
Abstract
Background
Tremendous progress in acute stroke therapy has improved short-term outcome but part of this achievement may be lost in the long run. Concepts for a better long-term management of stroke survivors are needed to address their unmet needs and to reduce the burden of post-stroke complications, residual deficits, and recurrent vascular events.
Aims
This review summarizes current knowledge on post-hospital care and the scientific evidence supporting individual programs.
Summary of review
A systematic search of electronic databases according to PRISMA guidelines identified 10,374 articles, 77 of which met the inclusion criteria. One large randomised controlled trial on a multifaceted care program delivered by the multidisciplinary stroke team reduced recurrent vascular events and improved quality of life and functional outcome one year after the event, while a number of studies offer solutions for individual components of post-hospital disease management like patient education, counselling, and self-management or the management of post-stroke complications and residual deficits. A majority of studies, however, was small in size and limited by a short follow-up. Most initiatives with a narrow focus on risk factor control failed to lower the risk of recurrent events. The caregivers’ central role in post-stroke patient management is broadly neglected in research.
Conclusions
Over the past years, first knowledge on how to best organize post-hospital care of stroke patients has emerged. Comprehensive and pragmatic programs operated by the multidisciplinary stroke team hold promise to reduce the long-term health burden of stroke. There is a clear need for further high-quality studies with both clinical endpoints and patient-reported outcomes to establish sustainable solutions in different settings and regions to improve life after stroke, a key priority of the Stroke Action Plan for Europe 2018–2030.
Background
Structured follow-up programs are a well-established standard of care for myocardial infarction and cancer but so far not for stroke.1,2 In coronary and cancer patients, there is compelling evidence that standardized disease pathways positively affect risk factor profiles, quality of life (QoL), and functional status,1,2 whereas high-quality studies testing follow-up programs for stroke patients have not been available until recently.
Stroke is a leading cause of death and disability globally. The current lifetime risk of stroke is 25% for both men and women. 3 There are 14 million new strokes each year and over 80 million stroke survivors with a strong upwards trajectory given the continuous ageing of societies, population growth, and declining stroke fatality. 4 Exciting recent advances in acute stroke therapy translate into improved short-term outcome 5 which, however, may be lost in the long run through unmet needs in post-stroke care, post-stroke complications, residual deficits, and recurrent vascular events. Stroke is considered preventable by guideline-compliant control of risk factors and adequate vascular prevention may also be effective in preserving cognitive abilities. However, there is a significant gap between recommended preventive measures and real-world target level achievement of risk factors, especially in secondary stroke prevention. 6
Concepts for a better long-term management of stroke patients are urgently needed and the Stroke Action Plan for Europe 2018–2030 has declared life after stroke a key priority. 7 We herein report a systematic review of randomised controlled trials and rigorous scientific evaluations of structured multimodal intervention programs targeting longer term care of stroke patients.
Methods
Study design
This systematic review was conducted according to PRISMA guidelines. 8 It included peer-reviewed, qualitative and quantitative articles in English or German language without restrictions in time frame or countries.
Search strategy and selection criteria
We systematically searched PubMed and the Cochrane Library and extracted articles from the start of each database until 29 January 2021. Articles were eligible if (a) they comprised multimodal post-stroke care programs, (b) the interventions were initiated within one year after stroke, and (c) the outcome was specified and assessed during follow-up. The review’s focus is on stroke patients but several studies also enrolled TIA-patients. We did not consider studies with a primary focus on rehabilitation programs or specific rehabilitation approaches, early supported discharge, individual post-stroke complications and prevention or therapy thereof, psychological support and social participation. The search strategy and terms are detailed in the Online Supplement (Supplementary Table 1). We used the following filters: clinical trial, randomised controlled trial (RCT), meta-analysis, review, systematic review, and cohort study. The clinicaltrials.gov website was scanned for the same search terms to detect ongoing and unpublished studies. All articles identified were screened for relevant content in the title and abstract by CB and TT. Duplicates and study protocols were excluded. The shortlist of remaining articles was read in full and the citations searched for additional relevant publications.
