
Abstract
The rate of stroke-related death and disability is four times higher in low- and middle-income countries (LMICs) than in high-income countries (HICs), yet stroke units exist in only 18% of LMICs, compared with 91% of HICs. In order to ensure universal and equitable access to timely, guideline-recommended stroke care, multidisciplinary stroke-ready hospitals with coordinated teams of healthcare professionals and appropriate facilities are essential.
Established in 2016, the Angels Initiative is an international, not-for-profit, public–private partnership. It is run in collaboration with the World Stroke Organization, European Stroke Organisation, and regional and national stroke societies in over 50 countries. The Angels Initiative aims to increase the global number of stroke-ready hospitals and to optimize the quality of existing stroke units. It does this through the work of dedicated consultants, who help to standardize care procedures and build coordinated, informed communities of stroke professionals. Angels consultants also establish quality monitoring frameworks using online audit platforms such as the Registry of Stroke Care Quality (RES-Q), which forms the basis of the Angels award system (gold/platinum/diamond) for all stroke-ready hospitals across the world.
The Angels Initiative has supported over 1700 hospitals (>1000 in LMICs) that did not previously treat stroke patients to become “stroke ready.” Since its inception in 2016, the Angels Initiative has impacted the health outcomes of an estimated 7.46 million stroke patients globally (including an estimated 4.68 million patients in LMICs). The Angels Initiative has increased the number of stroke-ready hospitals in many countries (e.g. in South Africa: 5 stroke-ready hospitals in 2015 vs 185 in 2021), reduced “door to treatment time” (e.g. in Egypt: 50% reduction vs baseline), and increased quality monitoring substantially.
The focus of the work of the Angels Initiative has now expanded from the hyperacute phase of stroke treatment to the pre-hospital setting, as well as to the early post-acute setting. A continued and coordinated global effort is needed to achieve the target of the Angels Initiative of >10,000 stroke-ready hospitals by 2030, and >7500 of these in LMICs.
Keywords
Introduction
In 2021, a global survey conducted by the World Stroke Organization (WSO) 1 and World Health Organization (WHO) found that only one in three hospitals have the infrastructure and resources required to qualify as a stroke center that can deliver guideline-recommended, life-saving stroke care. 1 About 70% of stroke patients in Europe lack access to a stroke center, and globally, less than 5% of patients who are eligible for intravenous thrombolysis receive it within the therapeutic time window.2,3 In low- and middle-income countries (LMICs), patients experience more than four times the rate of stroke-related death and disability compared with those living in high-income countries, yet dedicated stroke units exist in only 18% of LMICs (vs 91% in high-income countries).4,5
A stroke-ready hospital is defined by a network of trained, multidisciplinary, coordinated healthcare staff and facilities (imaging, interventional care, etc.) that ensure timely, guideline-recommended care based on written procedures and protocols. These protocols are constantly evaluated based on time and quality indicators, and care procedures are then revised and optimized to maximize patient benefit. The evidence for improved patient outcomes resulting from organized inpatient (stroke unit) care compared with alternative services (e.g. care on a general ward) is well established. In a Cochrane meta-analysis of 29 trials including 5902 participants, patients treated in a stroke unit were more likely to be alive, independent, and living at home 1 year after their stroke. 6 Improving access to stroke units and services globally, especially in LMICs, where the stroke burden is highest, is therefore an urgent global health priority.
Since its inception in 2016, the Acute Networks Striving for Excellence in Stroke (Angels) Initiative has supported over 1700 hospitals that did not previously treat stroke patients according to evidence-based guidelines to become “stroke ready.” This initiative has positively impacted the health outcomes of an estimated 7.46 million stroke patients (based on an assumption of ~500 patients treated per hospital). 7 In LMICs, >1000 new hospitals are now stroke ready, having benefited an estimated 4.68 million people. Despite this progress, a continued and coordinated global effort is needed to achieve the target of the Angels Initiative: >10,000 stroke-ready hospitals by 2030, and >7500 of these in LMICs. 8
In this article, we describe the foundational pillars of the Angels Initiative, outline its achievements to date, and issue a call to action to the global stroke community to help the Angels Initiative achieve its ambitious goal by 2030.
Reducing the burden of stroke: the role of the Angels Initiative
What is the Angels Initiative?
The Angels Initiative is a non-profit, non-promotional, global healthcare program supported by Boehringer Ingelheim. The initiative has two aims: first, to increase the number of stroke-ready hospitals, and second, to optimize the quality of existing stroke units. 9 Specifically, the Angels Initiative targets barriers to optimal stroke care at different stages of the patient pathway, namely, pre-hospital/early identification of stroke, including awareness-raising among carers and emergency services; in-hospital management, including patient admission, triage, and treatment with thrombolysis/thrombectomy; and implementation of acute care protocols to help manage common complications of stroke, such as fever, hyperglycemia, and dysphagia (Table 1).
