
Abstract
Background:
The incidence of stroke in developed countries is increasing selectively in young individuals, but whether this is secondary to traditional vascular risk factors is unknown.
Methods:
We used the Canadian Community Health Survey from 2000 to 2016 to create a large population-representative cohort of individuals over the age of 30 and free from prior stroke. All analyses were stratified by age decile. We linked with administrative databases to determine emergency department visits or hospitalizations for acute stroke until December 2017. We calculated time trends in risk factor prevalence (hypertension, diabetes, obesity, and smoking) using meta-regression. We used Cox proportional hazard models to evaluate the association between vascular risk factors and stroke risk, adjusted for demographic, co-morbid, and social variables. We used competing risk regression to account for deaths and calculated population-attributable fractions. In a sensitivity analysis, we excluded those with prior heart disease or cancer.
Results:
We included 492,400 people in the analysis with 8865 stroke events over a median follow-up time of 8.3 years. Prevalence of hypertension, diabetes, and obesity increased over time while smoking decreased. Associations of diabetes, hypertension, and obesity with stroke risk were progressively stronger at younger age (adjusted hazard ratio for diabetes was 4.47, 95% confidence interval (CI) = 1.95–10.28 at age 30–39, vs 1.21, 95% CI = 0.93–1.57 at age 80+), although the obesity association was attenuated with adjustment. Smoking was associated with higher risk of stroke without a gradient across age deciles, although had the greatest population-attributable fraction at younger age. The hazard ratio for stroke with multiple concurrent risk factors was much higher at younger age (adjusted hazard ratio for 3–4 risk factors was 8.60, 95% CI = 2.97–24.9 at age 30–39 vs 1.61, 95% CI = 0.88–2.97 at age 80+) and results were consistent when accounting for the competing risk of death and excluding those with prior heart disease or cancer.
Conclusions:
Diabetes and hypertension were associated with progressively elevated relative risk of stroke in younger individuals and prevalence was increasing over time. The association of obesity with stroke was not significant after adjustment for other factors. Smoking had the greatest prevalence and population-attributable fraction for stroke at younger age. Our findings assist in understanding the relationship between vascular risk factors and stroke across the life span and planning public health measures to lower stroke incidence in the young.
Introduction
The overall incidence of stroke is decreasing over time in developed countries.1,2 However, many studies have observed a paradoxical increase in stroke incidence among young individuals, primarily those <60 years of age.3–9 A high proportion of young people with stroke have traditional vascular risk factors, which has raised public health concerns about the potential role of these risk factors in driving stroke incidence in the population.8,10–13
Understanding whether the association between vascular risk factors and stroke differs at young age would be important in planning and promoting public health strategies and potentially mitigating the rise in stroke incidence. However, there is a lack of comprehensive, population-representative data on this question. Specifically, studies have not adequately evaluated the risk of stroke attributed to vascular risk factors at different ages in a large population and have not simultaneously assessed prevalence trends of these risk factors.
We sought to determine whether prevalence trends and risk of stroke with traditional risk factors of hypertension, diabetes, obesity, and smoking differed across the life span in a large, population-representative sample.
Methods
Canadian Community Health Survey
The Canadian Community Health Survey (CCHS) is an annual population-representative cross-sectional survey, representing 97% of the Canadian household population aged 12 years and older. 14 The survey randomly samples households nationwide and selects one respondent per household. The CCHS collects information about health status, health determinants, and health care utilization of the household population (Supplemental Methods).
Administrative linkages
Approximately 85% of total respondents agreed to have their responses linked to administrative records. Statistics Canada created sample weights to retain population representativeness. Linkages were performed by Statistics Canada and included the Canadian Institutes of Health Discharge Abstract Database (CIHI-DAD) for hospitalizations, the National Ambulatory Care Reporting System (NACRS) for emergency department (ED) visits, and the Canadian Vital Statistics Database (CVSD) for deaths.15,16 We linked the CCHS survey to CIHI-DAD, NACRS, and CVSD to determine stroke events and deaths after the survey response until 31 December 2017. All participants had a minimum of 1 year and a maximum of 18 years of full follow-up for events and were censored if alive on 31 December 2017.
Cohort
We used all available CCHS cycles from 2000 to 2016 (2000, 2003, 2005, 2007–2016) to capture data on vascular risk factors and other baseline covariates. We included all respondents aged 30 and above who did not have a prior stroke event from 1999 until the date of survey. Those younger than 30 were excluded due to very low risk of stroke. Each year’s cohort was then followed over time using linked healthcare administrative data to determine new strokes or deaths (Supplemental Figure 1).