Results
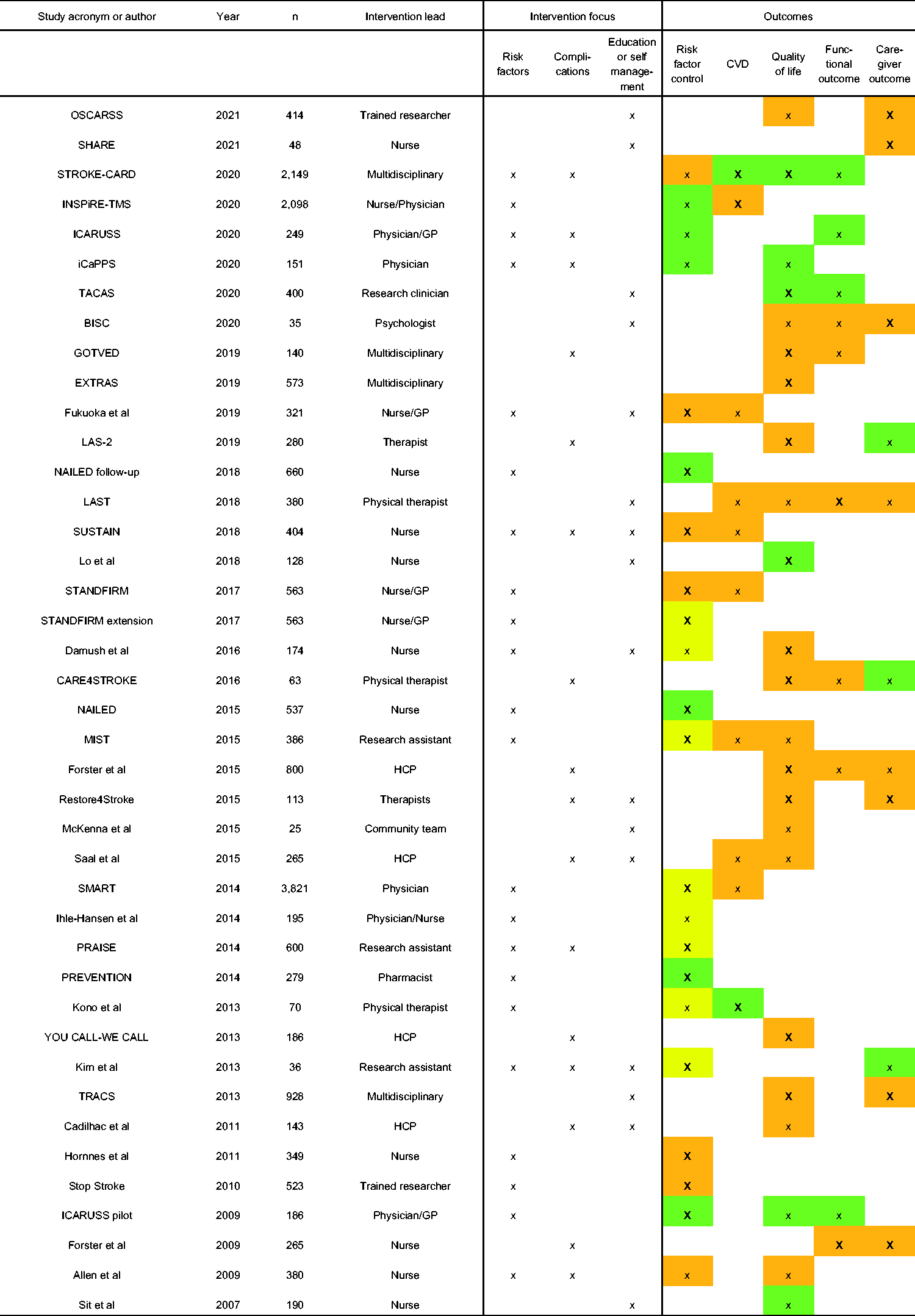
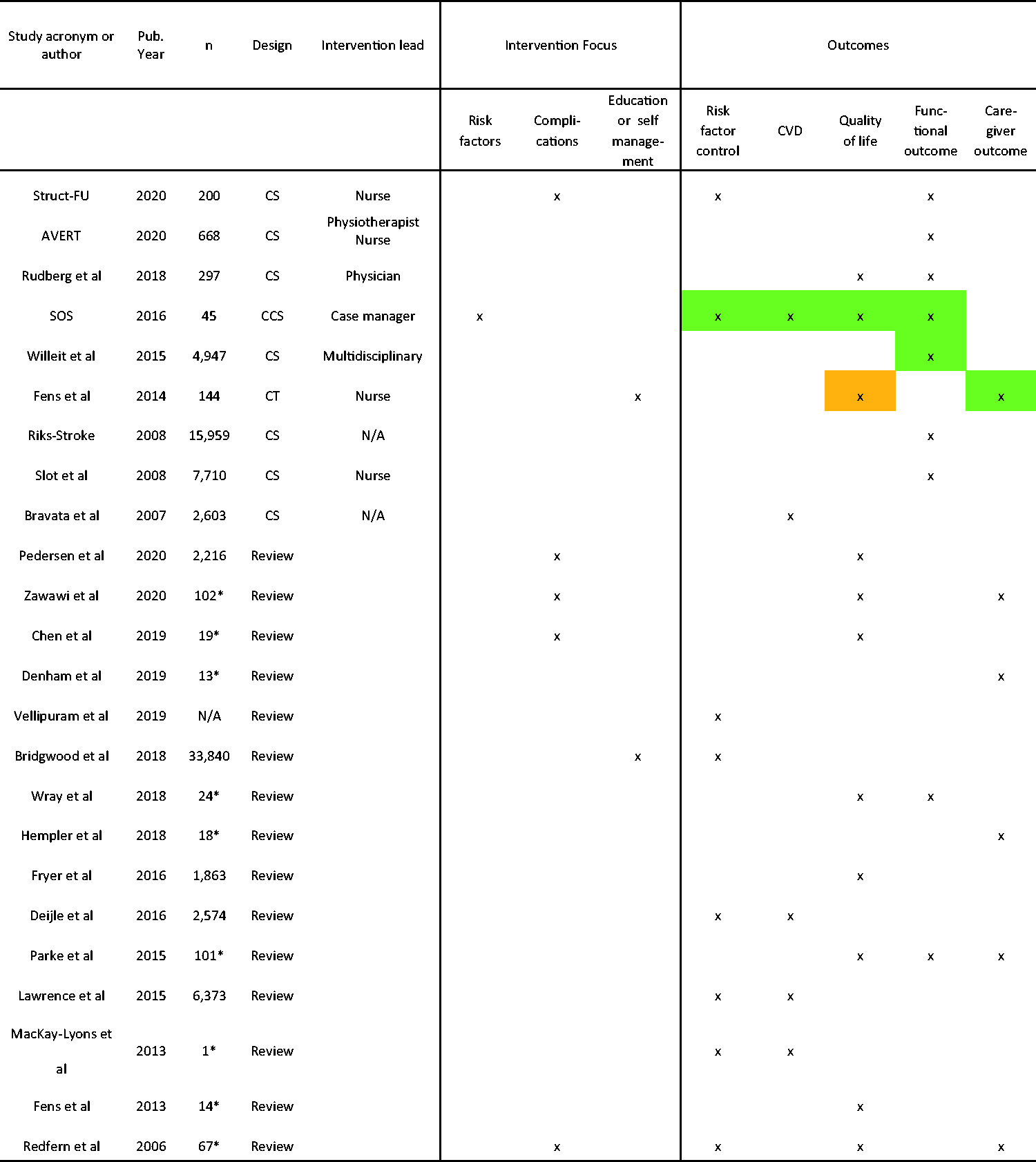
In total, 10,363 articles were retrieved from the database search and 11 additional records identified through check of citations and the clinicaltrials.gov website. Of 10,374 records, 99 were appropriate for the full-text review and 77 met the eligibility criteria. (Figure 1) Of the studies included, 41 were RCTs and 24 other types of studies and previous reviews. (Figures 2 and 3, Supplementary Table 2) Twelve additional studies have not reported final results, most are still ongoing (Supplementary Figure 1).