Barriers leading to delayed care/poor outcomes and solutions to improve stroke care and outcomes.
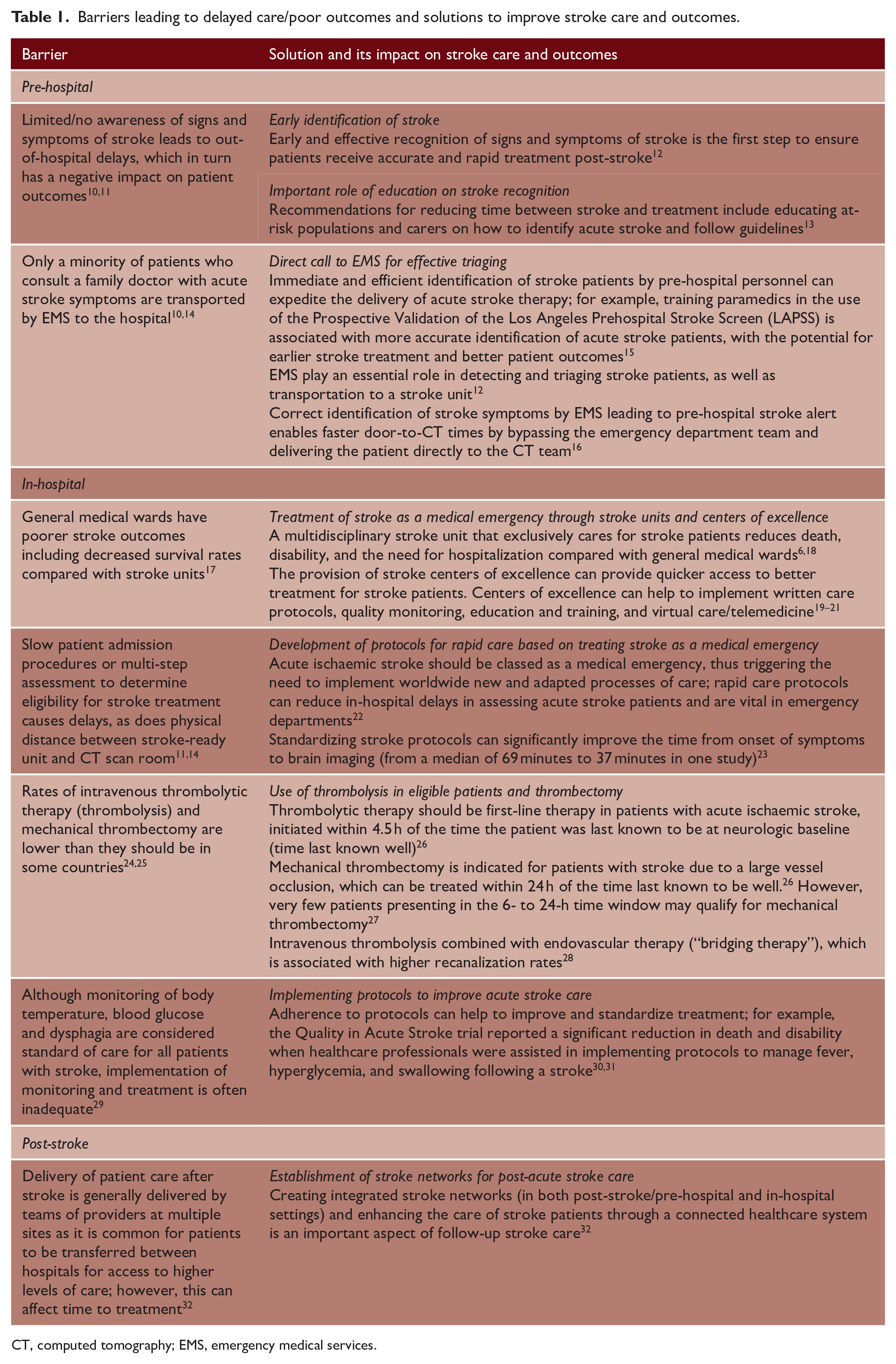
CT, computed tomography; EMS, emergency medical services.
