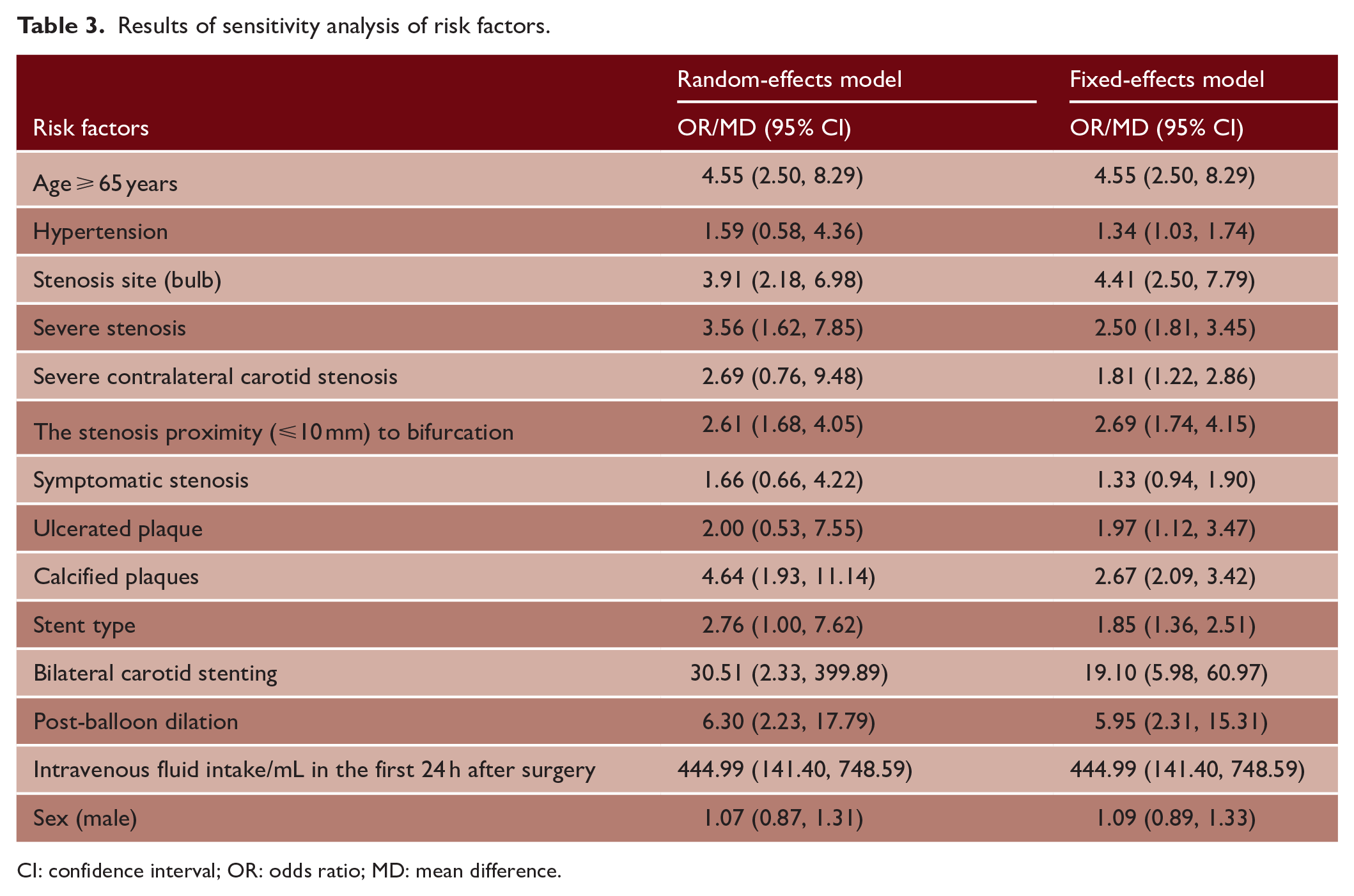
CI: confidence interval; OR: odds ratio; MD: mean difference.