Flow chart of the review process. Summary of randomised controlled trials included in the review. Summary of other studies included in the review.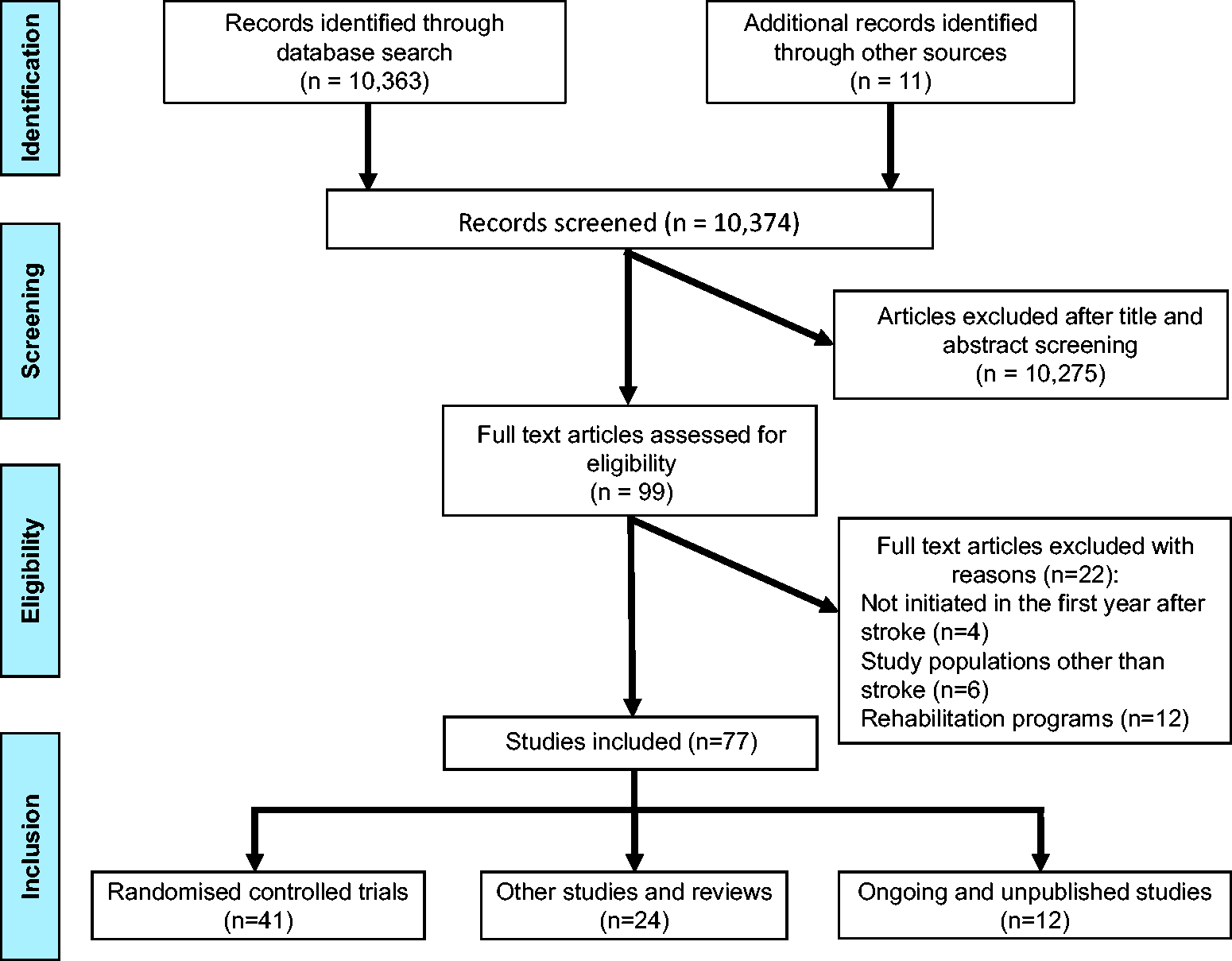
Large multifaceted RCTs
The SMART study (n = 3821, China) implemented a structured treatment and lifestyle modification algorithm involving stroke specialists. This in-hospital intervention did not show long-term effects on risk factor levels nor reductions in recurrent vascular events. 9 Two large European RCTs have been finished recently: INSPiRE-TMS (n = 2098, Germany/Denmark) employed a patient support program with up to eight outpatient visits including feedback and motivational interviews and repeated risk factor assessments to improve medication adherence. This trial included TIA and minor stroke patients and improved achievement of recommended prevention targets but failed to reduce recurrent vascular events during a follow-up of 3.6 years. In a post hoc analysis, patients attending more than half of scheduled appointments were less likely to suffer an outcome event. 10 The STROKE-CARD Study (n = 2149, Austria) included stroke and TIA patients except for patients with severe permanent disability. This study extended the responsibility of the multidisciplinary stroke team from acute therapy up to three months after the event, when a comprehensive outpatient re-evaluation was performed. It focused on residual deficits and additional rehabilitation demands, screening and treatment of post-stroke complications, management of vascular warning signs, re-evaluation of stroke aetiology, risk factor control, and patient/caregiver counselling. This study reduced recurrent vascular events and improved QoL (co-primary endpoints) as well as functional outcome (secondary endpoint) at 12 months. 11 However, it did not improve 12-month risk factor profiles compared with the control group, yet risk factor control was overall better than in real-world surveys from Europe. 12
Studies with a primary focus on risk factors
A majority of studies had their key focus on risk factor control which served as the primary study outcome. The ICARUSS program (n = 186, Australia) comprised four pre-scheduled three-monthly visits to the GP with constant advice by stroke specialists and improved target level achievement and functional outcome.13,14 The SOS project investigated a case manager-led pathway with educational sessions and regular check-ups. Pilot data on 45 patients revealed better risk factor control, less vascular events, and improved functional outcomes at 12 months. This pathway will be evaluated in a larger cohort study. 15 Another study (n = 70, Japan) enrolling minor stroke patients comprised salt restriction and exercise training offered by physical therapists once or twice per week for six months. 