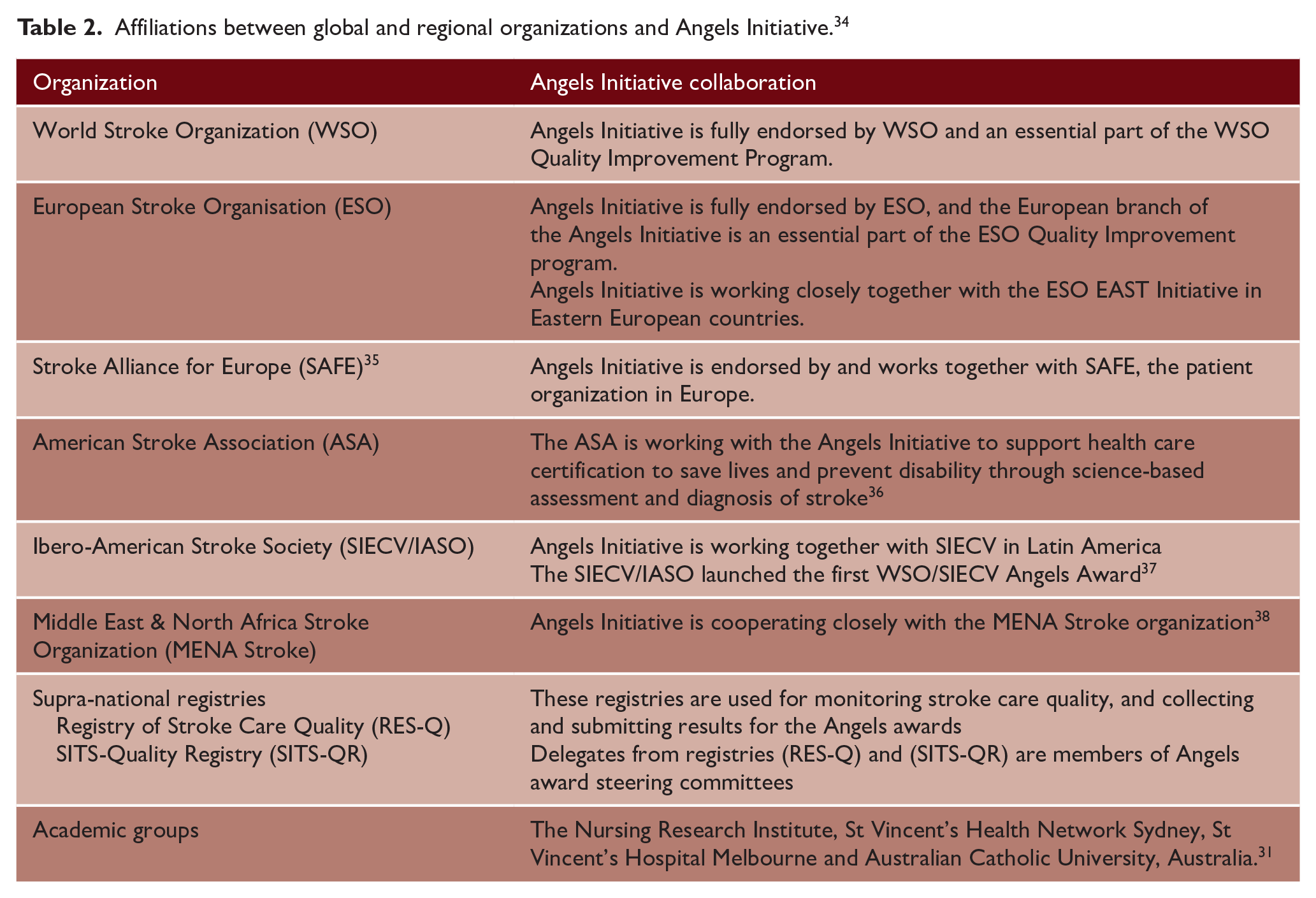
Launched in Europe in 2016, the Angels Initiative is now global in its reach and is endorsed by and run in partnership with the WSO, European Stroke Organisation (ESO), Stroke Alliance for Europe (SAFE), Ibero-American Stroke Society (SIECV), and many other organizations and healthcare professionals (HCPs) focused on improving stroke outcomes across the world (Table 2). 33 The Angels Initiative has received endorsement from national stroke societies, neurology societies, and stroke nurse organizations in more than 50 countries. The Angels Initiative has also collaborated with the World Bank and the WHO on the topics of implementing organized stroke care and raising awareness of stroke in specific regions.
Affiliations between global and regional organizations and Angels Initiative. 34
What are the pillars of the Angels Initiative?
The Angels Initiative is built upon five pillars, which form the basis of a behavioral change model. These pillars—consultancy, standardization, education, quality monitoring, and community—form the basis of all Angels activities, at national, regional, and hospital levels (Figure 1).