Exposure
Our four exposures were presence of self-reported hypertension, diabetes, obesity, and current smoking. The wording of questions for hypertension and diabetes is modeled after items contained in the US Behavioral Risk Factor Surveillance System and specifies that chronic conditions must represent a diagnosis from a health professional. Obesity was defined as body mass index (BMI) ⩾ 30 kg/m2, calculated from self-reported height and weight. Due to known biases in self-report of BMI, we employed a correction developed for the CCHS. 17 CCHS year 2000 did not contain BMI data for ages 70 and over so was excluded for analyses in those age groups. Current smoking was defined as smoking occasionally or daily, with never smokers or formers smokers as the reference. Smoking categories are determined by asking participants whether, at the present time, they smoke cigarettes daily, occasionally, or not at all and whether they have ever smoked cigarettes daily.
Covariates
Covariates were obtained from the CCHS, including age, sex, rural residence, and self-report of ethnicity, education level, total household income, marital status, heart disease, cancer, fruit and vegetable consumption, and alcohol consumption (Supplemental Table 1). Age was categorized into deciles as 30–39, 40–49, 50–59, 60–69, 70–79, and 80+. Leisure-time physical activity was obtained from years 2000 to 2014 and was measured as energy expenditure (metabolic equivalents) per week using the Minnesota Leisure Time Physical Activity Questionnaire. 18 Physical activity data from 2015 to 2016 could not be included due to a change in the measurement strategy.
Outcome
Our primary outcome was acute stroke (ischemic stroke or intracerebral hemorrhage (ICH)) at any time in follow-up until censoring on the record linkage date of 31 December 2017. These events were identified using International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA) codes (ischemic stroke: I63.x, I64.x, H34.1; intracerebral hemorrhage: I61.x) and ICD-9 codes (ischemic stroke: 434.01, 434.11, 434.91, 436; intracerebral hemorrhage: 431). We also determined risk of death during follow-up.
Statistical analysis
We calculated the proportion of each baseline characteristic in our study cohort, weighted to the Canadian population. We undertook three main analyses to determine the relevance of vascular risk factors to stroke risk. First, we determine trends in prevalence of risk factors over time (Supplemental Methods). Second, we used Cox proportional hazard models to determine the association between each vascular risk factor and incident stroke in follow-up. As there was modification by age group and not sex, all models were stratified by age decile. In our simple model, we included the exposure of interest (diabetes, hypertension, obesity, or smoking) and adjustment for sex only. The full model included the exposure of interest and adjustment for sex, the remaining three risk factors, and potential confounders of education, rural residence, income quartile, ethnicity, marital status, fruit and vegetable consumption, and alcohol consumption. We did not include heart disease and cancer in the models as they may be on the causal pathway between vascular risk factors or smoking and stroke. We also determined the association between total number of concurrent risk factors (categorized as 0, 1, 2, and 3–4) and hazard of stroke, adjusting for the remainder of the variables in the full model. We evaluated the proportional hazards assumption by assessing the significance (p < 0.05) of an interaction term between the risk factor and follow-up time. We conducted sensitivity analyses (1) stratifying by stroke type (ischemic stroke and ICH), (2) excluding people with prior heart disease and cancer, and (3) including physical activity as a covariate in the models. To account for the competing risk of death, we also conducted competing risk regression using the Fine and Gray subdistribution hazard model19–21 and determined cumulative incidence of stroke by age group, adjusting for the same variables in the full model. Third, we used population-attributable fractions (PAFs) to determine the population-level importance of each risk factor to stroke risk in each age group (Supplemental Methods).
Analyses were done in the Prairie Regional Research Data Centre at the University of Calgary using Stata 16.0 (College Station, TX, USA). All analyses used sample weights provided by Statistics Canada. Threshold of significance for p-values was <0.05. Under Tri-Council guidelines, this analysis did not require approval by a research ethics board. Our study adhered to STROBE guidelines (checklist in Supplemental Table 2). The data set from this study is held securely in coded form at Statistics Canada Prairie Regional Research Data Centre. Access to data may only be granted after approval by Statistics Canada.
Results
We included a total of 492,400 people in our analysis (see Supplemental Figure 1 for flow diagram). The median follow-up time was 8.3 (interquartile range (IQR) = 4.5–12.6) years. There was a total of 8865 stroke events in follow-up and 89% were ischemic stroke. Events were primarily from stroke admissions (90.5%) and the remainder were ED visits without admission. The median time from survey response until stroke was 5.3 (IQR = 2.7–9.1) years. A total of 66,385 people died in follow-up.
Baseline characteristics weighted to the Canadian population are shown in Supplemental Table 1. The largest proportion of people was at age 40–49 (24.9%) and the lowest was at age 80+ (4.5%), and 51% of the cohort was female. Hypertension was present in 21.3%, diabetes in 7.5%, obesity in 27.0%, and smoking in 20.2%. Hypertension and diabetes were more prevalent at older age, smoking was less prevalent at older age, and obesity was most prevalent in middle age (Supplemental Figure 2). Meta-regression showed a significant increase in diabetes prevalence for all age groups but the greatest relative increase in those aged 80+ and 40–49, with a similar pattern for hypertension (Figure 1). The two youngest age groups had the greatest absolute and relative increase in obesity prevalence and concurrent decrease in smoking prevalence. All meta-regression lines are shown in Supplemental Figures 3 to 6.