16 It improved risk factor control and reduced vascular events during a follow-up of almost three years. A Norwegian study (n = 195) implementing a comprehensive risk factor analysis and two lifestyle counselling visits reported improved risk factor control after one year. 17 In the NAILED trial (n = 537, Sweden), nurses performed a telephone-based risk factor assessment and counselling one month after discharge and a study physician adjusted pharmacological treatment if necessary. This procedure was repeated monthly until risk factor control was achieved. The program achieved sustained improvements in blood pressure and cholesterol levels up to three years.18,19 In the PREVENTION trial (n = 279, Canada), case management by pharmacists substantially improved risk factor control six months after stroke (compared with nurse-led case management) but this did not translate into less recurrent vascular events. 20 The PRAISE trial (n = 600, USA) tested potential effects of a group workshop intervention after discharge. The program reduced blood pressure on short notice but had no effect on other risk factors or medication adherence. 21 The MIST trial (n = 386, New Zealand) reported improved medication adherence but no sustained improvement in risk profiles and no cardiovascular disease benefit. 22 The STANDFIRM trial (n = 563, Australia), a multidisciplinary team approach including nurse-led home visits, showed no effects on risk factor control but patients were randomised in the post-acute phase and protocol adherence was suboptimal. 23 A long-term follow-up of STANDFIRM accomplished lower LDL-cholesterol levels at 12 months. 24 The Stop Stroke trial (n = 523, UK), providing electronic advice to patients, carers, and GPs failed to demonstrate effects on risk factors 25 as did a nurse-led intervention (n = 349, Denmark) based on four home visits for blood pressure measurement and counselling. 26 Four previous reviews on lifestyle interventions after stroke/TIA reported moderate reductions in systolic blood pressure but less consistent effects on other risk factors. Most studies considered had short follow-ups that only exceptionally exceeded six months. Interventions lasting longer than four months and using multiple techniques to achieve behavioural change were more effective. (Supplementary Table 2)
Studies targeting post-stroke complications and disability
A total of 23 studies employed standardized follow-up visits and screened for post-stroke complications and/or residual deficits. Post-discharge interventions including nurse-led, telephone-based, or more complex multidisciplinary approaches showed positive effects on anxiety and functional outcomes. Benefits, however, were mainly modest and partly disappeared over time. The Struct-FU study (n = 200, Sweden) 27 systematically applied a modified post-stroke checklist 28 and provided tailored advice, further diagnostic work-up, and therapeutic referrals. Over 90% of participants reported stroke-related health problems and over 80% required new interventions underscoring the relevance of an early comprehensive follow-up. 27 Two reviews suggested that treatment recommendations are often not implemented but documented positive effects on QoL especially if follow-up visits were combined with care and rehabilitation interventions. (Supplementary Table 2)
Studies focused on educational support or self-management programs