Five pillars of the Angels Initiative.
At its core, the Angels Initiative is a consultancy initiative, with around 140 experienced and dedicated Angels consultants providing full-time support and advice to hospitals globally.34,39 New and eligible hospitals are proactively identified by Angels consultants in collaboration with national steering committees and stroke networks, using a mapping tool that identifies gaps in geographical coverage. To qualify, a hospital must have the necessary resources to treat stroke, such as a computed tomography (CT) scanner, an emergency department, a clinical laboratory, and a dedicated area or ward for stroke patients. In any given country, Angels aims to achieve a ratio of five stroke-ready hospitals for every 1 million population, of which at least one must be a comprehensive hospital capable of delivering mechanical thrombectomy.
Once a hospital is identified, Angels consultants work closely with hospital staff to review and standardize care procedures, for example, through provision of “stroke bags” (which hospitals fill with cannulas, glucometers, syringes, test tubes, infusion pumps, cardiac monitors, thrombolytic medications, and other essentials required to provide thrombolysis for eligible stroke patients in the CT scan room), checklists, point-of-care devices, and other valuable tools and resources (Supplemental Table S1). 34 They also provide educational outreach to address knowledge gaps and build a community of informed HCPs. Education is typically delivered in an experiential way, for example, through on-site simulation training to help streamline the in-hospital workflow in the context of local needs and constraints. Angels consultants also provide support by establishing quality monitoring frameworks, which motivate hospitals, regions, and countries to establish and optimize monitoring frameworks on a long-term basis. These include encouraging clinicians to enter data into the Registry of Stroke Care Quality (RES-Q), an online audit platform developed to help registered sites and countries improve their stroke care systems, and the Safe Implementation of Treatments in Stroke-Quality Registry (SITS-QR), a short and simple stroke care quality protocol. 40 Finally, Angels consultants bring individual stroke teams together to develop a global community of excellence that works together to improve outcomes for stroke patients.
What has the Angels Initiative achieved to date?
As of September 2022, the Angels Initiative includes >100,000 HCPs from >7500 hospitals in 147 countries, and 1700 hospitals that did not previously treat stroke according to evidence-based guidelines are now stroke ready (Figure 2). 41 Within the 142 LMICs classified by the World Bank, where the need for improved stroke care infrastructure is greatest, the Angels Initiative has helped >1000 hospitals to become stroke ready, improving health outcomes for an estimated 4.68 million people between 2016 and 2021 (based on an assumption of ~500 patients treated per hospital; Figure 2). 42 Notable examples of countries where the number of stroke-ready hospitals has increased substantially thanks to the support of the Angels Initiative include Romania (13 stroke-ready hospitals in 2015 vs 46 in 2021), Algeria (zero in 2015 vs 48 in 2021), and South Africa (5 in 2015 vs 185 in 2021). Within LMICs, success stories regarding the number of new stroke-ready hospitals since 2016 include Argentina (664), India (451), Mexico (393), Brazil (328), Ecuador (271), Ukraine (263), Colombia (233), Indonesia (217), Thailand (171), Philippines (165), Peru (157), and Vietnam (139). 42 Among these countries, over 3.6 million patients have received treatment in a stroke-ready hospital. 42