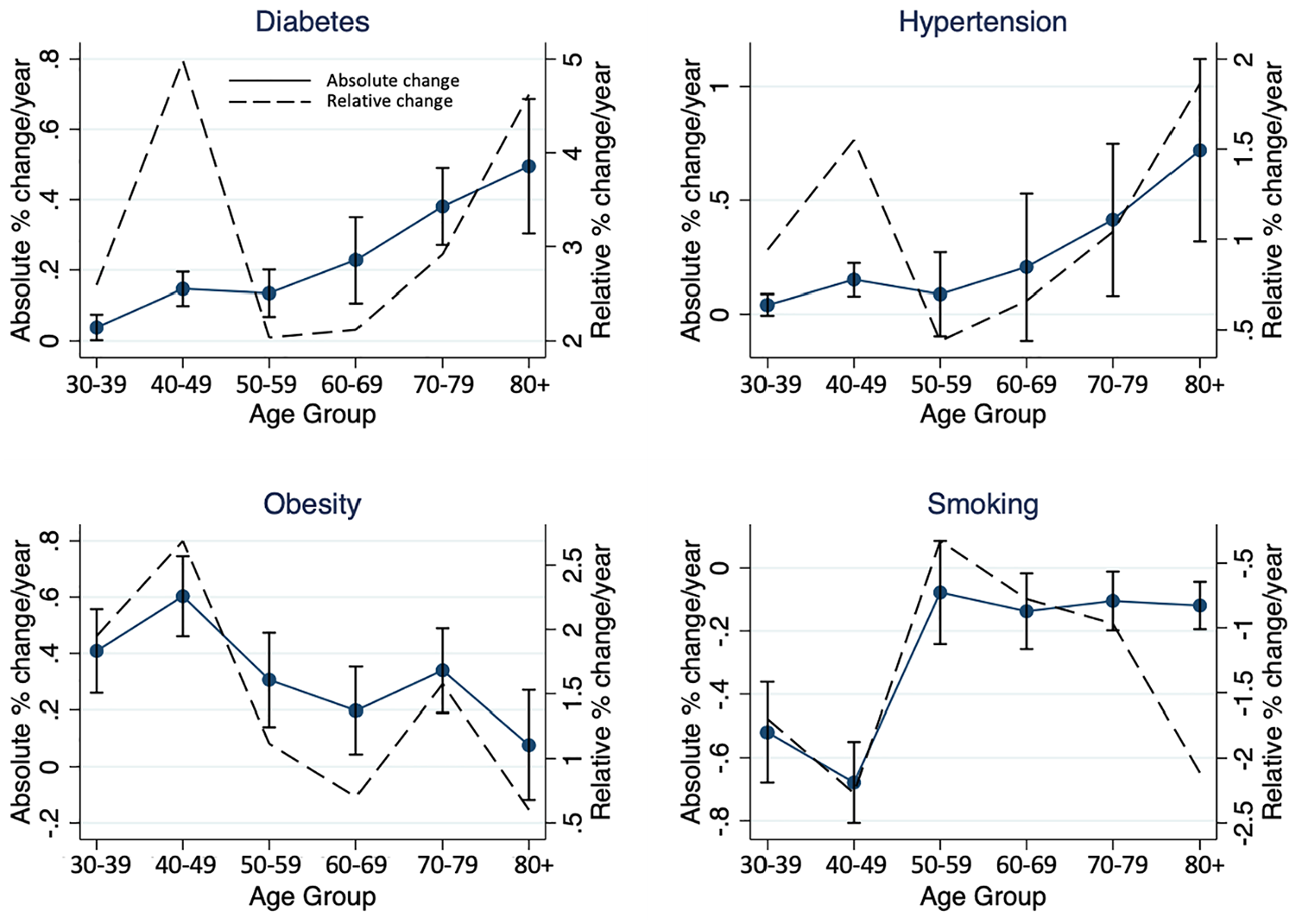
Annual change in population-weighted prevalence of diabetes, hypertension, obesity, and smoking from 2000 to 2016, stratified by age. Results display absolute (solid line with 95% confidence intervals) and relative changes (dashed line) per year, derived from coefficient of meta-regression line. Older individuals have greater absolute increases in hypertension and diabetes prevalence but individuals <50 years have prominent relative increases. Those <50 years have the greatest increase in obesity and decrease in smoking prevalence.
There was no evidence of violation of the proportional hazards assumption. In both simple and full Cox models, there was significant modification of the association with stroke by age group for diabetes (p-interaction < 0.001), hypertension (p-interaction < 0.001), obesity (p-interaction = 0.009 for simple model, 0.02 for full model), but not smoking (p-interaction = 0.49 for simple model, 0.57 for full model). In the age-stratified simple models, there was a progressively greater diabetes-stroke hazard ratio from older to younger age groups (adjusted hazard ratio (aHR) = 7.46, 95% confidence interval (CI) = 3.93–14.15 for age 30–39 compared with 1.18, 95% CI = 0.98–1.42 for age 80+). The pattern was similar for diabetes in the full model (aHR = 4.47, 95% CI = 1.95–10.3 for age 30–39 compared with 1.21, 95% CI = 0.93–1.57 for age 80+) and for hypertension in both models (Figure 2(a) and (b)).