Seven studies directed main attention on educational support. TACAS (n = 400, New Zealand) organized one or two home visits with an educational and motivational intervention to patients and family members six weeks after stroke. This simple measure resulted in better QoL and improved functional outcomes after 6–12 months. Interestingly, the intervention emerged as particularly favourable in patients living alone or with a permanent support person and in female patients. 29 A nurse-led program early after discharge in patients with minor stroke (n = 190, Hong Kong) elicited positive effects on behavioural issues and medication compliance, 30 another study (n = 36, Republic of Korea) offering web-based education (regular use, 63%) showed benefits on health behaviours and caregiver mastery but not on risk factor control. 31 The LAST Study (n = 380, Norway) relied on individual coaching and observed a trend towards less vascular events during long-term follow-up. 32 Other studies relying on home visits or web-based interventions and outpatient group sessions showed no effects on QoL, functional status, and risk factor control.
Most initiatives offering self-management programs to stroke survivors reported on short-term outcomes and excluded patients with severe persistent deficits or aphasia. Five studies operating educational sessions, telephone calls, or group sessions showed modest short-term effects on mental health, QoL, and medication adherence. Reviews on self-management programs in specific settings (e.g. in-patient rehabilitation) found improvements in activities of daily living and QoL if the programs were initiated early after stroke.
Studies reporting caregiver outcome
Few studies addressed caregiver outcomes. Three intervention trials (n < 150, each) with a duration up to 18 months demonstrated small favourable effects on caregiver depression and fatigue by continued rehabilitation in their homes with a multidisciplinary team, caregiver exercise programs, or regular home visits to screen for healthcare issues. LAS-2 (n = 280, Sweden) showed positive effects on depression even after five years. 33 Benefits for caregivers translated into less readmissions of the cared patients in one of the trials. 34 Several other trials, however, reported null effects on QoL and caregiver burden including one well-designed large RCT (TRACS, n = 928). 35 Reviews on caregivers’ unmet needs agree that support by healthcare professionals is insufficient. More direct support in caring for the patients and for themselves, and a better access to training and healthcare services are warranted (Supplementary Table 2).
Ongoing and unpublished studies
Three large trials with multifaceted post-stroke interventions, a variety of outcomes, and in part longer follow-up periods are expected to further inform about post-stroke care in near future (Supplementary Figure 1). The COMPASS-trial in the US aims to include 6,000 stroke patients with a follow-up of three months. The intervention involves a telephone call after two days and a visit to the post-acute stroke clinic after 7–14 days to assess early problems after discharge. Outcomes are QoL, post-stroke complications, mortality, functional status, and caregiver strain. 36 Several studies with a focus on various clinical outcomes are still recruiting and two trials have been completed but are still unpublished (Supplementary Figure 1).