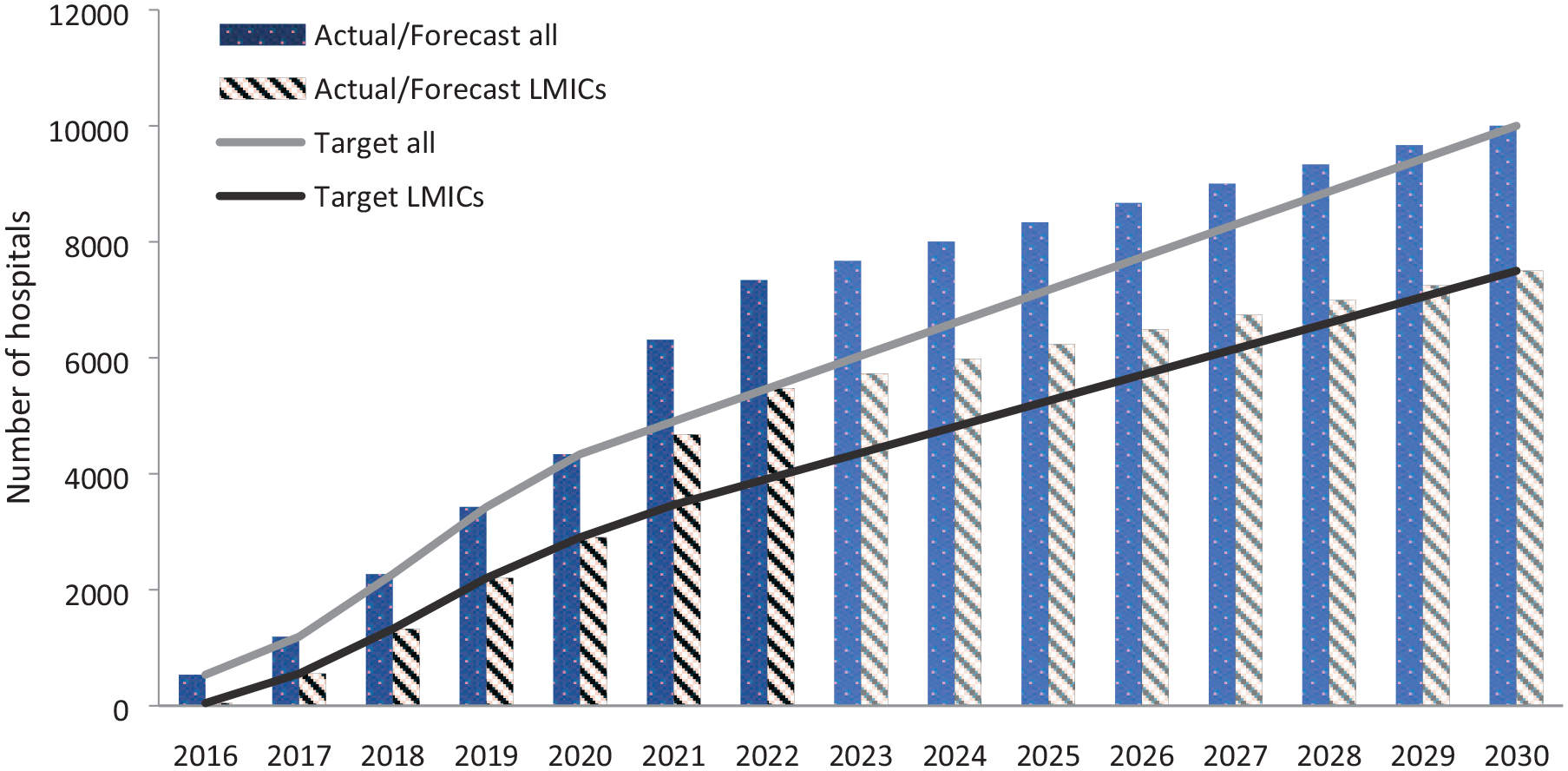
Number of hospitals involved in Angels Initiative (target vs actual), overall and by LMICs.
Regarding treatment indicators, “door to treatment time” among European hospitals registered in the Angels Initiative reduced thrombolysis administration time from 72 to 45 min between 2015 and 2020, representing a 37% relative reduction from baseline. Since registering with the Angels Initiative, the median door-to-treatment time for thrombolysis in stroke patients in Romania and Moldova has reduced by 35 min (40% reduction vs baseline) and 15 min (19% reduction vs baseline), respectively. In Egypt, door-to-treatment time decreased by 60 min between 2017 and 2021 (50% reduction vs baseline). 43 In terms of recanalization, the percentage of thrombolysis procedures carried out in Europe increased from 6.8% to 13.1% between 2015 and 2020. Similar improvements in quality monitoring have also been observed, with data for 500,000 stroke patients from more than 2000 hospitals captured within the RES-Q registry since 2016. 44 One notable example of a country where quality monitoring has increased substantially is Mexico, where 38 new centers have enrolled in RES-Q, SITS-QR, or national registries; 430 new HCPs have been trained in stroke management; 60 in-hospital stroke simulations have been carried out; and 35 hospitals have put in place checklists (protocols) since 2016. 42
The data collected by registries are used by the Angels Initiative to assess the performance of each stroke unit. RES-Q, for example, collects stroke unit performance data based on 24 variables, which are grouped into seven ESO-recommended key performance indicators (KPIs). 33 These KPIs provide the basis for the three tiers of ESO Angels awards, which are categorized as gold, platinum, and diamond (the highest accreditation) (Table 3). 33 The evaluation is carried out independently of the Angels Initiative by a steering committee, which includes delegates from participating registries (RES-Q, SITS-QR) and national coordinators, usually presidents of national stroke societies.45,46 A similar award system has been established by the Angels Initiative together with the WSO for all stroke-ready hospitals across the world, 40 thus encouraging even more hospitals to participate. The number of hospitals that have received Angels awards is steadily increasing, demonstrating the success of the initiative.40,47 In the second quarter (Q2) of 2017, 10 hospitals achieved ESO gold, platinum, or diamond status, and this increased substantially to 317 ESO Angels awards in 2021 Q2, 99 of which were diamond awards. As of Q2 2022, a total of 2707 awards had been granted, of which 729 were diamond awards. 42
ESO ANGELS Award: Criteria to achieve the levels “Gold Status,” “Platinum Status,” and “Diamond Status.”