Publication bias
The funnel plot results suggested some publication bias was present in the included studies, with heterogeneity being observed in some of the studies (Figure 4). Egger’s test (t = 1.35, P = 0.1962) further confirmed the funnel plot results, which may be related to the disparity in sample sizes among the included studies (Figure 5).
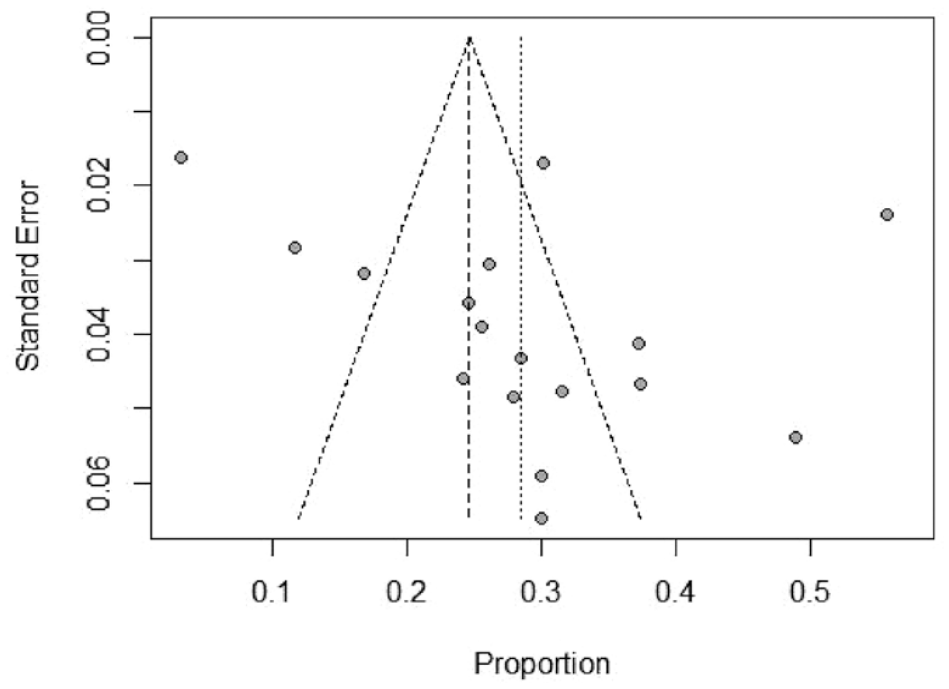
Funnel plot of meta-analysis for publication bias of included studies.
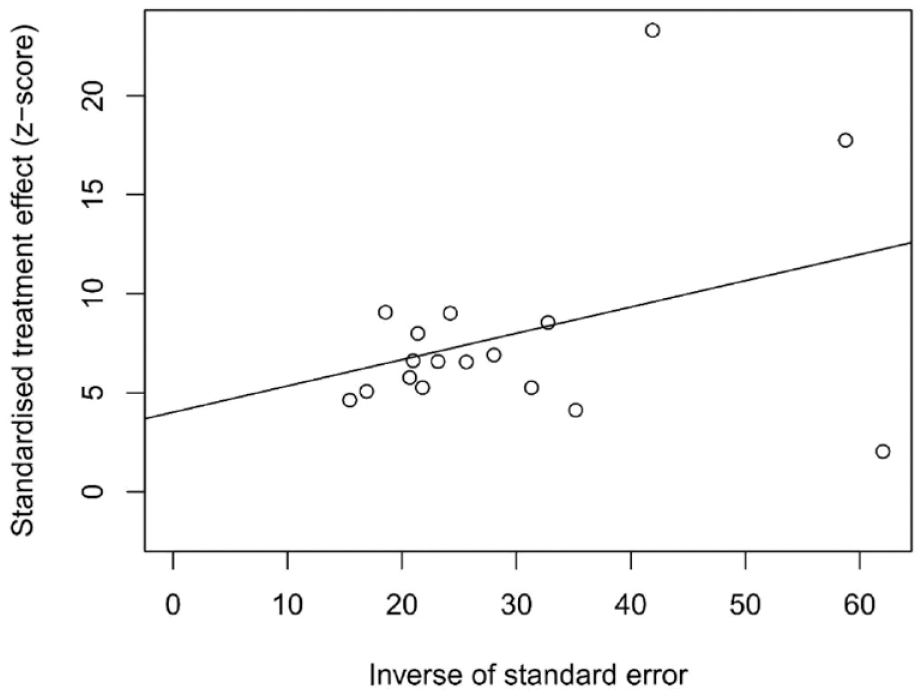
Egger’s test plot of meta-analysis for publication bias of included studies.