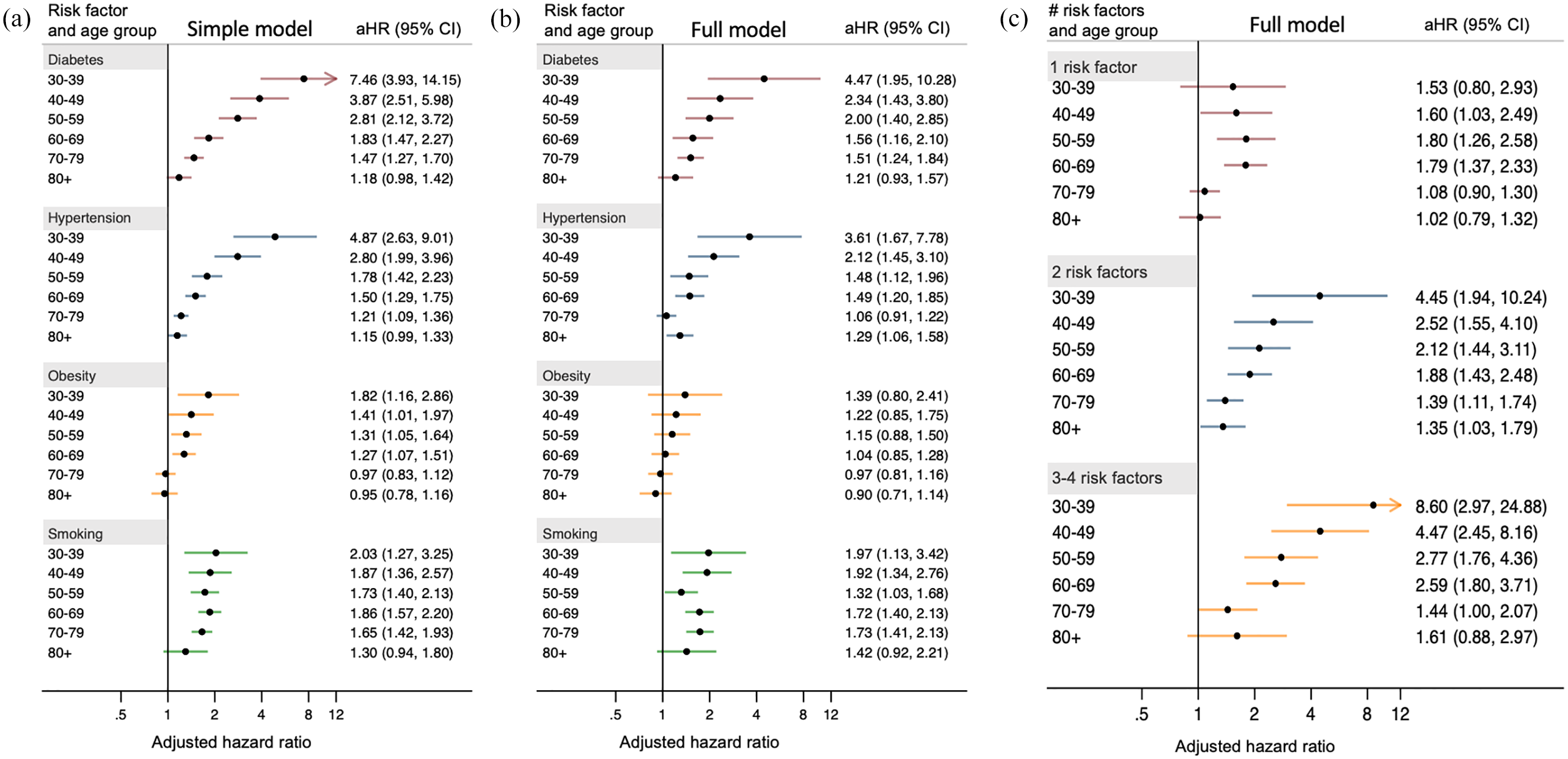
Adjusted hazard ratios for stroke stratified by presence of vascular risk factor and age, for individual risk factors with (a) simple and (b) full models, and (c) for number of concurrent risk factors. Hazard ratios are higher at younger age for diabetes and hypertension. Age-dependent association of obesity with stroke risk is attenuated after full adjustment. Hazard ratios for multiple concurrent vascular risk factors increase with younger age (reference category is 0 risk factors). Simple model adjusted for sex only. Full model adjusted for sex, remaining three risk factors, education, rural residence, income quartile, ethnicity, marital status, fruit and vegetable consumption, and alcohol consumption.