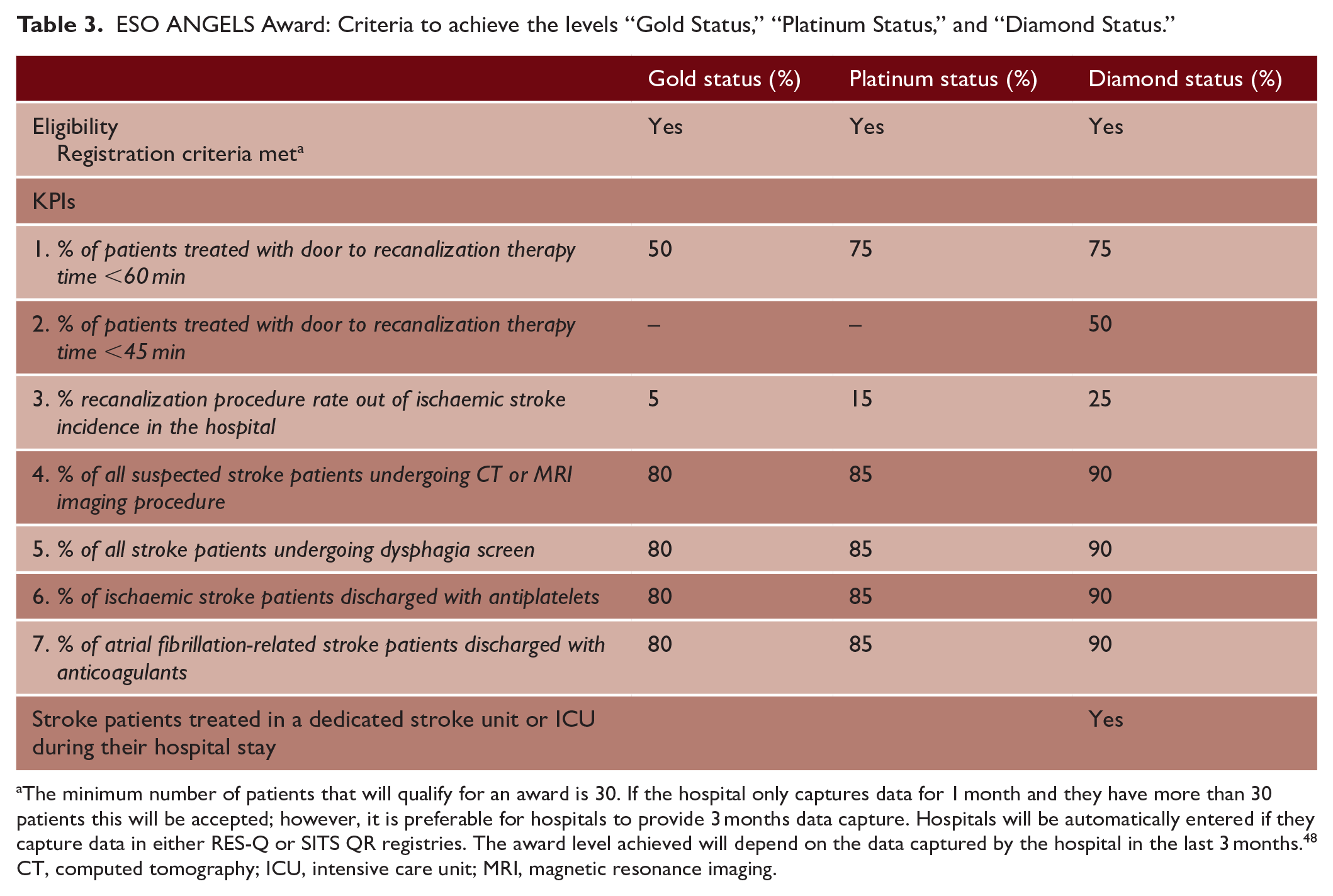
The minimum number of patients that will qualify for an award is 30. If the hospital only captures data for 1 month and they have more than 30 patients this will be accepted; however, it is preferable for hospitals to provide 3 months data capture. Hospitals will be automatically entered if they capture data in either RES-Q or SITS QR registries. The award level achieved will depend on the data captured by the hospital in the last 3 months. 48
CT, computed tomography; ICU, intensive care unit; MRI, magnetic resonance imaging.