Discussion
High incidence of hypotension after CAS
The results of this study demonstrated a 28.6% (95% CI (0.225, 0.347)) incidence of hypotension after carotid stenting, which is similar to the results of previous studies. Previous studies have suggested that the incidence of hypotension after carotid stenting was approximately 23.1%–31.2% according to different criteria.3 –5 Among the 17 included studies, 14 studies defined hypotension as a systolic blood pressure <90 mmHg in patients despite adequate treatment after CAS. However, 1 Korean study and 1 Japanese study defined it as a systolic blood pressure <80 mmHg,7,10 and 1 Japanese study defined it as a systolic blood pressure <100 mmHg, 17 which may be because there are no uniform criteria for the diagnosis of hypotension. 13 The occurrence of postoperative hypotension in CAS patients is the result of the synergistic effect of multiple factors. The carotid sinus is located at the beginning of the internal carotid artery or at the bifurcation of the carotid artery. When implementing CAS, carotid sinus pressure receptors are stimulated, and the development of hypotension may occur. The carotid artery is an important and vital blood vessel for the blood supply to the brain, and transient or persistent hypotension can affect cerebral perfusion and body circulation. 27 Previous studies have confirmed that persistent hypotension can cause cerebral hypoperfusion, aggravate existing cerebral ischemic symptoms, increase hospitalization times, and even increase the risks of cerebrovascular disease.22,27 In addition, patients with postoperative hypotension in CAS are more prone to perioperative transient ischemic attack, stroke, and infarction complications than other patients. 28 Therefore, it is crucial to identify the risk factors for postoperative hypotension in CAS patients for its prevention.
Preoperative factors
The results of this meta-analysis showed that age ⩾65 years, bulb stenosis, severe stenosis, stenosis proximity (⩽10 mm) to bifurcation, and calcified plaques were risk factors for the occurrence of hypotension in patients after CAS. The incidence of postoperative hypotension after CAS was 4.55-times higher in those individuals aged ⩾65 years than in those individuals aged <65 years. This result is consistent with the study of Lamanna et al. 29 This effect may be due to the replacement of pacemaker cells in the sinus node by fibrous connective tissue in elderly patients, thus resulting in a slower heart rate. However, some researchers23,25,30 have suggested that patients aged <65 years have a higher risk of hemodynamic depression (HD) after CAS. This needs to be further explored in-depth in the future because of the limited sample size included in this study.
The results of this study demonstrated a 4.41-fold increased risk of hypotension in patients with stenosis occurring in the bulb after CAS, which is consistent with the findings of Rubio et al. 9 and Gupta et al. 31 Specifically, they found that the carotid sinus is easily irritated by carotid stenting and balloon dilation, thus triggering HD.
In addition, CAS surgery in patients with calcified plaques increases the risk of postoperative hypotension by 4.64 times. This may result from the greater pressure required to be applied to the calcified plaque during CAS surgery,9,32 which causes the calcified plaque surface to rupture. The dilatability of the vessel wall was reduced, thus causing the sensitivity of the carotid sinus to be reduced and triggering HD. However, the study of Mylonas et al. 33 demonstrated no association between calcified plaque and the occurrence of hypotension in CAS subjects. This suggests that the relationship between calcified plaques and the development of hypotension after CAS is complex in nature and requires further investigation.