Obesity was also associated with greater hazard of stroke at younger age in the simple model, with a significantly elevated risk only for those <70 years of age (aHR = 1.82, 95% CI = 1.16–2.86 for age 30–39 years compared with 0.95, 95% CI = 0.78–1.16 for age 80+). However, the association between obesity and stroke risk was no longer significant in any age group after adjustment for hypertension, diabetes, and other factors (Figure 2(a) and (b)). Smoking was associated with increased risk of stroke but had no clear gradient across age groups. Sensitivity analyses were similar when evaluating ischemic stroke alone, when excluding people with prior heart disease and cancer, and when including physical activity in the models. However, associations were not significant in the sensitivity analysis with ICH alone (Supplemental Figure 7).
For total number of concurrent risk factors, there was a similar gradient with increased hazard ratio of stroke at younger age when 2 or 3–4 risk factors were present (Figure 2(c)).
Results were also consistent when accounting for the competing risk of death (Supplemental Figure 8). There was a greater relative increase in cumulative incidence of stroke among those with diabetes compared with no diabetes at younger age (Figure 3). The pattern was similar for hypertension (Supplemental Figure 9) and for multiple concurrent risk factors (Figure 4).
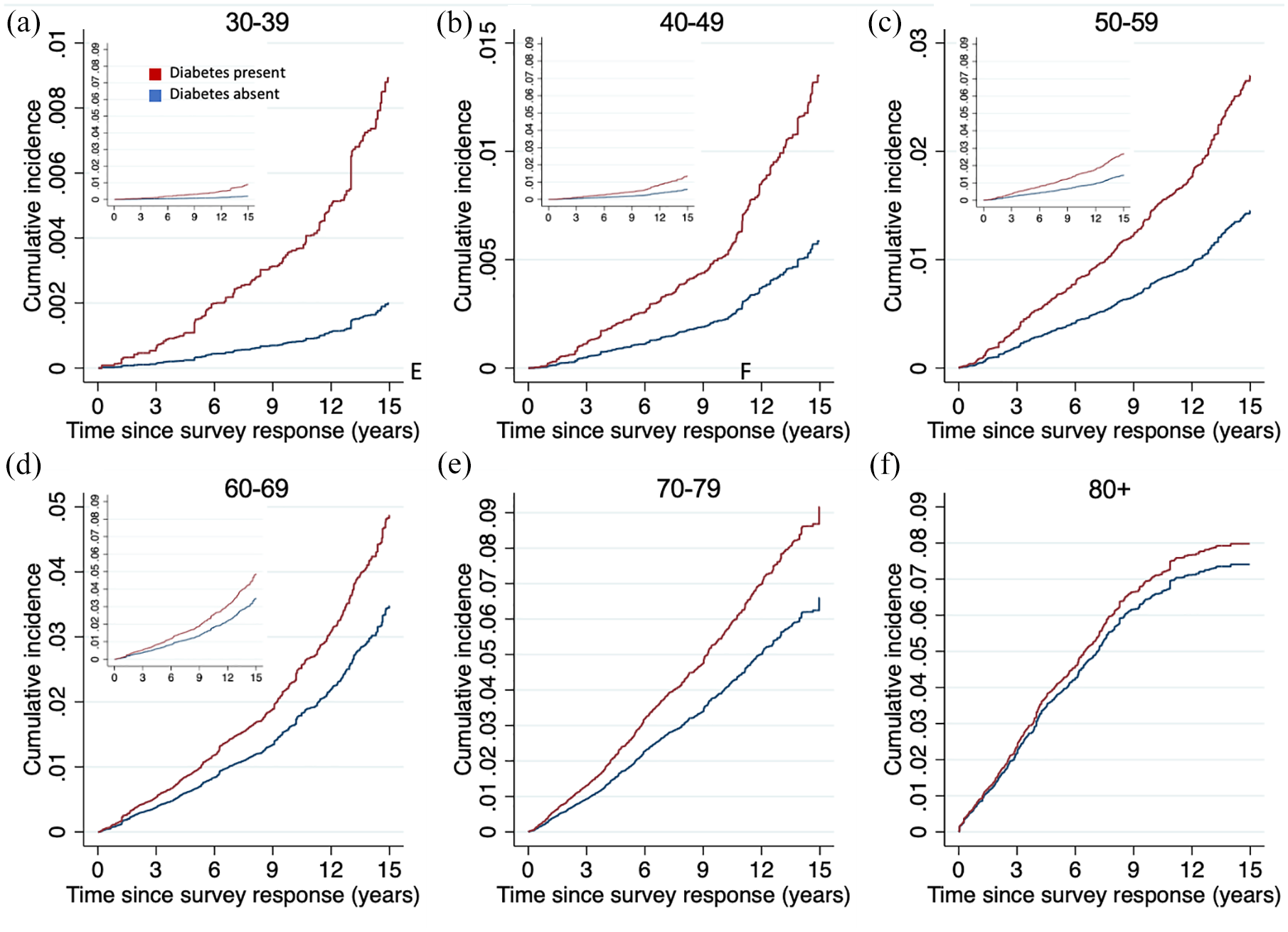
Cumulative incidence of stroke over 15 years, stratified by presence of diabetes and age group. Those at younger age have greater relative increase in cumulative risk with diabetes compared with no diabetes. Cumulative incidence functions are generated from Fine and Gray competing risk models. Models adjusted for sex, remaining three risk factors, education, rural residence, income quartile, ethnicity, marital status, fruit and vegetable consumption, and alcohol consumption. Y-axes show incidence proportion, and for main panels are scaled to range of data to emphasize relative differences at younger age, while insets all have same y-axis range as E and F to compare absolute risks.