In recognition of these achievements, the Angels Initiative was awarded the WSO Award for Stroke Services at the World Stroke Congress 2021. 41 The initiative has also been featured as a best practice example in the Access to Medicine Report 2021, funded by the Bill & Melinda Gates Foundation.
Strengths, weaknesses, and future directions
The key strength of the Angels Initiative is its non-commercial nature and international reach. As a public–private partnership, Angels works in collaboration with the WSO and ESO, regional and national stroke societies, governments, non-governmental organizations, and local hospital networks to leverage the most relevant expertise from each partner and maximize its impact. In this sense, Angels represents a bridge between science and implementation, designing and delivering practical solutions tailored to local needs.
Although substantial progress has been made, the number of stroke-ready hospitals is still low in many parts of the world (Figure 3). By 2030, the overall goal of the Angels Initiative is to achieve >10,000 stroke-ready hospitals, with >7500 in LMICs, by 2030. 41 To achieve this goal, several key challenges need to be overcome in order to streamline processes of patient care and management with the ultimate aim of improving stroke care globally. One of the key challenges is sustainable funding. As part of Boehringer Ingelheim’s 2030 Sustainable Development Goals, continued funding for the Angels Initiative is projected to provide >40 million patients with access to life-saving stroke medicines over the next 7 years. However, co-funding and the provision of resources and expertise from new partners are needed to ensure the continued success of the program. Quality monitoring represents another challenge in terms of measuring progress against the 2030 goals. As only 30% of Angels-supported hospitals currently have a formalized quality monitoring system, recruitment of more hospitals into quality monitoring initiatives such as RES-Q is critical to increasing and maintaining high standards of stroke care.
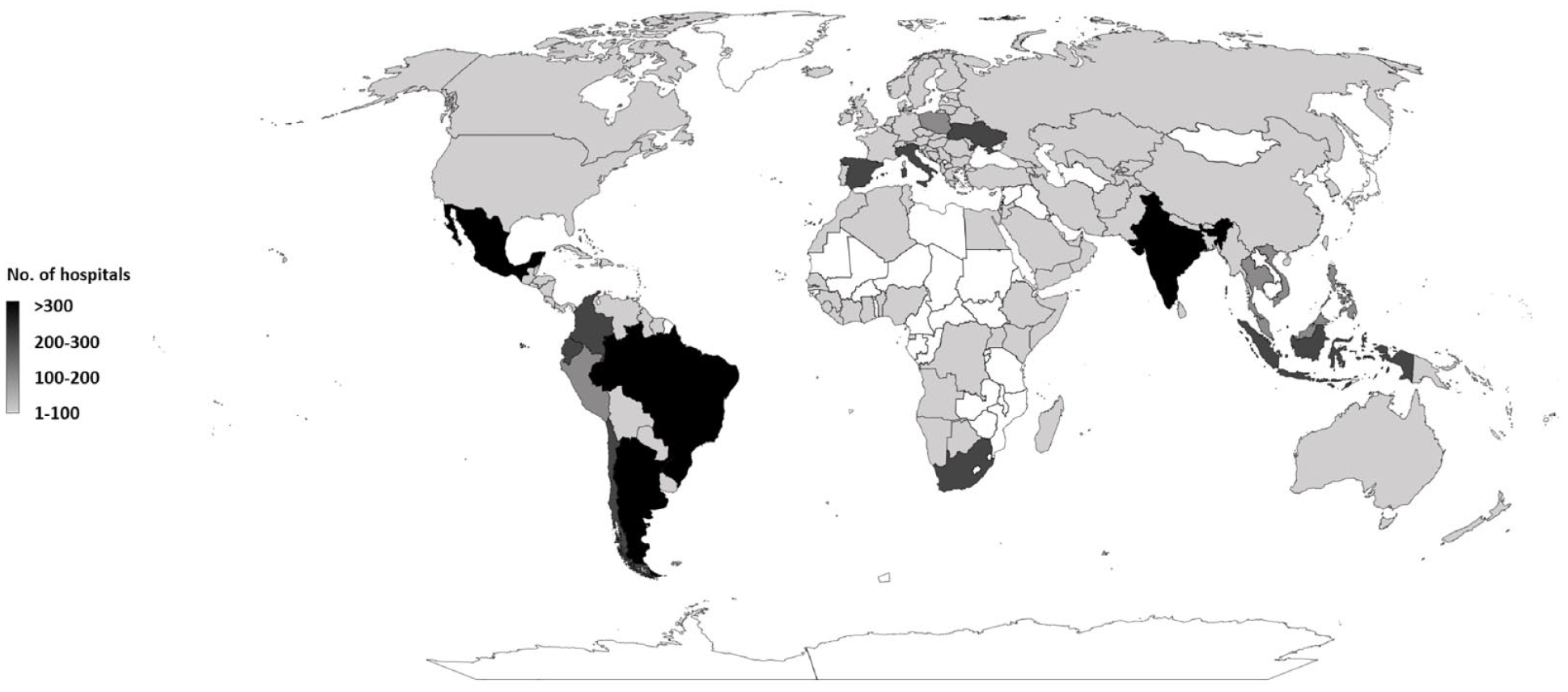
Global map showing number stroke-ready hospitals involved in Angels Initiative.