Discussion
Until now, no country in Europe is operating an evidence-based nationwide reimbursed post-stroke care pathway in spite of the many unmet needs for stroke survivors and their caregivers. Recurrent stroke and cardiovascular disease, post-stroke complications, residual neurological deficits, and inadequate medical and psychosocial care all contribute to long-term disability and QoL. A Swedish study revealed stroke-related health problems in 90% of stroke survivors necessitating medical interventions in more than 80%. 27 Moreover, half of stroke patients are readmitted to hospital (or die) within the first year. 37 The AVERT trial reported disappointing rehabilitation referral in working-age patients with minor stroke and only 6 of 10 patients finally returned to work. 38 On the other hand, good functional outcome three to six months after stroke predicts long-term survival and results in better QoL and lower healthcare costs.39,40 These findings altogether highlight the huge burden of post-stroke morbidity and suggest a window of opportunity for post-stroke care pathways early after stroke.
The Stroke Action Plan for Europe 2018–2030 gives life after stroke a key priority and claims for (a) national care pathways encompassing the entire chain from primary prevention to long-term care (overarching goal), (b) obligatory reviews of rehabilitation and patient needs three to six months after stroke and annually thereafter, and (c) broad expert support to patients and carers.7 Our systematic review summarizes current knowledge on post-stroke care and the evidence supporting individual programs. It indicates substantial under-research in this field compared to acute stroke therapy and long-term care of other major diseases but also emerging research interests in the last years. One large RCT (STROKE-CARD) successfully reduced the risk of recurrent stroke and cardiovascular disease and improved QoL and functional outcome. 11 This study considered multiple important aspects of post-stroke care (Supplementary Figure 2) and extended the responsibility of the multidisciplinary stroke team from acute management until the three-month intervention. Low-threshold contact to the team enabled frequent detection of vascular warning signs in this early vulnerable period after stroke (5% of all patients) and contributed to the prevention of vascular events. The pragmatic STROKE-CARD concept is suitable for routine application and reimbursement has been applied for in Austria to enable nation-wide implementation. Limitations are the short follow-up of one year and exclusion of patients with permanent severe disability who may also benefit from intensified care. A long-term extension of the RCT is currently underway (NCT04205006) and the ongoing STROKE-CARD registry will create evidence for patients with the most severe strokes (NCT04582825). A number of other promising RCTs on multifaceted care programs like COMPASS 36 (Supplementary Figure 1) will finish soon and inform about the optimal organization of post-stroke care in various settings.
The largest share of previous studies had a primary focus on risk factor control and demonstrated improvements in risk profiles, especially systolic blood pressure. Interventions longer than four months with multiple contacts to patients, involvement of stroke experts, and use of multiple techniques to achieve behavioural change were more effective.10,13–15,18–20,41,42 However, the few studies that reported effects on recurrent stroke and cardiovascular disease yielded disappointing findings.9,10,22,23,32,43 It is important to emphasize that these studies do not disregard the relevance of secondary stroke prevention but rather reflect short follow-up periods (effects of preventive measure increase over time) and the fact that patient enrolment per se improves medication adherence in both the intervention and control group. Accordingly, risk factor levels in the control groups of these trials were usually better than in real-world observational studies rendering it difficult to achieve additional benefits.10–12
A growing number of studies moved beyond risk factor management and addressed additional aspects of post-stroke care. Systematic screening for post-stroke complications and residual deficits has a considerable diagnostic yield. A majority of patients require tailored advice, further diagnostic work-up, and/or therapeutic and rehabilitation referrals. 27 In the STROKE-CARD trial, detection and management of post-stroke complications like anxiety, depression, fatigue, and attainment of additional rehabilitation demands contributed to improved functional outcome and QoL. Other studies revealed positive effects on anxiety, QoL, and activities of daily living, especially if follow-up visits were combined with care and rehabilitation interventions.29,33 This evidence endorse the recommendation of the Stroke Action Plan for Europe 2018–2030 to establish an obligatory three to six month review of stroke patients. 7 Patient-reported outcomes on QoL and mental health should be included in this review. Collection of robust data on health problems and outcome is relevant to convince healthcare stakeholders to reimburse post-stroke interventions.