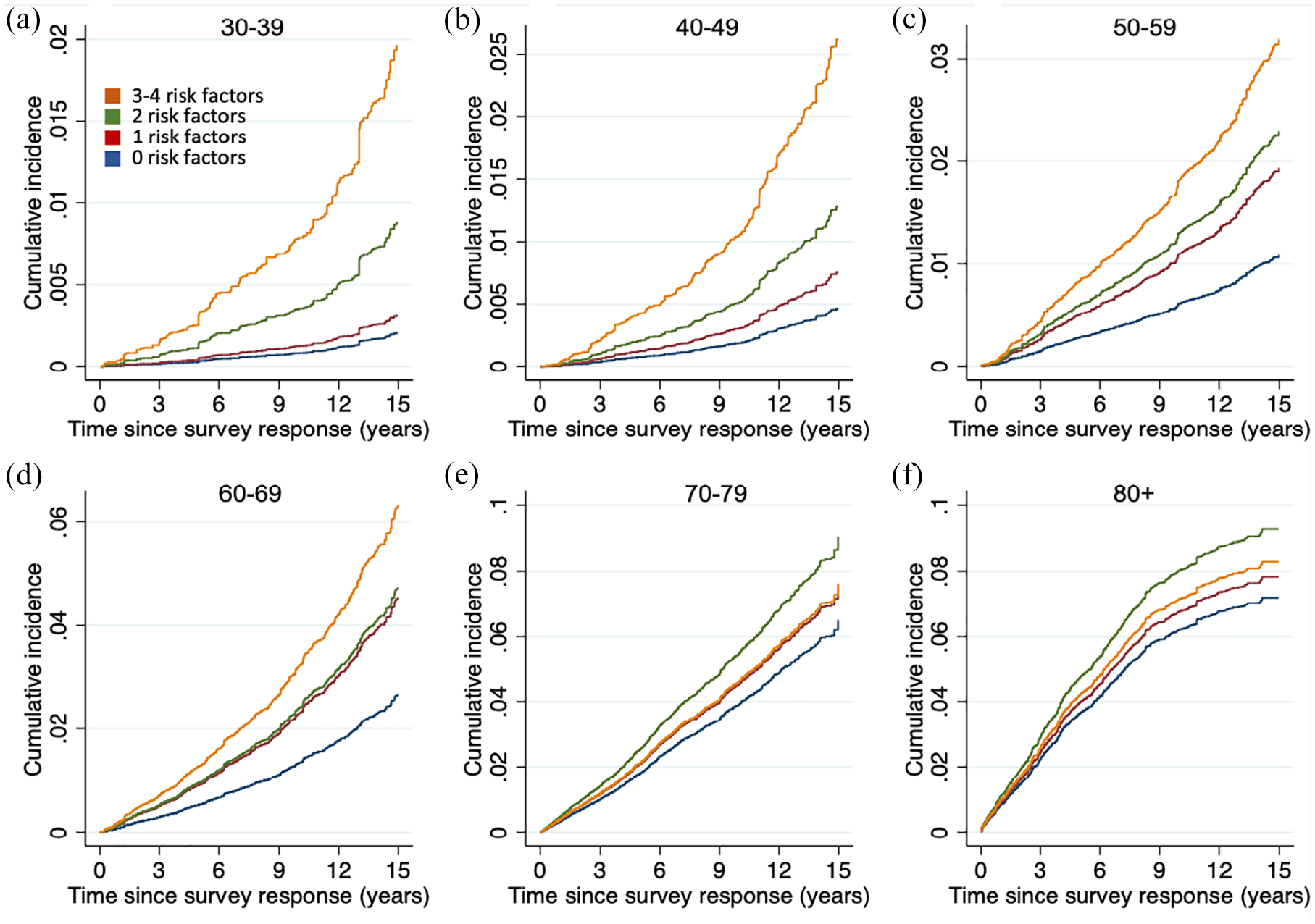
Cumulative incidence of stroke stratified by number of risk factors and age. Those at younger age have greater relative increase in cumulative risk with multiple risk factors compared with no risk factors. Cumulative incidence functions are generated from Fine and Gray competing risk models. Models adjusted for sex, education, rural residence, income quartile, ethnicity, marital status, fruit and vegetable consumption, and alcohol consumption.