On a practical level, the focus of the work of Angels has now expanded from the hyperacute phase of stroke treatment to the pre-hospital setting as well as to the early post-acute setting. One example is the Advanced Stroke Life Support course, an intensive e-learning program designed to improve stroke knowledge among emergency medical services (EMS) and thus pre-hospital care. 49 The training focuses on four action priorities: (1) diagnosing the patient, (2) choosing the correct hospital, (3) emergency transport, and (4) pre-notification to the in-hospital stroke team. Using these four criteria as KPIs, the EMS Angels Awards were created to reward the performance of pre-hospital stroke care providers. 50 Another awareness-raising initiative, FAST Heroes, play a key role in educating families, via a school-based program, to recognize key stroke symptoms and to increase their understanding of how to respond in an emergency. 51 Schools from more than 20 countries around the world are involved in this initiative. With the use of online games and e-books that are presented by their classroom teachers over a period of 5 weeks, FAST Heroes provide children with practical life-saving skills and tools to educate their parents and grandparents on the symptoms of stroke. 52
A continued area of focus is acute care for patients post-stroke. The Quality in Acute Stroke Care trial demonstrated that with facilitated introduction of nurse-initiated protocols to manage fever, hyperglycemia, and swallowing (FeSS), there was a significant reduction in death and disability following stroke.53–55 An international collaboration between researchers, the ESO, and the Angels Initiative resulted in successful implementation of the FeSS protocols within 64 hospitals in 17 European countries, including low-middle and upper-middle-income countries. The proportion of patients treated according to the FeSS protocols increased significantly by 33% (adjusted difference in proportion), 56 which is expected to have had an impact on reducing death and disability after stroke. Further investment will be required along every step of the patient pathway to optimize outcomes.
Supplemental Material
sj-docx-1-wso-10.1177_17474930231180067 – Supplemental material for Six years of the Angels Initiative: Aims, achievements, and future directions to improve stroke care worldwide
Supplemental material, sj-docx-1-wso-10.1177_17474930231180067 for Six years of the Angels Initiative: Aims, achievements, and future directions to improve stroke care worldwide by Valeria Caso, Sheila Martins, Robert Mikulik, Sandy Middleton, Stanislav Groppa, Jeyaraj Durai Pandian, Nguyen Huy Thang, Thierry Danays, Jan van der Merwe, Thomas Fischer and Werner Hacke in International Journal of Stroke
Footnotes
Acknowledgements
Author contributions
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE) All authors approved the final version for submission.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors did not receive payment related to the development of the manuscript. VC reports fees for speaking for Boehringer Ingelheim, Pfizer BMS, Bayer, Daiichi Sankyo, and Mindmaze, and for participating in advisory boards for Boehringer Ingelheim, Pfizer BMS, and Bayer. R.M. is supported by the Implementation Research Network in Stroke Care Quality of the European Cooperation in Science and Technology (project CA18118) and by the IRIS-TEPUS project from the inter-excellence inter-cost program of the Ministry of Education, Youth and Sports of the Czech Republic (project LTC20051). S.M. received funding from the European Stroke Organisation and worked with the Angels Initiative on the QASC Europe study. J.v.d.M. is an employee of Boehringer Ingelheim. T.F. was an employee of Boehringer Ingelheim during development of this article. T.D. is the owner of TDC (Aix en Provence, France), a company that received consulting fees from Boehringer Ingelheim during development of the article. W.H. is a member of the Angels steering committee. S.G., J.D.P., N.H.T., and S.M. have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medical writing support was funded by Boehringer Ingelheim. Boehringer Ingelheim was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.