Educational support involving targeted patient counselling and self-management programs are further appealing components of post-stroke care. The TACAS trial made a proof of concept that a pragmatic intervention with one or two home visits to conduct a motivational interview and verbalize the unmet needs of patients and caregivers translates into long-term benefits regarding QoL and functional outcome. 29 Self-management programs initiated early after stroke accomplished short-term improvements in activities of daily living, QoL, and medication adherence but most of these programs were not delivered to stroke patients with severe disability or aphasia.
The caregivers’ central role in patient management is broadly neglected in research. Few studies have addressed caregiver outcomes. Few studies including LAS-2 reported favourable effects on caregiver depression and fatigue 33 and in one of these trials, benefits for caregivers translated into less hospital readmissions of the cared patients. 34 However, the only large RCT (TRACS) failed to achieve improvements. 35 More information on support in caring for the patients and caring for themselves as well as a better access to training and healthcare services are warranted to improve the carers’ situation. There are unmet service needs and insufficient support delivered by healthcare professionals. Furthermore, the combination of behavioural interventions with improvements on the organizational level (i.e. implementation of multidisciplinary post-stroke care) seems to be crucial. 41
Limitations
We acknowledge that our selected search terms might not have detected all relevant articles, this may have affected the results. Though, by using two databases and the clinicaltrials.gov website as well as the reference lists, the risk for publication and reporting bias is low.
We did not consider programs targeting individual post-stroke complications including dementia, which is a major issue in stroke survivors, 44 and were not able to address all relevant aspects of post-stroke care.
Most intervention programs discussed herein were limited by short follow-ups compared to programs in myocardial infarction and cancer patients. Some studies might have yielded positive effects with longer follow-up periods, especially studies focusing on risk factor control.
Summary
Stroke care pathways improved patient outcome and currently cover acute stroke therapy 45 or stroke care at large including rehabilitation 46 but not post-stroke care. This systematic review identified one successful comprehensive post-stroke care program that extended the role of the multidisciplinary stroke team until three months after the event and a number of studies targeting individual important components of longer term post-stroke care like systematic screening for post-stroke complications and additional rehabilitation demands, refinement of secondary prevention, educational activities, patient counselling, and self-management programs. Most of these studies, however, were small in size, offered limited follow-up periods, and yielded partly inconsistent results. The carers’ needs and interests are substantially under-researched and broadly neglected in clinical routine. There is an urgent need for further high-quality RCTs with both clinical and patient-reported outcomes to further advance post-stroke care, establish sustainable solutions in different settings and regions, and improve life after stroke in the long run. Implementation of pragmatic nationwide long-term care programs with proper re-imbursement, involvement of the multidisciplinary stroke team, and continuous quality control holds great promise to reduce post-stroke morbidity and mortality and to meet the demands of stroke survivors and their caregivers, a key priority of the Stroke Action Plan for Europe 2018–2030. 7
Supplemental Material
sj-pdf-1-wso-10.1177_17474930211016963 - Supplemental material for Longer term patient management following stroke: A systematic review
Supplemental material, sj-pdf-1-wso-10.1177_17474930211016963 for Longer term patient management following stroke: A systematic review by Christian Boehme, Thomas Toell, Wilfried Lang, Michael Knoflach and Stefan Kiechl in International Journal of Stroke
Footnotes
Authors’ contributions
CB was involved in study design, screened papers for the review and prepared the manuscript. TT evaluated the screened articles and substantially revised the manuscript. WL and MK substantially revised the manuscript. SK was involved in study design, supervised the analysis and revised the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.