Adjusted PAFs can be seen in Figure 5. The largest PAFs in younger individuals were for smoking (20–21% for age <50), followed by hypertension (12–13%) and then diabetes (6–7%). Obesity was not associated with a significantly elevated adjusted PAF for any age group.
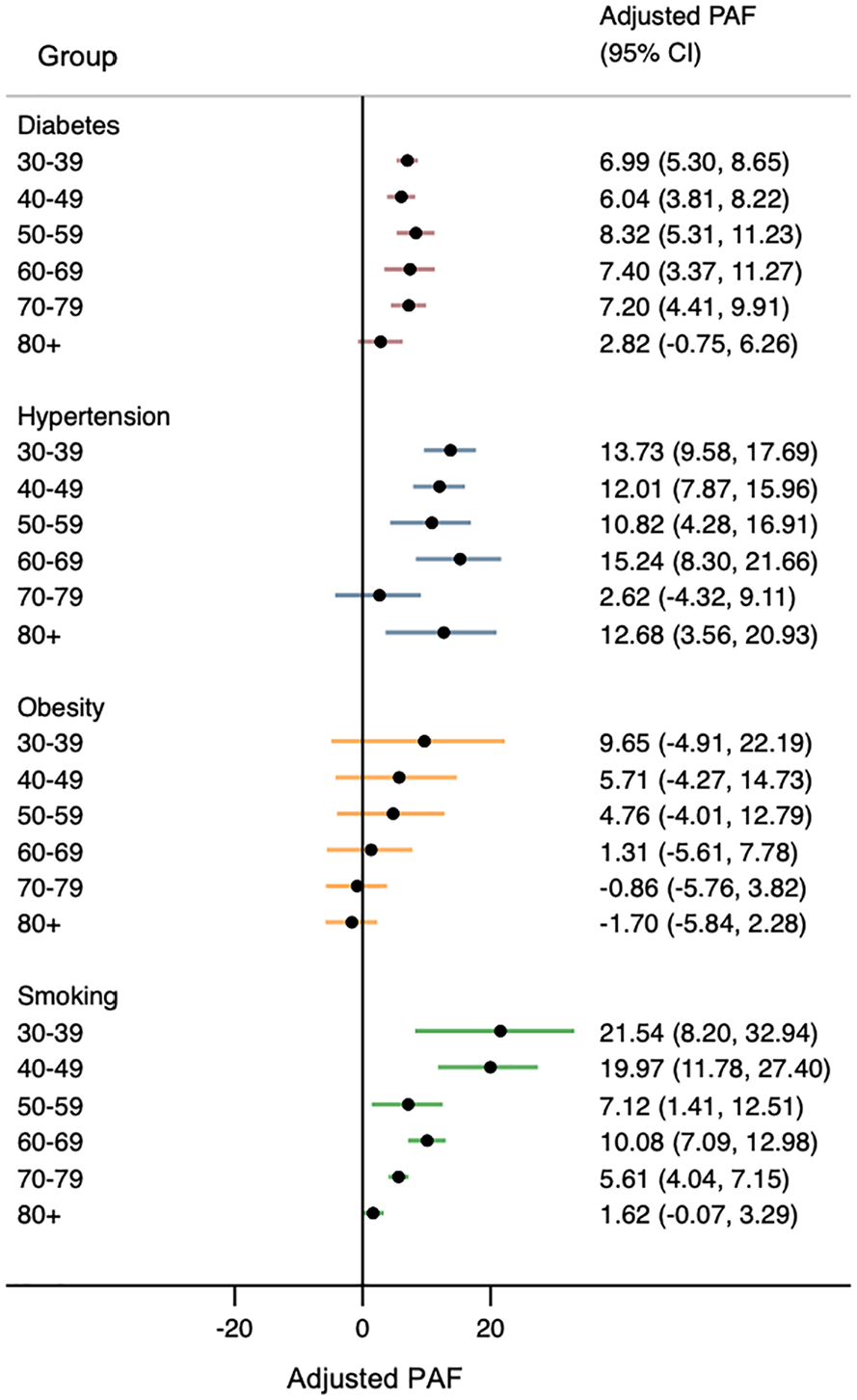
Adjusted population-attributable fraction for each risk factor, stratified by age. Smoking at younger age had the greatest adjusted PAF.
Discussion
In our population-representative cohort of approximately half a million respondents, we found that hypertension, diabetes, and the combination of risk factors were associated with higher risk of long-term stroke with escalating strength of association at younger age, even when accounting for the competing risk of death. In addition, prevalence estimates of diabetes, hypertension, and obesity were rising over time, particularly for younger individuals. Our findings provide novel insights into stroke risk factors across the life span on a population level and reveal potential underlying mechanisms for rising stroke incidence in young people.