In addition, this study also observed a 3.56-fold increased risk of postoperative hypotension in patients with severe stenosis. A 2.69-fold increased risk of postoperative hypotension was observed in patients with stenosis proximal (⩽10 mm) to the bifurcation. This effect may be related to the direct stimulation of the carotid sinus due to the restoration of cerebral blood flow after the alleviation of severe carotid stenosis, which causes reflex HD. In addition, as the carotid sinus is located at the beginning of the internal carotid artery or at the bifurcation of the carotid artery, the outer wall of the carotid sinus is rich in elastic fibers and special neuroreceptors. It is one of the pressure-sensing systems in the human body and mainly experiences the stimulation of carotid vasodilation. 19 Therefore, greater stimulation of the carotid sinus by stent placement and balloon dilation during CAS corresponds to a more pronounced elevation of vagal tone, making it more likely that the HD state will occur.
Intraoperative factors
The study found that post-balloon dilation increased the risk of postoperative hypotension by 5.95 times in CAS. This is mainly due to the fact that during the intraoperative operation of CAS, balloon dilation produces mechanical dilation and pulling on the carotid sinus. 12 This may lead to the functional stimulation of the carotid sinus receptors. Subsequently, the sympathetic tone at the end of the nucleus tractus solitarius triggers the carotid sinus reflex. Thus, there was a greater risk of postoperative hypotension, which is consistent with the results of the previous literature. 30 Therefore, appropriate balloon expansion should be intraoperatively selected. Balloon expansion should follow the principle of sequential multiple expansion of small balloons, which generally corresponds to a balloon-to-vessel diameter ratio of 0.5 to 0.6. After the balloon is in place, it is slowly and briefly filled to standard pressure. If the balloon can be rapidly deployed, it is rapidly deflated to reduce the duration of compression of the carotid sinus. 19
In addition, this study also found that bilateral carotid stenting increased the risk of postoperative hypotension in CAS by 30.51 times. Compared to unilateral stenting, bilateral carotid stenting simultaneously stimulates bilateral carotid receptors and alters the intensity of carotid compliance. This may result in a greater risk of severe hemodynamic flow disturbances.30,34 –36 Liu et al. 18 found that bilateral CAS placement improved cerebral blood supply, thereby regulating blood pressure.
Postoperative factors
This study found that intravenous fluid intake/mL on the first postoperative day was strongly associated with the occurrence of hypotension after CAS. This effect may be due to the hypoperfused state, which is relatively simple to manage. Observation of the condition is vital and significant because of the adverse effects that arise if it occurs. Hence, early detection and management are necessary.12,24
Limitations
Our study only included the published literature in English and Chinese languages. This criterion may have produced some publication bias in the findings. In addition, some of the exposure factors, such as the nature of stenosis and the type of surgery, have not been sufficiently explored. This may lead to the possibility that their association with the occurrence of postoperative hypotension in CAS patients could not be clarified. Furthermore, some of the exposure factors, such as the degree of stenosis (severe), could not be combined in the literature because of inconsistent classification criteria. This may result in some missing information. It is worth noting that although our heterogeneity is high, we have validated the robustness of the results of this study by converting fixed- and random-effect models. Most of the included studies were single-center studies with selection biases and small sample sizes, which may also lead to biased results. Similarly, we expect more studies to focus on the correlation between exposure factors, such as advanced age, stenosis involving the balloon, posterior balloon dilation, and postoperative hypotension in patients with CAS.
Conclusions
In our meta-analysis, we found that the incidence of hypotension after CAS was high. This finding suggested that seniority, bulb stenosis, severe stenosis, stenosis proximity to bifurcation, calcified plaques, balloon dilation, bilateral carotid stenting, and intravenous fluid volume were significant independent risk factors for postoperative hypotension in CAS patients. Clinical staff should focus on these risk factors during the perioperative period of CAS. It is necessary to assess hypotension early and to take active prevention measures in the perioperative period to reduce the incidence of hypotension and to promote rapid recovery after CAS. In addition, this study emphasizes the need for further research in this area.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.