The presence of diabetes or hypertension was associated with the greatest elevation of stroke risk in the young. Obesity was selectively associated with stroke risk in the young in unadjusted analyses, but this association was eliminated after adjustment for hypertension, diabetes, smoking, and other social and lifestyle variables, consistent with prior studies and suggesting the impact of obesity may be mediated through downstream cardiovascular risk factors. 22 In contrast, smoking was associated similarly with risk of stroke regardless of age. The reason for the age modification of hypertension, diabetes, and obesity in the risk of stroke is unclear. Prior studies have shown the associations between vascular risk factors and mortality and cardiovascular outcomes are greater at younger age.22–28 Our study extends these prior findings of age modification to vascular risk and stroke. It is possible that physiological reasons underlie these differences. For example, it has been postulated that the decreasing health impact of obesity at older age is due to the protective properties of nutritional or caloric reserves in frailer populations.29,30 Older people may also have developed greater resistance to the impact of chronic co-morbidities such as hypertension or diabetes. Additional explanations may include selective survival or competing causes of death and poor outcome which obscures the observable impact of select co-morbidities at older age.29,31
We found rising trends in prevalence of diabetes, hypertension, and obesity, consistent with prior studies,32,33 with a greater relative increase among younger individuals. Conversely, there was a decrease in smoking prevalence predominantly in the elderly and the young, consistent with prior findings in Canada and likely reflecting effective public health campaigns.34,35 Our results suggest that rising trends in risk factors combined with greater hazard of stroke in the young may partly underlie the observed increase in stroke incidence among young individuals in multiple jurisdictions.3–6,8,9 Our findings therefore encourage efforts to understand and mitigate the determinants and effects of diabetes, hypertension, and obesity in the young in order to blunt rising incidence of stroke and potentially other cardiovascular conditions. In addition, due to its high prevalence smoking had the highest adjusted PAF in those <50 years of approximately 20%%, compared with hypertension at 12–13% and diabetes at 6–7%, and should continue to be a focus of public health campaigns despite its decreasing prevalence.
Our analysis has numerous strengths, particularly with the quality and reliability of the data, the availability of a large number of baseline variables, and the large and population-representative sample and extensive follow-up. Nevertheless, there were some limitations to this study. First, exposure to vascular risk factors was reliant on self-report. However, self-report of hypertension and diabetes has shown substantial agreement with measured data and medical records.36-37 Furthermore, it is likely that any potential misclassification in self-reported risk factors was non-differential across age, which would bias estimates toward the null. Studies of self-report by age are inconsistent, with older individuals reported to be either more likely or less likely to acknowledge risk factors at interview.36, 38, 39 Although we used a correction of self-reported BMI, misreporting may still result in biased measures of association.40, 41 Self-report of smoking is valid in the Canadian population when compared with urine cotinine concentration. 42 However, due to the potential for underreporting of smoking, 43 we combined categories of occasional and daily cigarette smoking. Second, we used administrative linkages to determine stroke events, although the codes used have high validity in Canada, with a positive predictive value for ischemic stroke hospitalizations of 97.3% and for ICH of 91.9%. 44 Third, we could not capture incident vascular risk factors in follow-up after the initial survey. Fourth, we did not have information on hyperlipidemia or peripheral artery disease. Finally, despite adjustment for a variety of potential confounders, there remains the possibility of residual measured and unmeasured confounding.
In summary, in a large, population-representative sample, we demonstrate a progressive increase in hazard ratios for stroke at younger age with exposure to diabetes, hypertension, and obesity, and the prevalence of these risk factors is rising over time. The risk of stroke was drastically increased in younger individuals with multiple concurrent risk factors. These findings are important for planning primary and secondary prevention measures for vascular risk factors and understanding potential reasons for observed trends in stroke incidence in the young.
Supplemental Material
sj-pdf-1-wso-10.1177_17474930211070682 – Supplemental material for Vascular risk factors and stroke risk across the life span: A population-representative study of half a million people
Supplemental material, sj-pdf-1-wso-10.1177_17474930211070682 for Vascular risk factors and stroke risk across the life span: A population-representative study of half a million people by Raed A Joundi, Scott B Patten, Jeanne VA Williams and Eric E Smith in International Journal of Stroke
Footnotes
Acknowledgements
The analysis was conducted at the Prairie Regional Research Data Centre (RDC), which is part of the Canadian Research Data Centre Network. The services and activities provided by the Canadian Research Data Centre Network are made possible by the financial or in-kind support of the Social Sciences and Humanities Research Council, the Canadian Institutes of Health Research, the Canadian Foundation for Innovation, Statistics Canada, and participating universities whose support is gratefully acknowledged. The views expressed in this article do not necessarily represent those of the Canadian Research Data Centre Network or that of its partners. We thank Stephanie Cantlay for her assistance in the Prairie RDC.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.E.S. reports royalties from UpToDate and consulting fees from Alnylam, Biogen, and Javelin. The other authors report no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: R.A.J. is supported by a Fellowship Grant from the Canadian Institutes of Health Research (Reference No. MFE 164702).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.